
Abstract
Introduction
Acute myocardial infarction (AMI) is a serious cardiovascular disease that has long threatened human health. 1 Recently, with the widespread implementation of percutaneous transluminal coronary intervention (PCI), the mortality rate of AMI has decreased annually. 2 However, it is still high 3 and closely related to individual differences, 4 time of interventional therapy, 5 postoperative drug selection, 6 and other factors. Heart failure (HF) is a common complication of AMI. 7 Acute HF occurs when decompensation occurs within a short period due to coronary artery obstruction resulting in insufficient blood supply to the myocardium. 8 In addition, late replacement repair occurs due to myocardial damage, resulting in cardiac dysfunction of systolic function and leading to chronic HF. 9 HF affects in-hospital survival and has a significant impact on long-term prognosis. Clinical diagnosis of HF is made using a comprehensive evaluation of symptoms, signs, laboratory examination, and echocardiography. 10 Studies reported that the occurrence of HF is closely related to the nutritional status of patients. 11 Patients with poor nutritional status have inadequate cardiac compensatory capacity and are more likely to develop HF. In addition, patients with excessive nutrition, namely obese patients, will have symptoms of HF due to excessive afterload under local myocardial ischemic necrosis because of the long-term high load of the heart. 12
Triglyceride glucose (TyG) index is an indicator proposed recently. It was originally used to evaluate insulin resistance and guide the medication of diabetic patients. 13 The relationship of the TyG index with cardiovascular diseases, including atherosclerosis, hypertension, the acute coronary syndrome, has been investigated recently.14–16 The correlation between AMI and the TyG index has also been extensively studied. High TyG index is associated with poor prognosis in patients with acute st-segment elevation myocardial infarction (STEMI). 17 However, there are few reports on the correlation between the TyG index and HF in patients with AMI. Some scholars suggested that the TyG index is suitable for evaluating nutritional status, which is also closely linked to HF.18–20 Therefore, this study investigated the correlation between the TyG index, occurrence of HF, and prognosis among patients with AMI.
Methods
Study Population
A single-center retrospective observational study was conducted on consecutive patients with AMI who underwent primary PCI in Zhongda Hospital (Nanjing, China) from January 2018 to December 2020. The inclusion criteria were as follows: 18–80 years old; diagnosed with AMI with or without ST-segment elevation based on symptoms, electrocardiogram, myocardial injury marker examination and coronary angiography following European Society of Cardiology (ESC) guidelines.21,22 The exclusion criteria were as follows: Severe trauma; a history of a major operation in the last 3 months; malignant tumor; severe liver and kidney dysfunction; old myocardial infarction; incomplete follow-up. The complete screening process is shown in Figure 1. The present study was approved by Zhongda hospital's Ethics Committee and registered in the Chinese Clinical Trial Registry (Registration No. ChiCTR2000041071).
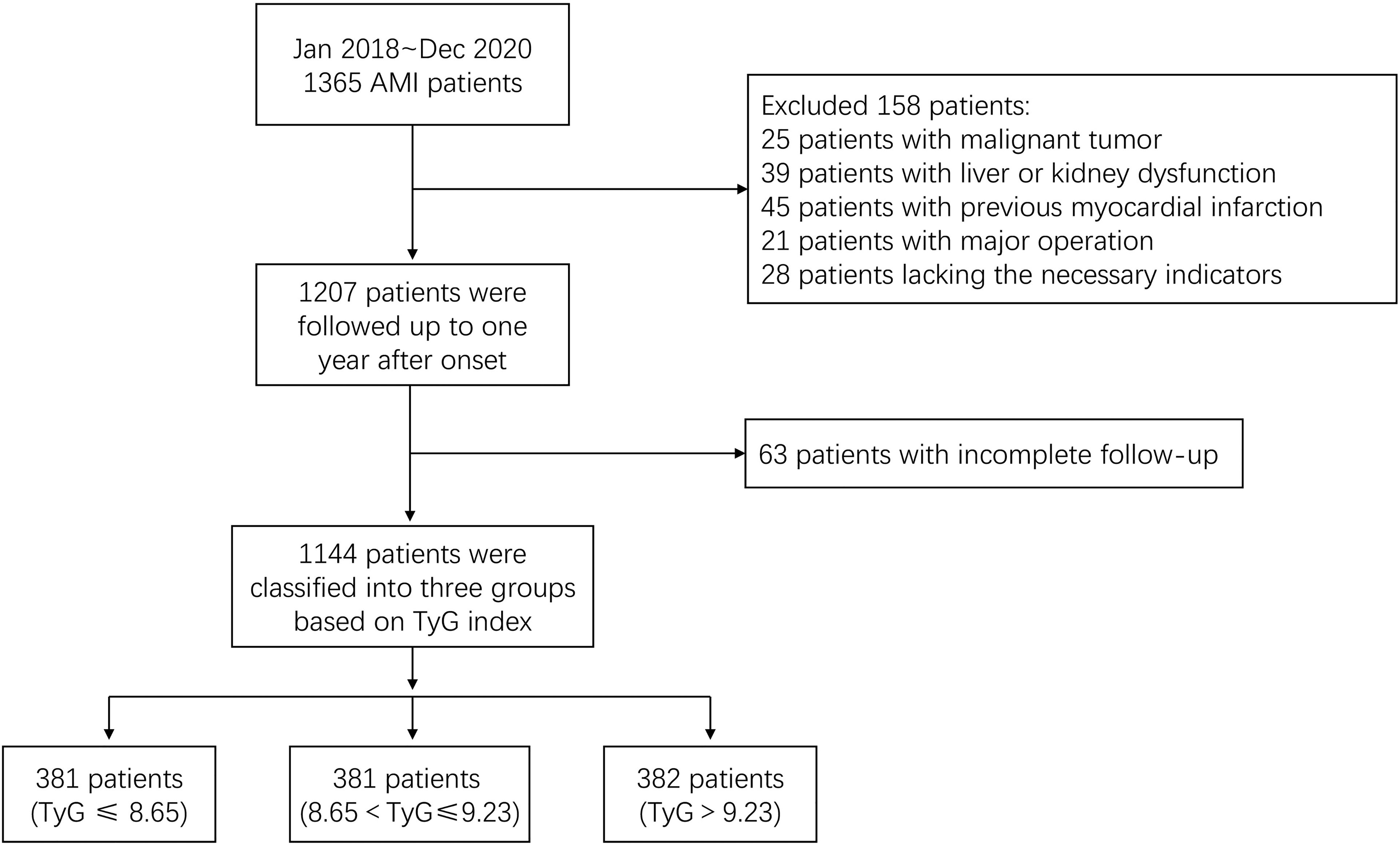
Study flow.
Laboratory Inspection
Emergency indicators including cardiac troponin I (cTnI) and brain natriuretic peptide (BNP) were tested within an hour of admission. Biochemical indicators, including albumin, fasting plasma glucose (FPG), triglyceride (TG), total cholesterol (TC), high-density lipoprotein (HDL), low-density lipoprotein (LDL), and Hemoglobin A1c (HbA1C) were tested using fasting blood samples taken in the morning on day two after the admission. All samples were immediately sent to the laboratory for testing. The TyG index was calculated according to the following formula: ln [fasting TGs (mg/dL) × FPG (mg/dL)/2].
Echocardiography
Color Doppler echocardiography was performed in all patients within 72 h of admission and analyzed by two experienced operators. Echocardiography was performed in accordance with the available guidelines of the European Association of Cardiovascular Imaging. Parasternal left ventricular long axis, short axis, left ventricular apical four-chamber heart, two-chamber heart, long axis, and apical four-chamber heart focusing on right ventricle were collected. The ventricular diameter was measured at the end of the systole. The atrial diameter was measured at the end of the diastole. Left ventricular ejection fraction (LVEF) was calculated using Simpson’s rule.
Percutaneous Coronary Intervention
All enrolled patients underwent the primary PCI on admission, including balloon dilation, thrombus aspiration, and/or stent implantation based on vascular lesions observed by coronary angiography (CAG). After the surgery, the patient was observed in the observation room for two hours and was sent to the cardiac care unit for close monitoring if there was no significant discomfort. The culprit vessel, the number of diseased vessels, stent implantation, and contrast agent dosage were recorded.
Study Endpoints and Definition
The primary endpoint was all-cause death. A 1-year follow-up was performed through outpatient visits or telephone interviews. The secondary end point was HF during hospitalization. The diagnosis of HF was based on a comprehensive assessment of the patient's symptoms, signs, electrocardiogram, BNP levels, and post-admission echocardiography confirmed by two or more cardiologists according to previously published ESC guidelines. 23 The diagnosis of other diseases in this paper were all based on previously published guidelines.24–26 Killip class > 1 means cardiac dysfunction or even cardiogenic shock in patients with AMI.
Statistical Analyses
According to the tertiles of the TyG index distribution, the study population was divided into three groups. Continuous variables conforming to normal distribution were tested by analysis of variance and reported as mean ± standard deviation (SD). For pairwise comparison between the three groups, the Bonferroni method was used when the variance was uniform, and Tamhane's T2 method was used when the variance was uneven. Rank sum test was performed on continuous variables that did not conform to the normal distribution, and they were expressed as median (interquartile range). The Kruskal–Wallis test was used for skewed data and pair-wise Mann Whitney U procedures were used for pairwise comparison between groups. The Chi-square test was performed on categorical variables and was expressed as proportions, and the Z Test was used for pairwise comparison between the groups. Potential associations between the TyG index and HF in AMI patients were investigated using binary logistic regression. Multivariable Cox regression analysis was used to estimate the hazard ratio (HR) and 95% confidence intervals (CI) for the TyG index in prognosing the all-cause mortality among AMI patients. Kaplan–Meier (KM) method was used to visualize the cumulative incidence and survival rates in different groups. All reported P-values were two-tailed. Statistical significance was set at P-value < .05, and analyses were conducted using SPSS statistical software (version 23.0).
Results
Baseline Characteristics
In total, 1144 patients completed the 1-year follow-up. Patients were approximately 62.1 (±12.8) years old, and 902 were males. Among them, 654 patients were diagnosed with STEMI. Based on the tertiles of the TyG index distribution, we divided them into three groups, group 1 (TyG ≤ 8.65), group 2 (8.65 < TyG ≤ 9.23) and group 3 (TyG > 9.23).
As shown in Table 1, the patients in group 1 had the highest mean age, the lowest body mass index (BMI), and the lowest mean heart rate. There were no significant differences in systolic blood pressure, diastolic blood pressure, and medical history of cerebrovascular disease (CVD), and chronic obstructive pulmonary disease (COPD) among the three groups. There were also no significant differences in commonly used cardiovascular medications. In contrast, there were significant differences in several laboratory tests among the three groups. Specifically, hemoglobin in routine blood examination, which was tested on admission and albumin, FPG, TG, TC, HDL, LDL, and HbA1C, which were tested on the second day showed significant differences. These results indicated differences in nutritional status among the three groups. Estimated glomerular filtration rate (eGFR) was calculated based on gender, age, and creatinine, and there were significant differences in eGFR among the three groups, suggesting differences in renal function.
Baseline Characteristics of Three Groups.

Data are expressed as mean ± standard deviation, medians with interquartile ranges or percentage. Abbreviations: BMI, body mass index; BP, blood pressure; STEMI, st-segment elevation myocardial infarction; AF, atrial fibrillation; COPD, chronic obstructive pulmonary disease; CVD, cerebrovascular disease; ACEI/ARB, angiotensin-converting enzyme inhibitor/angiotensin receptor blocker; CCB, calcium-channel antagonist; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BNP, brain natriuretic peptide; cTnI, cardiac troponin I; eGFR, estimated glomerular filtration rate; FPG, fasting plasma glucose; HbA1C, Hemoglobin A1C; HDL, high-density lipoprotein; LDL, low-density lipoprotein; PLT, platelets; RBC, red blood count; T3, triiodothyronine; T4, thyroxine; TC, total cholesterol; TSH, thyroid stimulating hormone; WBC, white blood cells; TyG index, triglyceride-glucose index.
Further, color Doppler echocardiography results were analyzed for all patients, and we found no significant differences in the size of all parts of the heart and LVEF between the three groups except the interventricular septum, and pulmonary arterial hypertension (Table 2).
Color Doppler Echocardiography for AMI Patients.

Data are expressed as mean ± standard deviation or percentage. Abbreviations: LA, left atrium; LV, left ventricular; RA, right atrium; RV, right ventricular; IVS, interventricular septum; LVEF, left ventricular ejection fraction; PAH, pulmonary arterial hypertension.
Characteristics of CAG are shown in Table 3. The main culprit vessels were the left anterior descending coronary artery and right coronary artery in 555 and 378 patients, respectively. The majority of patients had more than one vessel lesion, and the overall mean number of diseased vessels was 2.0 ± 0.8. Stent implantation is routine procedure in PCI, and the results showed no significant difference in the number of stent implantation (P = 0.766) between the groups.
Characteristics of CAG and PCI.
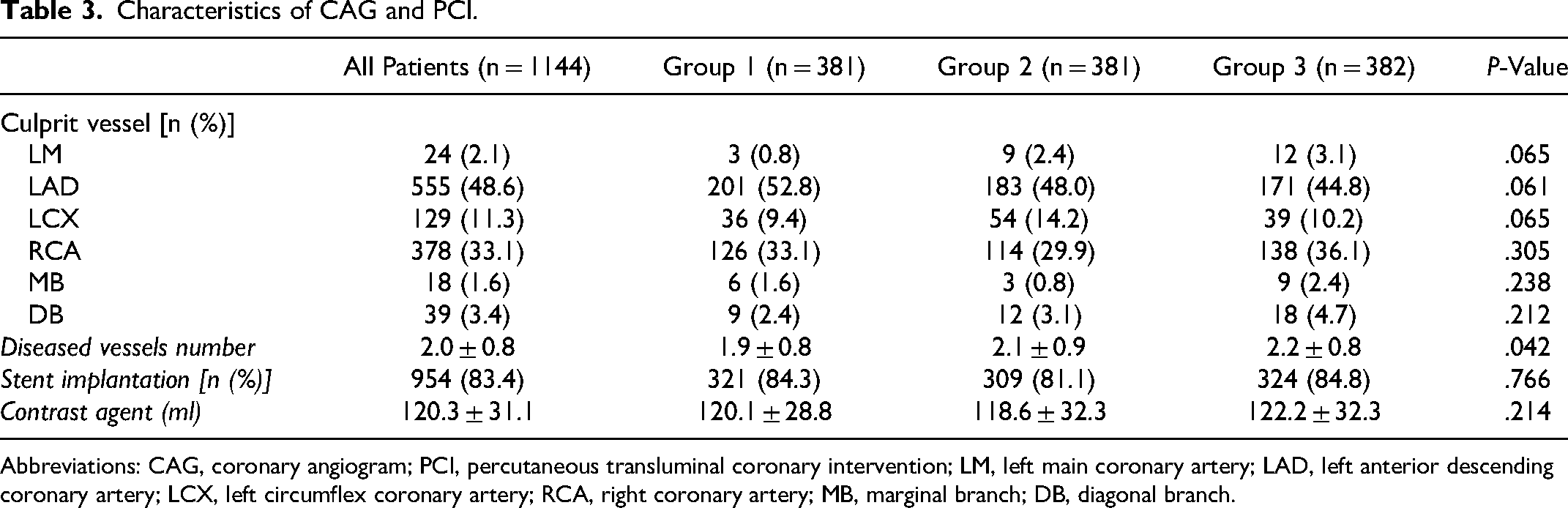
Abbreviations: CAG, coronary angiogram; PCI, percutaneous transluminal coronary intervention; LM, left main coronary artery; LAD, left anterior descending coronary artery; LCX, left circumflex coronary artery; RCA, right coronary artery; MB, marginal branch; DB, diagonal branch.
Examination of Potential Association Between TyG index and HF in AMI Patients
As one of the common complications of AMI, HF had a significant effect on the prognosis of AMI patients. HF occurred in 345 patients, and the baseline characteristics of patients with or without HF are shown in Table S1. Specifically, there was no significant difference in the TyG index between groups, suggesting that HF itself did not cause changes in the TyG index. We used logistic regression analyses to identify the potential association between the TyG index and the occurrence of HF. Variables strongly associated with HF were identified from previous studies and included in the univariate analysis. Next, variables with a statistically significant difference were included in the multivariable logistic regression analysis. According to Table 4, the TyG index, sex, age, Killip class, heart rate, BNP levels, hemoglobin levels, albumin levels, eGFR, FPG levels, LVEF and GRACE scores were the independent risk factors of HF. However, after incorporating these factors into multivariable logistic regression analysis, we found that only the TyG index, Killip class, heart rate, BNP levels, hemoglobin levels, LVEF, and GRACE scores were significantly different between the patients with HF and those without HF. Killip class, BNP levels, and LVEF were the main diagnostic criteria for HF, and we found that patients with a Killip class > 1 (odds raio [OR]: 19.835, 95% CI 10.433-37.709), higher BNP levels (OR: 1.013, 95% CI 1.011-1.015) or lower LVEF (OR: 0.001, 95% CI 0.000-0.004) were associated with complicated HF. Furthermore, patients in group 3 (OR: 9.070, 95% CI 4.359-18.875) had significantly higher rates of HF (P < .001) than those in group 2 (Table 4). However, among patients with Killip class > 1, we found that there was no significant correlation between TyG index and the incidence of HF (Table S2). Variance inflation factors of all these variables were thus tested, and the collinearity of these factors was low. To verify the regression model, 75% of the samples were randomly selected and a correlation analysis between TyG index and HF was conducted again. The results proved that the regression model was effective (Table S3). Because the proportion of individuals with diabetes in group 3 (32.2%) was significantly higher than that in other groups, we excluded diabetic patients to explore the influence of diabetes on the research results, and conducted regression analysis again. The results showed that the HF incidence in group 2 was still significantly lower than that in groups 1 (OR: 2.887, 95% CI 1.278-6.521, P = .011) and 3 (OR: 6.685, 95% CI 2.768-16.144, P < .001) (Table S4).
Univariate and Multivariate Logistic Regression Analysis for Occurrence of Heart Failure.

Abbreviations: TyG index, triglyceride-glucose index; TOR, time from onset to reperfusion; STEMI, st-segment elevation myocardial infarction; BNP, brain natriuretic peptide; eGFR, estimated glomerular filtration rate; FPG, fasting plasma glucose; HbA1C, Hemoglobin A1C; LVEF, left ventricular ejection fraction.
Associations Between the TyG index and the all-Cause Mortality in AMI Patients
We recorded patients’ survival up to 1 year of discharge during the follow-up, with all-cause death as the endpoint. According to Cox regression analysis adjust for the previously known risk factors for incident cardiovascular disease, we found that patients in group 3 had a significantly higher mortality rate (HR: 2.996, 95% CI 1.058-8.487, P = .039) compared to group 2, while patients in group 1 did not show a statistical difference (HR: 1.754, 95% CI 0.602-5.109, P = 0.303) (Table 5). As shown in Table S5, the TyG index was not significantly associated with all-cause death at the 30-day follow-up. At the 90-day follow-up, the TyG index was associated with all-cause death in univariate regression analysis but not in the multivariable regression analysis when multiple variables were included (Table S6). These results suggest that the predictive value of the TyG index for all-cause death among patients with AMI increases over time. In addition, after excluding patients with Killip class > 1, we further explored the correlation between TyG index and all-cause death. The results showed that TyG index was not significantly associated with all-cause death at the 30-day and 90-day follow-ups but patients in group 3 had a significantly higher mortality rate than those in group 2 at the 1-year follow-up (HR: 3.113, 95% CI 1.549-6.743, P = 0.022) (Table S7-S9). According to the KM cumulative incidence curves (Figure 2), group 2 had a significantly lower 1-year mortality rate than the other groups (log-rank test, P = .046), and the survival rate curves are shown in Figure S1. Similarly, to exclude the influence of diabetes on the study results, diabetes patients were excluded and Cox survival analysis was conducted again, which showed that the long-term all-cause mortality in group 2 was still significantly lower than that in group 3 (HR: 6.741, 95% CI 3.558-8.120, P = .015) (Table S10).

Cumulative incidence curves for all-cause mortality across the triglyceride-glucose (TyG) index tertiles.
Cox Proportional Hazards for All-Cause Mortality in AMI Patients.

Abbreviations: TyG index, triglyceride-glucose index; AF, atrial fibrillation; BNP, brain natriuretic peptide; CIN, contrast-induced nephropathy; COPD, chronic obstructive pulmonary disease; CVD, cerebrovascular disease; BP, blood pressure; eGFR, estimated glomerular filtration rate; FPG, fasting plasma glucose; HbA1C, hemoglobin A1C; HDL, high-density lipoprotein; LDL, low-density lipoprotein; LVEF, center ventricular ejection fraction; STEMI, st-segment elevation myocardial infarction; TC, total cholesterol; TOR, time from onset to reperfusion.
Further, we analyzed the correlation between the TyG index and the long-term prognosis of AMI patients with or without HF. The results showed that the TyG index lost its prognostic value when AMI patients were grouped according to the occurrence of HF (Tables S11 and S12).
Discussion
This study explored the correlation between the TyG index and long-term prognosis in patients with AMI. The results showed that patients with a high TyG index had significantly higher long-term mortality than patients with a median TyG index. This suggests that a high TyG index is closely associated with a poor prognosis.
Currently, there are many studies on the TyG index, mainly focusing on the prognostic evaluation of the TyG index for diabetes and cardiovascular diseases.27,28 According to the calculation formula, the TyG index, as an indicator of comprehensive blood glucose and lipid levels, is inevitably inseparable from diabetes. Further, as one of the high-risk factors of cardiovascular diseases, diabetes has long been extensively explored in basic and clinical studies for its important role in the occurrence and development of cardiovascular diseases. 29 This study also analyzed the correlation of blood glucose and lipid levels with HF and death. The results showed no correlation between blood lipid levels and HF, whereas blood glucose levels showed significant statistical correlation with HF in univariate analysis; however, both the factors were removed from the model in multivariable analysis. This result differs from those reported in many clinical studies,30,31 and it may be because of the bias caused by the limited sample number. Elevated TG levels are associated with an increased risk of developing HF in women. 32 In baseline data, there was no significant difference in the ratio of male to female between groups, but the TG levels in group 3 were significantly higher than those in the other groups. Perhaps women in group 3 were at a higher risk of developing HF than those in the other groups because of their higher TG levels. Further, we believe this is related to the TyG index itself. Currently, many clinical studies have a keen interest in combining classical indicators to find whether they may be of better or new clinical value. The same is true for the TyG index. Scholars have suggested that the TyG index is closely related to insulin resistance compared with simple blood glucose and blood lipids levels among patients. 33 Insulin resistance is closely related to type 2 diabetes and reflects the metabolic status of patients to a certain extent. 34 In this study, the incidence of diabetes in patients with a high TyG index was significantly higher than that in the other two groups. The same was true for TGs. However, the increase in blood glucose levels in diabetes patients is mainly related to insulin resistance, 35 whereas the increase in blood glucose levels among AMI patients is mainly related to stress state. 36 Diabetes patients may have a higher level of blood glucose when AMI occurs. 37 In this study, the TyG index was a comprehensive index of blood glucose and TG to avoid, to a certain extent, the instability of the prediction value caused by a simple increase in blood glucose levels. 38 The results of this study also confirmed that there was a significant correlation between TyG index and HF occurrence and long-term death among AMI patients with or without diabetes. These results suggest the TyG index is of greater value in patient's prognosis than a single factor.
Following AMI, patients are in a state of stress, and the duration of this state varies, which is also one of the reasons for the increased blood glucose and lipids.39,40 Therefore, patients with high TyG index may have normal baseline blood glucose and lipids, but due to individual reasons, the range of increase in blood glucose and lipids is greater than that of normal people under stress. This high increase in blood glucose and lipids represents a severe inflammatory response in patients following an AMI, leading to a high incidence of poor prognosis. Currently, Tardif et al 41 confirmed that low-dose colchicine could significantly improve the prognosis of patients with AMI by inhibiting the inflammatory response. Therefore, further evaluation of inflammatory state by adding the TyG index on the basis of existing inflammatory indicators has potential value in guiding clinical treatment.
HF is an important cause of poor prognosis among patients with AMI. 42 This study showed that patients with a high TyG index have a significantly high incidence of HF. Myocardial fibrosis is an important pathological process in HF. Excessive fibrosis leads to the limitation of ventricular systolic function and eventually leads to chronic HF. Numerous studies have confirmed that the TyG index is closely related to insulin resistance,43–45 which is closely related to inflammation and extracellular matrix deposition. All of these are important driving factors for the development of fibrosis.46,47 We believe that patients with a high TyG index may have excessive fibrosis because of insulin resistance, eventually leading to HF and poor prognosis. Recent studies have found that the TyG index is closely related to coronary microvascular dysfunction (CMD) and is an independent predictor of major adverse cardiac event among CMD patients with chronic coronary syndrome (CCS). 48 In fact, CMD not only occurs in patients with CCS, but is also closely associated with AMI and HF.49,50 Microthrombus caused by plaque rupture, or atherothrombotic debris formed during PCI, can block microvessels and cause microvascular dysfunction. A high TyG index may indicate microvascular dysfunction in AMI patients, which is also one of the possible reasons for poor prognosis. Further, the TyG index is one of the nutritional status indicators. The baseline data of HF patients showed that patients with a high TyG index had a higher BMI, and obese patients had a relatively high cardiac load over a long period and were more likely to develop decompensated HF after AMI-causing heart injury. 51 This may be the reason for AMI patients with high TyG index being prone to HF. The correlation between the TyG index and HF cannot be drawn based on BNP, LVEF, and other indicators commonly used in clinical practice. 52 However, as a readily available clinical indicator, the TyG index may be of potential value in indirectly improving the prognosis of patients with AMI and guiding the health management of normal individuals. These results suggest the importance of studying classical indicators in clinical practice.
There were several limitations in this study. Firstly, this was a single-center study with possible selection bias in the population. Secondly, the sample size was small. Thus, the results may be partially different from other studies. Thirdly, this study lacked the recovery of the cardiac function of patients during the follow-up. Fourthly, because the groups were grouped according to TyG index, there were differences in variables including diabetes among groups, which may also have an impact on the result. Therefore, increasing the sample size, adding follow-up results, and optimizing the grouping mode in further research is necessary.
Conclusion
Overall, we found a new clinical value for the TyG index, specifically the association of the TyG index with HF in patients with AMI. Further, we found that the long-term prognosis of AMI patients with high TyG index deteriorated significantly.
Supplemental Material
sj-docx-1-cpt-10.1177_10742484231181846 - Supplemental material for The Prognostic Value of the Triglyceride Glucose Index in Patients With Acute Myocardial Infarction
Supplemental material, sj-docx-1-cpt-10.1177_10742484231181846 for The Prognostic Value of the Triglyceride Glucose Index in Patients With Acute Myocardial Infarction by Qian Hao, Zhao Yuanyuan and Chen Lijuan in Journal of Cardiovascular Pharmacology and Therapeutics
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by Zhongda hospital Ethics Committee and registered in the Chinese Clinical Trial Registry (Registration No. ChiCTR2000041071)
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.