
Abstract
Background:
Because of logistic challenges associated with the COVID-19 pandemic, direct oral anticoagulants (DOAC) were favored over warfarin in patients presenting postoperative atrial fibrillation (AF) after cardiac surgery in our institution. Considering the limited evidence supporting the use of DOAC in this context, we sought to evaluate the safety and efficacy of this practice change.
Methods:
A retrospective study was performed with patients from the Quebec City metropolitan area who were hospitalized at the Institut universitaire de cardiologie et de pneumologie de Québec-Université Laval following cardiac surgery and who required oral anticoagulant (OAC) for postoperative AF. The primary objective was to compare the pre- and peri-COVID-19 period for OAC prescribing patterns and the incidence of thrombotic and bleeding events at 3 months post-surgery. The secondary objective was to compare DOAC to warfarin in terms of thrombotic events and bleeding events.
Results:
A total of 233 patients were included, 142 from the pre-COVID-19 and 91 from the peri-COVID-19 period, respectively. Both groups had equivalent proportions of preoperative AF (48%) and new-onset postoperative AF (52%). The proportion of patients treated with a DOAC increased from 13% pre-COVID-19 to 82% peri-COVID-19. This change in practice was not associated with a significant difference in the incidence of thrombotic or bleeding events 3 months postoperatively. However, compared to DOAC, warfarin was associated with a higher incidence of major bleeding. Only 1 thrombotic event was reported with warfarin, and none were reported with DOAC.
Conclusion:
This study suggests that DOAC are an effective and safe alternative to warfarin to treat postoperative AF after cardiac surgery and that this practice can be safely maintained.
Keywords
Introduction
Atrial fibrillation (AF) in a postoperative context of cardiac surgery refers to both patients affected preoperatively and those newly affected postoperatively. The incidence of new-onset postoperative atrial fibrillation (POAF) is approximately 17% to 33% after coronary artery bypass grafting surgery (CABG), 33% to 49% after heart valve replacement, and up to 60% after cardiac surgery combining a valve procedure and CABG. 1,2 Following CABG, POAF is independently associated with an increased hospital stay, an increased incidence of cerebral thromboembolic events, an increased risk of developing long-term AF, and increased mortality. 3 -6 Patients with preoperative AF are 3 times more likely to have postoperative AF and are at higher risk of a long hospital stay and long-term mortality compared to patients without AF. 7 The prevalence of preoperative AF is estimated at 28%. 8 Bleeding is also a major complication following CABG. 9 Some evidence indicates that the use of an anticoagulant after cardiac surgery may predispose patients to delayed pericardial effusion and even cardiac tamponade. 10 -13
Despite the significant thrombotic complications associated with AF in a postoperative context, guidelines offer few recommendations to prevent these events due to the lack of high-quality clinical evidence, particularly randomized controlled trials. 14 -18 Prior to the recent arrival of direct oral anticoagulants (DOAC), warfarin, a vitamin-K antagonist, was the only oral anticoagulant (OAC) available to treat AF in the post-cardiac surgery context and is currently the standard treatment for this condition, although the evidence supporting its use is limited and heterogeneous. 19 The use of DOAC for AF in this post-cardiac surgery context is poorly documented. The only clinical evidence available consists of observational or pilot studies, 20 most of which excluded patients with preoperative AF. However, the safety and efficacy of DOAC are superior to warfarin for the treatment of AF outside of the post-operative context. 21
Since the start of the SARS-CoV-2 (COVID-19) pandemic in 2020, DOAC have been prescribed more widely for AF post-cardiac surgery at the Institut universitaire de cardiologie et de pneumologie de Québec-Université Laval (Quebec Heart and Lung Institute, IUCPQ-UL). It is therefore important to confirm that DOAC are indeed a suitable alternative. The main objectives of this study were to compare the pre- and peri-COVID-19 period for OAC prescribing patterns and the incidence of thrombotic and bleeding events. The secondary objective was to compare DOAC to warfarin in terms of thrombotic and bleeding events.
Methods and Materials
Design and Patients
The IUCPQ-UL is a tertiary hospital in the province of Quebec, Canada, with a large cardiac surgery department. We performed a single-center, retrospective cohort study with patients aged 18 years and older from the Quebec City metropolitan area who were hospitalized at IUCPQ-UL following cardiac surgery and who required OAC for AF in a postoperative context, between January 1, 2019 and March 1, 2021. The analysis included postoperative events that occurred up to within 3 months of cardiac surgery.
The present study included Quebec City metropolitan area patients aged 18 and over who had heart surgery at the IUCPQ-UL between January 1, 2019 and March 1, 2021 and who required OAC for AF in a postoperative context. The pre-COVID period corresponded to the period prior to March 11, 2020, which is the date that the global pandemic was announced by the World Health Organization. 22 Patients on OAC for preoperative AF or flutter were included. Atrial flutter will be included in the term AF, since its management and complications are very similar. 16 The exclusion criteria corresponded to indications for which DOAC are not recommended or poorly studied: the implantation of a mechanical prosthetic heart valve, the implantation of a biological mitral or replacement tricuspid valve, heart transplantation, ventricular thrombus, antiphospholipid syndrome, or postoperative heparin-induced thrombocytopenia. 14,18 Transcatheter aortic or mitral valve implantation, thoracic endovascular aortic repair, patients with implantation of a left ventricular assist device and extracorporeal membrane oxygenation are other exclusions. The study sample consisted of a consecutive series of patients who met the eligibility criteria during the data collection period.
This project was approved by the research ethics committee of the IUCPQ-UL and the CHU de Québec-Université Laval.
Variables
Data on patient demographics, medical comorbidities, operative characteristics, concomitant medication at discharge (antiplatelet agents, proton pump inhibitor, therapeutic parenteral anticoagulation), discharge anticoagulants and outcomes was extracted from the existing IUCPQ-UL cardiac surgery database or via the electronic patient record of the IUCPQ-UL and the CHU de Québec-Université Laval. Postoperative AF was defined as AF/flutter requiring cardioversion or AF on a rhythm strip or cardiac telemetry. The patient with AF had to be discharged with an OAC to be included. Data on baseline thrombotic risk and bleeding risk according to the CHADS2-VASc score and modified HAS-BLED score (excluding alcoholism, labile international normalized ratio [INR] and drugs except antiplatelet drugs) was collected.
Outcomes
The 2 primary outcomes identified for our analysis included thrombotic events and bleeding events during hospitalization and up to 3 months postoperatively. A thrombotic event was defined as one of the following events: stroke, transient ischemic attack (TIA), biological aortic valve thrombosis, systemic arterial embolism, pulmonary embolism or deep vein thrombosis. Bleeding was defined as any type of bleeding complication: hematuria, hemoptysis, pericardial effusion, tamponade, hemothorax, intracranial, intraspinal, intraocular, retroperitoneal, intra-articular bleeding, intramuscular bleeding with compartment syndrome, or other bleeding. Other collected information, such as a drop in hemoglobin, number of blood transfusions, surgical hemostasis, use of vasoconstrictor amines, and bleeding-related death were necessary to categorize the bleeding severity according to the recognized classifications of the International Society on Thrombosis and Haemostasis (ISTH) and Bleeding Academic Research Consortium (BARC). 23,24 The BARC type 4 bleeding definition was slightly modified to fit existing data in the cardiac surgery database. A BARC 4 event was defined as perioperative intracranial bleeding within 24 hours; reoperation after closure of sternotomy for the purpose of controlling bleeding; transfusion of 5 units of whole blood or packed red blood cells within a 48-hour period; or chest tube output of 2 liters within a 48-hour period.
Statistics Analysis
Continuous variables were presented as mean ± standard deviation, and categorical variables were presented as numbers and percentages. Continuous variables were analyzed using one-way ANOVA. For some variables, the one-way ANOVA was performed on separate residual variances in each group, as the effect that specifies heterogeneity in the covariance structure was significant (heteroscedasticity) compared to the same variance between groups. The Satterthwaite’s degree of freedom statement was added for variables analyzed using unequal variance structures. The normality assumption was verified with the Shapiro-Wilk test on residuals from the statistical model. The Brown and Forsythe’s variation of Levene’s test statistic was used to verify the homogeneity of variances. Categorical variables were analyzed with Fisher’s exact test. Univariable and multivariable logistic regressions were performed to determine independent predictors of receiving warfarin. Continuous variables were checked for the assumption of linearity in the logit using graphical representations. The final model was selected based on the smallest Akaike’s criterion. Analyses were considered statistically significant with P value less than 5%. Analyses were performed using SAS version 9.4 (SAS Institute Inc, Cary, NC).
Results
Patients and Operative Characteristics
The study period included a total of 5372 cardiac surgeries, 3615 of which were performed in the pre-COVID-19 period and 2113 performed in the peri-COVID-19 period. A total of 233 patients meeting the inclusion and exclusion criteria received an OAC for AF in the post-cardiac surgery context. There were 142 patients in the pre-COVID-19 period and 91 in the peri-COVID-19 period. The mean age was 71 for the pre-COVID-19 group and 70 for the peri-COVID-19 group. CABG was the most frequent cardiac surgery, performed in around 50% of patients in both groups. Bioprosthetic aortic valve replacement (AVR) or pulmonary valve replacement (PVR) represented approximately 30% of the surgeries (Supplemental Appendix 1). The majority of the surgeries were elective. The proportion of preoperative AF (48%) was similar to that of new-onset postoperative AF (52%). The mean CHA2DS2-VASc score and modified HAS-BLED score was 3.5 and 2.8 for the pre-COVID-19 period and 3.6 and 2.9 for the peri-COVID-19 period, respectively. Almost all patients had concomitant antiplatelet and gastroprotective medication. All baseline characteristics were similar for the 2 groups, except for bleeding events before OAC initiation, which was driven by more perioperative BARC 4 bleeding events (Table 1). There were more BARC 4 bleeding events in the peri-COVID-19 period than in the pre-COVID-19 period (9% vs <1%, P = .003). There were 3 strokes before OAC initiation in the pre-COVID-19 period and none in the peri-COVID-19 period.
Baseline Characteristics.
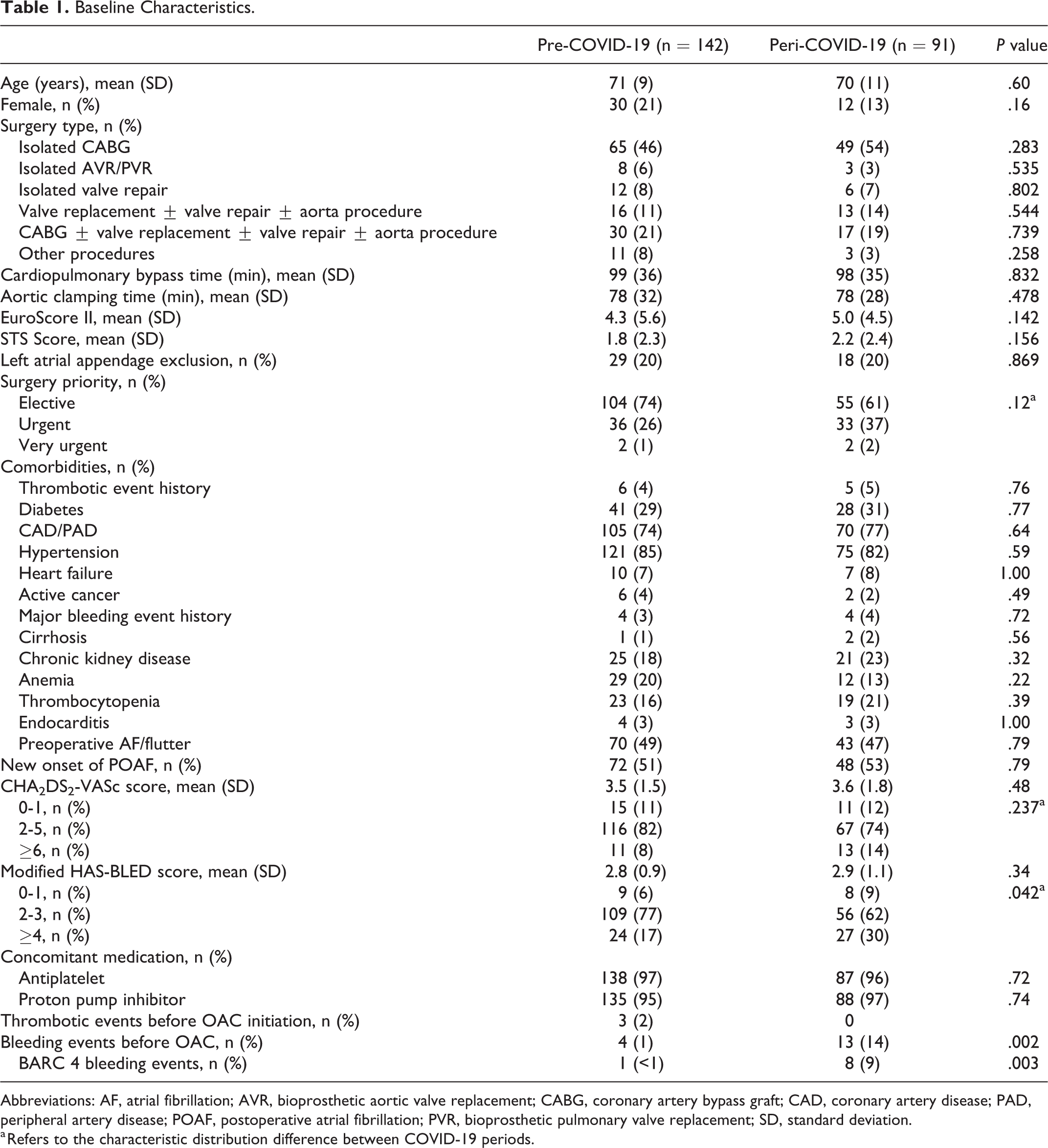
Abbreviations: AF, atrial fibrillation; AVR, bioprosthetic aortic valve replacement; CABG, coronary artery bypass graft; CAD, coronary artery disease; PAD, peripheral artery disease; POAF, postoperative atrial fibrillation; PVR, bioprosthetic pulmonary valve replacement; SD, standard deviation.
a Refers to the characteristic distribution difference between COVID-19 periods.
Prescription Pattern of Anticoagulant Therapy
In the pre-COVID-19 period, 87% and 13% of patients were discharged on warfarin and DOAC, respectively (Table 2). In the peri-COVID-19 period, these proportions were reversed, with 18% and 82% of patients discharged on warfarin and DOAC, respectively. In this period, only 13% of patients with preoperative OAC were changed from DOAC to warfarin, and 80% continued their DOAC. Independent of the COVID-19 period, apixaban (24%) and rivaroxaban (14%) were prescribed more frequently than dabigatran (0.9%) and edoxaban (1%). DOAC were initiated significantly further from surgery than warfarin was (7.0 ± 6.1 days vs 3.6 ± 2.0 days, P < .0001) independent of the COVID-19 period, but there was no difference in the proportion of therapeutic parenteral use before OAC initiation or in the delay of parenteral anticoagulation initiation (mean: 4 days) after surgery between the groups.
Prescription Patterns of Anticoagulants for AF in the Post-Cardiac Surgery Context.

Abbreviations: AF, atrial fibrillation; DOAC, direct oral anticoagulant; OAC, oral anticoagulant; SD, standard deviation.
a Refers to the characteristic distribution difference between COVID-19 periods.
Based on multivariate analysis, patients with baseline hemoglobin <110 g/L were associated with a 4-fold increased risk of being discharged on warfarin (OR 4.04, 95% CI 1.67-9.76). Patients with coronary or peripheral vascular disease were less likely to have been discharged on warfarin (OR 0.48, 95% CI 0.23-0.998). A similar tendency was also observed in patients with platelet levels <150 000/mm3 and in urgent procedures (OR 0.49, 95% CI 0.24-1.01; OR 0.56, 95% CI 0.30-1.07).
Outcomes
During the study period, only 1 thrombotic event occurred in a patient while on OAC. This patient had a stroke while on warfarin. His elective cardiac surgery (mitral valve repair + AVR + aorta replacement) was done during the pre-COVID-19 period. The patient had preoperative AF, and his CHA2DS2-VASc score was 2.
During the study period, bleeding episodes on OAC occurred in 14 patients (10%) in the pre-COVID-19 period and 6 patients (7%) in the peri-COVID-19 period, respectively (Table 3). More major bleeding episodes tended to occur in the pre-COVID-19 period when reported on the ISTH and BARC type 3A scale.
Incidence of Thrombotic Events and Bleeding Events on OAC.

Abbreviations: BARC, Bleeding Academic Research Consortium; CRNMB, clinically relevant non-major bleeding; ISTH, International Society on Thrombosis and Haemostasis; OAC, oral anticoagulant.
Independent of the COVID-19 period, significantly more patients experienced bleeding on warfarin compared to DOAC (17 vs 3 events, P = .017) and the bleeding events were more severe (BARC 3B: 7 vs 0 events, P = .044; Major ISTH: 9 vs 0 events, P = .012) (Table 4). The median time between surgery and bleeding event was 16 days (IQR 16) on warfarin and 14 days (IQR 2.5) on DOAC. Forty-one percent of patients who experienced bleeding events on warfarin needed to be hospitalized, while none on DOAC required hospitalization. There were 6 pericardial effusion/tamponade bleeding events, all of which occurred on warfarin at a median time of 10.5 days after surgery. Only 1 major bleeding episode according to BARC and ISTH classifications (BARC 3A gastrointestinal bleeding) occurred with DOAC (rivaroxaban). Further information regarding bleeding outcomes or bleeding events is provided in Table 3, Table 4 and Supplementary Appendix 2.
Baseline Characteristics and Outcome Comparisons Between Warfarin and DOAC Independent of COVID-19 Period.
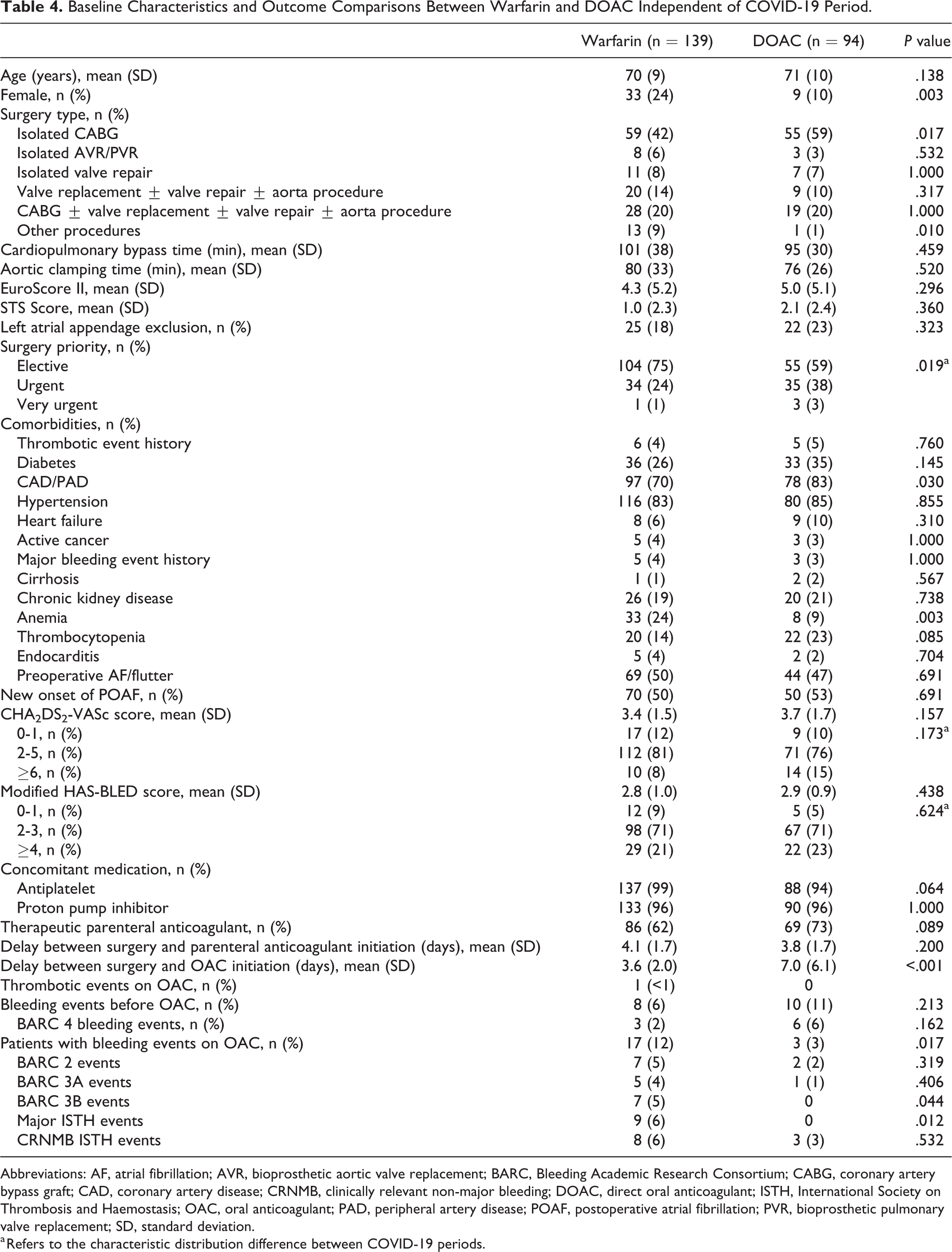
Abbreviations: AF, atrial fibrillation; AVR, bioprosthetic aortic valve replacement; BARC, Bleeding Academic Research Consortium; CABG, coronary artery bypass graft; CAD, coronary artery disease; CRNMB, clinically relevant non-major bleeding; DOAC, direct oral anticoagulant; ISTH, International Society on Thrombosis and Haemostasis; OAC, oral anticoagulant; PAD, peripheral artery disease; POAF, postoperative atrial fibrillation; PVR, bioprosthetic pulmonary valve replacement; SD, standard deviation.
a Refers to the characteristic distribution difference between COVID-19 periods.
There was a significant difference in emergency room consultations not related to bleeding or thrombotic events, but not a significant difference in hospitalizations, between the pre-COVID-19 and the peri-COVID-19 period (Supplementary Appendix 3).
Discussion
This retrospective study describes an important change in the OAC prescription pattern in our healthcare facility since the beginning of the COVID pandemic. Even though increases in DOAC use are consistent with updates guidelines recommending DOAC’s over warfarin therapy in AF in the years leading up to COVID-19, it was important to confirm that this practice was safe in a postoperative context of cardiac surgery. The proportion of patients treated with a DOAC increased from 13% in the pre-COVID-19 period to 82% in the peri-COVID-19 period. This increase is consistent with data from the Society of Thoracic Surgeons registry from showing a significant proportion of patients being discharged with a DOAC for AF after CABG since 2011. 25 In the study period, we found no difference between time periods in terms of thrombotic (1 vs 0 events) or bleeding events (7% vs 10%, P = .476) in patients on OAC. Independent of the COVID-19 period, significantly more patients experienced bleeding on warfarin compared to DOAC (12% vs 3%, P = .017), and more major bleeding events occurred (BARC 3B: 7 vs 0 events, P = .044; Major ISTH: 9 vs 0 events, P = .012).
The COVID-19 pandemic also impacted the ability of healthcare facilities to perform surgeries. In this study, there was a 25% reduction in the number of cardiac surgeries at the IUCPQ-UL during the peri-COVID-19 period, although there was no difference in surgery priority. This outcome is different from that of an Ontario cohort study by Tam and colleagues, who reported that patients referred for CABG procedures during the pandemic period were more likely to be urgent patients presenting with an acute coronary syndrome. They found that referral to cardiac surgery during the pandemic period was a significant predictor of increased all-cause mortality for CABG (HR 1.96, 95% CI 1.28-3.01) but not for surgical valve referrals. 26 In our study, baseline characteristics including comorbidities were comparable between the periods, which is similar to the Ontario study. We reported more BARC 4 bleeding events in the peri-COVID-19 period, which might indicate a population with a higher bleeding risk despite no differences in surgical priority, comorbidities, cardiopulmonary bypass time, aortic clamping time, STS score, Euroscore II, mean CHA2DS2-VASc score or modified HAS-BLED score between the 2 periods.
In our study, isolated CABG was the most prevalent surgery and accounted for 49% of total cardiac surgeries, while 30% and 19% of cardiac surgeries included a bioprosthetic AVR/PVR or a mitral/tricuspid valve repair procedure, respectively. The use of DOAC within the 3-month post-cardiac-surgery period is poorly documented, as all major randomized controlled trials evaluating DOAC in AF exclude AF in the post-cardiac surgery context. There is also scarce data on the use of DOAC use in patients with bioprosthetic AVR, since few of them were included in these studies. 27 International guidelines give divergent recommendations for anticoagulation for AF in the post-cardiac surgery context. The 2020 CCS AF guidelines suggest a DOAC in preference to warfarin in the absence of a recent cardiac surgery (<3 months). 14 The AHA/ACC guidelines for the management of patients with valve disease mention that it is reasonable to administer antithrombotic medication to patients who develop postoperative AF, as is advised for non-surgical patients. A vitamin-K antagonist is recommended for 3 to 6 months after a bioprosthetic aortic valve replacement. They do not give any recommendations on DOAC in this context. 18 The ESC/EACTS guidelines to manage valvular diseases mention that DOAC should be considered over warfarin after 3 months following the surgical implantation of a bioprosthetic heart valve in patients with AF. 28 Two large retrospective cohort studies compared DOAC to warfarin after CABG or valve surgery. 29,30 Nauffal and colleagues did not find any association between anticoagulant type and 30-day major bleeding complications (OR 0.76, 95% CI 0.49-1.18), stroke/TIA (OR 0.94, 95% CI 0.53-1.67), all-cause mortality (OR 1.08, 95% CI 0.80-1.45) and pericardial effusion/tamponade (OR 1.09, 95% CI 0.80-1.47). 30 Beller and colleagues found no difference in 30-day reoperation for bleeding (OR 0.79, 95% CI 0.49-1.28), mortality (OR 1.94, 95% CI 0.84-4.49) or pericardial effusion requiring pericardiocentesis (0.3% vs 0.3%). 29 Our overall observed bleeding rate is comparable to or lower than what is reported in these studies; however, these studies overall are consistent with ours, since they also had reassuring outcomes for the use of DOAC post-cardiac surgery. Our study is complementary, as we included patients who experienced in-hospital postoperative stroke/TIA or major bleeding complications, patients with preoperative AF, and reported OAC timing of initiation. Prevalence of valve intervention in patients with DOAC was high in both studies (31.7%) and (53.9%) as in ours (38%). 29,30 Although data supporting the premature use of DOAC (<3 months) after a biological aortic valve intervention is lacking, our study shows encouraging safety outcomes that are in keeping with the findings in the literature. 20
Significantly more patients had clinically relevant bleeding events on warfarin compared to DOAC, but it is important to note that bleeding outcomes on OAC were recorded starting from OAC initiation. Our bleeding rate on warfarin compared to DOAC is much higher than the rate reported in a meta-analysis of randomized controlled trials in AF. 21 Patients in the warfarin group may have been at increased risk for bleeding at baseline given greater incidence of anemia at baseline. In our study, DOAC were initiated significantly further from surgery compared to warfarin (7.0 vs 3.6 days, P = <.0001), which could be explained by warfarin longer onset of action and the limited access of DOAC antidote in Canada. The median time of surgery to bleeding event was 16 days on warfarin and 14 days on DOAC, with no difference in bleeding events before OAC between the groups. Furthermore, there was no difference in the proportion of therapeutic parenteral use before OAC initiation and in the mean delay of parenteral anticoagulation initiation (4 days) after surgery between the groups. In our study, there were 6 pericardial effusion/tamponade bleeding events, all of which occurred on warfarin at a median time of 10.5 days after surgery. Yu and colleagues’ results differed from ours, as they reported more invasive procedures for pleural or pericardial effusion (26.6% vs 13.2%, P = <.014) in patients who were anticoagulated with DOAC vs warfarin after CABG. Interestingly, the median time of initiation of DOAC and warfarin was earlier, on postoperative day 4 and day 3, respectively. 11 The incidence of delayed pericardial effusion/tamponade timing in our study, or 2 weeks after cardiac surgery, is consistent with the literature. 31,32 Apixaban was favored at our institution due to local practices and safety data in AF. 21
Even though there were no thrombotic events in the DOAC group and only 1 on warfarin, our study did not have the statistic power required to assess this outcome. However, there was no signal of increased risk when patients were discharged on DOAC, which is consistent with a meta-analysis of randomized controlled trials in non-valvular AF, in which DOAC demonstrated a significant reduction in stroke vs warfarin. 21
Our study has several limitations. In terms of internal validity, its retrospective nature can lead to information bias. Although the electronic patient records at the CHU-Université Laval and the IUCPQ-UL provided postoperative events for the entire Quebec City metropolitan area, a slight underestimation in the number of events is possible if patients consulted outside of but near this region. The COVID-19 pandemic might also have caused an underestimation of primary outcome events or deaths in the peri-COVID-19 group, since fewer patients in our study went to emergency rooms during the peri-COVID-19 period for non-related thrombotic or bleeding events, probably out of fear of the virus. However, there was no significant difference in the hospitalization rate between the COVID-19 periods. As for therapeutic adherence, the INR (warfarin) and the dose administered (DOAC) were not measured in our study; an overestimation of bleeding episodes therefore remains possible if any patients were not adhering to INR monitoring or were receiving an inadequate dose. However, at our center, patients discharged on warfarin are closely monitored at the anticoagulation therapy clinic for at least 1 month, which reduces the risk of extreme INR values. Once stabilized, patient’s follow-up was transferred to their community pharmacy. Regarding external validity, the fact that these cardiac surgeries were performed at a single center may reduce the generalization of these results, as surgical practices may vary from center to center. The exclusion of patients from outside the Quebec City metropolitan area may limit how these findings can be generalized to rural communities due to comorbidities and demographic discrepancies.
Conclusion
DOAC have been prescribed more widely for AF after cardiac surgery at our center during the COVID-19 pandemic that started in 2020. We found that more DOAC prescriptions in the peri-COVID-19 period were not associated with worse outcomes in our cohort. It therefore appears safe to maintain this clinical practice in the future. Our study stands out from other retrospective studies as we included preoperative AF, intrahospital events, biological AVR and PVR surgeries, reported timing of OAC initiation after surgery, and baseline bleeding risk. Even though our results are promising and consistent with other studies, randomized controlled trials are needed to confirm these observations. Interestingly, 4 randomized controlled trials evaluating anticoagulation after cardiac surgery are in progress 33 -36 and 3 are comparing DOAC to warfarin. 34 -36
Supplemental Material
Supplemental Material, sj-docx-1-cpt-10.1177_10742484221128124 - Impact of COVID-19 on the Prescribing Pattern of Oral Anticoagulants for Atrial Fibrillation After Cardiac Surgery
Supplemental Material, sj-docx-1-cpt-10.1177_10742484221128124 for Impact of COVID-19 on the Prescribing Pattern of Oral Anticoagulants for Atrial Fibrillation After Cardiac Surgery by Dannick Brochu, Amélie St-Arnaud, Louis-Étienne Marchand, Pierre Voisine and Julie Méthot in Journal of Cardiovascular Pharmacology and Therapeutics
Footnotes
Authors’ Note
This project was approved by the research ethics committee of the IUCPQ-UL and the CHU de Québec-Université Laval.
Acknowledgments
Special thanks to Serge Simard, Sébastien Perreault, Stéphanie Dionne, Sophie Proulx, Maude Dansereau, and Ariane Croteau for their invaluable contributions to this project.
Author Contributions
Amélie St-Arnaud and Louis-Étienne Marchand contributed equally to the manuscript. All authors contributed to the study concept and design. Dannick Brochu and Serge Simard were responsible for data acquisition and statistical analysis. Dannick Brochu wrote the initial manuscript draft. All authors provided a critical review of the manuscript and approved of revision. All authors approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.