
Abstract
The present systematic review was conducted to assess the efficacy and safety of apixaban versus other anticoagulants, for the prevention of venous thromboembolism (VTE) following total hip replacement (THR) and total knee replacement (TKR) surgery. Electronic databases were interrogated to identify relevant randomized controlled trials. A series of direct/indirect comparisons and a network meta-analysis were conducted. Indirect comparisons found that the odds ratio of “all VTE and all-cause death” were significantly higher for dabigatran than for apixaban in patients with THR (odds ratio [OR], 2.51; 95% confidence interval [CI], 1.50-4.21) and TKR (OR, 1.72; 95% CI, 1.22-2.42). Rivaroxaban showed similar efficacy to apixaban in patients with THR and TKR (OR, 0.69; 95% CI, 0.38-1.25 and OR, 0.83; 95% CI, 0.57-1.19, respectively). No significant differences were observed in bleeding outcomes between treatments. The novel anticoagulants apixaban, rivaroxaban, and dabigatran demonstrated similar or improved efficacy and similar safety compared with current therapies in this indication.
Keywords
Introduction
Venous thromboembolism (VTE) collectively describes the sometimes debilitating, painful, and potentially fatal conditions of deep vein thrombosis (DVT) and pulmonary embolism (PE). Deep vein thrombosis is the formation of a thrombus in a deep vein, most commonly of the lower limbs, and the potentially fatal PE is caused when such thrombi become dislodged and travel to the lungs.
Venous thromboembolism represents a considerable preventable morbidity and mortality burden to patients and is estimated to be responsible for 25 000 preventable deaths annually in the United Kingdom. 1 Risk factors for VTE include increasing age, obesity, cancer, and medical conditions such as cardiac and respiratory diseases, surgery, and inherited or acquired clotting tendency. High-risk surgical procedures can lead to VTE, and patients undergoing major orthopedic surgery, such as total hip replacement (THR) or total knee replacement (TKR) are in the highest risk category for VTE. 2 In the absence of anticoagulant prophylaxis, the estimated incidence of DVT following orthopedic surgery ranges from 40% to 60%, and the overall risk of fatal PE has been estimated to be between 0.2% and 0.3%. 3
Thromboprophylaxis, both mechanical and pharmacological, is a current standard practice for the prevention of VTE in patients undergoing orthopedic surgery. Current treatment guidelines recommend the routine administration of a prophylactic anticoagulant for at least 10 days and up to 35 days following orthopedic surgery. 3,4 Currently available anticoagulant therapies include warfarin, fondaparinux, and the more commonly used low-molecular-weight heparins (LMWHs), such as enoxaparin, bemiparin, and tinzaparin. These agents have demonstrated efficacy but are associated with a number of limitations. There is a requirement for regular monitoring of warfarin and, in some regions, a requirement for the monitoring of platelet counts in those on LMWHs. Both LMWHs and fondaparinux require parenteral administration, and warfarin has a narrow therapeutic window which is difficult to attain. 2
A number of new oral anticoagulants have been developed and are undergoing evaluation as thromboprophylaxis in orthopedic surgery. Rivaroxaban (a highly specific factor Xa inhibitor) and dabigatran etexilate (a direct thrombin inhibitor) have been assessed in large randomized controlled trials (RCTs) of THR and TKR surgery and have demonstrated similar or greater efficacy and similar safety compared with standard LMWH. 5 -10 Both rivaroxaban and dabigatran etexilate have been approved in over 70 countries for the prevention of VTE in patients having elective THR or TKR surgery. 11
Apixaban, recently approved in the European Union for the prevention of VTE following THR or TKR surgery, is a highly specific factor Xa inhibitor that is administered orally and does not require routine laboratory monitoring. 12 Clinical trials in patients who have undergone elective THR and TKR have demonstrated that apixaban has improved efficacy, when compared with enoxaparin, in reducing VTE and all-cause death, with a similar or lower risk of bleeding. 13,14
The aim of this systematic review and meta-analysis was to compare the efficacy and safety of apixaban versus other key comparators, for the prevention of VTE following elective TKR or THR surgery, via a series of direct and indirect comparisons and a network meta-analysis (NMA).
Methods
Systematic Review
Searches of MEDLINE, EMBASE, the Cochrane library, and CINAHL were conducted on July 8, 2010. Using Boolean operators, the searches combined terms (including MeSH headings as appropriate) for (1) VTE, (2) interventions, (3) clinical trial design, and (4) hip/knee replacement. The following conference proceedings were handsearched (2008-2010 inclusive): American Society of Hematology British Orthopaedic Association International Congress on Thrombosis International Society on Thrombosis and Haemostasis American College of Chest Physicians American College of Cardiology American Academy of Orthopedic Surgeons European Orthopaedic Research Society European Federation of National Associations of Orthopaedics and Traumatology European Hematology Society British Society of Haematology.
Handsearching was also performed by reviewing the bibliographies of included studies and previously published systematic reviews identified through the database search. Prespecified inclusion and exclusion criteria for the systematic review are shown in Table 1
.
Summary of Inclusion and Exclusion Criteria for the Systematic Review
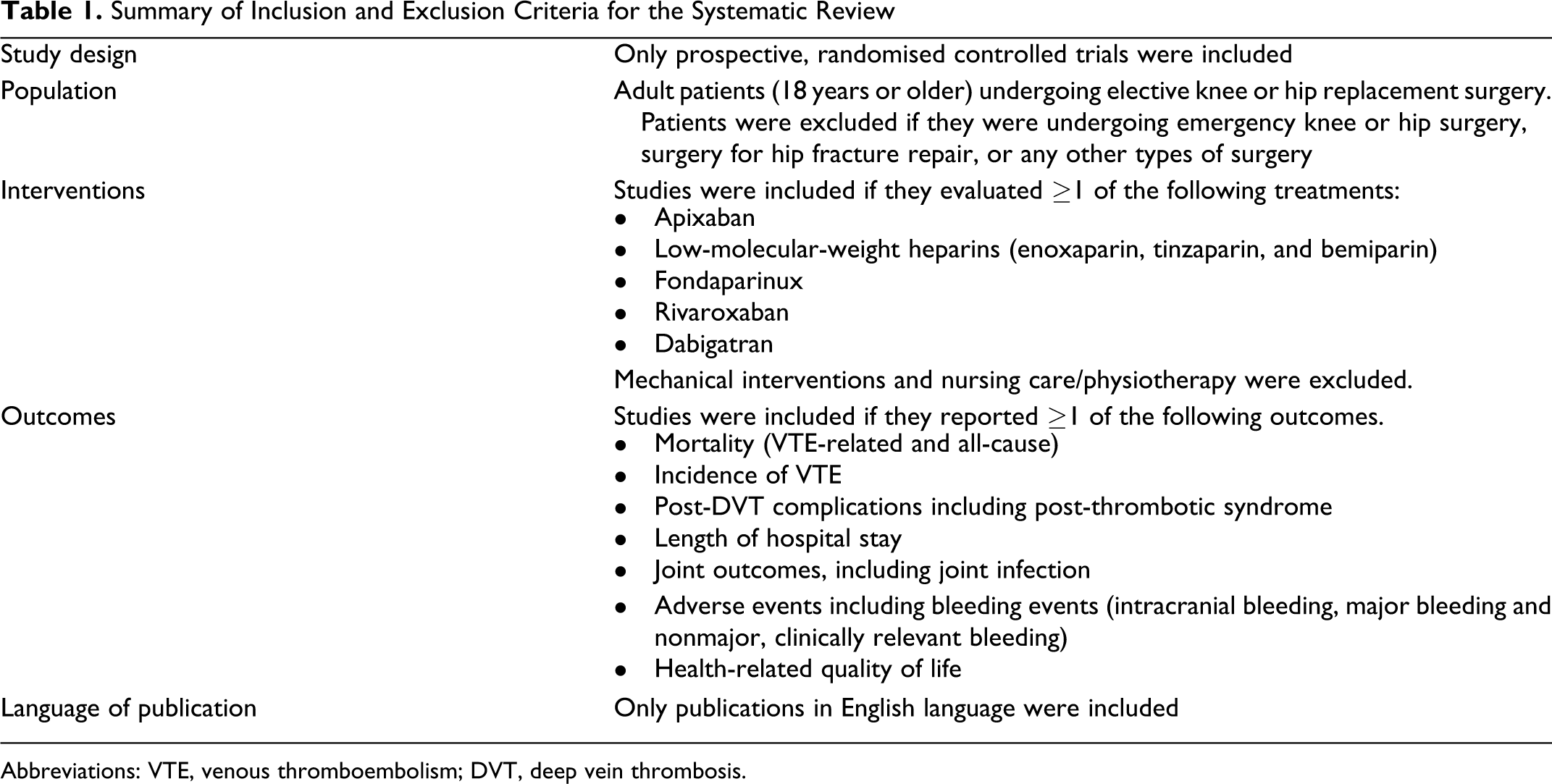
Abbreviations: VTE, venous thromboembolism; DVT, deep vein thrombosis.
Identified studies were independently assessed by 2 reviewers in order to ascertain that they met the predefined inclusion/exclusion criteria and any discrepancies were resolved by a third party. Relevant information was extracted into a predefined document by a reviewer. A second reviewer checked the data extraction, and any inconsistencies were resolved through discussion.
Evaluation of Outcomes
The outcomes considered in the meta-analyses and corresponding definitions are summarized in Table 2 . This manuscript focuses on the primary efficacy outcomes of VTE composite and major VTE, and the primary safety outcomes of major bleeding, clinically relevant nonmajor (CRNM) bleeding, and any bleeding. Results from the analyses of the other outcomes are available as Supplement Data.
Outcomes of Interest for Meta-Analysis
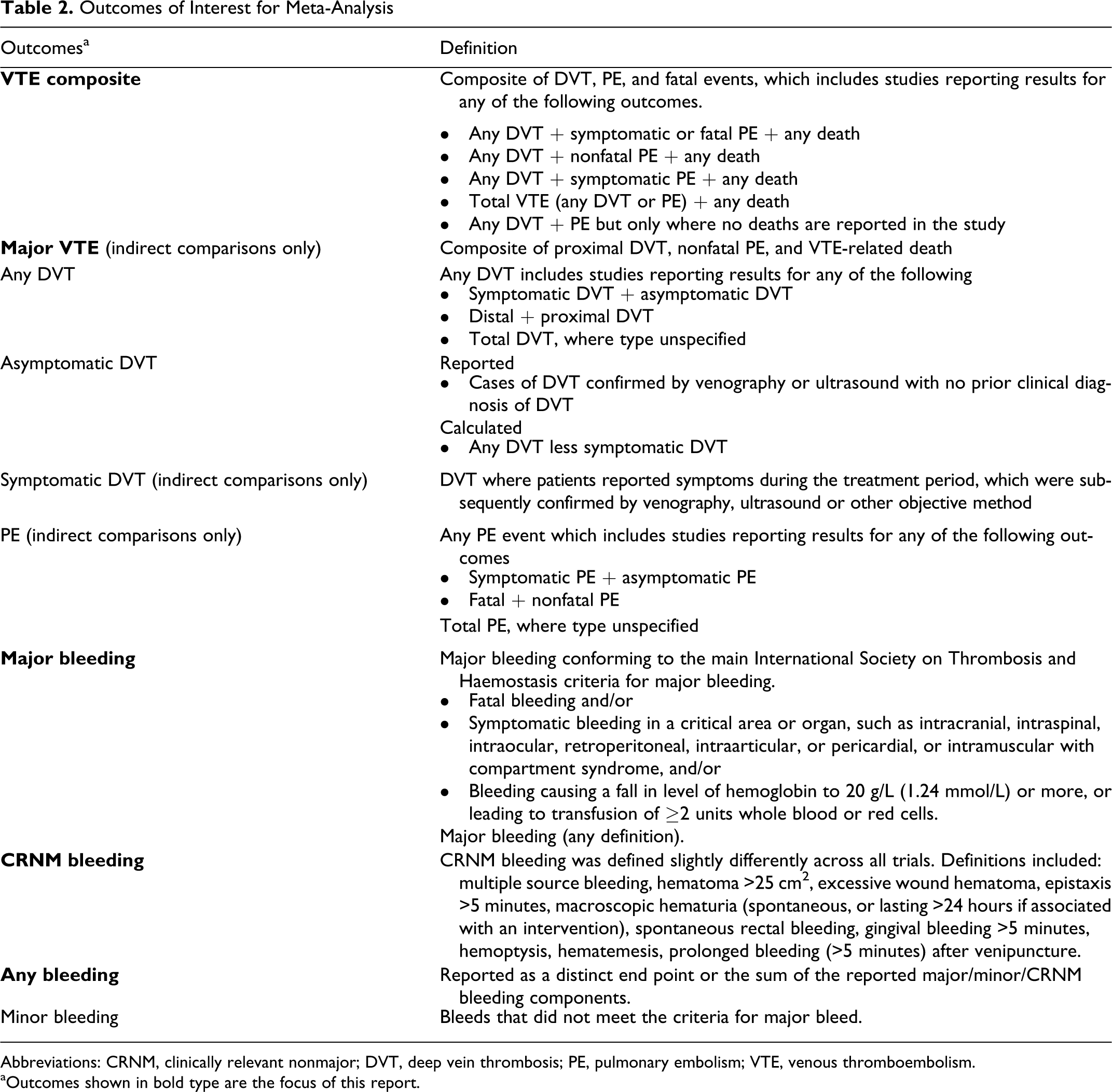
Abbreviations: CRNM, clinically relevant nonmajor; DVT, deep vein thrombosis; PE, pulmonary embolism; VTE, venous thromboembolism.
aOutcomes shown in bold type are the focus of this report.
Statistical Methods for Meta-Analysis
It was decided a priori to conduct the following meta-analyses, where there were sufficient data for analysis. Both THR and TKR patient populations were analyzed separately. A series of direct comparisons of head-to-head RCT data for the treatments of interest A series of adjusted indirect comparisons to derive efficacy and safety effect sizes for apixaban versus the other anticoagulant treatments of interest, where head-to-head data were not available An NMA allowed all evidence from both direct (head-to-head RCTs) and indirect (calculated from trials with common comparators) analyses to be evaluated. The NMA method allows the relative efficacy of several different treatments to be estimated by evaluating the entire network of RCT evidence.
15
–18
Treatments were grouped according to European licensed dose of launched products or doses in clinical development; other doses were included in the network if they contributed to the evidence for the treatment of interest. In addition, it was noted that the duration of treatment in some trials was longer than that indicated in Europe. Therefore, wherever feasible, the treatments of interest were separated into 3 prophylaxis groups: duration as European indication, extended prophylaxis where extension was less than 1 week, and extended prophylaxis where extension was 1 week or more. The reference treatment in the analyses was the treatment evaluated in the largest number of RCTs for the outcome measure considered; this was either enoxaparin 40 mg once daily (European licensed dose) or enoxaparin 30 mg twice daily (US licensed dose).
All the key outcomes of interest were measured using a dichotomous variable. The analyses were conducted on an intent-to-treat (ITT) basis for the outcomes of bleeding. However, since asymptomatic DVT can only be detected via an evaluable venogram, the evaluable population (those individuals with an evaluable venogram) was used in all analyses that included asymptomatic DVT (any DVT, asymptomatic DVT, major VTE, and VTE composite). The ITT analyses for these outcomes were conducted as sensitivity analyses (data not presented, available from the authors on request).
Wherever a direct meta-analysis was possible, this was conducted in Stata IC version 10.1 using the metan package SJ9_2: sbe24_3. 19,20 Results were expressed as odds ratios (ORs) and pooled using the DerSimonian and Laird random-effects method, which takes account of between-study variance. The estimate of heterogeneity was via the Mantel-Haenszel model.
The indirect comparisons between apixaban and other treatments of interest via a common comparator were made using the Bucher method 21 and the pooled ORs produced from the direct meta-analysis. This method preserves randomization of treatments being compared indirectly.
The (indirect) OR between apixaban and the treatment of interest is given by

For the direct and indirect comparisons, 2 analyses were conducted for rivaroxaban 10 mg once daily in the THR patient population, one including and one excluding the RECORD 2 study. RECORD 2 compared rivaroxaban 10 mg once daily with enoxaparin 40 mg once daily; however, enoxaparin was administered for only 10 to 14 days compared with 31 to 39 days of rivaroxaban. The shorter period of enoxaparin treatment, half that recommended in the National Institute of Health and Clinical Excellence (NICE) VTE guideline, 4 could lead to an overestimation of the treatment effect for rivaroxaban. Consequently, the 2 analyses were conducted in order to assess the variation in treatment effect contributed by this study.
Results
Systematic Review Results
A total of 1809 publications were identified through electronic searches and a further 4 through handsearching and manufacturer databases. Following assessment and exclusion of studies based on title, abstract, and full text, 40 records, reporting on 43 RCTs, were included in the final data set for the NMA (Figure 1 ).
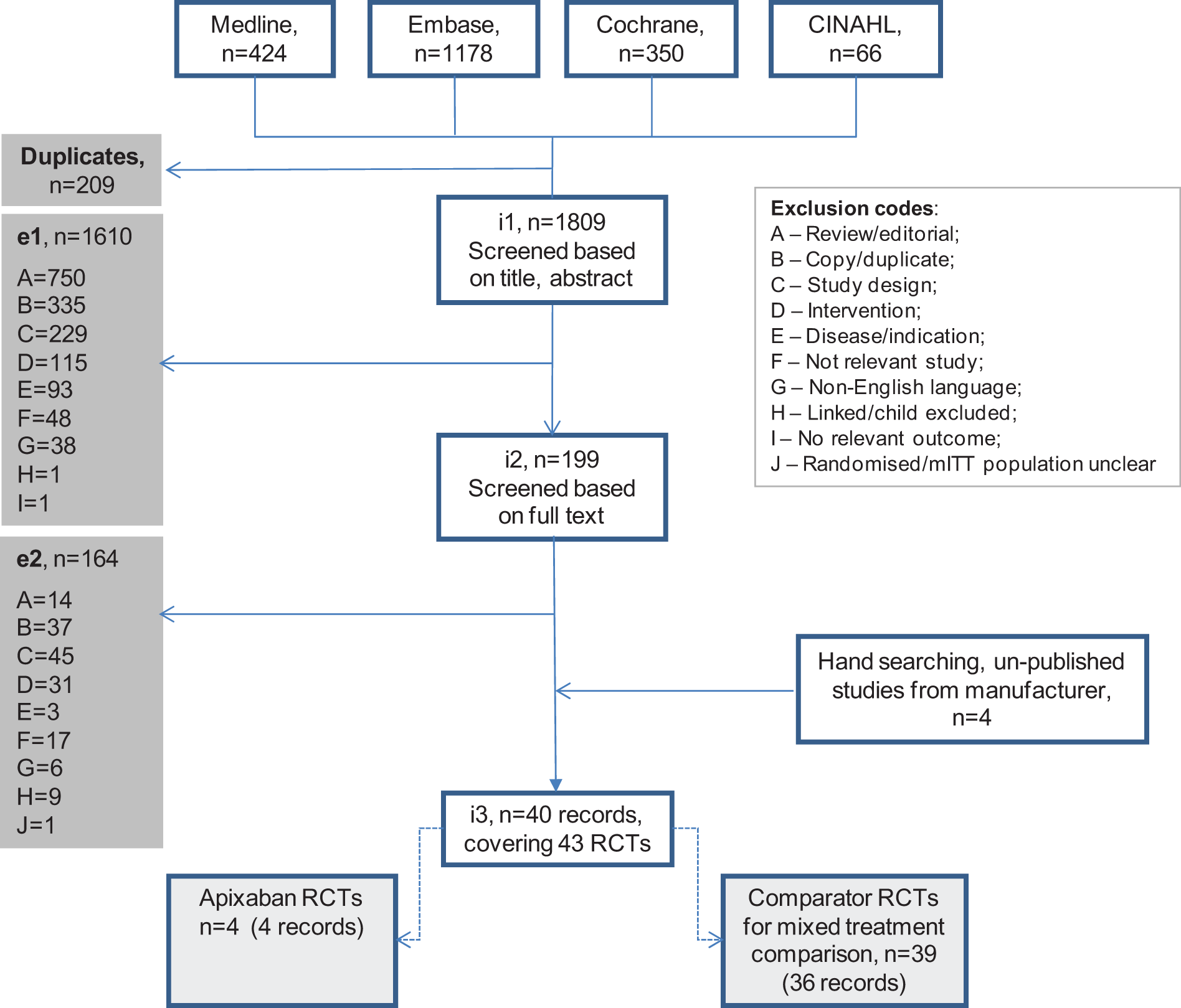
Schematic representation for the systematic review of RCT evidence. Studies identified (i1) were initially assessed based on title and abstract. Articles not meeting the inclusion criteria were excluded (e1) and allocated a “reason code” to document the rationale for exclusion. Articles included after this stage (i2) were then assessed based on the full text; further articles were excluded (e2), yielding the final data set for inclusion (i3). CINAHL indicates cumulative index to nursing and allied health literature; mITT, modified intention-to-treat; RCT, randomized controlled trial.
Of the 43 studies identified in the final NMA data set, 25 did not compare the European licensed dose of the drug of interest with enoxaparin 40 mg once daily or enoxaparin 30 mg twice daily and were excluded from the direct/indirect meta-analyses.
Table 3 lists the studies identified by the systematic review, the interventions evaluated, and the outcomes evaluated in the TKR and THR patient populations. All the studies were included in the NMA, and highlighted studies were included in the indirect comparison.
Studies Identified by the Systematic Review and Considered for the NMA (All Studies) and Indirect Comparison (Shaded), Where Interventions and Outcomes Are Evaluated
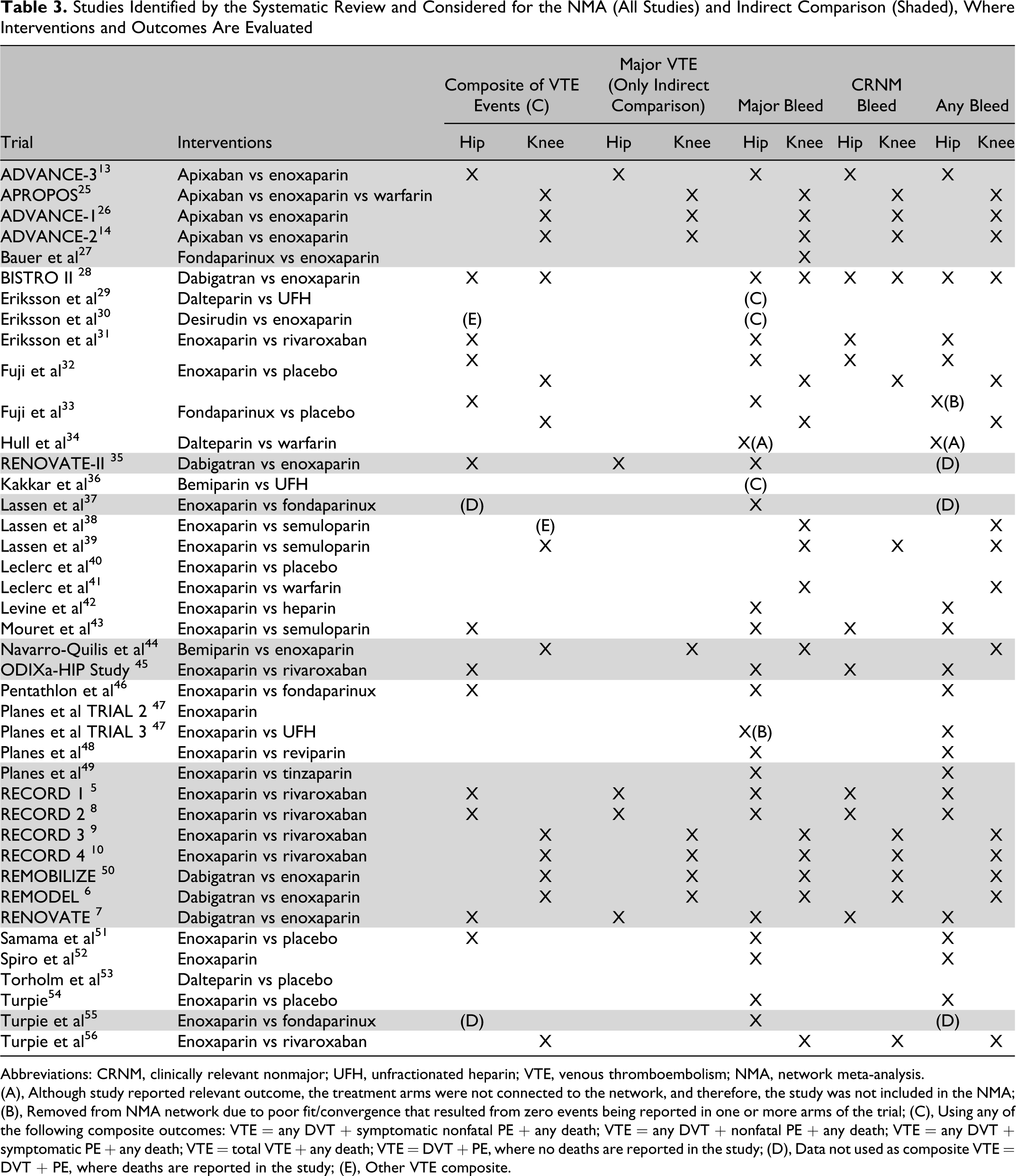
Abbreviations: CRNM, clinically relevant nonmajor; UFH, unfractionated heparin; VTE, venous thromboembolism; NMA, network meta-analysis.
(A), Although study reported relevant outcome, the treatment arms were not connected to the network, and therefore, the study was not included in the NMA; (B), Removed from NMA network due to poor fit/convergence that resulted from zero events being reported in one or more arms of the trial; (C), Using any of the following composite outcomes: VTE = any DVT + symptomatic nonfatal PE + any death; VTE = any DVT + nonfatal PE + any death; VTE = any DVT + symptomatic PE + any death; VTE = total VTE + any death; VTE = DVT + PE, where no deaths are reported in the study; (D), Data not used as composite VTE = DVT + PE, where deaths are reported in the study; (E), Other VTE composite.
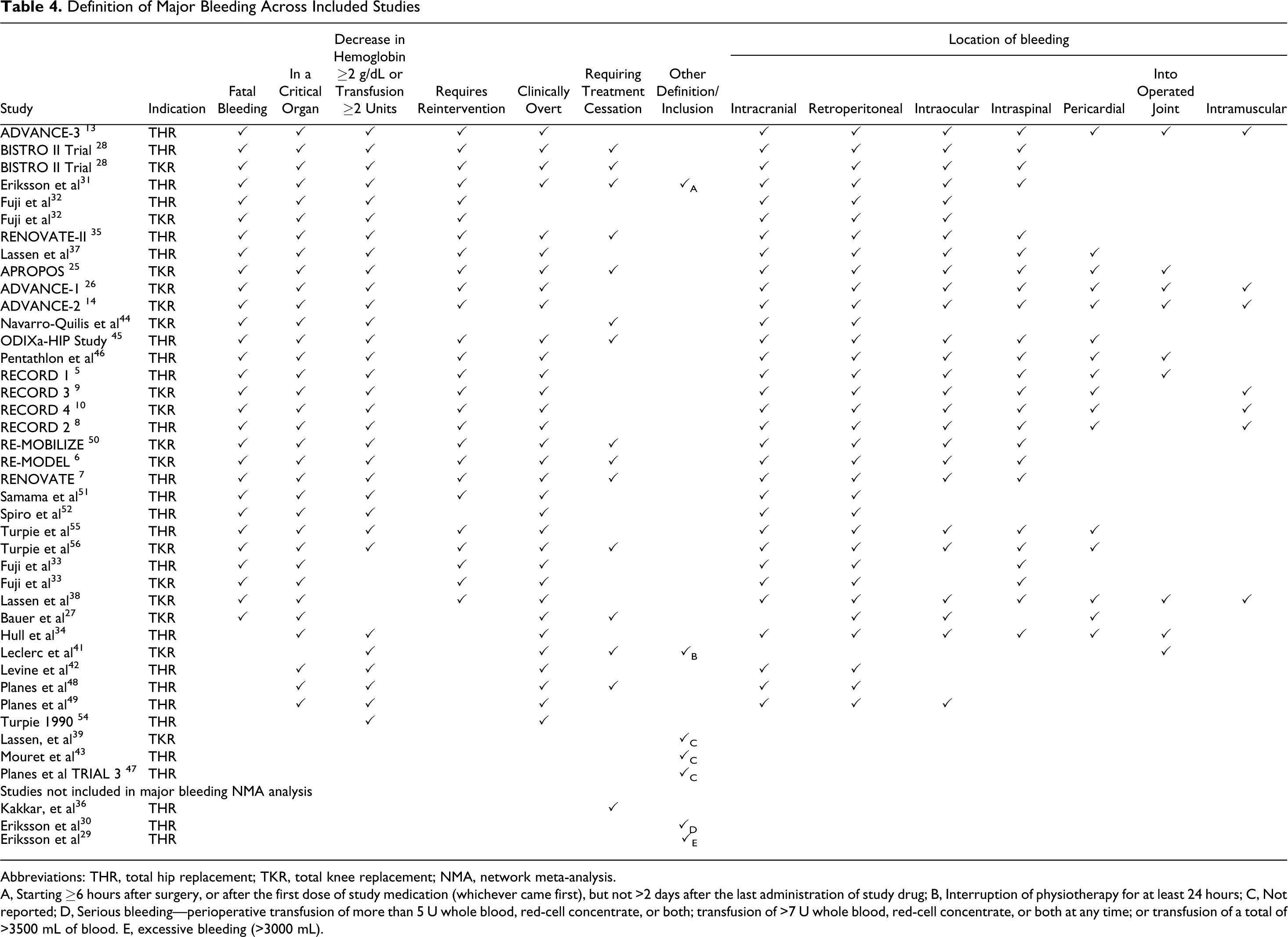
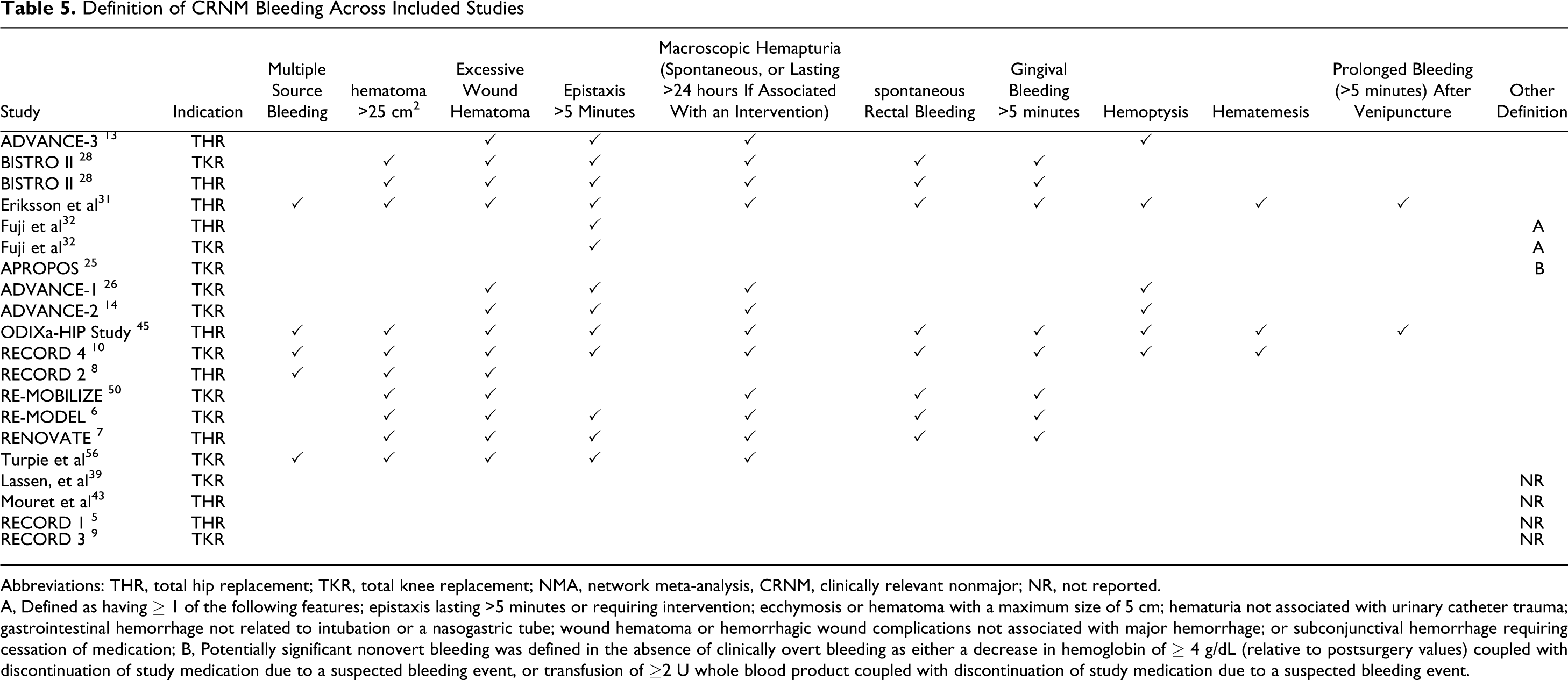
The definition of major bleeding varied across studies (Table 4 ). Twenty-two studies reported a comparable major bleeding outcome in the THR patient population and 16 studies in the TKR patient population. All other studies did not report a major bleeding outcome. There was a slight variation in the definition of CRNM bleeding across studies (Table 5 ). Nine studies in the THR patient population and 11 in the TKR patient population reported a comparable CRNM bleeding outcome. Any bleeding was not reported as a distinct end point in all studies, therefore for these studies, the any bleeding end point used the reported major/minor/CRNM end points. If CRNM bleeding was reported as a distinct category of bleeding from minor bleeding, then major, minor, and CRNM bleeds were totaled, otherwise major and minor bleeds were totaled (a summary of the “any bleeding” definition is available as an online Supplement).
Definition of Major Bleeding Across Included Studies
Abbreviations: THR, total hip replacement; TKR, total knee replacement; NMA, network meta-analysis.
A, Starting ≥6 hours after surgery, or after the first dose of study medication (whichever came first), but not >2 days after the last administration of study drug; B, Interruption of physiotherapy for at least 24 hours; C, Not reported; D, Serious bleeding—perioperative transfusion of more than 5 U whole blood, red-cell concentrate, or both; transfusion of >7 U whole blood, red-cell concentrate, or both at any time; or transfusion of a total of >3500 mL of blood. E, excessive bleeding (>3000 mL).
Definition of CRNM Bleeding Across Included Studies
Abbreviations: THR, total hip replacement; TKR, total knee replacement; NMA, network meta-analysis, CRNM, clinically relevant nonmajor; NR, not reported.
A, Defined as having ≥ 1 of the following features; epistaxis lasting >5 minutes or requiring intervention; ecchymosis or hematoma with a maximum size of 5 cm; hematuria not associated with urinary catheter trauma; gastrointestinal hemorrhage not related to intubation or a nasogastric tube; wound hematoma or hemorrhagic wound complications not associated with major hemorrhage; or subconjunctival hemorrhage requiring cessation of medication; B, Potentially significant nonovert bleeding was defined in the absence of clinically overt bleeding as either a decrease in hemoglobin of ≥ 4 g/dL (relative to postsurgery values) coupled with discontinuation of study medication due to a suspected bleeding event, or transfusion of ≥2 U whole blood product coupled with discontinuation of study medication due to a suspected bleeding event.
Data used in the meta-analyses are available as an online supplement.
Direct/Indirect Comparison Results
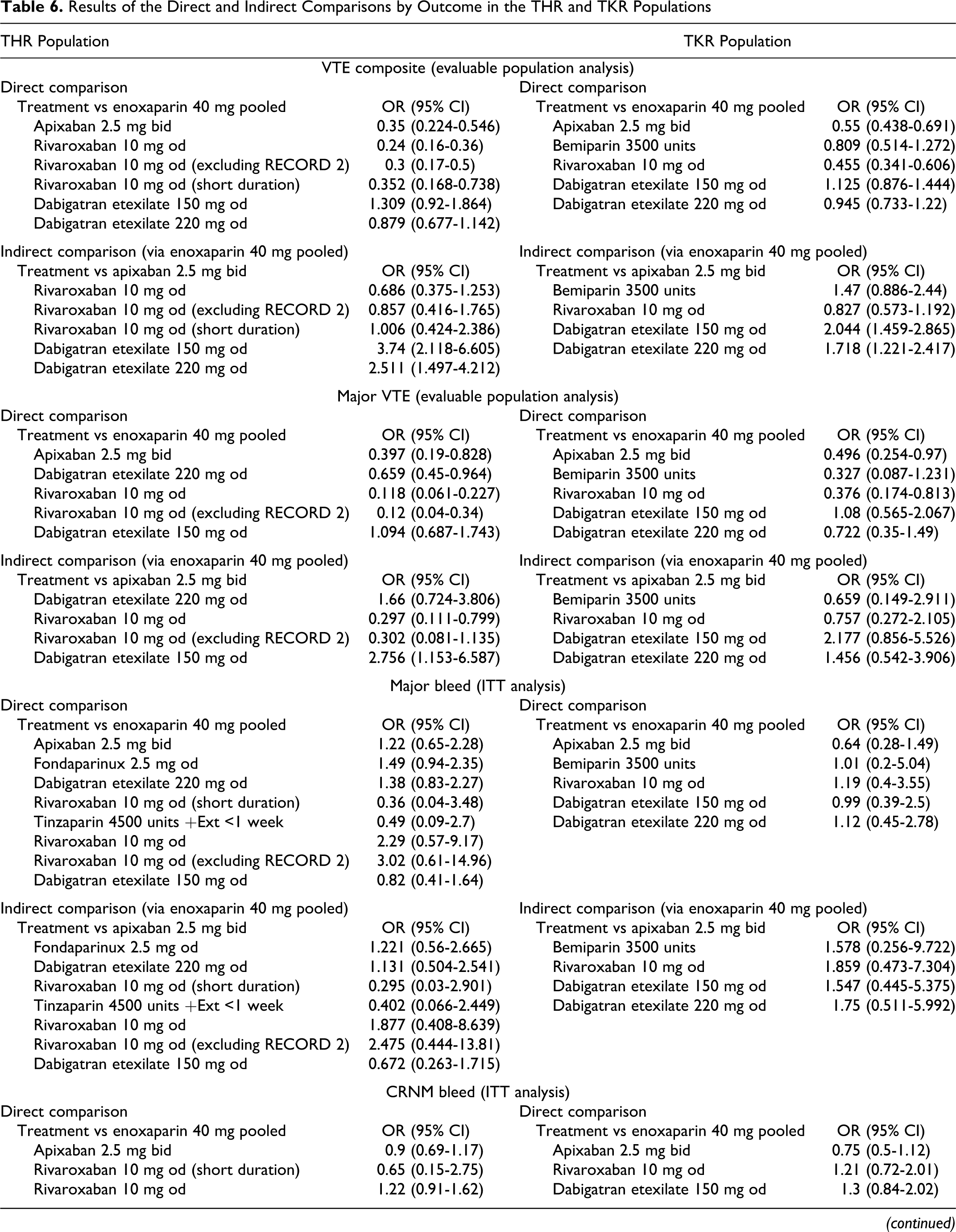
Results of the direct/indirect comparisons are summarized in Table 6 .
Results of the Direct and Indirect Comparisons by Outcome in the THR and TKR Populations
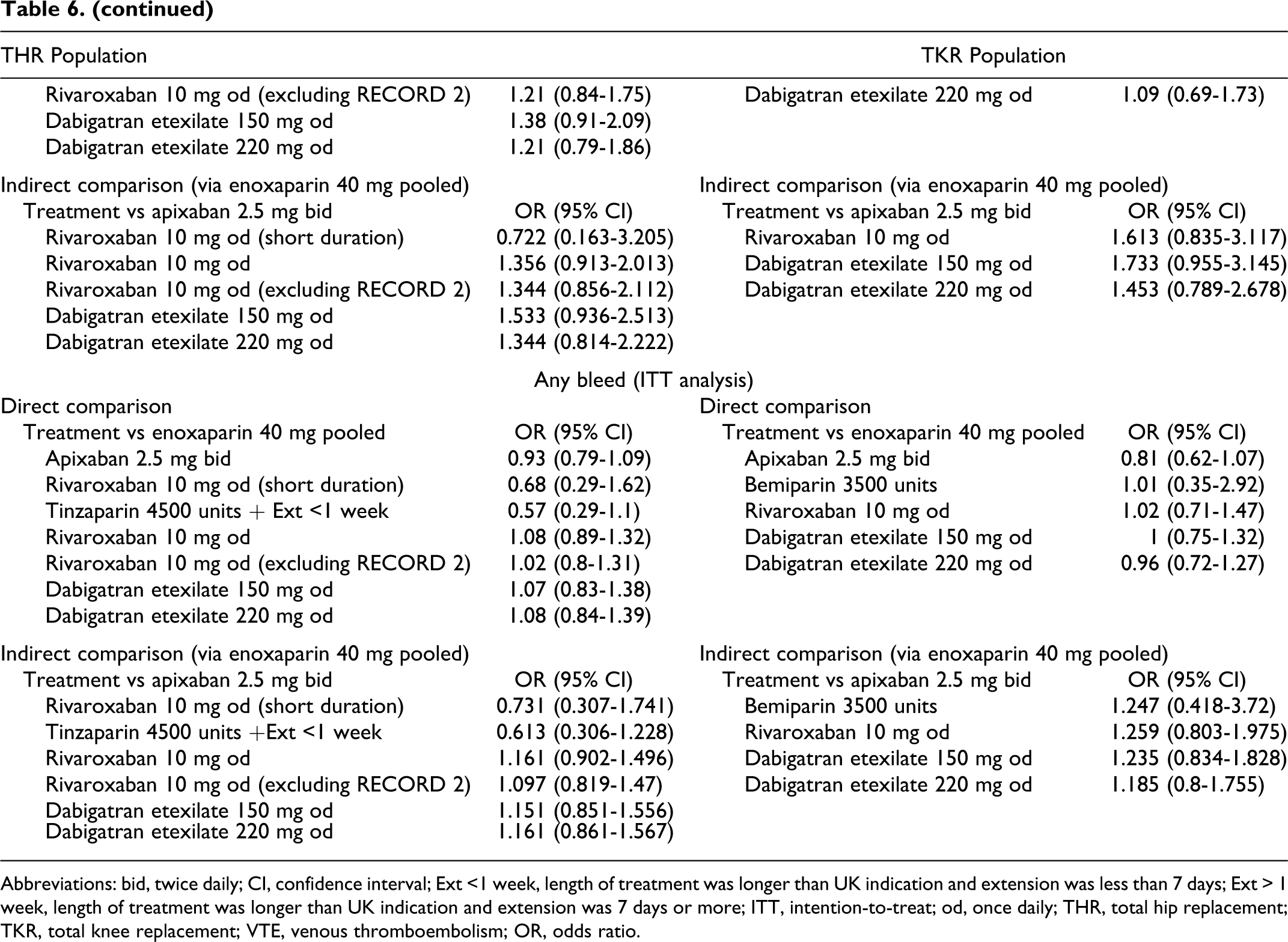
Abbreviations: bid, twice daily; CI, confidence interval; Ext <1 week, length of treatment was longer than UK indication and extension was less than 7 days; Ext > 1 week, length of treatment was longer than UK indication and extension was 7 days or more; ITT, intention-to-treat; od, once daily; THR, total hip replacement; TKR, total knee replacement; VTE, venous thromboembolism; OR, odds ratio.
All VTE and All-Cause Death
Results are shown in Table 6 and Figure 2 . In direct comparisons, apixaban 2.5 mg twice daily was significantly better than enoxaparin 40 mg once daily for the prevention of the primary efficacy outcome “all VTE and all-cause death,” in both patients with THR (OR, 0.35; 95% confidence interval [CI], 0.224-0.546) and TKR (OR, 0.55; 95% CI, 0.438-0.691). Similarly, rivaroxaban 10 mg once daily was superior to enoxaparin for the prevention of all VTE and all-cause death for both THR surgery (OR, 0.24; 95% CI, 0.16-0.36) and TKR surgery (OR, 0.455; 95% CI, 0.341-0.606). Dabigatran etexilate 220 mg once daily showed similar efficacy to enoxaparin 40 mg once daily for this outcome for the THR (OR, 0.879; 95% CI, 0.677-1.142) and TKR (OR, 0.945; 95% CI, 0.733-1.22) patient populations.
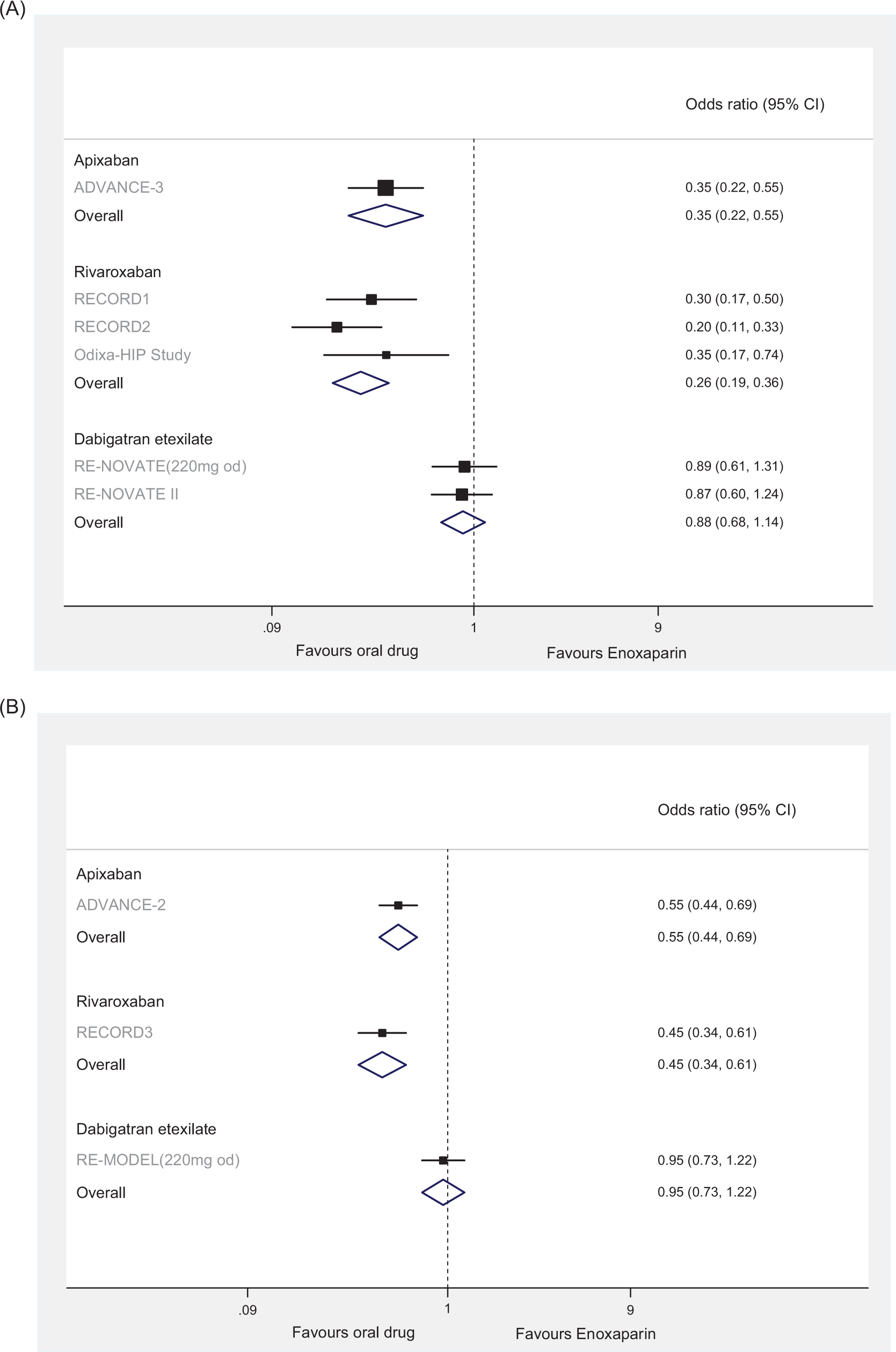
Pooled estimates of the results of randomized controlled trials comparing the effects of apixaban, rivaroxaban, and dabigatran versus enoxaparin on venous thromboembolism (VTE) composite outcome for patients undergoing (A) total hip replacement and (B) total knee replacement.
The adjusted indirect comparison found that apixaban 2.5 mg twice daily was significantly better than dabigatran 220 mg once daily for the prevention of all VTE and all-cause death in patients with THR (OR dabigatran vs apixaban, 2.511; 95% CI, 1.497-4.212), and TKR (OR dabigatran vs apixaban, 1.718; 95% CI, 1.221-2.417). Rivaroxaban 10 mg once daily showed similar efficacy to apixaban 2.5 mg twice daily in both the patients with THR and TKR (OR, 0.686; 95% CI, 0.375-1.253 and OR, 0.827; 95% CI, 0.573-1.192, respectively).
Major VTE
Direct ORs (Table 6 ) suggest that apixaban 2.5 mg once daily (THR and TKR patient populations), dabigatran etexilate 220 mg once daily (THR patient population), and rivaroxaban 10 mg once daily (THR and TKR patient populations) are superior to enoxaparin 40 mg for the prevention of major VTE; and that bemiparin 3500 units (TKR patient population) has similar efficacy.
The adjusted indirect comparison suggested that rivaroxaban 10 mg once daily was superior to apixaban 2.5 mg once daily for the prevention of major VTE in the THR patient population (OR, 0.297; 95% CI, 0.111-0.799); however, on removal of the RECORD 2 study, this difference was not significant (OR, 0.302; 95% CI, 0.081-1.135). Apixaban 2.5 mg once daily was similar to dabigatran etexilate 220 mg once daily (THR and TKR patient populations), rivaroxaban 10 mg once daily (TKR patient population), and bemiparin 3500 units (TKR patient population) for this outcome.
Outcomes of Bleeding
For all outcomes of bleeding (major bleed, CRNM bleed, and any bleed), no significant differences between the treatments evaluated were observed in direct and indirect comparisons in either THR or TKR patient populations (Table 6 and Figure 3 ).
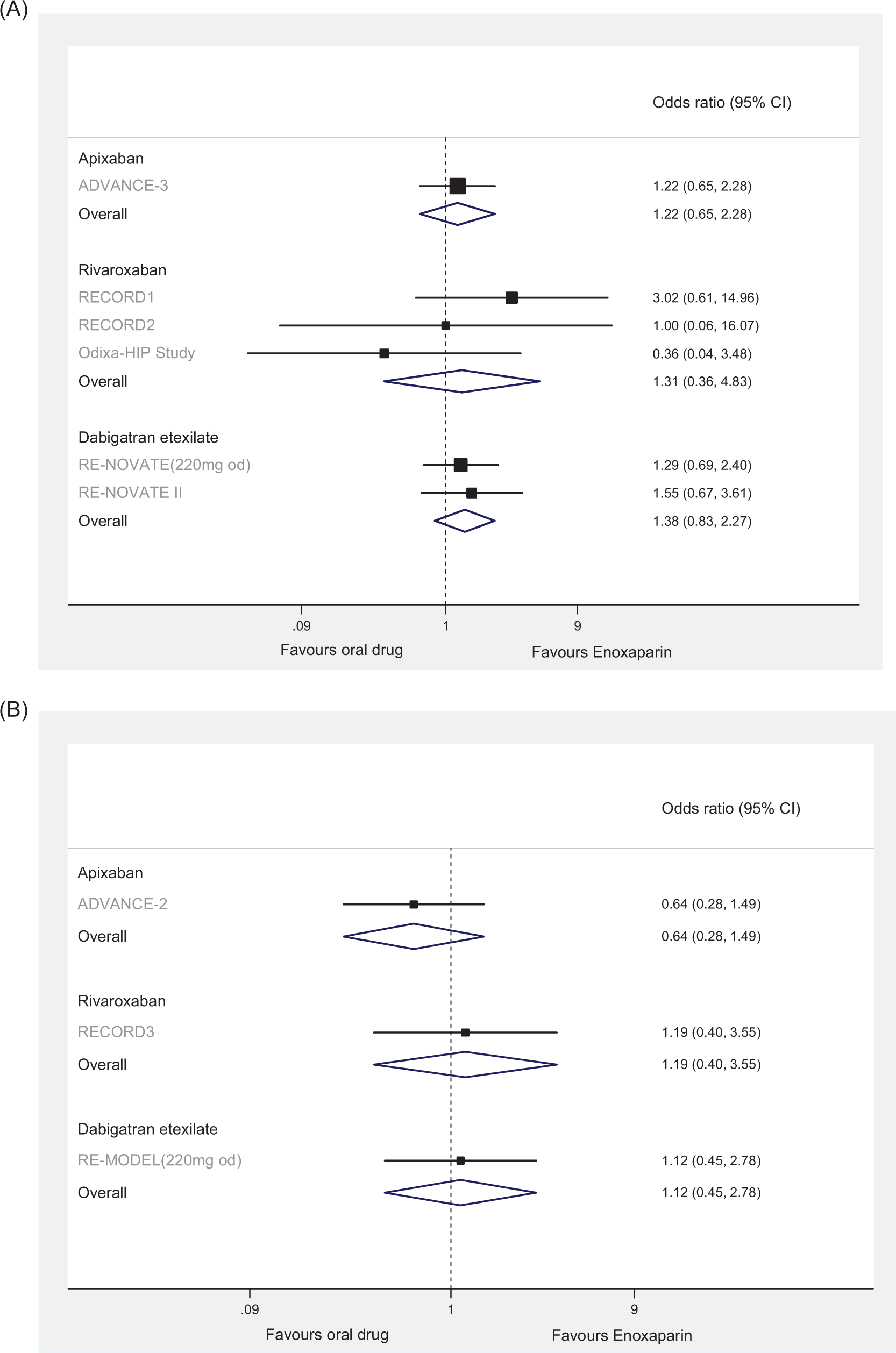
Pooled estimates of the results of randomized controlled trials comparing the effects of apixaban, rivaroxaban, and dabigatran versus enoxaparin on major bleeding for patients undergoing (A) total hip replacement and (B) total knee replacement.
Results of NMA
Results of the NMA are summarized in Table 7 . An example of the network of evidence for the VTE composite outcome in THR surgery is shown in Figure 4 . Due to the small number of studies reporting major VTE, an NMA was not possible for this outcome. In general, for all outcomes, there were few significant differences reported between the treatments. The wide credibility intervals were in contrast to the narrower CIs observed in the adjusted indirect comparisons for the same outcomes. The NMA results for apixaban 2.5 mg twice daily versus dabigatran 220 mg once daily for the VTE composite outcome were not in agreement with those observed in the adjusted indirect comparison. Furthermore, for the primary efficacy outcome, all VTE and all-cause death, the NMA results of apixaban 2.5 mg twice daily versus enoxaparin 40 mg once daily and rivaroxaban 10 mg once daily versus enoxaparin 40 mg once daily were inconsistent with the direct head-to-head RCT comparisons of these treatments.
Results From the NMA Base Model in the THR and TKR Populations
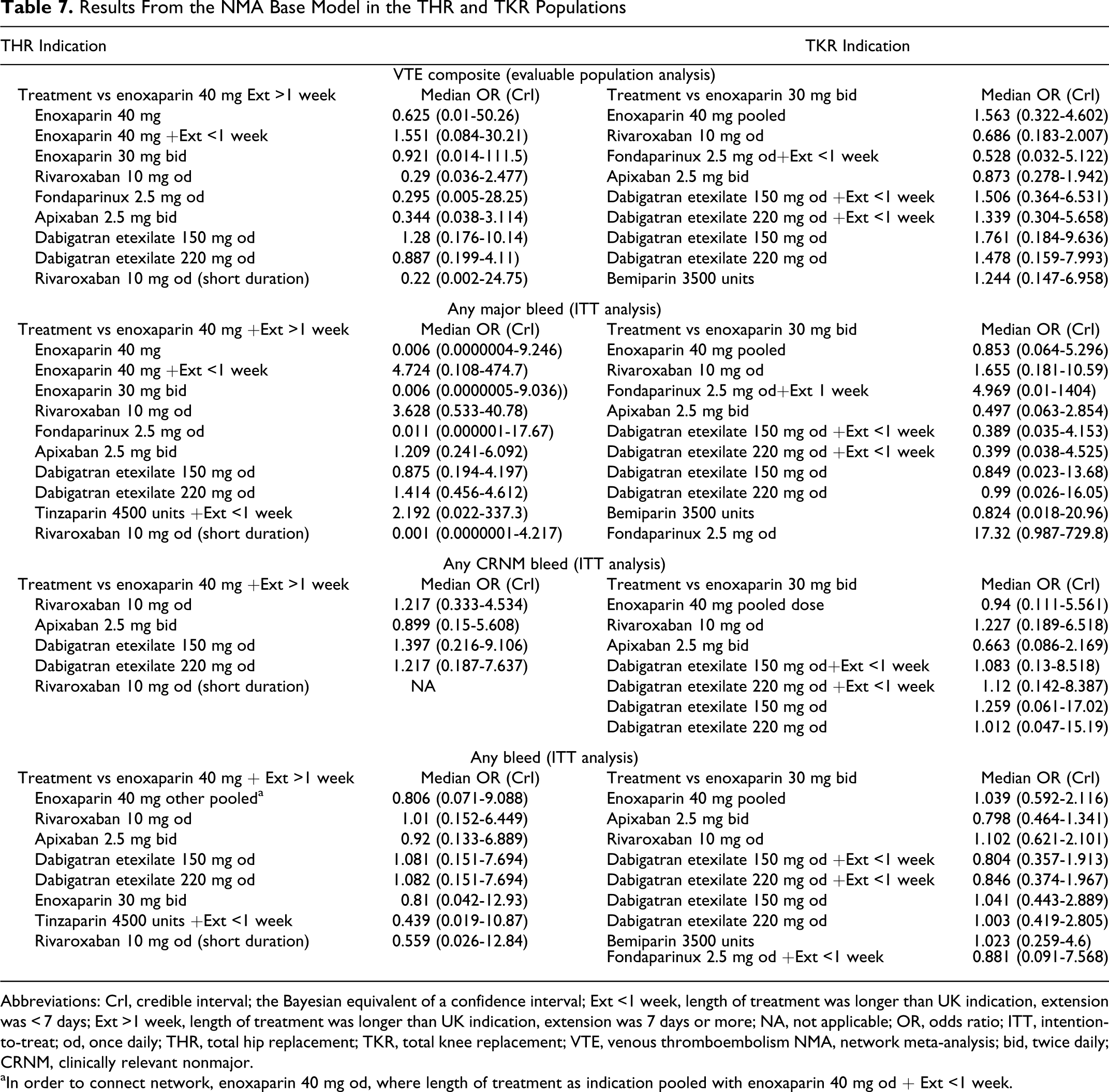
Abbreviations: CrI, credible interval; the Bayesian equivalent of a confidence interval; Ext <1 week, length of treatment was longer than UK indication, extension was < 7 days; Ext >1 week, length of treatment was longer than UK indication, extension was 7 days or more; NA, not applicable; OR, odds ratio; ITT, intention-to-treat; od, once daily; THR, total hip replacement; TKR, total knee replacement; VTE, venous thromboembolism NMA, network meta-analysis; bid, twice daily; CRNM, clinically relevant nonmajor.
aIn order to connect network, enoxaparin 40 mg od, where length of treatment as indication pooled with enoxaparin 40 mg od + Ext <1 week.
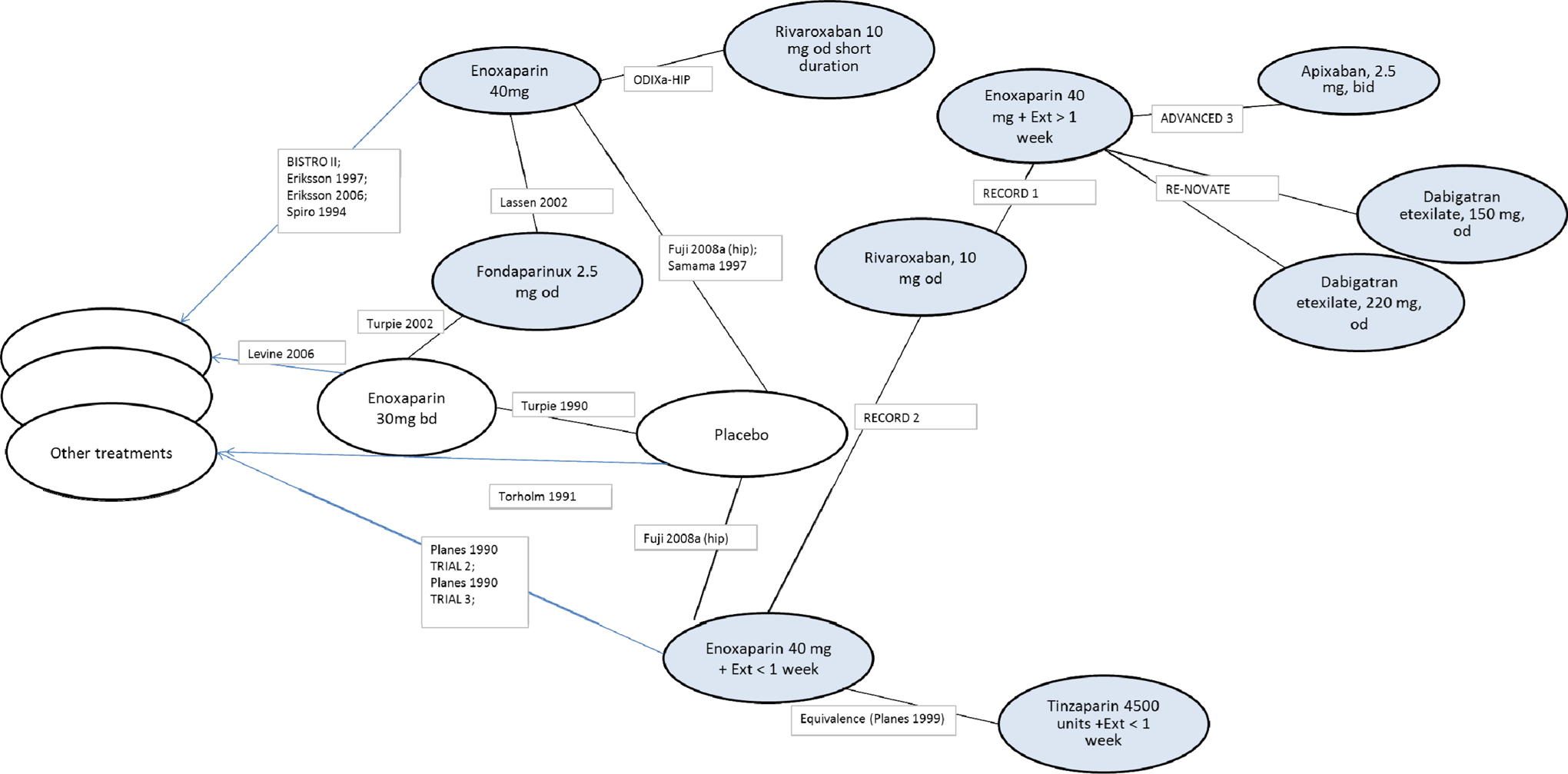
Network diagram for venous thromboembolism (VTE) composite outcome in the hip indication.
Discussion
In the absence of head-to-head RCT evidence for the new oral anticoagulants apixaban, rivaroxaban, and dabigatran, an adjusted indirect comparison with enoxaparin 40 mg once daily as the common comparator and an NMA were conducted to determine efficacy and safety effect sizes for these treatments.
The adjusted indirect comparison found that in both the THR and TKR patient populations, apixaban was superior to dabigatran etexilate and similar to rivaroxaban for the prevention of the primary efficacy outcome all VTE and all-cause death (Table 6 ). Apixaban was similar to dabigatran and rivaroxaban for the prevention of major VTE, in both THR and TKR patient populations.
The incidence of PE events was similar for apixaban, dabigatran etexilate, and rivaroxaban; however, the number of PE events across all the treatments was small (data shown in online Supplement Appendix).
The incidence of all bleeding events (minor, major, and CRNM) was comparable for apixaban, rivaroxaban, and dabigatran etexilate, in both THR and TKR patient populations. In the THR patient population, apixaban and fondaparinux had a similar incidence of major bleeding.
The results from the NMA and the adjusted indirect comparison were inconsistent for some treatment comparisons. Wide credibility intervals around treatment differences for some outcomes were observed in the NMA, which may have been due to the large number of trials contributing to the enoxaparin 40 mg once daily node within the NMA network. The NMA allows for more sources of uncertainty, which explains in part the wider credibility intervals. Some of the trials included in the NMA were of lower quality than the recent apixaban, rivaroxaban, dabigatran, and fondaparinux RCTs included in the main pairwise meta-analyses and adjusted indirect comparisons, with fewer study quality criteria reported. Many had fewer than 100 patients per treatment arm, and many compared enoxaparin 40 mg once daily against treatments not meeting the defined criteria of this review. All these factors could have contributed to a lack of precision and an increase in uncertainty in the relative treatment effects for enoxaparin 40 mg once daily observed in the NMA results, despite the apparent increase in power (ie, more eligible studies) afforded by the NMA study inclusion criteria.
In contrast, the adjusted indirect comparison approach, although restricting the number of studies for inclusion to those possessing a common comparator (ie, enoxaparin 40 mg once daily), may allow for more precision in the relative treatment effect estimates of interest. This is because included studies tended to report and fulfill more study quality criteria, have larger patient numbers (all in excess of 600 patients randomized per arm), and report similar outcome definitions and measures. However, it should be noted that some outcome definitions were inconsistent across included trials, particularly for the outcomes of bleeding (Tables 4 and 5).
The results of the direct and indirect comparisons are consistent with those observed in a recent meta-analysis and adjusted indirect comparison of rivaroxaban and dabigatran for the prevention of VTE. 57 The study found that for the prevention of VTE (for THR and TKR patient populations pooled), rivaroxaban was superior to enoxaparin (relative risk [RR], 0.56; 95% CI, 0.43-0.73, P < .0001), and dabigatran was not superior to enoxaparin (RR, 1.12; 95% CI, 0.97-1.29, P = .12), 57 thus in line with the conclusions of the current study. Adjusted indirect comparison showed that rivaroxaban was superior to dabigatran in preventing VTE; RR, 0.50 (95% CI, 0.37-0.68). 57
NMA and indirect comparison allow the efficacy of interventions to be compared in the absence of head-to-head evidence, which can be invaluable to health care providers, physicians, and patients for decision making when a number of new effective interventions are available. A limitation of meta-analysis is the underlying assumption that trials and outcomes are sufficiently similar to allow for data to be pooled. In particular, it assumes that all the studies relate to the same patient population and that any differences in study design, inclusion criteria, or baseline characteristics will not influence the relative efficacy of the various treatments. 16 In the current analysis, methods for diagnosing DVT and PE and definitions of outcomes of bleeding may not have been comparable between trials (Tables 4 and 5). In addition, trials may have used different follow-up times or patient populations may have differed in the baseline risk of DVT.
In clinical trials, the new oral anticoagulants apixaban, rivaroxaban, and dabigatran etexilate have demonstrated similar or improved efficacy and similar safety compared with current therapies, such as LMWH, for the prevention of VTE in patients undergoing orthopedic surgery. 5-10,13,14,25,26 The adjusted indirect comparison results reported here reflect the observations made in the clinical trials. Results of the adjusted indirect comparison also suggest that apixaban has an efficacy profile that is better than that of dabigatran etexilate and similar to that of rivaroxaban, while all 3 have a comparable safety profile. In addition to improved efficacy compared with current therapies, apixaban, dabigatran etexilate, and rivaroxaban have the advantage of oral administration and do not require routine laboratory monitoring. 58 Apixaban and rivaroxaban have a further benefit of not requiring dose adjustment for moderate or severe renal impairment or patient weight. 59
Considering practical and economic advantages, such as the ease of oral dosing and the substantial reduction in costs related to this, these new anticoagulants represent an appealing alternative to conventional thromboprophylaxis regimens in patients undergoing THR and TKR surgery and may improve patient compliance and standard of care.
Footnotes
Authors– Note
N.M. and D.R. are the employees of Pfizer Ltd. P.D. and T.S. are the employees of Bristol Myers Squibb. A.C., S.M., M.O. and A.S. were paid consultants to Bristol Myers Squibb and Pfizer Inc. in connection with conducting the meta-analysis and development of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: funded by Bristol Myers Squibb and Pfizer Inc.