
Abstract
von Willebrand disease (vWD) is classified into partial (type 1), qualitative (type 2), and total deficiency (type 3).The aims of the study were to evaluate prospectively the potency of the DDAVP infusion test together with von Willebrand factor (vWF) ristocetin cofactor (vWF:RCo), vWF antigen (vWF:Ag), factor VIII coagulant activity (FVIII:C), and platelet function analyzer (PFA)-100 to distinguish vWD types. Genetic analysis and multimeric analysis of vWF was not applied. We classified the 112 patients and 47 healthy children phenotypically according to the laboratory test results and bleeding severity score. PFA-100 closure times (CT), FVIII:C, vWF:RCo, vWF:Ag, ristocetin-induced platelet aggregation (RIPA), and the response of FVIII:C and vWF parameters to desmopressin (DDAVP) were used to define types 1, 2, and 3 vWD. Type 1 vWD is mild in 34 cases (vWF:RCo % 40-55), moderate in 29 (vWF:RCo %27-40), severe type 1 vWD or nonclassical type 2 vWD in 12 cases (vWF:RCo % 4-16), and type 2 vWD in 23 cases (vWF:RCo %4-38).The response to DDAVP of vWF parameters is normal in all patients with mild/moderate type 1 vWD, 6 patients with severe type 1 vWD or nonclassical type 2 vWD and 11 patients with type 2 vWD. In conclusion, this study showed that measurement of vWF:RCo, vWF:Ag, FVIII:C, and PFA-100 parameters can differentiate vWD types but not severe type 1 vWD or nonclassical type 2 vWD. In the differentiation of severe type 1 vWD and nonclassical type 2 vWD, DDAVP response may be used.
Introduction
von Willebrand disease (vWD) is the most common inherited bleeding disorder, diagnosed following a clinical and physical review, with personal and familial evidence of (primarily mucocutaneous) bleeding, and characterized by low levels of, or abnormal function in, the plasma protein von Willebrand factor (vWF). 1 In at least 2 large prospective epidemiological studies, up to 1% of a predominantly pediatric population was found to manifest symptoms and laboratory signs of vWD. 2 The heterogenity of the disease manifests both in the clinical symptoms and in the variable laboratory parameters. The severity of bleeding can vary greatly among individuals with this disorder, even for members of the same family.
The most common test of vWF activity, the assay of vWF ristocetin cofactor (vWF:RCo) together with vWF antigen (vWF:Ag) is traditionally considered the first step in the diagnosis of vWD. The platelet function analyzer (PFA-100) may also have a role in the identification of vWD. 3,4 The revised classification scheme for vWD identifies 2 major categories: quantitative or qualitative defects of vWF. Types 1 and 3 are quantitative defects. Type 1 individuals produce low levels of otherwise functionally normal vWF, and vWF is completely absent in type 3 vWD. In contrast, type 2 vWD represents qualitative defects characterized by the presence of dysfunctional vWF, with the particular defect or dysfunction characterized within the subtype (2A, 2B, 2M, and 2N). 5,6 In this study, patients with a positive bleeding history were evaluated according to laboratory tests that are most often used in the diagnosis of vWD to characterize phenotypes and permit their classification. Accordingly, the aims of the study were to evaluate prospectively the potency of the DDAVP infusion test together with vWF:RCo, vWF:Ag, factor VIII coagulant activity (FVIII:C), and PFA-100 to distinguish vWD types in Turkey. Genetic analysis and multimeric analysis of vWF were not applied to patients.
Patients, Materials, and Methods
All patients who were admitted to the outpatient service of the Pediatric Hematology Department of Ege University Faculty of Medicine, with a positive bleeding history underwent a routine blood workup inclusive of hemostasis analysis. Whole blood count, prothrombin time (PT), activated partial thrombin time (APTT), and fibrinogen levels were evaluated in all patients. Patient characteristics are shown in Table 1 .
Patient Characteristics, Demographic, and Bleeding Severity Score Data
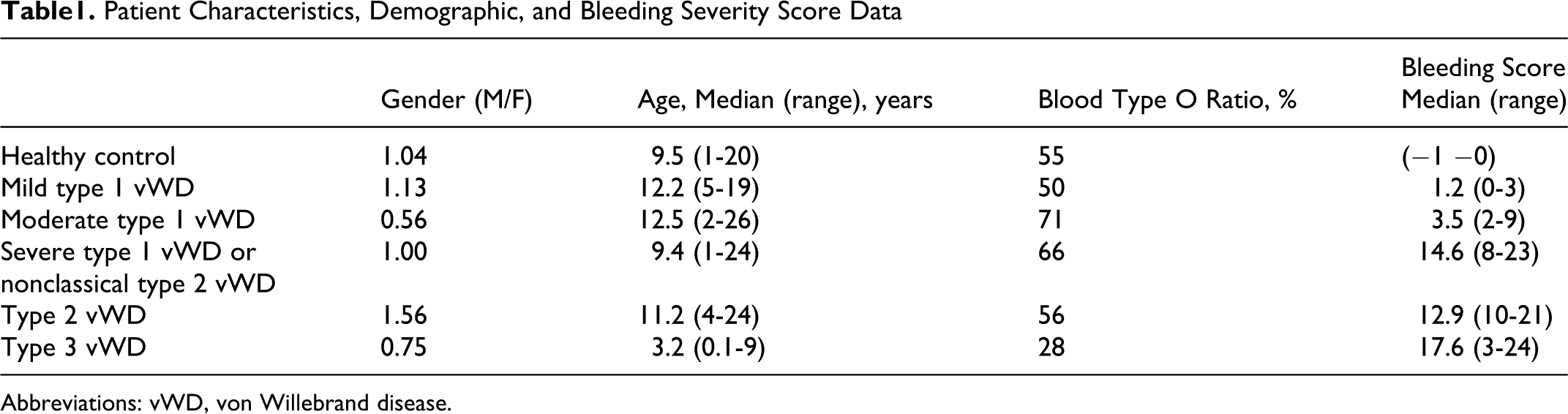
Abbreviations: vWD, von Willebrand disease.
Blood type O is associated with vWF levels approximately 25% lower than the population average. For this reason the blood group 0 ratio in mild type 1 vWD and healthy controls was kept closed in order to determine vWF:Ag limit value of mild type 1 vWD.
Written infoRmed consent was obtained for blood from all patients and healthy children and the study had the approval of the local ethic committee.
In patients with normal test results or only with prolonged APTT, vWF:RCo, vWF:Ag, FVIII:C, PFA- 100 testing (using both collagen/epinephrine [Col/Epi] and collagen/adenosine diphosphate [Col/ADP] test cartridges), and blood group analyses were performed. Laboratory tests were repeated at least twice before undertaking a diagnosis of vWD. Ristocetin-induced platelet aggregation (RIPA) assay is performed to aid in diagnosing type 2B vWD. RIPA may be done as part of routine platelet aggregation testing. Low-dose RIPA is carried out in platelet-rich plasma, using a low concentration of ristocetin (usually <0.6 mg/mL, although ristocetin lots vary, resulting in the use of slightly different ristocetin concentrations). Normal closure time reference mean (ranges) values for PFA-100 were 92 seconds (71-118 seconds) for Col/ADP cartridge and 132 seconds (85-165 seconds) for Col/Epi cartridge. Abnormal (high test results for) PFA-100 closure time (CT) were graded as slightly, moderately, and maximally prolonged and are shown in Table 2 .
Normal Ranges of PFA-100 Levels and Classification of Prolonged PFA-100 Values
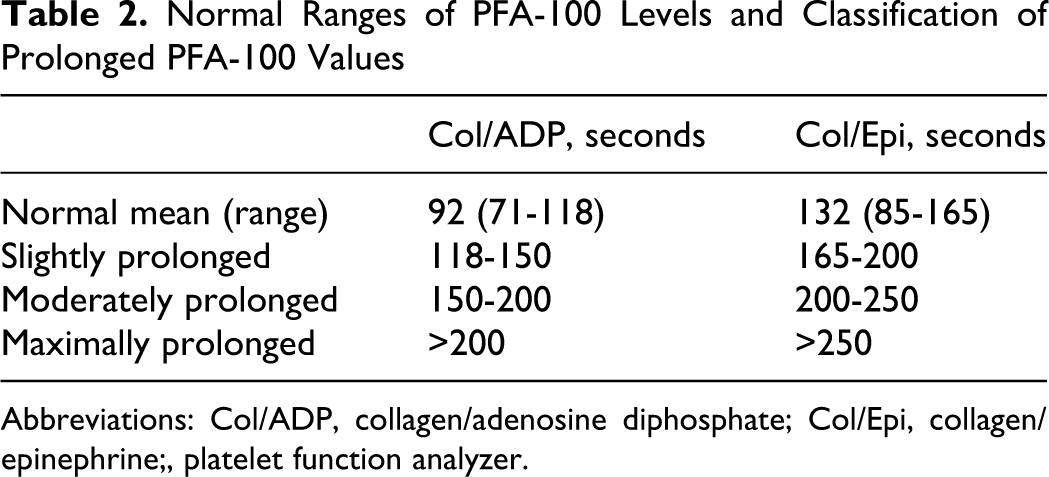
Abbreviations: Col/ADP, collagen/adenosine diphosphate; Col/Epi, collagen/epinephrine;, platelet function analyzer.
Patients with infection, low hemoglobin or low platelet levels or on treatment with nonsteroid anti-inflammatory drugs were excluded from the study.
Forty-seven sex- and age-matched healthy children were taken as the control group. Eight milliliters of blood was collected into standard 3.8% buffered sodium citrate tubes from patients and healthy children. PFA-100 analysis was performed immediately and plasma was stored at −80°C for a maximum period of 3 months to detect vWF:RCo, vWF:Ag, FVIII levels. vWF:RCo levels were detected by aggregometry (Apact 4004, Tokra, Germany) and normal ranges was between 60% and 160%, and vWF:Ag levels were determined using a latex immunoassay using the STA-Compact analyzer (Diagnostica Stago, Asniéres, France). Normal ranges for vWF:Ag was 60% to 150%. Factor VIII coagulant (FVIII:C) activity was assayed by means of automatic coagulation machines (Sysmex, CA- 1500, Dade-Behring, Leusden, The Netherlands) using FVIII deficient plasma. The lower limit level for FVIII:C detection is below 1%. Normal ranges for FVIII:C was 50% to 150%. Closure time (CT, Col/Epi) was assessed using the Platelet Function Analyser (PFA-100® Dade-Behring, Marburg, Germany).
The current classification of congenital vWD is based on the successive recommendations of the vWF Scientific Standardization Committee (SSC) decided at the annual SSC meetings of the International Society on Thrombosis and Hemostasis (ISTH) between 2000 and 2006. 6,7 The vWF-SSC classification of vWD patients is based on a few laboratory tests, including FVIII: coagulant activity (C), vWF:antigen (Ag), vWF:ristocetin cofactor (RCo), and RIPA.
We classified the patients phenotypically according to the laboratory test results and the severity of the clinical symptoms. 8,9 Grades of bleeding severity were used to compute the bleeding score in the Molecular and Clinical Markers for the Diagnosis and Management of Type 1 von Willebrand disease (MCMDM-1 VWD) study. A bleeding questionnaire was administered by a physician to each enrolled 112 vWD and 47 healthy controls. 10 Based on these considerations, patients were grouped as follows (Table 3 ).
Laboratory Parameters in Patients With vWD Types 1, 2, and 3 a
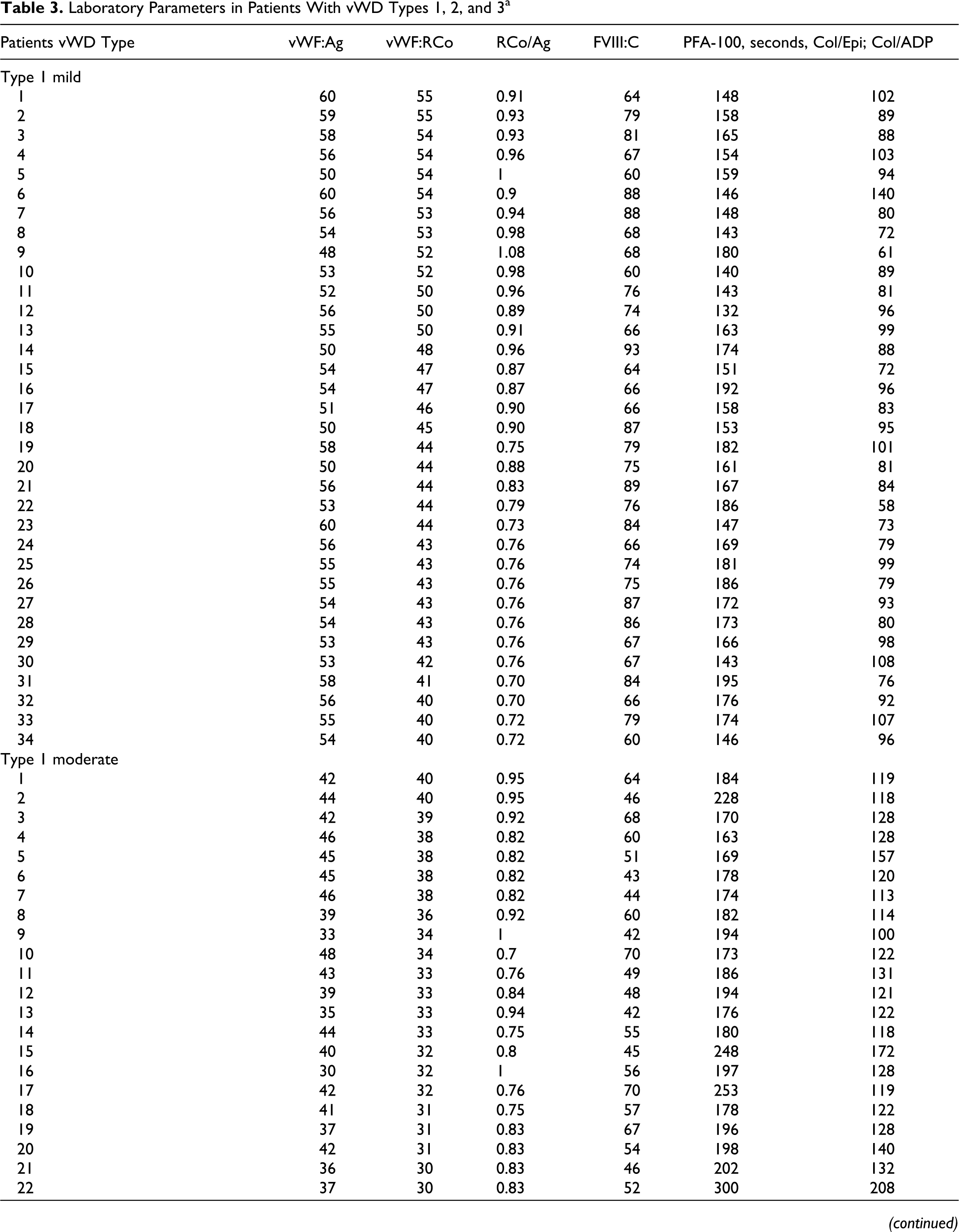
Abbreviations: Col/ADP, collagen/adenosine diphosphate; Col/Epi, collagen/epinephrine; PFA, platelet function analyzer.
Mild Type 1 vWD
Only 1 or 2 unclear minor bleeding symptoms occur and secondary bleeding following trauma and/or surgery is absent. A quantitative vWF deficiency with slightly decreased values of 2 vWF parameters (vWF:RCo 40%-55% or vWF:Ag levels 50%-60%) and normal FVIII:C level. In PFA-100 analysis, both Col/Epi and Col/ADP normal or only Col/Epi slightly prolonged. This group mainly consisted entirely of ‘mild type 1 vWD’ (n = 34).
Moderate Type 1 vWD
Bleeding symptoms are mostly mucocutaneous, that is frequent episodes of epistaxis and/or prolonged or profuse menstruation which usually do not require medical treatment or administration of factor VIII (FVIII)/vWF concentrate.
A quantitative vWF deficiency with equally decreased values of all vWF parameters and a normal ratio of close to unity for vWF:RCo/Ag, vWF:Ag (30%-48%), and vWF:RCo (27%-40%), FVIII:C levels normal or near-normal (40%-70%), either Col/Epi and Col/ADP slightly prolonged or only Col/Epi moderately prolonged. This group mainly consisted entirely of “moderate type 1 vWD” (n = 29).
Severe Type 1 vWD or Nonclassical Type 2 vWD
The patient has recurrent mucocutaneous bleeding episodes since early childhood, more than 2 bleedings after tooth extraction, trauma, or surgery and bleeding requiring medical treatment and/or FVIII/vWF concentrate transfusion because of abnormal bleeding after surgery and/or trauma or for severe menstrual blood loss in women. Prolonged bleeding for a few to several hours or even >24 hours after a tooth extraction, minor trauma, or surgery.
Moderate-severe deficiency of vWF:Ag and vWF:RCo parameters below 27%, FVIII:C level below 40%, both Col/Epi and Col/ADP are moderately or maximally prolonged. Some patients with the diagnosis of type 2 vWD may reveal laboratory findings similar to severe type 1 vWD. This group mainly consisted entirely of “severe vWD type 1 or non-classical vWD type 2” (n = 12).
Type 2 vWD
The patient has recurrent mucocutaneous bleeding episodes since early childhood, more than 2two bleedings after tooth extraction, trauma or surgery and bleeding requiring medical treatment and/or FVIII/vWF concentrate transfusion because of abnormal bleeding after surgery and/or trauma, or for severe menstrual blood loss in women. Prolonged bleeding for a few to several hours or even >24 h after a tooth extraction, minor trauma or surgery.
FVIII:C and vWF:Ag values may be normal, near-normal or decreased, and vWF:RCo value decreases remarkably compared to vWF:Ag levels. This is a qualitative vWF deficiency situation, being the ratio (<0.70) for vWF:RCo/Ag. This group consisted entirely of “type 2 vWD” (n = 23). Patients from this group, plus patients with type 2 vWD from group C, underwent the RIPA test to determine the subtypes of type 2 vWD. Increased RIPA (0.5 mg/mL) with both Col/Epi and Col/ ADP moderately or maximally prolonged is attributted to type 2B vWD.
Type 3 vWD
A moderate/severe type of mucocutaneous bleeding since early childhood in addition to hemarthrosis, muscle bleeding, and a need for prophylactic treatment with FVIII/vWF concentrate. Undetectable vWF:Ag, vWF:RCo below 12%, FVIII:C levels between 1% and 9%, both Col/Epi and Col/ADP maximally prolonged would represent type 3 vWD (n = 14).
All patients with mild, moderate, severe type 1 vWD or nonclassical type 2 vWD and type 2 vWD should be given a test dose of DDAVP for diagnostic purposes to establish whether the response is sufficient or insufficient for clinical use. If FVIII:C, vWF:RCo, vWF:Ag, and PFA-100 reach normal levels after 0.3 μg/kg infusion of DDAVP followed by near-normal, response of vWF parameters is sufficient.
Results
This study included 34 patients with mild type 1 vWD, 29 patients with moderate type 1 vWD, 12 patients with severe type 1 vWD or nonclassical type 2 vWD, 23 patients with type vWD, 14 patients with type 3 vWD, and 47 healthy control (Table 3).
Mild type 1 vWD in 34 cases (vWF:RCo 40%-55%), moderate type 1 vWD in 29 (vWF:RCo 27%-40%), severe type 1 vWD or nonclassical type 2 vWD in 12 cases (vWF:RCo 4%-16%), type 2 vWD in 23 (vWF:RCo 4%-38%), and type 3 vWD in 14 (vWF:RCo 0%-12%). Eight of the type 2 vWD patients had vWF:RCo values of <16% and were similar to those of severe type 1 vWD or nonclassical type 2 vWD but vWF:Ag and FVIII:C levels of the 8 patients were normal or near-normal. The PFA-100 result has demonstrated to be abnormal in the majority of persons with vWD. Mild type 1 vWD patients had normal to slightly prolonged Col/Epi (>165). Moderate type 1 vWD had normal to slightly prolonged Col/ADP (>118) and slightly to moderately prolonged Col/Epi (165-200). All patients with severe type 1 vWD or nonclassical type 2 vWD, vWD types 2 and 3 had a moderately/maximally prolonged PFA-100 (Col/ADP: >150 and Col/Epi: >200). The percentage of patients identified by bleeding severity score, according to vWD types, are shown in Table 1. The most common symptoms seen in vWD types are epistaxis, bruise, bleeding after dental extractions and minor wounds, and menorrhagia. Bleeding symptoms are usually mild in type 1, increasing in severity in severe type 1 or nonclassical vWD type 2, and vWD types 2 and 3. The clinically more severe symptoms such as bleeding after circumcision occur in higher proportions of type 3 patients compared with severe type 1 or nonclassical type 2 vWD and type 2 vWD patients. However, this difference is rather small for epistaxis, menorrhagia, and bleeding from minor wounds. Severity of bleeding was similar between Type 2 vWD and severe type 1 vWD or non-classical type 2 vWD. In mild/moderate type 1 vWD patients, 1 hour after DDAVP, the FVIII:C, vWF:Ag, vWF:RCo, and PFA (ADP and Epi) returned to normal values and a 2- to 3-fold increase in the plasma concentrations of FVIII:C, vWF:Ag, vWF:RCo were observed.
The 6 non-responsive severe type 1 vWD or nonclassical type 2 vWD patients showed a good response of FVIII:C and vWF:Ag but a poor response of vWF:RCo to DDAVP with no correction of PFA (Epi and ADP). vWF:Ag levels of the 4 nonresponsive severe type 1 vWD or nonclassical type 2 vWD patients were 44% to 69%, levels of vWF:RCo 18% to 22%, and PFA-100 values Col/Epi: 206 to 254 seconds and Col/ADP: 154 to 188 seconds. Of the 4 patients, 2 displayed abnormally increased RIPA response against low level of ristocetin. So these 2 patients were evaluated as type 2B vWD. Only 2 of 6 responsive severe type 1 vWD or nonclassical type 2 vWD patients showed a restricted response of vWF:RCo (34% and 32%) and PFA (Epi: 166 and 161, ADP: 121 and 116) to DDAVP compared to those of FVIII:C and vWF:Ag. For these patients a poor response was obtained in Col/Epi results of 236 and 224 seconds, Col/ADP results of 186 and164 seconds, vWF:RCo values of 24% and 13%, vWF:Ag levels of 41% and 38% but showed FVIII:C to normal levels, respectively, 4 hours after the DDAVP.
The 12 nonresponsive vWD type 2 patients (vWF:RCo <27%) showed poor responses of vWF:RCo and PFA (ADP and Epi) while good responses of vWF:Ag and FVIII:C to DDAVP (Table 3).
Discussion
von Willebrand disease is the most commonly seen hereditary bleeding disorder, and diagnosis requires a detailed clinical history including bleeding manifestations of patient and family especially mucocutaneous bleeding evidences and should be followed by some laboratory tests: vWF:Ag, vWF:RCo, FVIII:C, RIPA, vWF multimers, and genetic analysis. However vWF:Ag, vWF:RCo, and FVIII:C are still the main tests for the diagnosis of vWD in most of the centers. 11 –13 However, these tests may lead to error in the diagnosis of vWD or its types up to 30% particularly in type 1 vWD. 14 In this study, PFA-100, which is important in the identification of vWD was included in the first-step diagnostic tests of the disease. 15,16
The sensitivity of the PFA-100 to vWD varied according to vWD types, with the highest sensitivity being to types 2 and 3 vWD, then to type 1 vWD individuals with lower plasma vWD, followed by type 1 vWD with borderline abnormal/normal vWF. 17 –19 In the current study if PFA-100 test showed maximally prolonged closure time, the patients who had a ratio of vWF:RCo/Ag below 0.7 were accepted as type 2 vWD. The patients who had the same ratio of vWF without maximally prolonged CT were included in severe type 1 vWD or nonclassical type 2 vWD. PFA-100 CT was maximally prolonged for severe type 1 vWD nonclassical type 2 vWD, and types 2 and 3vWD, and this alone is not enough in the differential diagnosis of these groups. Patients with mild type 1 vWD may be related to overdiagnosis of vWD, and they could really be healthy persons. However, these patients were different than the healthy control with regard to clinical bleeding history and laboratory findings. 20,21 Identification of types 1 and 3 vWD is not so hard or complicated. 22 The serious problem is in defining the most heterogenous type of type 2 vWD. Although multimer analysis of Analysis of High molecular weight multimers (HMWM) of vWF or genetic tests makes it possible to differentiate type 2 vWD easily in developed centers, this method is not available in many centers. 23,24 In the current study PFA-100, RIPA, and DDAVP response which are easily available and practical tests for all centers were used in addition to main laboratory tests (vWF:Ag, vWF:RCo, and FVIII:C levels) to differentiate the type of vWD. Family members with bleeding evidence of the patients were evaluated via the same tests.
Moderate type 1 vWD is easy when the patient has a significant mucocutaneous bleeding history, decreased vWF, without relevant qualitative abnormalities, and a positive family history with autosomal dominant inheritance. Some of the patients with moderate type 1 vWD represent the clinical and laboratory features of classical type 2 vWD (normal levels of vWF:Ag and FVIII:C, low vWF:RCo). In the European type 1 study, MCMDM-1 vWD, 38% of families diagnosed as type 1 by expert laboratories had mutations and phenotypes more compatible with types 2A or 2M. 25 In our study, we did not perform multimer and mutation analysis but used DDAVP response and reexamined the family members with bleeding history.
Patients with mild/moderate type 1 vWD usually respond well to DDAVP (Table 4 ). Interestingly, the response of FVIII:C to DDAVP is higher than that of vWF:Ag.
Response of vWF:Ag, vWF:RCo, FVIII:C, and PFA-100 before and 1 hour After DDAVP in Patients With vWD Types a
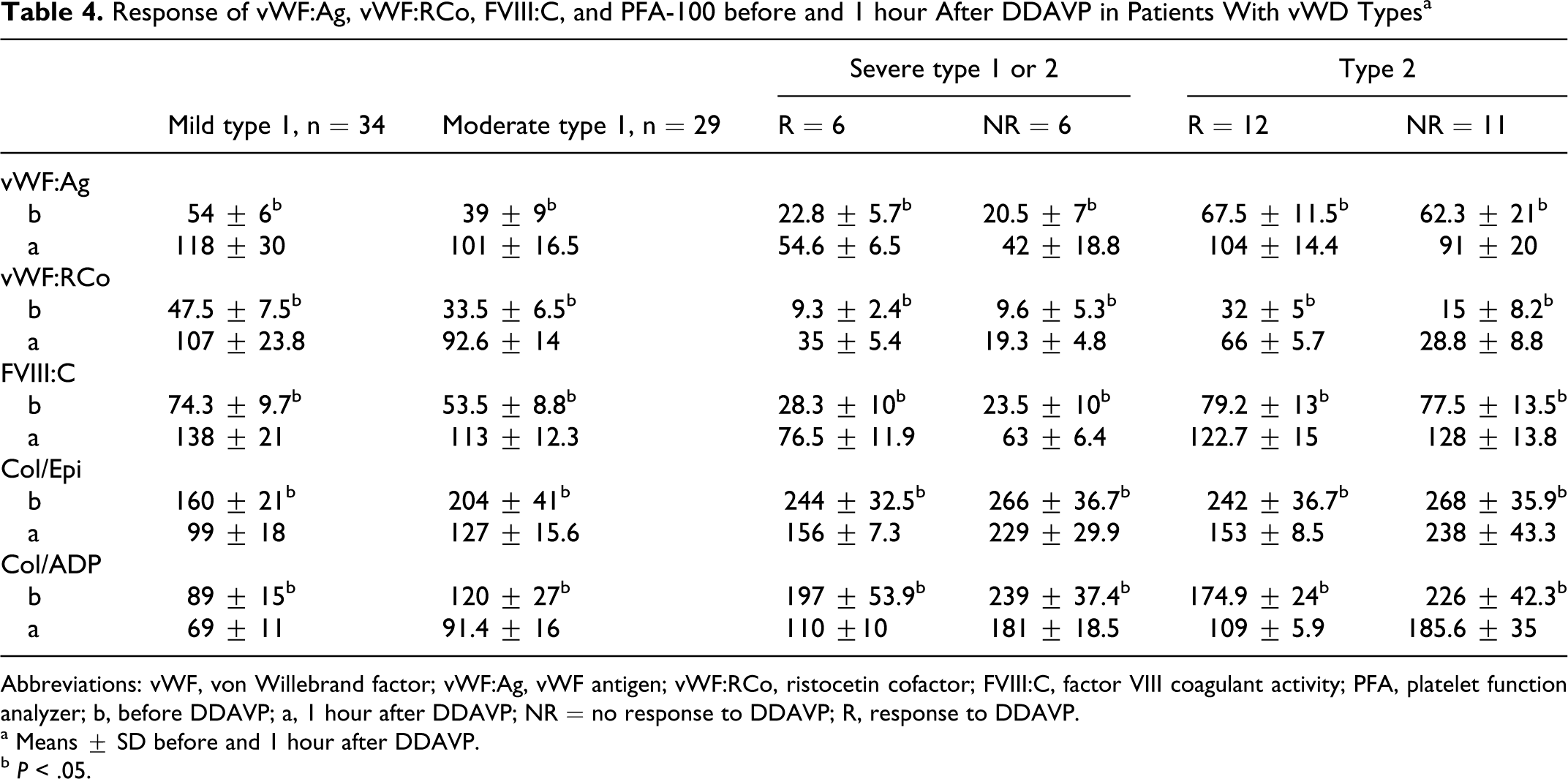
Abbreviations: vWF, von Willebrand factor; vWF:Ag, vWF antigen; vWF:RCo, ristocetin cofactor; FVIII:C, factor VIII coagulant activity; PFA, platelet function analyzer; b, before DDAVP; a, 1 hour after DDAVP; NR = no response to DDAVP; R, response to DDAVP.
a Means ± SD before and 1 hour after DDAVP.
b P < .05.
When we evaluated the family members of the patients who had positive response to DDAVP, it was seen that all clinical findings resolved by time and laboratory findings were consistent with moderate type 1 vWD. However, the family members of the patients who did not respond to DDAVP showed persistence of mucocutaneous bleeding history and abnormal laboratory findings compatible with classical type 2 vWD. 26 –28 Type 2 vWD patients who not respond to DDAVP showed a good response of FVIII:C and vWF:Ag but a poor response of vWF:RCo, with no correction in PFA-100. vWD type 2 patients who respond to DDAVP are characterized by near-normal to prolonged values of PFA-100, normal FVIII:C, vWF:Ag, and low vWF:RCo (Table 4).
Budde et al reported that of the cases previously diagnosed as severe type 1 vWD, 38% showed deviations of the multimer patterns and were reclassified as nonclassical vWD type 2. vWF:RCo/vWF:Ag ratio of <0.7 was suggestive of a functional vWF defect; however, only 51% of these cases had a low vWF:RCo/vWF:Ag ratio of below 0.7. 29 This indicates that the vWF:RCo/vWF:Ag ratio was not always reliable to distinguish between severe type 1 vWD and nonclassical type 2 vWD. Because we could not do multimer analysis, DDAVP response was evaluated in the discrimination of severe type 1 vWD and type 2 vWD. According to DDAVP response, we thought that the 4 nonresponsive participants in severe type 1 or 2 vWD groups were nonclassical type 2 vWD because they had near-normal or normal vWF:Ag levels together with unrecovered vWF:RCo and PFA-100 levels. Although DDAVP did lead to greater intensity in low- to-intermediate molecular weight vWF, it did not lead to the release of high-molecular-weight vWF. Therefore, post DDAVP the recovered near-normal vWF:Ag levels and unrecovered PFA 100 CT as well as vWF:RCo levels were correlated closely with the function of vWF instead of vWF:Ag. 30 There were increased RIPA response in 2 of these patients, and they were considered type 2B vWD. 31
In conclusion, this study showed that measurement of vWF:RCo, vWF:Ag, FVIII:C, and PFA-100 parameters can differentiate vWD types but not the severe type 1 vWD or nonclassical type 2 vWD. In the differentiation of severe type 1 vWD or nonclassical type 2 vWD, the DDAVP response may be used. The PFA-100 may have a role in the monitoring of DDAVP therapy for individuals with vWD because this test is a simple and rapid tool to discriminate good and nonresponders to DDAVP. Although multimer analysis and mutation tests should be performed for definitive diagnosis of vWD and types of vWD, PFA-100 DDAVP response in addition to vWF:Ag, vWF:RCo, and FVIII:C tests give a less expensive and more practical option to differentiate the types of vWD for many patients.
Footnotes
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.