
Abstract
Venous thromboembolism (VTE) complications are the leading cause of preventable in-hospital mortality and morbidity in the United States. Initiatives by the National Quality Forum, the Joint Commission, and the Surgical Care Improvement Project aim to improve the prevention of VTE and emphasize the need to recognize the risk of the condition in hospitalized patients. In clinical practice, individual risk assessment using a validated scoring system provides patients with the best care in the prevention of VTE. This is accomplished by a weighted scoring of risk factors, selection of the most appropriate prevention strategy for patients at risk, and regular risk review across the continuum of care. All hospitals should have a local, written, care pathway which assesses inpatient risk of VTE as early as possible upon admission and identifies members of the health care team responsible for applying risk assessment. Venous thromboembolism risk should be regularly reassessed for any changes in the level of risk, with extended out-of-hospital prophylaxis considered for patients with continued risk factors, such as prolonged immobility or illness, treated at home, or in a long-term care facility. Finally, a mandatory alert system requiring the clinician to address the issue of prophylaxis before any orders are carried out by the nursing staff is one way to protect all hospitalized patients.
Keywords
Introduction
Venous thromboembolism (VTE), comprising deep vein thrombosis (DVT) and pulmonary embolism (PE), is a leading cause of preventable in-hospital mortality and morbidity in the United States. 1 Fatal PE is frequently the first sign of VTE and accounts for up to 10% of all hospital deaths.2,3 Prevention of VTE has been identified by the Agency for Healthcare Research and Quality (AHRQ) as the most important strategy for improving the safety of hospitalized patients. 4 Despite the existence of evidence-based consensus guidelines on the prevention of VTE, including recommendations from the American College of Chest Physicians (ACCP), 1 many patients remain at unnecessary risk of VTE during hospitalization. 5 These considerations are consistent with The National Quality Forum (NQF) standards, which call for all patients to be evaluated for VTE risk upon hospital admission and periodically thereafter, with appropriate VTE prophylaxis prescribed if necessary. 6 The NQF in collaboration with The Joint Commission has recently drafted an extended set of seven hospital-focused performance measures.6,7 These measures provide a venue to assess the implementation of safe-practice guidelines which target assessment, prophylaxis, and care management.6,7 A similar initiative was launched earlier for surgical patients, the Surgical Care Improvement Project (SCIP), with VTE-related performance measures aimed at reducing complications in surgical patients. 8 These initiatives emphasize the need to recognize the risk of VTE in hospitalized patients and act upon it accordingly. Adherence to, and reporting of, SCIP and NQF/Joint Commission VTE performance measures is increasingly becoming mandatory, linked to pay-for-performance measures and other reimbursement schemes.
This review discusses the importance of VTE risk assessment early after hospital admission, with emphasis on the continuation of prophylaxis and risk monitoring across the continuum of care.
The Disease Burden of DVT/PE
Anderson et al reported that 31% of all patients (both medical and surgical patients) hospitalized in the United States each year (>12 million patients) are at risk of VTE and meet current criteria for VTE prophylaxis.9,10 Venous thromboembolism has been traditionally regarded primarily as a complication occurring after surgery. However, a postmortem study into in-hospital deaths revealed that up to three quarters of fatal PE events and approximately two thirds of symptomatic VTE episodes occur in medical inpatients. 2
Pulmonary embolism and DVT are among the top 10 most common hospital adverse events. 11 In addition to the risk of fatal PE, VTE is associated with long-term health complications, including recurrent VTE, postthrombotic syndrome (PTS), and chronic pulmonary hypertension.12–16 A long-term clinical study reported that 30% of patients with VTE experienced a recurrent event after 8 years. 12 Postthrombotic syndrome, encompassing limb pain, swelling, and ulcers, is an important long-term complication of VTE occurring in 15% to 50% of patients within 8 years of an initial VTE episode.12–14,17 In a quality-of-life (QoL) study carried out during a 2-year period after a diagnosis of DVT in 387 patients, 47% of patients developed PTS. Development of PTS was the principal determinant of health-related QoL after VTE (P < .0001). Patients with PTS had lower scores on QoL questionnaires compared with those who did not develop PTS, and less improvement in QoL over time. 15
Venous Thromboembolism Risk Factors
Several independent risk factors for VTE have been identified. 10 Venous thromboembolism risk factors in hospitalized surgical and medical patients are listed in Table 1 and grouped according to their relative weight.18,19 Hospitalization per se has been shown to be an independent risk factor for the development of VTE. 10 Prolonged venous stasis due to bed rest and immobilization, and acuteness and severity of medical illness, or surgery are likely factors contributing to the overall increased risk associated with hospital confinement. 10
Venous Thromboembolism (VTE) Risk Factors in Hospitalized Surgical and Medical Patients According to Relative Strength
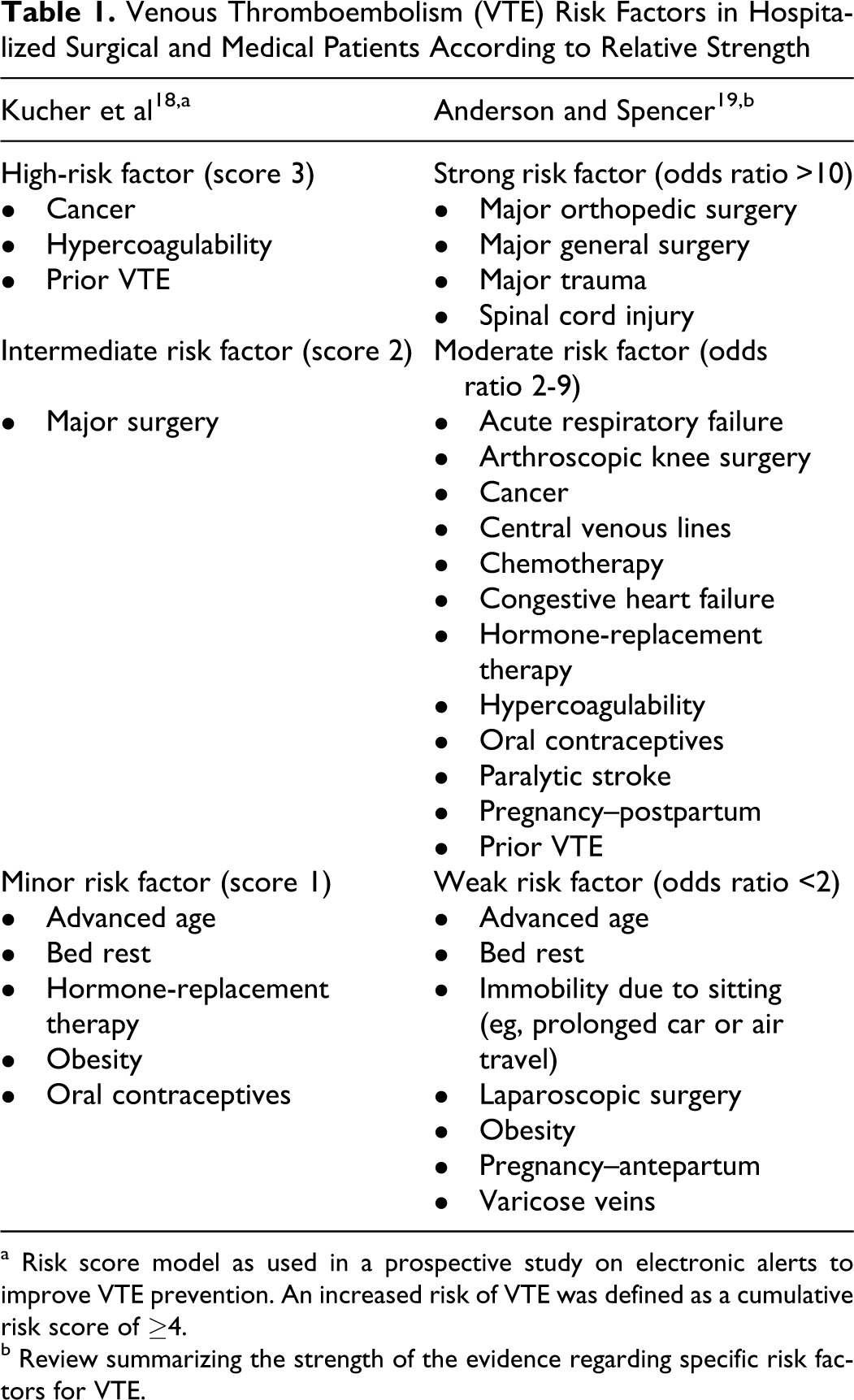
a Risk score model as used in a prospective study on electronic alerts to improve VTE prevention. An increased risk of VTE was defined as a cumulative risk score of ≥4.
b Review summarizing the strength of the evidence regarding specific risk factors for VTE.
Predisposing or patient-related risk factors that affect the incidence of VTE among inpatients include increasing age, obesity, cancer, previous VTE, varicose veins, thrombophilia, oral contraceptives, and hormone replacement. 20 A study by Borow and Goldson reports that age >60 years and length of surgery are factors significantly increasing the risk of VTE. 21
Venous thromboembolism is an important complication of malignancy 22 and the second most common cause of death among the patients with cancer. 23 In addition to cancer, major surgical procedures, chemotherapy, and central venous catheters contribute to the cancer patients with systemic thromboembolic risk.10,24 Individual patients are often exposed to multiple risk factors that are cumulative to the overall risk.19,22,25
Individual VTE Risk Assessment
One approach to identify patients at VTE risk is a group-specific routine approach, as detailed in the 2008 ACCP recommendations for thromboprophylaxis of hospitalized patients. 1 These guidelines stratify surgical patients into group-specific categories of risk (Table 2 ); risk levels are less well defined for medical patients. 1 In the most recent update, the guidelines state in a section (1.4.5) on application of evidence to individual patients: “Decisions about prescribing thromboprophylaxis for the individual patient are best made by combining knowledge of the literature (including the recommendations provided herein) with clinical judgment, the latter based on specific knowledge about each patient’s risk factors for VTE.” 1
Recommended Prophylaxis Options1
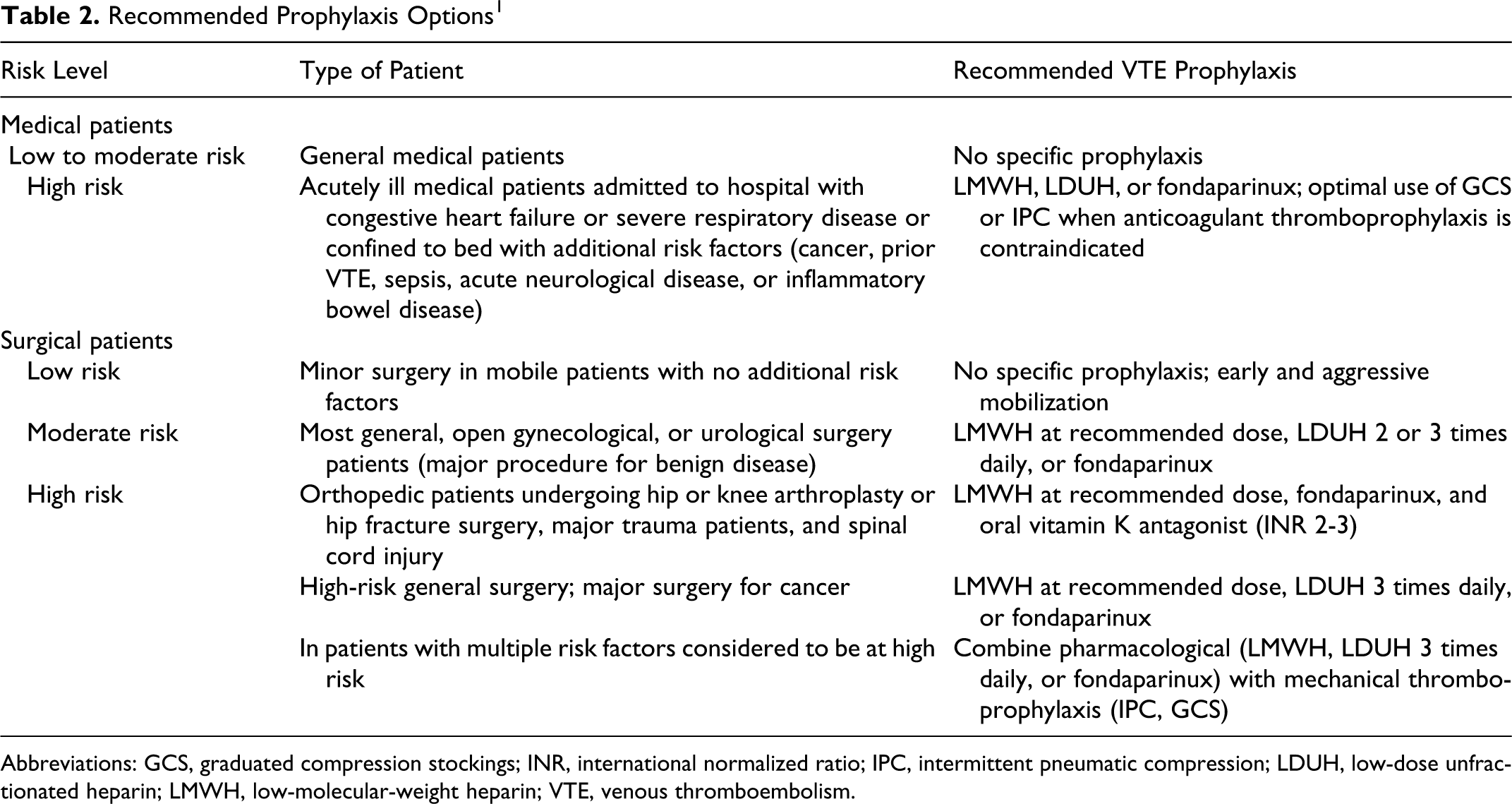
Abbreviations: GCS, graduated compression stockings; INR, international normalized ratio; IPC, intermittent pneumatic compression; LDUH, low-dose unfractionated heparin; LMWH, low-molecular-weight heparin; VTE, venous thromboembolism.
This section seems to contradict an earlier section (1.3) on risk stratification where a group-specific approach for routine thromboprophylaxis for all patients who belong to each of the major target groups is supported, rather than individual thromboprophylaxis prescribing. 1 The use of clinical judgment suggested by the former statement is an important concept because many of the patients seen in clinical practice do not match inclusion criteria of clinical trials and the clinical trial data may not apply.
Each patient has a unique set of thrombotic risk factors which may not “fit” neatly into a preset level of risk.5,26 Therefore, both the strength of the patient’s risk factors and the cumulative weight of these risk factors must be taken into account when assessing the overall VTE risk. Accurate VTE risk assessment for individual patient is important for selecting patients who benefit from prophylaxis. 5 Due to the unique VTE risk profile of each patient, individual risk assessment should be carried out as early as possible using a clinically validated, hospital-approved risk-assessment model18,27–34 (RAM; Figure 1 ). Advantages of individual risk assessment include individual risk-factor profiles with tailored prophylaxis measures.28,29
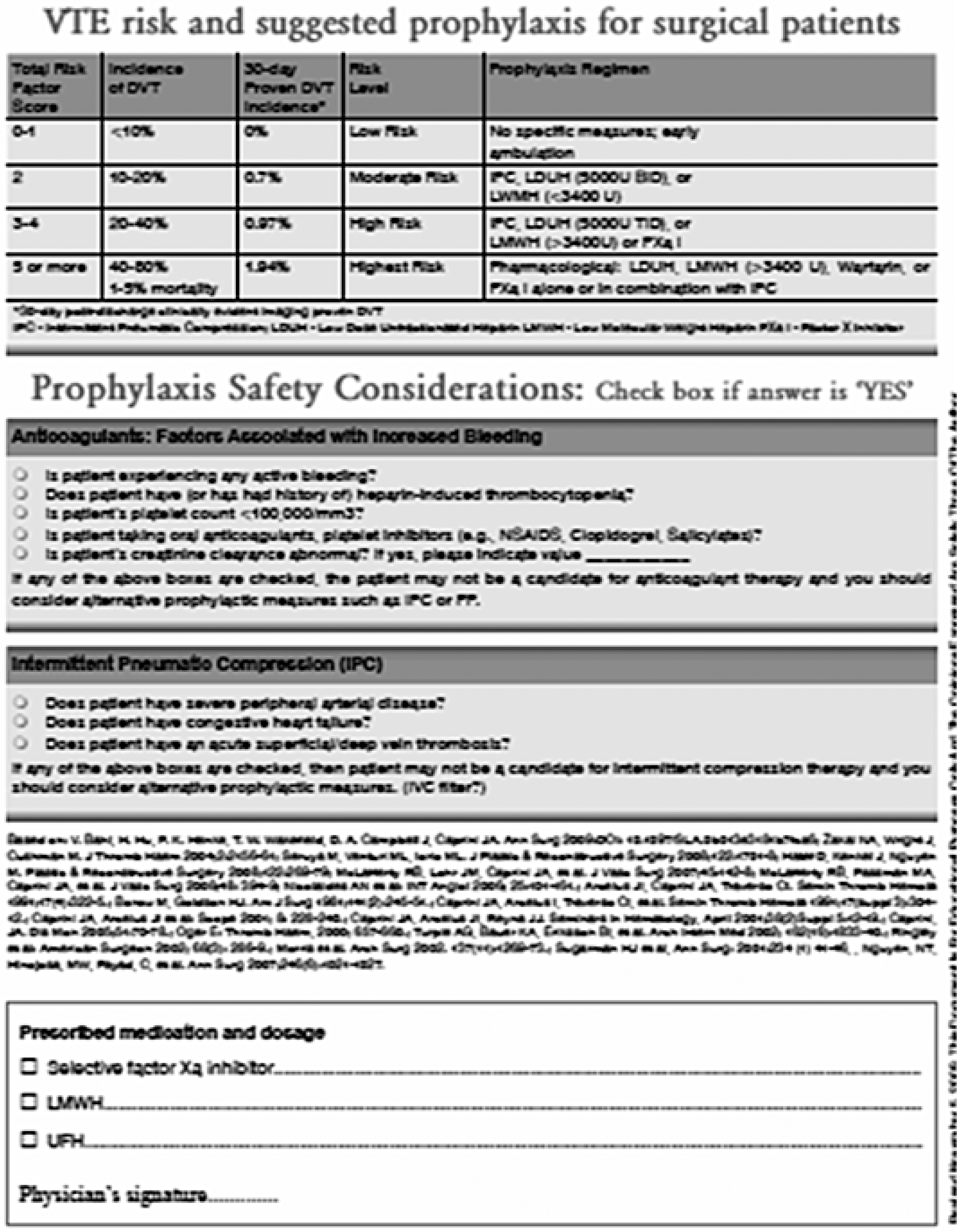
Example of a risk-assessment model.
The case study described in Table 3 exemplifies the case of individual versus group prophylaxis; according to patient groups identified to be at risk in the ACCP guidelines, this patient would not have been considered to be at risk of VTE due to the nature of her injury and the surgical procedure. However, individual risk calculation identified her to be at high risk of VTE. 35
Case Study
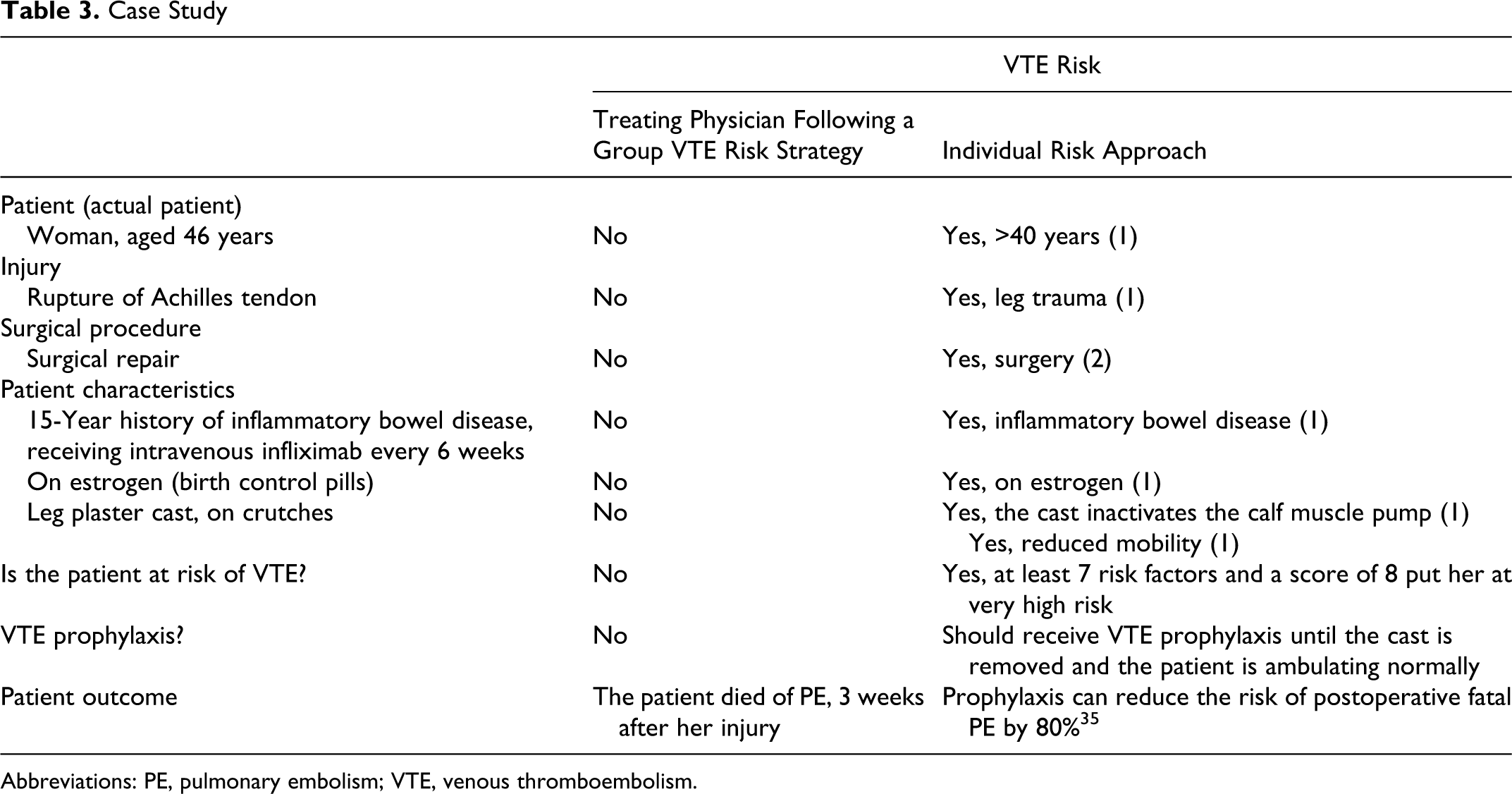
Abbreviations: PE, pulmonary embolism; VTE, venous thromboembolism.
Risk of VTE cannot, however, be viewed in isolation, and the concomitant risk factors for bleeding must also be taken into account when considering the appropriateness of thromboprophylaxis. Recently, Decousus and colleagues utilized a multivariate analysis to identify and score factors associated with bleeding risk in medical patients (Table 4 ). The authors also created an online resource where bleeding risk can be assessed (available at: http://www.outcomes-umassmed.org/IMPROVE/bleeding_risk_score.cfm). 36
Bleeding Risk Factors in Medical Patients According to Relative Strength36
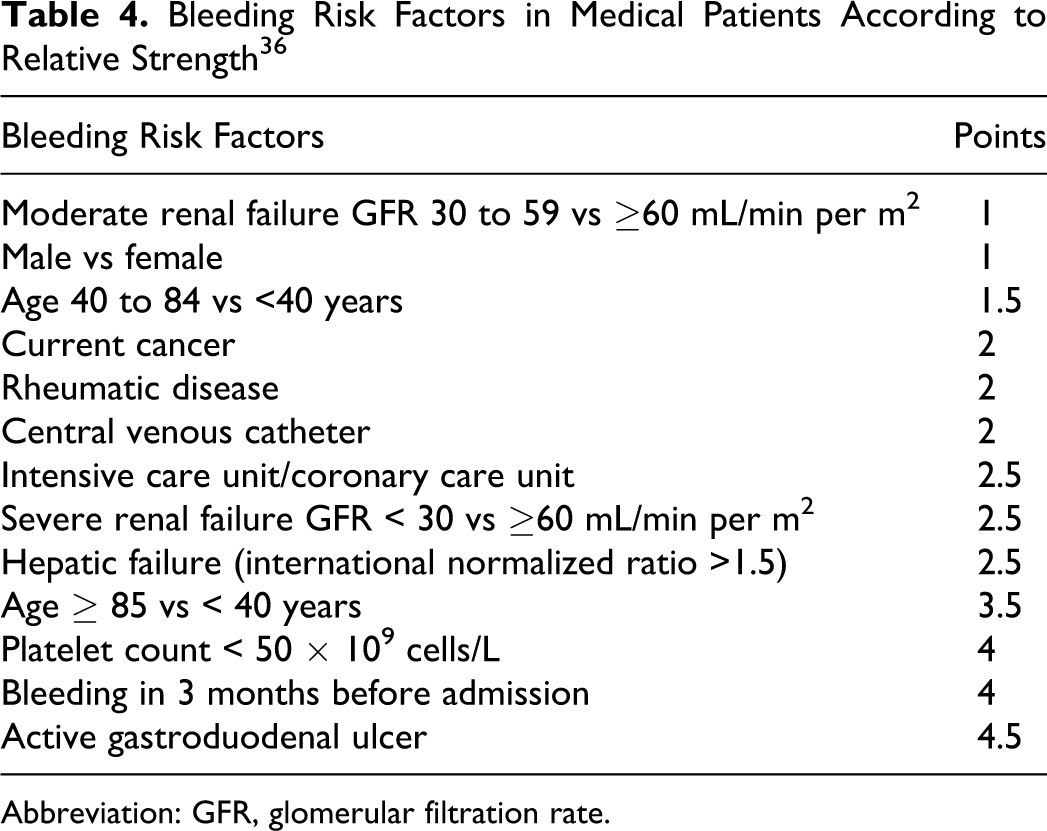
Abbreviation: GFR, glomerular filtration rate.
In summary, certain broad groups of patients should be considered for VTE prophylaxis. Although data suggest that for large heterogeneous patients groups, such as medical patients, the absolute benefits of VTE prophylaxis may be small, 1 individualized risk assessment offers a possible route for the optimization of patient care. Through the identification of those patients not at risk of VTE, those patients at risk of bleeding, and those patients at very high risk of VTE, individualized risk assessment allows the tailoring of appropriate patient-specific prophylactic regimens. Such targeted prophylaxis may result in an increase in the absolute benefits to patients, although large-scale studies would be required to confirm this. In addition to RAMs and consensus recommendations from the literature, a decision concerning any patient is best made by applied clinical judgment and extrapolation from limited clinical data in some patient groups.
Venous Thromboembolism Prophylaxis
The current recommended VTE prophylaxis options for surgical and medical patients are listed in Table 2. Methods used to establish a diagnosis of DVT include
Several further studies have shown that reductions in asymptomatic VTE events with thromboprophylaxis parallel a similar reduction in symptomatic VTE.39–42 A meta-analysis by Eikelboom et al, of 3999 patients analyzed from 9 studies demonstrated that in patients undergoing hip or knee replacement surgery, extended-duration prophylaxis for 30 to 42 days significantly reduced the risk of symptomatic VTE versus placebo or untreated control (1.3% vs 3.3%; odds ratio [OR], 0.38; 95% CI, 0.24%-0.61%). 40 This reduction in symptomatic VTE paralleled a reduction in asymptomatic, venographically detected DVT (9.6% vs 19.6%; OR, 0.48; 95% CI, 0.36%-0.63%). Extended-duration prophylaxis versus control was not associated with an increase in major bleeding (0.1% vs 0.3%; OR, 0.62; 95% CI, 0.22%-1.75%) but did increase the rate of minor bleeding (3.7% vs 2.5%; OR, 1.45; 95% CI, 1.08%-2.26%). 40 These studies highlight the importance of risk-appropriate, evidence-based prophylaxis to reduce the number of asymptomatic VTE events in high-risk patients and to reduce the risk of these events becoming symptomatic.
No randomized controlled trials have been performed for patients such as the one presented in the case study (Table 3). However, Kakkar showed that prophylaxis cuts the risk of fatal PE by 80% compared with no prophylaxis in surgical patients (0.098% [2 of 2045] vs 0.771% [16 of 2076]; P < .005). Wound hematomas occurred more frequently with prophylaxis (7.7% [158 of 2045] vs 5.6% [117 of 2076]; P < .01). 35 Collins et al reaffirmed these results in 16 000 patients from 70 medical centers collected in the decade that followed the original multicenter trial, reporting a reduction of 64% ± 15% (P < .0001) in fatal PE but with increased bleeding. 43 A more recent study reported that anticoagulant prophylaxis was also associated with a significant reduction in fatal PE in medical patients (relative risk [RR], 0.38; 95% CI, 0.21%-0.69%), with a nonsignificant increase in major bleeding (RR, 1.32; 95% CI, 0.73%-2.37%). 44 Logic and experience should guide the physician in appropriately using preventive measures in those patients for whom clear guidance is lacking, but who were individually identified to be at risk of VTE.
The Care Pathway in VTE Prevention
At Admission
All hospitals should have a local, written, care pathway based on clinical guidelines, which assesses inpatient risk of VTE at admission and which allows the treating physician to decide on the most appropriate management. Indeed, the current ACCP guidelines include “that every hospital develop a formal strategy that addresses the prevention of VTE,” as a key recommendation. 1 In order to improve the quality of care and early identification of patients at VTE risk, a multidisciplinary team or steering committee should be established in every hospital. It is important to identify members of the health care team, such as nurses, pharmacists, VTE specialists, and treating physicians, who could be responsible for applying RAMs. Nurses could play a greater role in VTE risk assessment, timely diagnosis, appropriate prophylaxis, patient education, and psychological support. Successful nurse involvement, such as a nurse-managed VTE care pathway, would heighten clinical surveillance on individual patients.45,46 The skills of nurses should be utilized to a greater extent. However, at the present time, they are required to assess the patient for fall risk, psychosocial risk, ulcer risk, and others. Some feel these nurses may experience “assessment fatigue” and should not be asked to add yet another assessment to their long list. However, it is well known that VTE is the number one preventable cause of in-hospital mortality, 1 and this should be considered when setting assessment priorities for nurses. The importance of pharmacists in the care pathway has recently been underlined in a systematic review by Mahan and Spyropoulos. 47 Five pharmacy-driven interventions aimed at improving VTE prophylaxis were reviewed and demonstrated substantial improvements in patient care. It should be noted, however, that although pharmacy-driven, all 5 interventions were multidisciplinary in nature. The importance of an integrated multidisciplinary approach to the care pathway cannot be overstated. In addition, further education across all professional groups regarding risk assessment and administration of appropriate prophylaxis would improve the coordination of patient care through the continuum.
One helpful technique would be to involve patients in their own care. This can be accomplished by asking each patient to complete a simple form listing most of the common risk factors. This can be done on admission or earlier in the physician’s waiting room. The completed form can be given to the admitting physician, nurse, or physician assistant who can then complete the risk-assessment form.
Active multifaceted systems aimed at reducing VTE risk have the greatest effect. The systematic review by Mahan and Spyropoulos advocates both human- and computer-based active alert systems. 47 The use of a computer-prescribing alert system linked to altered care procedures significantly increases the use of prophylaxis by physicians.18,48 Computer alert systems can also reduce the incidence of VTE. In one series by 41% during a 90-day study period (4.9% vs 8.2%; P = .001), with no difference in major (1.5% vs 1.5%; P = .87) or minor bleeding complications (6.5% vs 7.0%; P = .43) or mortality (22.5% vs 22.3%; P = .74). 18 Computerized decision-support software linked to patient VTE risk assessment can be highly successful in increasing appropriate prophylaxis. 49 However, in a study of 866 patients at high risk of VTE who were not receiving thromboprophylaxis, a majority of physicians (62.3%) did not order VTE prophylaxis, despite receiving an electronic alert. These results suggest that electronic alerts alone may be insufficient. 50
There are other ways to ensure early VTE risk assessment of patients upon admission to hospital. Mahan and Spyropoulos stress the potential utility of RAMs in identifying specific at-risk populations to allow targeted use of prophylaxis. 47 Caprini et al proposed a RAM, comprising a simple, hospital-wide, and self-contained scoring sheet for risk stratification of both surgical and medical patients based on clearly defined clinical settings and the presence of specified risk factors (Figure 1). Partial validation has been carried out in medical patients and in patients screened in the American Venous Forum screening program.29,51 Recently, formal validation of this tool was published in a study by Bahl et al of 8216 surgical patients from the University of Michigan. The risk score correlated with the 30-day incidence of clinically evident and imaging-proven VTE. This retrospective VTE risk scoring method based on the Caprini RAM has shown that the rate of acquired VTE within 30 days appears to accelerate for patients identified as having the highest cumulative risk score, whereby patients with a score of 9+ have a VTE incidence rate of 6.5% (Figure 2 ). 32 Further data validating the Caprini RAM, in a varied cohort of 1126 cosmetic and reconstructive surgery patients, has recently been published by the Venous Thromboembolism Prevention Study (VTEPS) Network. Importantly, as well as confirming the increasing VTE risk with increasing Caprini score, this study showed that individuals with a score of >7 experienced 50% of their VTE events at 15 to 60 days postsurgery. Thus, the use of this RAM offers an opportunity to identify high-risk patients who may benefit from extended duration prophylaxis. 52 Validation of the previously mentioned electronic alert-based RAM developed by Kucher et al revealed a similar correlation between risk score and VTE rate. However, this model showed a lesser sensitivity for low-risk patients, likely due to incorporating less risk factors than the Caprini/Bahl model. 47 A further predictive and evidence-based VTE risk score, specifically designed for medical patients and based on a large multicenter study of 15 156 patients, derived a weighted scoring system from the hazard ratios of 7 independent VTE risk factors. These risk factors are previous VTE (assigned 3 points), thrombophilia (2 points), lower limb paralysis (2 points), current cancer (2 points), immobilization ≥7 days (1 point), ICU/CCU stay (1 point), and age >60 years (1 point).53,54
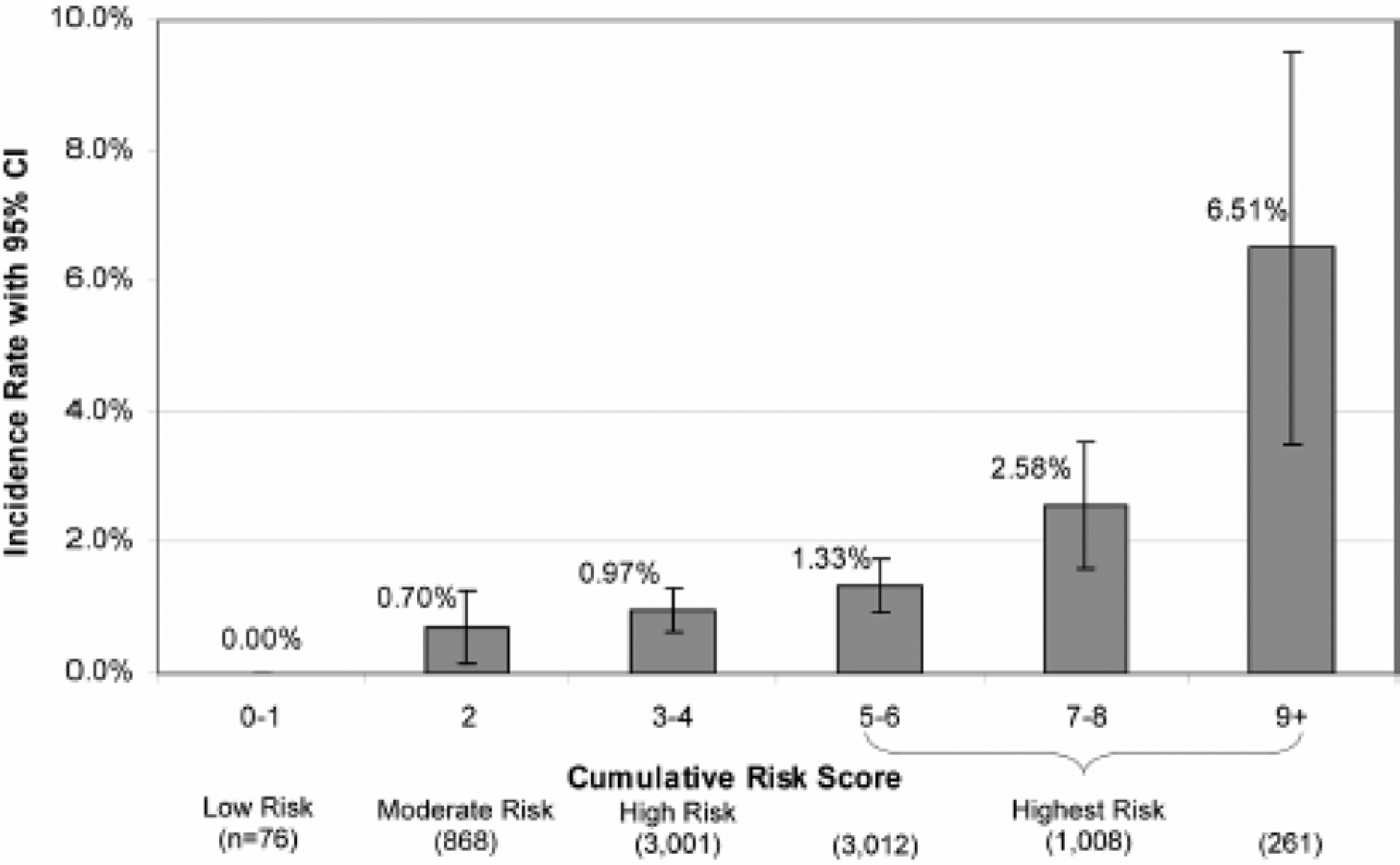
Clinically proven venous thromboembolism rates at 30 days: incidence rate by risk level and cumulative risk score. 32 Reprinted with permission.
A valuable source of information recently provided by the AHRQ is a guide for the practitioner on important steps in the quality improvement process, including the creation or adaptation of protocols that standardize VTE risk assessment embedded in patient care (http://www.ahrq.gov/qual/vtguide/).
During Hospital Stay
Venous thromboembolism risk should be regularly reassessed during a patient’s stay in hospital for any change in the level of risk. Potentially, additional VTE risk factors may arise as a result of hospitalization, for example, prolonged immobility or sepsis. A decrease in VTE risk during hospitalization is less likely to occur. Individual risk assessment is important in determining the timing of onset, intensity, and duration of prophylaxis, as well as the choice of prophylaxis method.
Continued Care After Hospital Discharge
Continued outpatient prophylaxis is of particular importance, given the continued VTE risk in the outpatient setting and the trend for reduced duration of hospital stays.19,55–57 Data from the Registro Informatizado de la Enfermedad TromboEmbólica (RIETE) registry illustrate that more than half (55%) of symptomatic, postoperative VTE events occur over 15 days after surgery. Overall, 77% of the 3500 DVT patients entered into the database developed their VTE events following hospital discharge and 53% of these events occurred after prophylaxis was stopped. 55 The Million Women Study reveals that increased risk of VTE subsequent to surgery can, in fact, persist for a duration of 12 weeks. 57 This was a prospective cohort study involving 947 454 women followed for 6 years. Surgery was carried out in 239 614 patients with 5419 VTE events, including 270 VTE-related deaths. Compared with not having surgery, women were 70 times more likely to be admitted with VTE in the first 6 weeks after an inpatient operation and 10 times more likely after a day case operation. The risks were lower, but still substantially increased, 7 to 12 weeks after surgery. 57
In medical patients, the increased VTE risk is similarly prolonged; in a study of 158 325 medical discharges, the median time for developing VTE was 74 days. 56 These data along with the Bahl et al 32 and Panucci33,52 data illustrate another important feature of the scoring system, namely the significant incidence of VTE events at 30 and 60 days in those with high scores. Repeat risk assessment as part of the discharge planning process may, therefore, be useful in identifying patients who will remain at risk of VTE postdischarge; in particular, to determine which patients would benefit the most from long-term prophylaxis and guide the decision on the duration of prophylaxis that individual patients should receive.
Standard recommended duration of prophylaxis in major orthopedic surgery, for example, is a minimum of 10 days, 1 which effectively means that most patients should receive outpatient prophylaxis as the average hospital stay is approximately 4 days. 19
Further extended prophylaxis for up to 35 days is recommended after total hip replacement, total knee replacement, or hip fracture surgery. 1 Ample clinical evidence is available that extended prophylaxis with either a low-molecular-weight heparin (enoxaparin or dalteparin) or fondaparinux can prevent late-occurring VTE complications after several major surgical procedures, including major orthopedic surgery and abdominal surgery (Table 5 ).40-42,58,59 The Extended Prophylaxis for Venous ThromboEmbolism in Acutely Ill Medical Patients With Prolonged Immobilization (EXCLAIM) study provided clinical evidence that the use of extended prophylaxis with enoxaparin also reduced VTE more than it increased major bleeding events in certain groups of acutely ill medical patients, namely those with level 1 immobility, those aged >75 years, and women. 60 Two trials, A Phase 3 Randomized, Double-Blind, Parallel-group, Multi-center Study of the Safety and Efficacy of Apixaban for Prophylaxis of Venous Thromboembolism in Acutely Ill Medical Subjects During and Following Hospitalization (ADOPT) and Multicenter, Randomized, Parallel Group Efficacy and Safety Study for the Prevention of Venous Thromboembolism in Hospitalized Medically Ill Patients Comparing Rivaroxaban With Enoxaparin (MAGELLAN), are investigating extended duration prophylaxis with new oral anticoagulants. 61 The trials will investigate the efficacy of extended duration prophylaxis with apixaban and rivaroxaban in medical patients, for 30 and 35 days, respectively, in comparison to enoxaparin during hospitalization (6-14 days) and placebo after hospital discharge. Data from these trials may offer additional information as to the benefits of extended prophylaxis in medical patients. Further studies will be needed to identify subgroups of high-risk medical patients for whom there is a cost-effective clinical benefit of extended thromboprophylaxis.
Clinical Evidence for the Use of Extended-Duration Prophylaxis in Surgical Patients
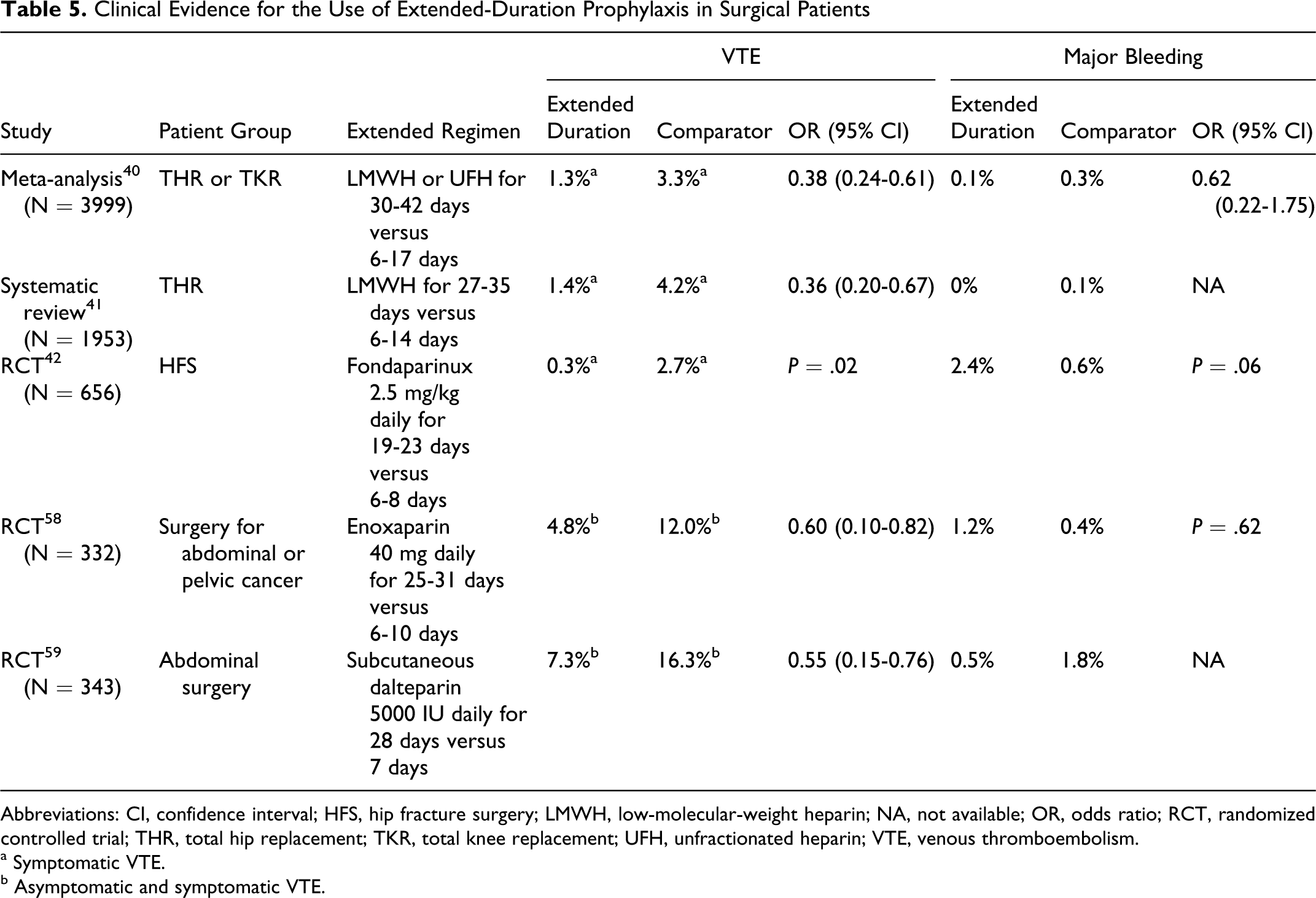
Abbreviations: CI, confidence interval; HFS, hip fracture surgery; LMWH, low-molecular-weight heparin; NA, not available; OR, odds ratio; RCT, randomized controlled trial; THR, total hip replacement; TKR, total knee replacement; UFH, unfractionated heparin; VTE, venous thromboembolism.
a Symptomatic VTE.
b Asymptomatic and symptomatic VTE.
For many patients, outpatient prophylaxis is advised due to short hospital stay or prolonged prophylaxis. 62 There is a need for hospital protocols that allow for appropriate transition of care. The transition between acute and long-term care is an important opportunity to reduce the incidence of VTE. 63 The NQF recommends that provision be made for guideline-directed therapy that addresses care setting transitions. 6 Risk factors for VTE during transition of patients, such as the elderly, through subacute care settings or rehabilitation centers have not been clearly defined, except for major surgical procedures and stroke.1,26,64 Nursing-home residents who develop VTE are 4.6 times (95% CI, 1.65%-13.06%; P = .004) more likely to have returned from hospital compared with nursing-home residents who do not develop DVT. They are also more likely to require assistance with mobility-related activities, such as personal hygiene (OR, 3.35; 95% CI, 1.26%-8.94%; P = .02), toileting (OR, 4.00; 95% CI, 1.37%-11.70%; P = .01), or wheelchair use (OR, 2.69; 95% CI, 1.26%-5.74%; P = .01). 63 There is an urgent need to define the risk factors and assess the benefit of extended-duration prophylaxis in this growing population of patients hospitalized in long-term care or rehabilitation centers.
Conclusions
Assessment of individual patient’s VTE risk is vital for the selection of appropriate, evidence-based thromboprophylaxis. Venous thromboembolism risk assessment should occur as early as possible after patients are admitted to hospital and involve a multidisciplinary team. The use of a validated risk-assessment tool featuring risk factors tied to the development of clinically relevant VTE at 30 and 60 days is suggested. Venous thromboembolism prophylaxis prescribing plans should encompass the entire period of VTE risk (including postdischarge period) and include prescribing plans for prolonged prophylaxis (if required) and treatment plans in case of bleeding complications. A multidisciplinary team involved in risk assessment and regular reviews of VTE prophylaxis across the continuum of care should help reduce the incidence of symptomatic VTE. Finally, mandatory implementation of prophylaxis carefully balanced to the patient’s risk of both thrombosis and bleeding should reduce the incidence of these thrombotic complications.
Footnotes
Acknowledgments
The author received editorial/writing support from Hester van Lier, PhD, of Excerpta Medica, in the preparation of this manuscript funded by sanofi-aventis, NJ, USA.
The author has no current consulting agreements but has been a consultant in the past for Sanofi, GSK, Covidian, and Pfizer.
The author(s) received no financial support for the research and/or authorship of this article.