
Abstract
Venous gangrene is a rare complication of deep venous thrombosis. It is certain from review of literature that there is a significant causative relationship between malignant disease and venous gangrene. Data from the National hospital discharge survey from 1979 to 2006 showed that 0.43% of patients with deep venous thrombosis had gangrene, while 1.39% patients with gangrene had deep venous thrombosis. Toes and fingers are frequent site of venous gangrene in patients with massive deep venous thrombosis, as evident by review of literature. A possible explanation for this occurrence can be the fact that because of the scarcity of subcutaneous fat and the small spaces of fingers and toes, massive edema can generate large compressive forces; these forces may have a compressive effect on the arterioles, which may contribute to the development of venous gangrene. Lower extremities develop venous gangrene more commonly than upper extremities. The condition has an extremely high rate of mortality either from pulmonary embolism or from the serious underlying disease, such as neoplasms.
Introduction
Gangrene of the extremities due to vascular disturbances can almost invariably be ascribed to pure arterial occlusion, mixed arterial and venous occlusion, or venous obstruction alone. 1 Venous gangrene is an unusual and severe form of venous thrombosis of an extremity. 2 In a review article by Haimovici, 1 it was stated that Fabricius Hildanus was the first to recognize the possibility of gangrene of venous origin as early as 1593. In the same article, it was mentioned that it was not until 1859 when a case published by Hueter gave an excellent account of the clinical and pathologic criteria of this type of gangrene. 1 The condition has an extremely high rate of mortality either from pulmonary embolism or from the serious underlying disease, such as neoplasms. 3
Case Report
A 59-year-old male was brought in for painful massive swelling of his right lower extremity and yellow discoloration of the sclera. He had nonsignificant past medical and surgical history. He was an alcoholic and smoker for the past 30 years. Physical examination showed blackish-purple discoloration of his right great, second and third toe. Scleral icterus, shifting dullness, and marked hepatomegaly were other pertinent findings on physical examination. Peripheral pulses were not appreciated in the right leg because of massive swelling. There were blisters seen on the right great toe; the gangrenous-looking toes (Figure 1) were anesthetic but not painful. Patient had intact pressure sensation; proprioception and no necrotic area were seen. Patency of the right common iliac, internal iliac, external iliac, femoral, anterior tibial, tibioperoneal, peroneal, and posterior tibial arteries by duplex arterial ultrasound ruled out arterial occlusion as the cause of gangrene. High-resolution duplex venous ultrasound showed near-complete occlusive thrombus extending from the distal right external iliac vein to the right common femoral vein, right superficial femoral vein, right profunda vein, and right popliteal vein. Abdominal computed tomography showed diffuse pulmonary, hepatic, and bilateral renal metastases. Bilateral lower extremity deep venous thromboses were noted, more extensive on the right, with filling defect and distention of the right external iliac vein (Figure 2) through the common femoral vein, superficial femoral vein, visualized portion of profunda femoris, and greater saphenous vein along with soft-tissue edema. Nonocclusive thrombus was noted in the left lower extremity, extending from left external iliac vein through the common femoral vein, left superficial femoral vein anterior portion of profunda femoris vein. The common iliac and inferior vena cava were grossly noninvolved. Biopsy of the liver mass confirmed, pancreatic adenocarcinoma.

Blackish-purple discoloration of patient’s right great, second and third toe, with blister seen at the base of great toe.
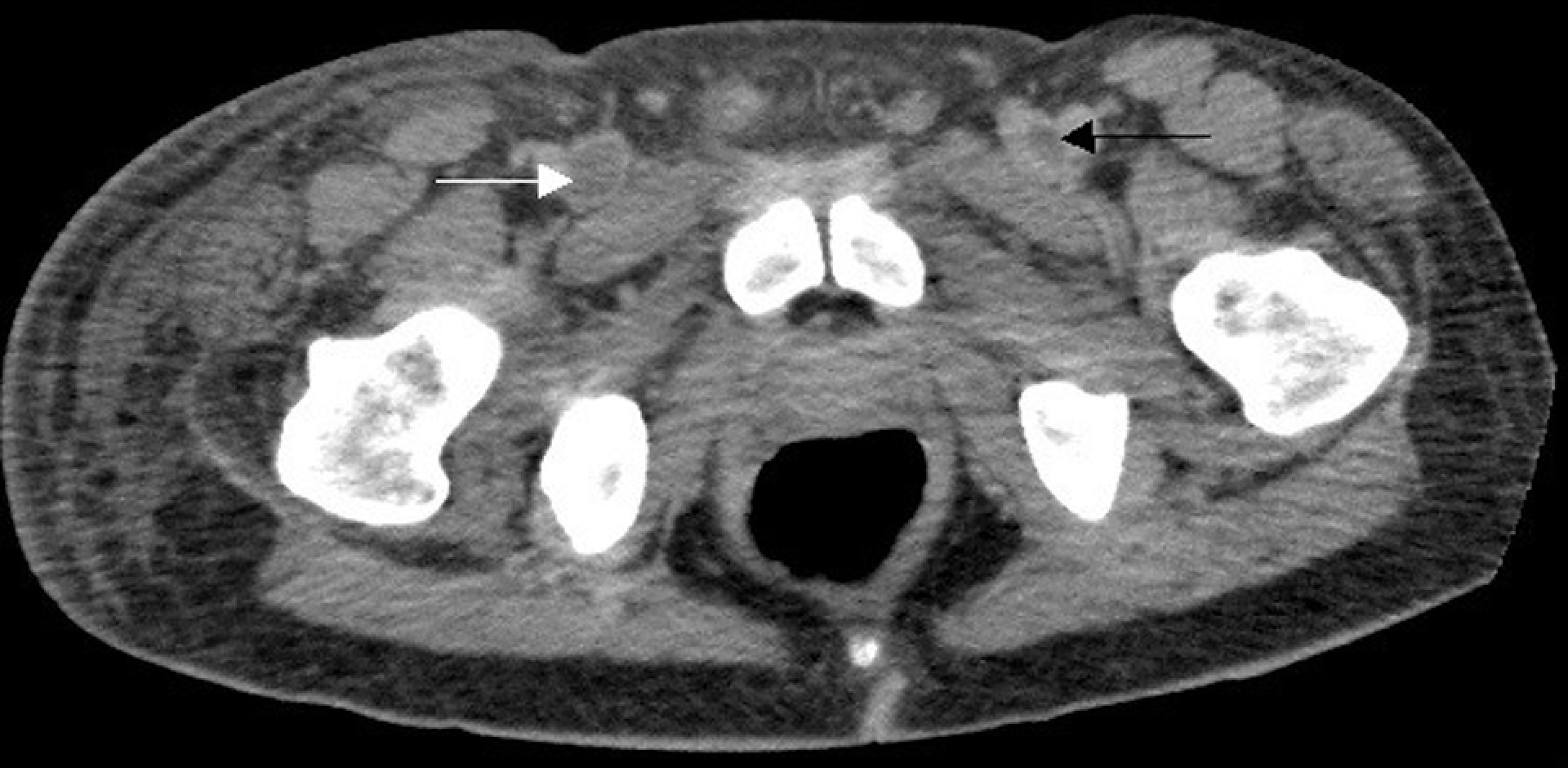
Abdominal computerized tomography (CT) scan showing completely occluded right external iliac vein (white arrow) and partially occluded left external iliac vein (black arrow).
Coagulation profile showed prothrombin time of 13.9 seconds (control 12.5), partial thromboplastin time 51.0 seconds (control 34.1 seconds), and fibrinogen activity of 204 mg/dL. The patient was started on intravenous heparin once the diagnosis of acute deep venous thrombosis was made, along with warfarin. The patient expired 10 days after he was diagnosed with metastatic pancreatic carcinoma. All treatments were withheld and patient was put in hospice care for the last few days.
Discussion
To make diagnoses of gangrene of venous origin, it is necessary to establish the fact that there is thrombophlebitis without arterial occlusion. 1 Manifestations typical for venous gangrene consists of (1) onset usually sudden; (2) cyanosis appearing early, developing rapidly, and extending to the entire extremity; (3) excessive edema of a woody consistency; (4) skin temperature, sometimes conserved, contrasting with the other signs of vascular deficit; and (5) patent peripheral arteries. 1
Cyanosis is one of the characteristic signs. Its maximum intensity is at the distal parts (toes, heels, and fingers). 1 Pain of venous gangrene tends to be more intense than in the common form of thrombophlebitis. 1 Edema, considered as the pathognomonic sign of venous occlusion, may be absent at the inception in some cases. 1 Gangrene is wet and appears to develop slowly in most cases as compared to that from arterial occlusion. 1 Gangrene seen in this condition can be superficial and raises the question of the status of the extremely small arteries and arterioles in the subcutaneous tissue. 1
Phlegmasia cerulea dolens and venous gangrene have an overlapping presentation, 2 and they constitute reversible and irreversible subdivision of ischemic thrombophlebitis, respectively. 4 Before the onset of irreversibility, the extremity is cyanotic. 2 Areas of deep-red discoloration then develop, progressing to purple or black and often accompanied by large bullae filled with dark fluid. 2 As apparent in our case, blistering in the gangrene of lower extremity is most prominent on the toes and dorsum of the foot. 2 At the outset, the gangrenous process appears to involve the skin and the subcutaneous tissues preferentially, only later do myonecrosis and ischemic neuritis develop. 2 Toes and fingers are frequent site of venous gangrene in patients with massive deep venous thrombosis, as evident by review of literature. A possible explanation for this occurrence can be the fact that because of the scarcity of subcutaneous fat and the small spaces of fingers and toes, massive edema can generate large compressive forces; these forces may have a compressive effect on the arterioles, which may contribute to the development of venous gangrene.
In a review article by Haimovici, 388 limbs (321 patients) with ischemic form of venous thrombosis were studied; 51% had venous gangrene, while 49% were thought to have phlegmasia cerulean dolens. 4 Lower extremities more commonly developed venous gangrene (in 89% of the cases) compared to the upper extremities (11%). 4 Neoplasia puts the patients with deep venous thrombosis at a very high risk of developing venous gangrene followed by postpartum state, recurrent thrombophlebitis, and underlying chronic cardiac disease. 4 Though venous gangrene of the upper extremity is a rare occurrence,5,6 early intervention and identification may improve outcome. 5
We looked into the national hospital discharge survey from 1979 to 2006 and it showed that 0.43% of patients with deep venous thrombosis had gangrene at the time of discharge from the hospital. We could not determine whether these patients had arterial occlusion causing gangrene or venous gangrene.
High elevation of leg with regular passive flexion to express the entrapped blood diminishes venous engorgement and allows fresh arterial blood to enter. 7 However, this should not be practiced considering the risk of dislodgement of the clot and causing pulmonary embolism, 8 though the opinion has been changed about patients' need for bed rest after deep venous thrombosis. Treatment with warfarin may contribute to the pathogenesis of cancer-associated venous limb gangrene by leading to severe depletion of protein C while failing to reduce thrombin generation. 9 The current evidence suggests that low-molecular-weight heparin provides promise as a safe and effective measure in the management of venous thromboembolism and gangrene. 10
Venous gangrene is a rare condition despite high incidence of deep venous thrombosis, but watch out for it.