
Abstract
Background:
Despite advances in treatments, myocardial infarction (MI) remains a significant cause of morbidity and mortality worldwide. Our team has previously shown that valproic acid (VPA) is cardio-protective when administered to rats post-MI. The aim of this study was to investigate the association of VPA use with post-MI heart failure (HF) development in humans.
Methods:
This study was a random effects meta-analysis of two retrospective case–control studies collected from electronic health record (Michigan Medicine) and claims data (OptumInsight). Cases with an active prescription for VPA at the time of their MI were matched 1:4 to controls not taking VPA at the time of their MI by multiple demographic and clinical characteristics. The primary outcome, time-to-HF development, was analyzed using the Fine-Gray competing risks model of any VPA prescription versus no VPA prescription. An exploratory analysis was conducted to evaluate the association of different VPA doses (≥1000 mg/day vs <1000 mg/day vs 0 mg/day VPA).
Results:
In total, the datasets included 1313 patients (249 cases and 1064 controls). In the meta-analysis, any dose of VPA during an MI tended to be protective against incident HF post-MI (HR = 0.87; 95% CI = 0.72-1.01). However, when stratified by dose, high-dose VPA (≥1000 mg/day) significantly associated with 30% reduction in risk for HF post-MI (HR = 0.70; 95% CI = 0.49-0.91), whereas low-dose VPA (<1000 mg/day) did not (HR = 0.95; 95% CI = 0.78-1.13).
Conclusion:
VPA doses ≥1000 mg/day may provide post-MI cardio-protection resulting in a reduced incidence of HF.
Introduction
According to the American Heart Association (AHA) it is estimated that ∼800 000 Americans have a myocardial infarction (MI) every year. 1 Despite improvements in treatment, within 5 years of their first MI, ∼40% of patients over the age of 45 will die, and 20% will develop heart failure (HF). 1 Risk factors for the development of HF post-MI include increased age, female sex, previous MI, and certain comorbidities. 2 Death and HF post-MI are also directly linked to the extent of myocardial destruction that occurs secondary to the infarction, with larger infarcts conveying a greater risk of mechanical dysfunction and death. 3,4 For decades, rapid reperfusion of the afflicted artery has been a critical component of MI treatment 5,6 due to its ability to reduce final infarct size and improve patient mortality. 7,8 However, it is now known that reperfusion itself can induce damage as well. 9
In a phenomenon known as lethal reperfusion injury (LRI), reperfused myocardial tissue experiences increased oxidative stress, calcium overload, rapid pH correction, inflammation, and dissipation of mitochondrial membrane potential leading to cell death and fibrosis. 9 The impact of LRI is substantial, with estimates of its contribution to final infarct size being close to 40%. 10 To date, treatments aimed at mitigating LRI, or conveying cardioprotection, have had little success in humans. 11,12 It has been hypothesized that this may be due to a narrow focus on individual components of ischemic injury, rather than utilization of a more comprehensive approach. 11 Our research team proposes that inhibition of histone deacetylases (HDACs) could provide such a multi-faceted approach by modifying cardiac gene expression and increasing cell plasticity.
Transcriptional regulation of genes is controlled, in part, through histone modification. Histone acetyltransferases (HATs) acetylate specific lysine residues located on the N-terminal tail of histones, leading to increased transcription. 13,14 Conversely, HDACs deacetylate terminal histone lysines which leads to transcriptional silence. 15,16 HDACs in particular have emerged as potential therapeutic targets due to their influence on numerous cellular pathways. In the setting of cardiovascular disease, animal studies have found that HDAC inhibition decreases inflammation, apoptosis, autophagy, hypertrophy, and fibrosis, leading to improved cardiac contractility. 17 -22 Our study team has recently shown that these effects translate into a ∼50% reduction in infarct size and significant improvements in left ventricular function in rats treated with the HDAC inhibitor valproic acid (VPA) at the time of MI. 23 To our knowledge, no research has investigated the impact of VPA treatment on MI severity or clinical outcomes in a human population. It was our hypothesis that patients taking VPA at the time of MI would have a lower incidence of heart failure post-MI compared to non-VPA treated controls.
Methods
Data Collection
This study was a meta-analysis of two retrospective case–control studies. The first study was conducted utilizing data obtained from the OptumInsight claims database. 24,25 The Clinformatics™ Data Mart Database (OptumInsight, Eden Prairie, MN) is a de-identified database from a large national insurance provider. It includes commercial and Medicare Advantage claims data from ∼83 million insured individuals, including inpatient, outpatient, prescription, geographic and socioeconomic details, and month of death for patients. The initial dataset for this analysis consisted of all patients with a documented MI as identified by corresponding International Classification of Diseases (ICD) 9th and 10th revision codes in the first or second diagnosis position. A list of all utilized ICD codes can be found in the supplement. Data collected included patient birthdate, sex, race, height, weight, body mass index (BMI), tobacco use history, ICD codes for prior diagnoses, medication claims, prior surgeries and procedures, and date of death if applicable. From this initial dataset, patients who had received VPA in the past were identified by the presence of prior claims for “VALPROIC ACID,” “VALPROIC ACID (AS SODIUM SALT),” “VALPROATE SODIUM,” and “DIVALPROEX SODIUM.” Cases were then identified as patients whose MI occurred between a claim for any of the aforementioned VPA keywords and the end of the medication days’ supply for that claim. Comorbidity data was collected by identifying relevant ICD 9 and 10 codes noted in the patient diagnosis list prior to the index date. Time to HF development was defined as the time between the index MI and the first documented ICD code corresponding to a HF diagnosis. Similarly, medication data was collected by using generic medication names to identify relevant medications filled in the 90 days preceding to their MI. Procedure and surgical data was collected by identifying relevant procedure codes and ICD codes for the 30 days surrounding the index MI in order to ensure that procedures occurring during the index hospitalization were not missed. In order to identify matching controls, cases were 1:4 propensity matched against a subset of 100000 randomly selected patients not receiving VPA at the time of their MI. 26 Cases and controls were propensity matched for the baseline characteristics bipolar disorder, epilepsy, gender, race, age, MI type, HF, history of MI, dementia, pulmonary disease (PD), diabetes, renal disease, hypertension (HTN), hyperlipidemia (HLD), atrial fibrillation, valvular disease, index MI treatments (percutaneous coronary intervention [PCI] and Coronary Artery Bypass Graft [CABG]), and prior cardiovascular medication use including beta-blockers, angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARB), statins, mineralocorticoid receptor antagonists (MRA), antiplatelet therapy, loop diuretics, thiazide diuretics, non-dihydropyridines (DHP) and DHP calcium channel blockers (CCB), and digoxin. Patients were excluded from analysis if they had developed heart failure prior to the date of their index MI, or if they were receiving an HDAC inhibitor other than VPA when the MI occurred (vorinostat, romidepsin, belinostat, and panobinostat, etc).
The second dataset was created from electronic health records for ∼4 million patients from Michigan Medicine located in Ann Arbor, MI. DataDirect, a self-serve clinical data tool provided by the University of Michigan, was used to identify potential cases who had a history of MI during a period of VPA use. Once potential cases were identified, manual chart review was utilized to confirm that patients were on VPA at the time of their index MI. A list of confirmed cases and index dates were then provided to the University of Michigan Data Office for Clinical and Translational Research who provided additional data for cases as well as a set of matched controls. Controls were matched 1:4 on age, sex, race, VPA indication (bipolar disorder or epilepsy), and the type of MI (ST-Segment Elevation Myocardial Infarction [STEMI] vs non-ST-Segment Elevation Myocardial Infarction [NSTEMI]). Data was collected in a similar fashion to the OptumInsight dataset, with the exception that comorbid conditions were included if they were documented no later than 15 days after the index date and medications were considered present at baseline if they had been documented in the year prior to the index date. These changes were made to accommodate reporting differences between claims and electronic health record (EHR) data. Key variables, including HF development, VPA dose at the time of MI, type of MI, and presence/absence of PCI were verified using manual chart review. As both datasets created for this study were secondary uses of existing data and de-identified, a waiver of informed consent was approved by the Institutional Review Board at the University of Michigan (approval #HUM00163968). The data includes protected health information and thus it cannot be publicly shared.
Statistical Analysis
Categorical baseline variables are presented as counts and percentages. Continuous baseline variables are presented as median (interquartile range). Baseline variables are presented for the overall patient population in addition to being stratified by the presence or absence of VPA at the time of the index MI. The primary outcome in this study was the time from MI to the development of HF. Patients were censored when they either died, or patient data became unavailable, such as when a patient no longer had insurance coverage through Optum. All remaining patients were censored on the date corresponding to the end of available records in their respective datasets. Categorical variables were compared using the chi-square test (Fisher’s exact test where appropriate). Continuous variables were compared using the Mann-Whitney U test. Time-to-HF analysis was performed using the Fine-Gray competing risks model to account for patients that died during follow-up. 27,28 Classical survival methods are not appropriate to analyze the time-to-event data in a complex situation with competing risks where an individual in the risk set is exposed to more than one cause for a failure. One of the classical methods for analyzing the competing risk data is the proportional hazard (PH) model to examine the effect of covariates on the cause-specific hazard function. The major limitation of using a PH model in a competing risk setup is that during estimation of regression parameters under a specific cause it considers the individuals failing from causes other than the cause of interest as censored observations. To overcome this limitation, Fine and Gray developed a survival regression model based on cumulative incidence function (CIF) which describes the probability of occurring an event prior to a specific time. Unlike PH model, using CIF does not ignore the other competing risks when a specific cause is of interest. 27,28
Variables were selected for inclusion into the model by stepwise selection with entry and stay levels at the P < .15 and P < .05 levels, respectively. Only variables that had complete data for all patients were eligible for entry into the model. Obesity and smoking status were excluded due to poor detection sensitivity. 29,30 Time-to event analyses were performed for both datasets and consisted of the primary analysis investigating the association of any VPA dose on post-MI HF development, as well as an exploratory analysis evaluating the effect of higher VPA doses (≥1000 mg/day) as compared to lower doses (<1000 mg/day), and an absence of VPA (0 mg/day). Given the small number of cases identified, the results of the 2 datasets were then combined in random effects meta-analyses to evaluate the association of any VPA and different dose levels of VPA. The random effects meta-analysis model was chosen over the fixed effect model because it allows the true effect size to differ among studies, 31 and the 2 datasets that we had available for this analysis had different clinical characteristics. Based on our sample size and length of follow-up, we estimated we had 80% power to detect a hazard ratio ≤0.77. All statistical analyses were performed using SAS version 9.4 (Cary, NC).
Results
In total, 1313 eligible patients were identified for analysis consisting of 249 VPA-treated cases and 1064 non-VPA treated controls. The sample size of patients identified in the OpumInsight dataset consisted of 1223 patients (223 cases and 1000 controls). Baseline characteristics of the patients analyzed from the OptumInsight dataset are presented in Table 1. The average patient was 76 (22) years old, white (61.2%), and male (57.9%). The most common comorbidities were hypertension (76%; 925/1223), diabetes (43%; 528/1223), and hyperlipidemia (45%; 553/1223). The cases and controls were relatively well-balanced regarding baseline characteristics with the exception of prior stroke. Obesity and smoking history were also imbalanced, however, claims data has poor sensitivity to identify these variables. 29,30 Regarding the index MI, 42.2% of patients had STEMIs and 11.3% underwent PCI. Overall, in the OptumInsight dataset, 41.0% of patients developed HF, and 21.8% died during the 33 (216) day follow-up period. Significantly more cases than controls died 38.6% versus 18.1% (P < .0001), but cause of death was not available. In comparison, the dataset derived from Michigan Medicine consisted of 90 patients (26 cases and 64 controls; Table 2). The average patient in this dataset was 59 (17) years old, white (100.0%), and male (60.0%). Similar to the OptumInsight dataset, the most common comorbidities were hypertension, hyperlipidemia, and diabetes. There were a number of significantly different baseline characteristics between cases and controls in this dataset including: BMI, type of MI (STEMI vs NSTEMI), bipolar disorder, baseline ACE inhibitor and loop diuretic use, and post-MI catherization. These differences likely arose from post-matching exclusion of patients with prior HF and changes due to manual chart review. In regard to the index MI, 16.7% of patients had a STEMI and 28.9% were treated with PCI. During the median follow-up period of 731 (1399) days, 51.1% of patients developed HF and 47.8% died. In contrast to the OptumInsight dataset, significantly fewer cases than controls died (30.8% [8/26] vs 54.7% [35/64]; P = .040).
OptumInsight Dataset Baseline Characteristics and Outcomes.a

Abbreviations: STEMI, ST-segment elevation myocardial infarction; MI, myocardial infarction; PD, pulmonary disease; ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; MRA, mineralocorticoid receptor antagonist; CCB, calcium channel blocker; PCI, percutaneous coronary intervention; CABG, coronary artery bypass graft surgery; VPA, valproic acid.
aBolded P-values indicate P < .05.
Michigan Medicine Dataset Baseline Characteristics and Outcomes.a
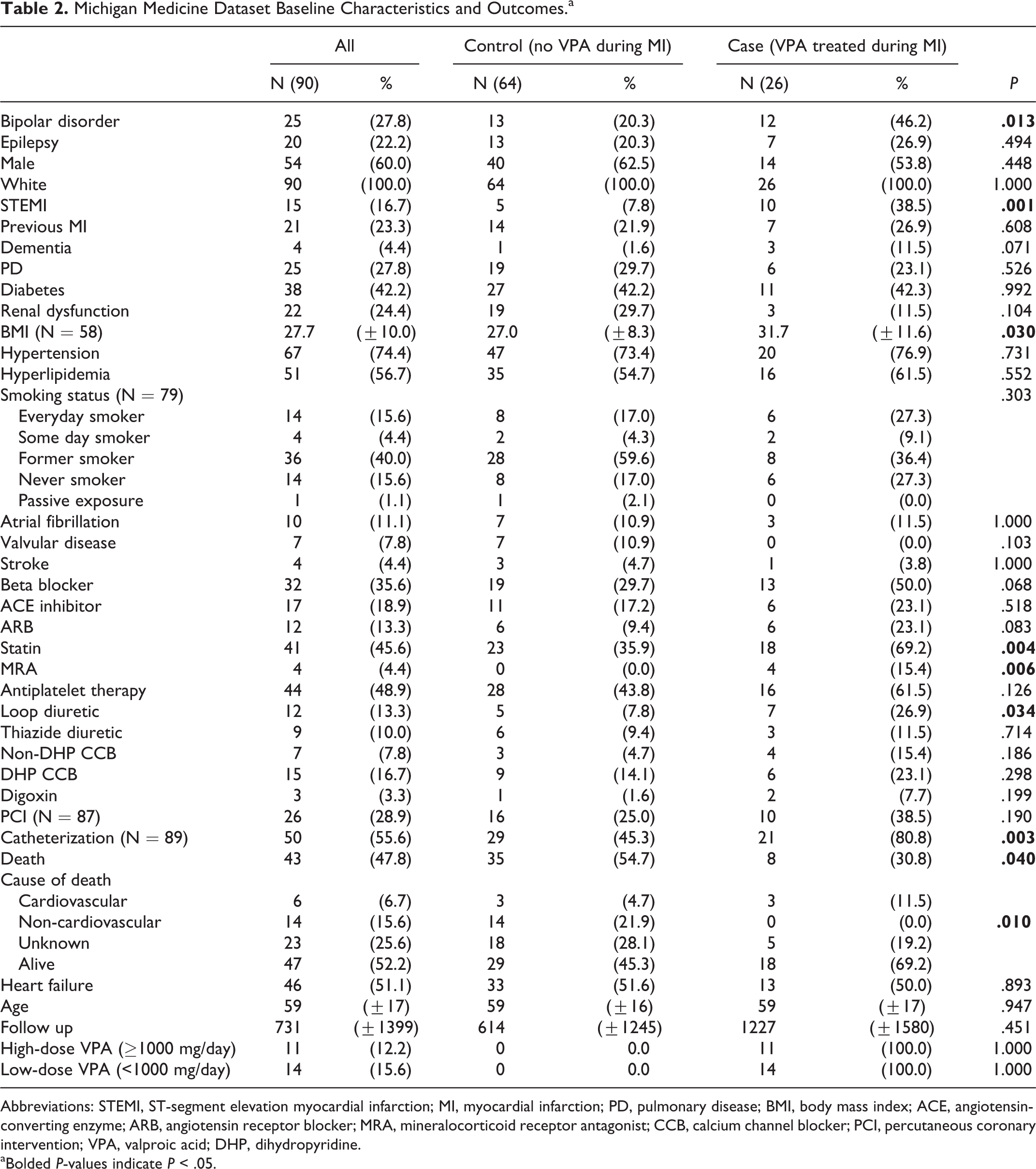
Abbreviations: STEMI, ST-segment elevation myocardial infarction; MI, myocardial infarction; PD, pulmonary disease; BMI, body mass index; ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; MRA, mineralocorticoid receptor antagonist; CCB, calcium channel blocker; PCI, percutaneous coronary intervention; VPA, valproic acid; DHP, dihydropyridine.
aBolded P-values indicate P < .05.
The results from the adjusted Fine-Gray competing risks models for both datasets are displayed in Figure 1 and include the results of the binary (VPA present vs absent) and dose level analyses. Neither of the models in the individual datasets reached the threshold for statistical significance, but the high-dose VPA group trended toward benefit in both datasets: hazard ratios (95% confidence intervals) and P values for high VPA dose in the OptumInsight and Michigan Medicine datasets were 0.72 (0.48-1.08) P = .116 and 0.51 (0.22-1.20) P = .125, respectively. The models were adjusted for variables found to be significant via stepwise selection. For the Michigan Medicine Dataset this included age, sex, race, and diabetes. The OptumInsight dataset was adjusted for age, loop diuretic use, treatment with CABG, PD, hyperlipidemia, diabetes, and MRA use. In the meta-analysis, high-dose VPA ≥1000 mg/day was significantly associated with reduced risk of HF development with a hazard ratio = 0.70 (95% CI: 0.49-0.91). Kaplan Meier curves for time-to-HF and stratified by high-dose, low-dose, and no VPA are displayed in Figures 2 and 3 for each dataset. The logrank P value in the OptumInsight dataset in Figure 2 was near statistical significance (P = .0501), but the logrank P value in the Michigan Medicine dataset in Figure 3 was P = .3988.

Forest plot of HR’s corresponding to any VPA use and stratified by dose (low < 1000 mg/day; high ≥ 1000 mg/day) in the OptumInsight, Michigan Medicine, and combined (meta-analysis) datasets. HR indicates hazard ratio; VPA, valproic acid.
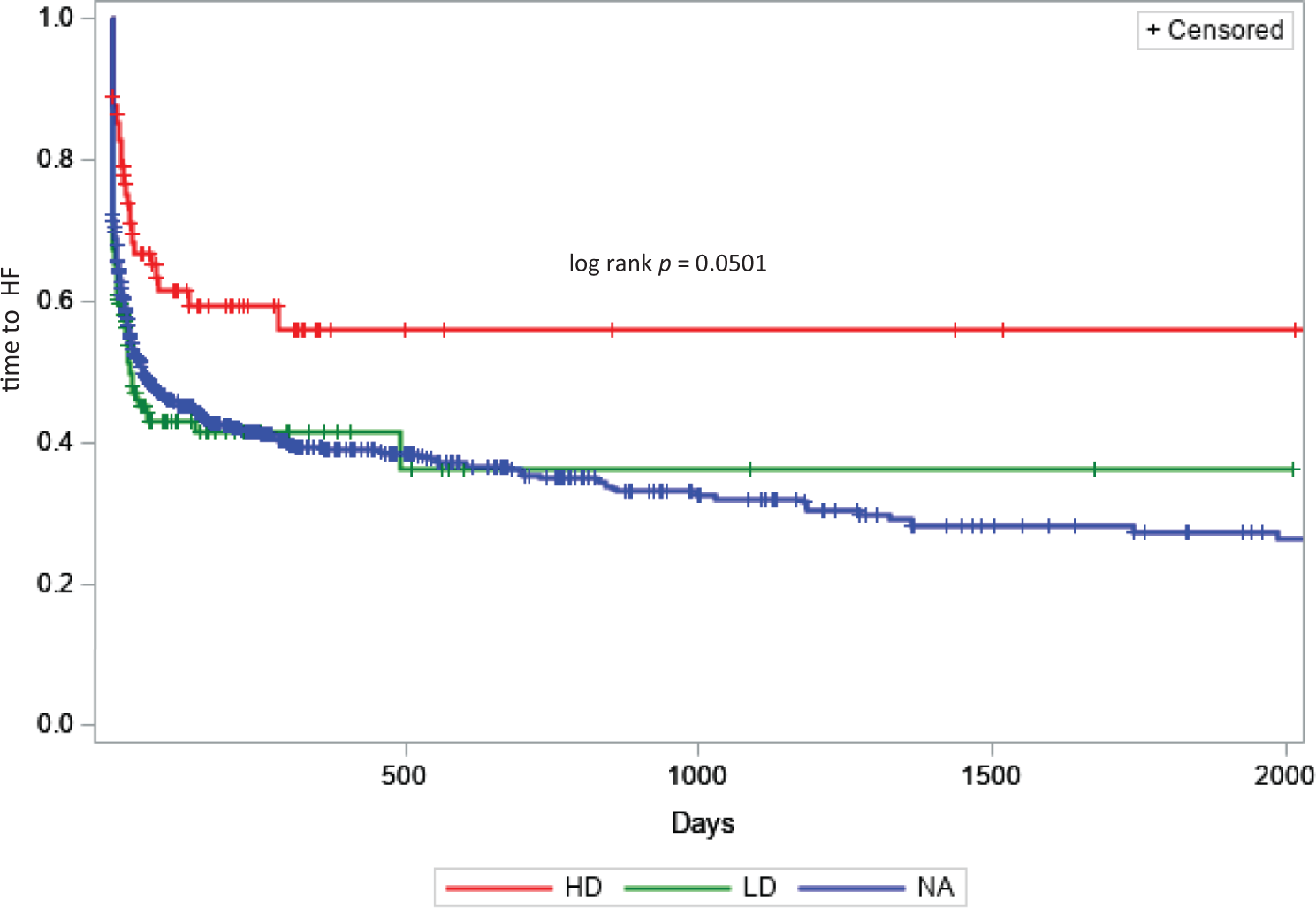
Kaplan-Meier curves for time-to-HF stratified by no VPA treatment (NA; blue), low-dose (LD) VPA (<1000 mg/day; green), and high-dose (HD) VPA (≥1000 mg/day; red) at the time of the MI in the OptumInsight dataset. HF indicates heart failure; VPA, valproic acid; MI, myocardial infarction.

Kaplan-Meier curves for time-to-HF stratified by no VPA treatment (NA; blue), low-dose (LD) VPA (<1000 mg/day; green), and high-dose (HD) VPA (≥1000 mg/day; red) at the time of the MI in the Michigan Medicine dataset. HF indicates heart failure; VPA, valproic acid; MI, myocardial infarction.
Discussion
Our research team previously demonstrated that VPA treatment reduced post-MI infarct size and improved left ventricular function in rats. 23 Therefore, the aim of the present study was to evaluate the association of VPA use with post-MI HF development in humans. VPA use at doses equal to and greater than 1000 mg/day trended toward being protective in 2 independent datasets, and it reached statistical significance in the combined meta-analysis. VPA treatment has also shown benefit in multiple ischemic rodent models targeting other organs, including the lung, 32 kidney, 33,34 and brain. 35 While, to our knowledge, some studies have shown that VPA has the potential to reduce the incidence of MI in epilepsy patients. 36 However, there have been no other studies investigating the use of VPA for the treatment during or after MI occurred in humans, and our findings are in line with those in small animal models. Consistent with the studies in rodents, the analysis of clinical data in the present study shows that VPA’s beneficial effects at the onset of MI in human patients. Long-term efficacy in animals is further supported by a 2007 study by Lee et al in which rats treated with VPA and tributyrin displayed attenuated post-MI ventricular remodeling 37 and a 1997 study in which post-infarction sodium valproate protected left ventricular function. 38 Beyond promoting organ recovery, VPA has also been shown to prolong stimulated tissue plasminogen activator (t-PA) activity in humans by blunting the natural exhaustion of t-PA release. Increased t-PA responses would, in turn, increase endogenous fibrinolytic activity and promote thrombus degradation to reduce the risk of MI recurrence. 39 Our results further demonstrate the long-term effects of VPA on preventing post-MI heart failure in humans.
Potentially related to increased fibrolytic activity, observational studies in humans have associated VPA use with a decreased risk of MI. 36,40 Dregan et al performed a retrospective case–control analysis of EHR for patients diagnosed with epilepsy and prescribed antiepileptic drugs, including 1153 MI cases and 7109 controls. They found a significant association between ever being prescribed sodium valproate with reduced risk for developing an MI (OR = 0.78, 95% CI: 0.67-0.90, P < .001). Patients in the highest quartile of treatment duration had the lowest odds of MI (OR = 0.29, 95% CI: 0.20-0.44, P < .001). 40 Olesen et al collected data for 2 cohorts of patients (n = 53 086 and n = 102 003) with valproate-treated epilepsy and sex- and age-matched controls from the general Danish population by individual-level-linkage of nationwide registries and followed for 10 years. 36 The 2 cohorts comprised patients treated with valproate at baseline and valproate-naïve patients initiating treatment in the study period, respectively. The risk of MI was significantly decreased in both cohorts (HR 0.75, 95% CI: 0.59-0.97 and HR 0.62, 95% CI: 0.53-0.73), and the benefit was significant for both high-dose (>1000 mg daily) and low-dose (≤1000 mg daily) valproate. The results of this meta-analysis indicate that higher dosages of VPA may be required to observe benefit in patients with MIs. Fortunately, short infusions of high-dose VPA are typically well tolerated. A dose escalation study identified doses of up to 140 mg/kg being tolerable, with the dose-limiting side effects being headache and prolonged nausea. 41 Notably, the higher doses did not elicit other signs of VPA toxicity, including lethargy, encephalopathy, respiratory depression, CNS depression, and myoclonus. In addition to these studies by Dregan et al and Olesen et al that indicate VPA treatment can reduce the occurrence of MI, our study also shows short-term and long-term beneficial effects of VPA after MI occurred in humans, suggesting its drug repurposing potential for treating MI and post-MI heart failure.
This study had a number of limitations. First, this is an observational study, which is subject to confounding by treatment, and it is not a randomized controlled trial, which is the gold standard for determining the effectiveness of a drug. However, as this is the first investigation of VPA during an MI in humans, observational data must first be investigated in order to support the progression to a clinical trial. Second, the data was collected retrospectively and predominantly via electronic extraction, making it subject to potentially entry and extraction errors and missing data. We were able to collect most of the risk factors for HF post-MI, 2 but due to the limitations of the datasets available, we were not able to collect all risk factors for HF post-MI. Third, the Michigan Medicine dataset had a number of baseline characteristics that were uneven between the VPA-treated and non-treated groups. This occurred because the dataset was initially intended to evaluate death in addition to heart failure, and matched accordingly when the data was received. Unfortunately, upon receiving the data it became clear that time to death would not be an appropriate endpoint due to a lack of attributable cause in the OptumInsight data set, and combination of significant non-cardiovascular death and missing death data in the Michigan Medicine data set. Further, we felt that the significant association between epilepsy, bipolar disorder, and mortality 42 -44 could cause confounding of the death outcome by indication, despite our attempts to match the cases and controls by VPA indication to the best of our ability. Despite these unbalanced variables, stepwise selection did not identify any of the mismatched variables as significant. A fourth limitation was a significant underreporting of BMI and smoking status data in the OptumInsight dataset due to low sensitivity of ICD codes to identify these variables in claims databases. 29,30 Of note, the 2 datasets were composed of 2 different patient populations with the OptumInsight dataset being significantly older, having a higher proportion of STEMIs to NSTEMIs, a lower proportion of PCI, and a much shorter follow up period. Despite these differences, the results of the Fine-Gray competing risks models were similar across the 2 studies. The 2 most common indications for VPA are bipolar disorder and epilepsy, which is why we matched cases and controls by those 2 indications. However, VPA can also be used to treat other neurologic conditions, such as chronic headaches and migraines, and the proportion of patients taking VPA for indications other than bipolar disorder and epilepsy was larger than we initially expected. Therefore, an additional limitation of our study is that we only matched cases and controls based on the indications of bipolar disorder and epilepsy, and patients treated with high-dose VPA were more commonly taking VPA for bipolar and epilepsy than the patients treated with low-dose VPA (Supplemental Tables 1 and 2). Evidence shows that risk of adverse clinical outcomes after MI differs among mental illnesses. 45 Although this study provides potential insight into the required VPA dose for effective treatment of MI, it also leaves additional questions. Future studies should consider the timing of VPA administration relative to the MI, as patients in this study were already on VPA at the time of their infarction. This study also did not assess how long VPA treatment was continued post-MI, or whether VPA treatment was interrupted during hospitalization.
Supplemental Material
Supplemental Material, sj-docx-1-cpt-10.1177_10742484221140303 - Association of Valproic Acid Use With Post-Myocardial Infarction Heart Failure Development: A Meta-Analysis of Two Retrospective Case–Control Studies
Supplemental Material, sj-docx-1-cpt-10.1177_10742484221140303 for Association of Valproic Acid Use With Post-Myocardial Infarction Heart Failure Development: A Meta-Analysis of Two Retrospective Case–Control Studies by Joseph D. English, Shuo Tian, Zhong Wang and Jasmine A. Luzum in Journal of Cardiovascular Pharmacology and Therapeutics
Footnotes
Author Contributions
Conceptualization: JAL, ST, and ZW; Formal analysis: JDE and JAL; Investigation: JDE and JAL; Methodology: JDE and JAL; Writing—oringinal draft: JDE and JAL; Writing—review and editing: JDE, JAL, ST, and ZW.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: University of Michigan MCube3.0 grant #U064172 (JAL and ST); NHLBI grant #K08HL146990 (JAL); NHLBI R01HL139735(ZW).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.