
Abstract
Introduction
von Willebrand Disease (vWD), the most frequent inherited hemorrhagic disorder, is caused by deficiency or abnormal function of von Willebrand factor (vWF). 1 In at least 2 large prospective epidemiological studies, up to 1% of a predominantly pediatric population was found to manifest symptoms and laboratory signs of vWD. 2 The clinical spectrum of the disease is characterized by an extreme heterogeneity of bleeding symptoms, ranging from a few, doubtful hemorrhagic symptoms to the occurrence of severe life-threatening episodes. The current revised classification of vWD identifies 2 major categories, characterized by quantitative (type 1 and 3) or qualitative (type 2) vWF defects. Type 3 vWD is characterized by total absence or trace amounts of VWF in plasma and platelets. Type 3 vWD is an extremely rare disease. These patients are usually homozygotes or compound heterozygotes for vWF gene mutations in both alleles, leading to severely reduced or absent plasma and platelet vWF. 3
A wide heterogeneity of plasma and/or platelet vWF levels are usually observed among obligatory carriers (OCs) of type 3, pointing at the heterogeneity of the molecular basis responsible for the deficiency. Indeed, these participants may be asymptomatic and phenotypically normal or may have bleeding symptoms.4,5 Hence, diagnosis of the OC type 3 vWD cases might be missed and misdiagnosed as hemophilia or other vWD types.
It is important to diagnose OC type 3 vWD in countries where marriages between relatives is common, such as Turkey. However, mild bleeding or no bleeding in such patients complicates the diagnosis of the disease. It is not clear how the diagnosis of OC type 3 vWD will be made based on FVIII:C (Factor VIII activity), vWF:Ag (von Willebrand factor antigen), vWF:RCo (von Willebrand factor ristocetin cofactor activity), and PFA (platelet function analyzer )-100 parameters. Therefore, the purpose of the study is to investigate how OC type 3 vWD diagnoses may be established by studying laboratory phenotypes of close relatives of patients diagnosed with 3 vWD.
Patients and Methods
A total of 8 patients with type 3 vWD (index cases) and 20 patients who were defined as OC type 3 vWD were enrolled in the study. None of the 20 OC type 3 vWD diagnosed cases had bleeding complaints and only 1 male and 1 female patients were misdiagnosed as hemophilia A and type 1 vWD, based on their routine preoperatively screened prolonged Active Partial Thromboplastin Time (APTT) measurements.
Forty-seven healthy children were taken as the control group. The ratio of blood type O in patients in the control group was 55%.
Definition of OC Type 3 vWD
Type 3 OCs were identified on the basis of a pedigree showing that they were parents, brother, sister. or children of a patient with type 3 vWD.
In 1 of the 8 type 3 vWD index cases, there was consanguinity between the parents of the case. Not all parents of the cases were included in the current study due to divorces, deaths, and loss of communication with parents; but those who could be contacted with and those with abnormal test results were included in the analysis.
Definition of Type 3 vWD Patients
Patients with moderate-to-severe bleeding, undetectable vWF:Ag, vWF:RCo below 5%, FVIII:C levels between 1% and 9%, and maximally prolonged Col/Epi and Col/ADP were defined as type 3 vWD.
Definition of Type 1 vWD Patients
The definition of type 1 vWD patients is according to the 2 studies of Akin et al 6 and Michiels et al. 7
Mild type 1 vWD
A quantitative vWF deficiency with slightly decreased values of 2 vWF parameters (vWF:RCo 40%-55% or vWF:Ag levels 50%-60%) and normal FVIII:C level. In PFA-100 analysis, both Col/Epi and Col/ADP are normal or only Col/Epi is slightly prolonged.
Moderate type 1 vWD
A quantitative vWF deficiency with equally decreased values of all vWF parameters and a normal ratio of close to unity for vWF:RCo/Ag, vWF:Ag (30%-48%), and vWF:RCo (27%-40%), FVIII:C levels are normal or near normal (40%-70%), either Col/Epi and Col/ADP is slightly prolonged or only Col/Epi is moderately prolonged.
Severe type 1 vWD or nonclassical type 2 vWD
Moderate-to-severe deficiency of vWF:Ag and vWF:RCo parameters below 27% includes FVIII:C level below 40%, both Col/Epi and Col/ADP are moderately or maximally prolonged.
Bleeding History
Grades of bleeding severity were used to compute the bleeding score in the MCMDM-1VWD Study. 8 A bleeding questionnaire was administered by a physician to each enrolled 20 OC type 3 vWD.
FVIII:C, PFA-100 (Platelet Function Analyzer) and VWF Measurement
Laboratory tests were repeated at least twice before undertaking a diagnosis of vWD. Eight milliliter blood was collected into standard 3.8% buffered sodium citrate tubes from patients and healthy children. Testing with the PFA-100 should be conducted no sooner than 15 minutes after blood collection and blood sample was stored at −80 C for a maximum period of 3 months to detect vWF:RCo, vWF:Ag, and FVIII.C levels. vWF:RCo levels were detected by aggregometry (Apact 4004, Tokra, German) and normal range was between 60% and 160%, vWF:Ag levels were determined using a latex immunoassay using the STA-Compact analyzer (Diagnostica Stago, Asniéres, France). Normal range for vWF:Ag was 60% to 150%. Factor VIII coagulant (FVIII:C) activity was assayed by means of automatic coagulation machines (Sysmex, CA- 1500, Dade-Behring, Leusden, The Netherlands) using FVIII-deficient plasma. The lower limit level for FVIII: C detection is below 1%. Normal ranges for FVIII:C was 50% to 150%. Closure time (CT, collagen/ epinephrine) was assessed using the Platelet Function Analyzer (PFA-100; Dade-Behring, Marburg, Germany).
Normal closure time reference mean (ranges) values for PFA-100 were 92 (71-118) seconds for Col/ADP cartridge and 132 (85-165) seconds for Col/Epi cartridge. Closure time values > 250 seconds are considered maximally prolonged. 9
Results
Laboratory values (min-max) of control groups are vWF:Ag 62 to 200; VWF:RCo 60 to 120; FVIII:C 68 to 196; PFA-100 Col/Epi <153 seconds and Col/ADP <111 seconds.
The median bleeding score (range) of the 20 OC type 3 vWD cases was found to be -1-0. Table 1 presents 8 type 3 vWD cases (index cases) and beneath each case OC type 3 vWD-diagnosed relatives and their vWD types, which had similar laboratory phenotypes, are shown.10,11
Laboratory Diagnosis of Obligator Carrier Type 3 vWD
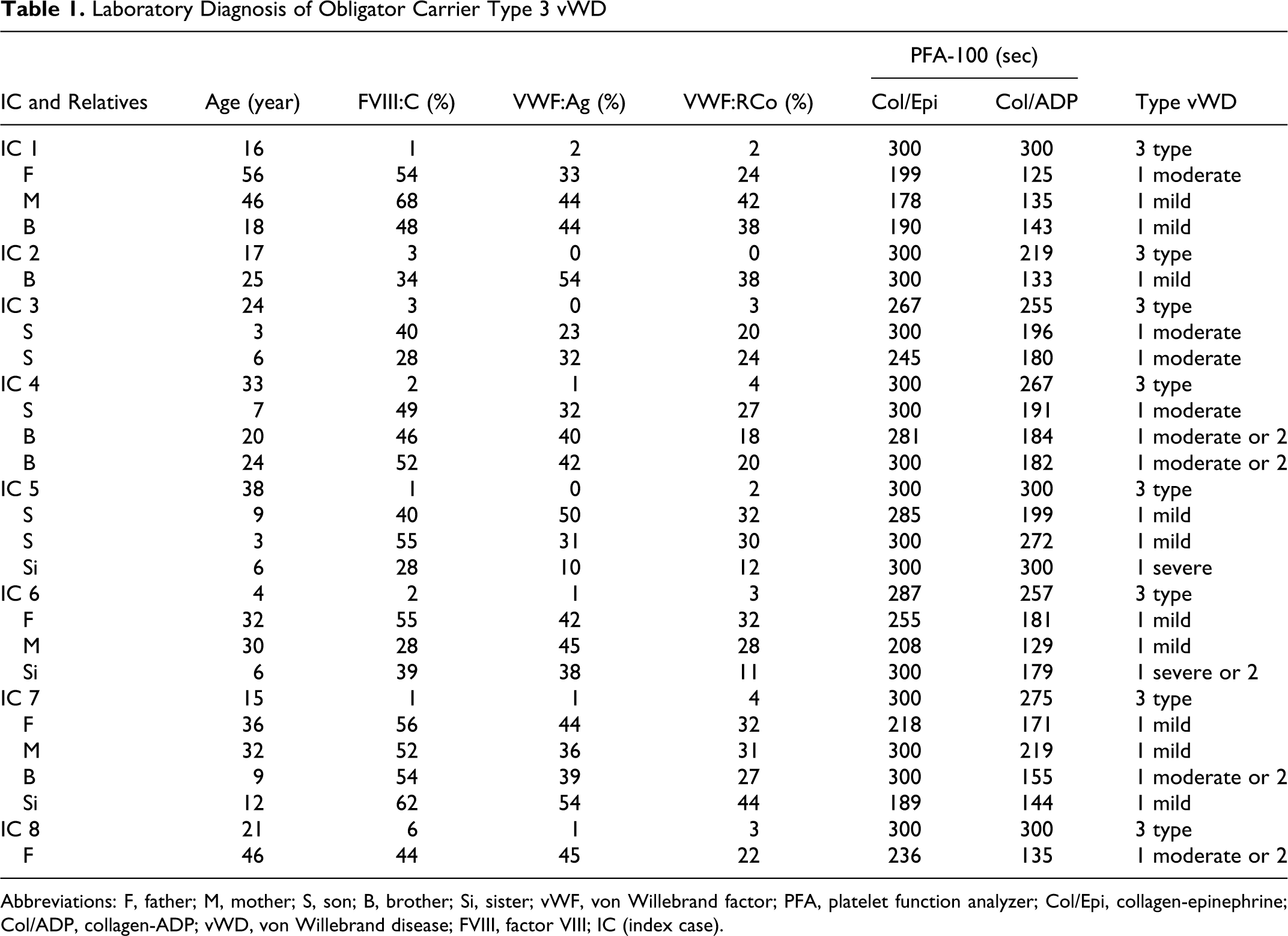
Abbreviations: F, father; M, mother; S, son; B, brother; Si, sister; vWF, von Willebrand factor; PFA, platelet function analyzer; Col/Epi, collagen-epinephrine; Col/ADP, collagen-ADP; vWD, von Willebrand disease; FVIII, factor VIII; IC (index case).
According to the 2 studies (Akin et al 5 and Michiels et al 6 ), 10 cases had similarity with mild type vWD, 4 cases had similarity with moderate type 1 vWD, 4 other cases had type 1 or 2 vWD similarities, 1 case had similarity with severe type 1 vWD, and 1 case also had similarity with severe type 1 or 2 vWD, based on their laboratory phenotypic characteristics.
While FVIII:C, vWF:Ag, vWF:RCo, and PFA-100 CT (Col/ADP and Col/Epi) laboratory findings of OC type 3 cases have similar characteristics as type 1 and type 2 vWD classification, PFA-100 CT (Col/ADP and Col/Epi) values were both significantly higher in OC type 3 vWD than in mild type 1 vWD.
Laboratory phenotypic characteristics of OC type 3 vWD cases even show differences between brothers, sisters, parents, and children of the cases in typology.
Discussion
The signs and symptoms of vWD depend on the type and severity of the disease. Many people have such mild symptoms that they do not realize they have the disease. The severe type 3 form of the disease shows a recessive pattern of inheritance, with parents and children not usually manifesting clinical symptoms.
The most severe form of vWD is type 3 vWD. Its diagnosis is easier compared to other types of vWD due to severity of bleeding symptoms and its laboratory phenotypic characteristic.
However diagnosis of OC type 3 is not easy if they do not have a family member with type 3 vWD. The actual risk of bleeding in OC type 3 vWD has not been described clearly. Discordant results have been reported on the risk of bleeding of these subjects, not always related to the actual level of circulating vWF. 12
Obligatory carriers of a nonsense mutation related to vWD type 3 in the population are asymptomatic or manifest mild bleeding and have vWF levels at 50% of normal (true type 1 of vWD according to the law of Mendel). From a genotypic point of view, OCs of a null allele in vWD type 3 are very similar to asymptomatic or mild vWD type 1 patients. Parents of patients with recessive vWD type 3 have no history of bleeding or present with minor bleedings (1 or 2 bleeding symptoms, mainly epistaxis, bruises, and/or prolonged menstruations with no abnormal bleeding after tooth extraction, trauma, or surgery).13,14
Obligatory carrier of type 3 with a null mutation have bleeding symptoms and meet the criteria of mild vWD type 1. Using the bleeding score assessment, Castaman et al compared the severity of bleeding symptoms in 70 OC of recessive vWD type 3, 42 OC of vWD type 1, and 215 normal controls. Obligatory carrier of vWD type 3 with a null mutation had clearly less severe bleeding than patients diagnosed as vWD type 1. 15
They also showed that the OC of vWD type 3 is very similar to asymptomatic or mild vWD type 1 patients with a single mutated allele.
In this study, OC type 3 vWD had mimicking mild, moderate, and severe type 1 vWD patients.
PFA-100 CT was prolonged moderately or maximally in all OC type 3 VWD, and it was significantly higher in OC type 3 vWD than in mild type 1 vWD. The results of this study show that a great heterogeneity of vWF levels and reported bleeding history could be observed in heterozygotes carrying the same mutation, without a clear relationship between vWF levels and bleeding history. This heterogeneity adds to the difficulties of clinical and laboratory diagnosis of vWD. 16
In conclusion, we identified that OC type 3 vWD is similar specifically to type 1 vWD in terms of laboratory phenotypic character. Therefore, the OC type 3 vWD cases may speciously be misdiagnosed as the other vWD types.
It is important to diagnose OC type 3 vWD in close relatives of the type 3 vWD cases since the percentage of marriage between relatives is up to 20% in some regions of Turkey. We suggest that it may be used with PFA-100 as an easy and fast method in screening relatives.
Footnotes
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.