
Abstract
Introduction:
The Veterans Health Administration (VHA) provides multidisciplinary team-based care with peer-to-peer support for diabetes and obesity, but not for most heart diseases.
Objective:
To inform disease-care models, assess physical and psychological functioning in veterans with, or at high risk of, heart disease.
Methods:
Retrospective, cross-sectional cohort analysis of data from the National Survey on Drug Use and Health, 2015-2019, based on standard measures of functioning: self-rated health, serious psychological distress, and high-risk substance use. Cohorts were veterans with respondent-reported heart disease, or at high risk of cardiovascular disease based on age/comorbidity combinations (HD/risk); nonveterans with HD/risk; and veterans without HD/risk. Ordinal logistic regression models adjusted for demographics, social determinants of health, and chronic conditions. A priori alpha was set to 0.01 because of large sample size (N = 28,314).
Results:
Among those with HD/risk, veterans (n = 3,483) and nonveterans (n = 16,438) had similar physical impairments, but distress trended higher among veterans (adjusted odds ratio = 1.36, 99% confidence interval [CI] = 0.99-1.86). Among those with comorbid HD/risk and behavioral health problems, regression-adjusted treatment rates were similar for veterans and nonveterans with psychological symptoms (55.9% vs. 55.2%, respectively, P = 0.531) or high-risk substance use (18.7% vs. 19.4%, P = .547); veterans were more likely to receive outpatient mental health treatment (36.1% [CI = 34.4%-37.8%] vs. 28.9% [CI = 28.2%-29.6%]).
Conclusion:
An upward trend in distress among veterans compared with nonveterans with HD/risk was not explained by differences in behavioral health treatment utilization. Further research should test multidisciplinary team-based care for veterans with HD/risk, similar to that used for other chronic diseases.
Keywords
Introduction
Of chronic diseases affecting an estimated 6 in 10 United States (US) adults, cardiovascular disease (CVD) is among the most prevalent. 1,2 A well-documented bidirectional association between CVD and stress-related mental disorders 3 -7 has potentially important implications for physical and mental functioning. These implications include markedly elevated risks of CVD morbidity and mortality in patients with concomitant CVD and mental illness. 8 -12
Military veterans are an important population in which to measure impairments in physical and mental functioning associated with chronic illness, including CVD and risk factors for CVD. Compared with the US civilian population, veterans are at higher risk of poor physical and mental health and have higher rates of CVD and diabetes. 7,13 -17 Veterans are also more likely than civilians to have been exposed to post-traumatic stress disorder (PTSD); obesity and obesity-related conditions; and, for Persian Gulf and later veterans, environmental contaminants. 14,18 -21 Thus, they may face greater risks of comorbidity and mortality related to CVD and CVD risk factors than civilian populations do.
Despite these associations between military service and risk factors for adverse effects of chronic diseases, diabetes was associated with similar physical and psychological impairments in veterans and nonveterans in a previous cross-sectional retrospective analysis of national survey data. 15 Additionally, among those with diabetes, veterans had equivalent or slightly better functioning, defined using standard measures and diagnostic criteria, than did nonveterans. 15 The authors of that study noted that the multidisciplinary team-based care models used by the Veterans Health Administration (VHA) for diabetes and obesity, which include extensive peer-to-peer support and holistic care management, 22 -24 might explain their findings. 15
Whether veterans with heart disease have similarly positive functional measures compared with their nonveteran counterparts is unknown. Since about 2005, VHA chronic care improvement initiatives and healthy lifestyle promotion programs have targeted risk factors for CVD, such as diabetes, hypertension, obesity, and substance use disorders, as part of the VHA’s strategic focus on disease prevention. 22 -26 Examples include the MOVE!® weight management program 23 and shared medical appointments for diabetes, which offer multidisciplinary health care and health education provided in group settings to encourage peer support. 24,25 In contrast, heart disease is rarely a focus of shared appointment programs, with the exception of congestive heart failure. 25 The VHA’s strategic plan describes its “stress [on] preventive interventions” to “eliminate or significantly reduce conditions that impair veteran quality of life,” citing diabetes and obesity as examples, but the plan does not mention care for heart disease. 26 If, as previously suggested, the generally equivalent health status of veterans with diabetes, compared with nonveteran counterparts, is due to use of multidisciplinary preventive care strategies, 15 one would not necessarily expect the same favorable outcomes for veterans with heart disease.
To date, information on this topic is limited. Although several studies have documented an elevated rate of heart disease in veterans, 7,14 none has compared the functioning of veterans and nonveterans with heart disease. This information could inform chronic care models by identifying patient populations in which additional holistic care targeted to both physical and psychological functioning should be considered.
To address this gap, the primary a priori purpose of this study was to assess physical and psychological functioning in veterans with or at high risk of heart disease (heart disease/risk). Like the previous study of veterans with diabetes, 15 this analysis had 2 comparator groups: nonveterans with heart disease/risk and veterans without heart disease/risk. A secondary purpose, developed post hoc to explain the findings of the a priori analysis, was to identify predictors of treatment for mental health and substance use disorders, which could affect physical and psychological functioning.
Methods
The study was a retrospective analysis of respondent cohorts created from data collected in the National Survey on Drug Use and Health (NSDUH) from 2015 through 2019. The NSDUH is an annual, cross-sectional, cluster-randomized, US population household-interview survey on psychological symptoms, use and misuse of controlled medications and alcohol, and use of illicit drugs, conducted annually by Research Triangle Institute (RTI) under the authority of the Substance Abuse and Mental Health Services Administration (SAMHSA). 27 Survey data are publicly available, fully de-identified, and commonly used in published studies of mental health and substance use in the US, including studies of military veterans. 15,28 -30 The NSDUH sampling frame excludes active-duty military and persons who are institutionalized, such as those residing in prisons, hospitals, assisted living, or nursing facilities. 31 To facilitate candid responses, data on sensitive topics, such as use of controlled substances and alcohol, are collected on an RTI laptop using computer-assisted self-interviewing performed by respondents without interviewer involvement. 31
Sampling and Cohort Classification
Sampling criteria and cohort classification methods were similar to those used in the previous study of veterans and nonveterans with diabetes. 15 Survey respondents aged ≥18 years were included in the study if they either (1) were veterans of the US military, (2) had heart disease in adulthood, or (3) were at high risk of CVD. Nonveterans without heart disease/risk were excluded from the sample. As in previous research using NSDUH data to study veterans, 15,30 current military reservists, who are eligible for but not currently serving on active duty, were also excluded.
Heart disease in adulthood was the primary measure of disease in this study because the NSDUH does not specifically query respondents about CVD, but does query about the age at which heart disease was diagnosed. We required that the heart disease be present in adulthood because heart diseases diagnosed and treated only in childhood could have represented surgically corrected genetic anomalies. Those with high CVD risk were included in the heart disease/risk cohort because treatment to prevent CVD morbidity and mortality would likely be extended to these patients due to their multiple risk factors. 32 To address possible error in the validity of this construct, a sensitivity analysis was performed in which cohort membership was based on presence or absence of heart disease without consideration of risk factors.
Measures used to identify adult heart disease and high CVD risk
Chronic conditions, including heart disease, CVD risk factors, and other comorbidities, are identified in the NSDUH based on responses to queries on whether “a doctor or other health professional” had “ever told you that you had” the conditions named in a series of checklist items.31 Adult heart disease in the present study was defined as diagnosis at aged ≥18 years or having heart disease in 1 year prior to the survey, based on the checklist item “heart condition” and questions about (1) the age when the respondent’s “heart condition or heart disease was first diagnosed” and (2) whether the respondent had “any kind of heart condition or heart disease in the past 12 months.” High risk of CVD was defined as being either aged 50-64 years with ≥2 risk factors or aged ≥65 years with ≥1 risk factor of 3 chronic conditions: diabetes, hypertension, and kidney disease. These conditions were chosen because they are recognized as CVD risk factors and available in the NSDUH. 31,33
Measures used to identify military veterans
Veteran status was determined based on answers to questions about whether the respondent had “ever been in the United States Armed Forces” and about current military service. 31 Those indicating they were currently “separated or retired from the military” were defined as veterans. Those indicating they were currently serving “in a reserves component” were ineligible for sample inclusion. 15,30
Outcome Variables
Like sampling criteria, outcomes were similar to those used in the study of diabetes. 15 They included measures of psychological functioning, substance use and misuse, and physical functioning.
Psychological functioning
The NSDUH measures psychological functioning with standard Diagnostic and Statistical Manual (DSM)-IV definitions. 31 The primary psychological outcome measure in the present study was nonspecific serious psychological distress. Psychological distress is measured in the NSDUH using the Kessler 6-item (Kessler-6) distress scale, a measure of nonspecific distress that has been validated against structured clinical interviews based on DSM criteria and has been previously used in a veteran sample. 31,34,35 Kessler-6 scale scores range from 0-24 (6 items, Likert scale of 0-4). A Kessler-6 score of ≥13 indicates serious distress.
Past-year major depressive episode (MDE) is defined in the NSDUH, as in the DSM-IV, as both of the following: (1) respondent reports ≥5 of 9 depressive symptoms (e.g., change in appetite or weight, insomnia or hypersomnia) and (2) ≥1 reported symptom is loss of pleasure in daily activities or depressed mood. 31 For these questions, respondents are asked to recall the worst period of time during the previous year. Suicidality is measured by asking if the respondent had “seriously [thought] about trying to kill yourself” during the past year.
Mental illness is not self-reported by NSDUH respondents. Instead, indicators for any mental illness and serious mental illness are based on a validated statistical model. The model includes measures of past-year suicidality and MDE, the World Health Organization Disability Assessment Schedule, the Kessler-6, and demographic information. 31,36
Substance use and misuse
Like psychological measures, substance use and misuse measures in the NSDUH are based on standard questions and DSM-IV definitions, applied to respondent-reported behaviors and symptoms. 31 For example, use of controlled substance medications is measured by showing respondents images of pills in various therapeutic categories, briefly describing the use of the pills, and asking about use of each by name. 37 The categories measured include pain relievers (i.e., opioids), tranquilizers (i.e., benzodiazepines), stimulants, and sedatives (i.e., z-hypnotic medications). Prescription medication misuse is identified by asking the respondent to report any use of these products “in any way a doctor did not direct you to use them,” including use of someone else’s prescription, use for a greater duration or dosage than prescribed, or any other nonmedical use. Measures of binge drinking are based on the standard US Centers for Disease Control and Prevention (CDC) definition: ≥4 drinks for females or ≥5 drinks for males on a single occasion. 31,38
The present study’s substance use outcome, high-risk substance use, was based on the CDC definition, use predisposing to adverse health outcomes or life consequences.
39
Any ≥1 of the following was defined as high-risk substance use: Past-month frequent binge drinking (heavy drinking in the NSDUH nomenclature, defined as binge drinking on ≥5 separate occasions during the 1 month prior to the interview); Past-year history of nonmedical use of prescription controlled substances as defined above; Past-year use of illicit drugs other than marijuana (cocaine, hallucinogens, heroin, inhalants, or methamphetamine); Past-year substance dependence, defined as meeting ≥3 DSM diagnostic criteria (e.g., tolerance, withdrawal, inability to set limits on use); Past-year nondependent substance misuse, defined as meeting ≥1 of 4 criteria representing physical danger or life problems related to substance use; or Most recent alcohol use was combined with prescription controlled substances or with any illicit drug, including marijuana.
Physical functioning
The primary physical functioning measure used in the present study was self-rated overall “health in general.” 31 This item is measured on a Likert scale (excellent, very good, good, fair, and poor) and has been criterion-validated against objective measures including health-related behaviors. 40 Additional measures included a count of total chronic conditions excluding heart disease; binary indicators of inpatient hospital or emergency room use in the past year; count of office or clinic visits reported by the respondent in the past year; impairments in sight or hearing; and impairments in daily activities including walking, climbing stairs, dressing, or running errands. 31
Statistical Analytic Methods
All analyses were performed using IBM SPSS for Complex Samples (v27.0), which weights results, statistical tests, and confidence intervals to account for the homogeneity of variance resulting from the multistage sampling design. Because of the large sample size, 99% confidence intervals were calculated, and the a priori alpha was 0.01. Estimates reported herein meet National Center for Health Statistics statistical reliability standards for analyses of federal complex sample data except where otherwise noted. 41,42
A priori analyses
Bivariate analyses of the cohorts included demographic characteristics, body mass index (BMI) categories, tobacco use, and the outcome measures described above. For bivariate analyses, between-cohort differences were tested with Pearson chi-square.
Ordinal logistic regression-adjusted analyses of each primary outcome were used to estimate the association of cohort (veterans with and without heart disease/risk, compared with the reference cohort, nonveterans with heart disease/risk) with each of the 3 primary outcomes. Coefficients in an ordinal logistic regression represent the odds of moving from lower to higher scores on an ordinal scale, for example, from excellent health coded as 1 to poor health coded as 5. 43 Models were adjusted for age, sex, race, education, marital status, employment, income category, and number of chronic conditions.
Post hoc analyses
An additional post hoc set of binary logistic regression models assessed the association of veteran status with past-year receipt of treatment for mental health and substance use disorders. Mental health treatment was measured as an affirmative response to (1) receiving “treatment or counseling for any problem you were having with your emotions, nerves, or mental health” in a general or psychiatric hospital, residential treatment center or other facility, outpatient mental health or medical center or clinic, therapist or physician’s office, day treatment program, or group therapy; or (2) taking “any prescription medication that was prescribed for you to treat a mental or emotional condition.” 31
Substance use disorder treatment included either mental health treatment, excluding medication, or an affirmative response to the question “have you received treatment or counseling for your use of alcohol or any drug, not counting cigarettes,” where treatment was delivered in any of the following settings: hospital, including rehabilitation hospital or facility; outpatient rehabilitation; mental health center; physician’s office, prison or court-ordered setting; group (e.g., Alcoholics Anonymous, Narcotics Anonymous); or a methadone or buprenorphine/suboxone/subutex clinic. Anti-abuse medications were not included because the NSDUH does not measure them. Mental health treatment was included because professional standards call for treatment of substance use disorders as part of care for psychological problems. 44 -46
Treatment receipt models were limited to those evidencing need for treatment; for example, the model predicted mental health treatment for respondents with past-year psychological symptoms (MDE, serious distress, or suicidality). These models were adjusted for the same covariates as in the a priori analysis, plus sensory or daily living impairments for all models predicting in-person services (e.g., outpatient mental health treatment). Additionally, the mental health treatment model adjusted for substance misuse, and the substance use disorder treatment model adjusted for psychological symptoms.
Results
Of 214,505 adult NSDUH respondents in 2015-2019, 14,151 reported any heart disease, 8,901 had combinations of age and risk factors that met the criteria for high CVD risk, and 11,876 were veterans (Figure 1). After sample exclusions, the final sample comprised 28,314 adults: veterans without heart disease/risk (n = 8,393), veterans with heart disease/risk (n = 3,483), and nonveterans with heart disease/risk (n = 16,438). Demographic characteristics of the respondents were generally similar across cohorts, except that the veteran cohorts contained far fewer females than the nonveteran cohort, and the cohorts with heart disease/risk contained proportionately more unemployed/retired persons and fewer tobacco users than the cohort without heart disease/risk (Table 1).
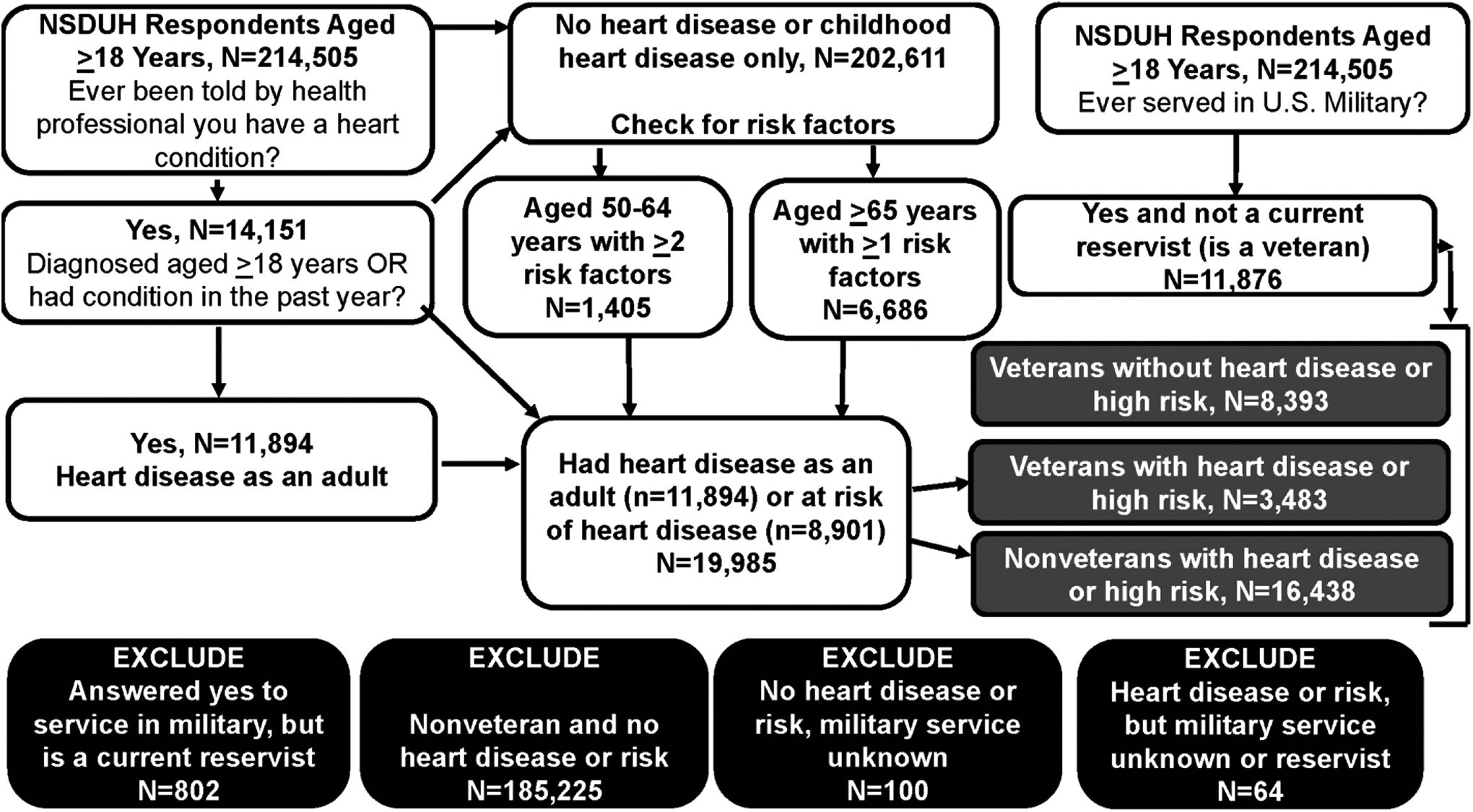
Sample selection process. NSDUH indicates National Survey on Drug Use and Health.
Demographics and Health-Related Risk Factors, Veterans With or At Risk of Heart Diseasea and Comparator Cohorts, Respondents to National Survey on Drug Use and Health, 2015-2019.

Abbreviations: BMI, body mass index; CI-L, lower limit of the 99% confidence interval; CI-U, upper limit of the 99% confidence interval; CVD, cardiovascular disease; FPL, federal poverty level; kg/m2, body weight in kilograms divided by squared height in meters.
a All between-cohort comparisons were statistically significant (P < .01) using Pearson χ2. Significance tests and confidence intervals are adjusted for the design effect (homogeneity of variance) associated with the complex sampling design. All estimates meet federal statistical reliability standards.
b Veterans are respondents who reported serving in the US military, were not current reservists, and were separated or retired from military service. Respondents with heart disease or risk are those who reported ≥1 of the following: (1) told of a heart condition by a health professional at aged ≥18 years, (2) reported having a heart condition in the year prior to the interview, (3) aged 50-64 years with ≥2 CVD risk factors, or (4) aged ≥65 years with ≥1 CVD risk factors. CVD risk factors included diabetes, kidney disease, and hypertension.
c Calculated by applying federal poverty standards, based on age, family size, and number of children in home, to total family income.
d Calculated from self-reported height and weight.
Bivariate Analyses
Regardless of veteran status, heart disease/risk was associated with impaired physical and overall functioning (Table 2). For example, excellent self-rated general health was reported by 8.5% (99% confidence interval [CI] = 7.2%-9.9%) of veterans with heart disease/risk and 8.0% (CI = 7.2%-8.8%) of nonveterans with heart disease/risk, but by 20.4% (CI = 18.7%-22.3%) of veterans without heart disease/risk. Similarly, the rate of inpatient hospital use in the past year for those with heart disease/risk (range 21%-23%) was more than double that of veterans without heart disease/risk (9.2%, CI = 8.0%-10.4%). Office/clinic use displayed a similar pattern.
Measures of Physical, Psychological, and Behavioral Functioning, Veterans With or At Risk of Heart Disease and Comparator Cohorts,a Respondents to National Survey on Drug Use and Health, 2015-2019.

Abbreviations: CI-L, lower limit of the 99% confidence interval; CI-U, upper limit of the 99% confidence interval; CVD, cardiovascular disease; DSM-IV, Diagnostic and Statistical Manual of Mental Disorders, fourth edition.
a All between-cohort comparisons were statistically significant (P < .01) using Pearson χ2, except for suicidality (P = .030). Significance tests and confidence intervals are adjusted for the design effect (homogeneity of variance) associated with the complex sampling design. All estimates meet federal statistical reliability standards.
b Veterans are respondents who reported being separated or retired from military service. Respondents with heart disease or risk are those who reported ≥1 of the following: (1) told of a heart condition by a health professional at aged ≥18 years, (2) reported having a heart condition in the year prior to the interview, (3) aged 50-64 years with ≥2 CVD risk factors, or (4) aged ≥65 years with ≥1 CVD risk factors. CVD risk factors included diabetes, kidney disease, and hypertension.
c Sum of asthma, cancer, chronic obstructive pulmonary disease, cirrhosis, diabetes, hepatitis B or C, hypertension, human immunodeficiency virus, and kidney disease.
d Difficulties walking or climbing stairs, dressing, or running errands.
e Based on validated predictive model encompassing psychological distress, functional disability due to psychological symptoms, suicidal thinking, and demographic information.
f Respondent reported having ≥5 of 9 DSM-IV symptoms, of which ≥1 was depressed mood or loss of interest or pleasure in daily activities, for ≥2 weeks in the year prior to the interview.
g Score of ≥13 on the Kessler Psychological Distress Scale, which ranges from 0-24, for the worst month experienced in the year prior to the interview.
h Past-month heavy drinking (binge drinking on ≥5 occasions, where a binge is ≥4 drinks for females or ≥5 drinks for males on a single occasion); past-year nonmedical use of prescription controlled substances (pain relievers, sedatives, tranquilizers, or stimulants); past-year use of illicit drugs other than marijuana; substance dependence; nondependent substance misuse; or most recent alcohol use was combined with prescription controlled substances or with any illicit drug.
Measures of psychological functioning displayed a more complex pattern (Table 2). No clear differences in past-year mental health problems were observed among the cohorts, except for a modestly higher rate of mental illness among nonveterans (18.9%, CI = 18.0%-19.9%) than veterans (range 14%-15%). However, veterans without heart disease/risk were more likely to engage in high-risk substance use (16.7%, CI = 15.6%-17.9%) than were those with heart disease/risk including veterans (9.8%, CI = 8.4%-11.5%) or nonveterans (8.5%, CI = 7.8%-9.2%). Veterans without heart disease/risk were also more likely to engage in binge drinking.
Regression-Adjusted Analyses
In ordinal logistic regression analyses, declining overall self-rated health was associated with several social determinants of health (e.g., less than high school education, lower income, unemployment); with chronic conditions in addition to heart disease; with nonwhite race; and with being aged 25-64 years (Table 3). After adjustment for these factors, veterans and nonveterans with heart disease/risk did not significantly differ. As expected, having no heart disease/risk was associated with a 50% reduction in the odds of declining self-rated health (odds ratio [OR] = 0.50, CI = 0.44-0.56).
Ordinal Logistic Regression Analyses of Key Measures of Functioning, by Veteran and Heart Disease/Risk Status.a

Abbreviations: CI-L, 99% confidence interval lower limit; CI-U, 99% confidence interval upper limit; FPL, federal poverty level; HD, heart disease; OR, odds ratio.
a Bolded coefficients denote statistically significant associations.
b Five-point Likert scale; excellent = 1, very good = 2, good = 3, fair = 4, poor = 5.
c Score of ≥13 on the Kessler Psychological Distress (K6) scale.
d Past-month heavy drinking (binge drinking on ≥5 occasions, where a binge is ≥4 drinks for females or ≥5 drinks for males on a single occasion; past-year history of nonmedical use of prescription controlled substances (pain relievers, sedatives, tranquilizers, or stimulants); past-year use of illicit drugs other than marijuana; substance dependence; nondependent substance misuse; or most recent alcohol use was combined with prescription controlled substances or with any illicit drug.
e Model Wald chi-square for binary logistic regression with fair or poor health, serious psychological distress, or high-risk substance use as dependent variables, calculated using this method because the SPSS Complex Samples ordinal logistic regression procedure produces no model significance test.
f Relative standard error ≥ 30%; indicates coefficient does not meet statistical reliability test; interpret cautiously.
The strongest predictor of both serious distress and high-risk substance use was younger age (Table 3). Compared with age ≥65 years, being aged 18-25 years multiplied the odds of serious distress approximately 14-fold (OR = 13.81, CI = 10.35-18.43) and of high-risk substance use approximately 6-fold (OR = 6.46, CI = 4.82-8.66). After adjusting for age and other demographic factors, the veteran and nonveteran cohorts did not significantly differ; however, among those with heart disease/risk, a trend toward increased rates of serious distress in veterans compared with nonveterans was noted (OR = 1.36, CI = 0.99-1.86).
Results were similar in the sensitivity analysis in which cohorts were defined based on heart disease only, rather than on the combination of heart disease/risk (Online Appendix 1). Veterans without heart disease had a 53% reduction in the odds of declining self-rated health (OR = 0.47, CI = 0.41-0.53), compared with the reference group of nonveterans with heart disease. Compared with the same reference group, veterans with heart disease experienced a nonsignificantly higher trend in the odds of serious distress (OR = 1.44, CI = 0.96-2.16). No other significant differences or trends were noted.
Post-Hoc Analysis of Treatment
As a follow-up analysis to explain the nonsignificant trend for elevated serious distress among veterans with heart disease/risk, the post hoc analysis of treatment receipt tested for statistically significant differences between veterans and nonveterans, although results for all 3 cohorts are displayed (Figure 2). There were no significant differences in rates of any treatment or mental health medication for psychological symptoms, or in inpatient or outpatient treatment for high-risk substance use. However, veterans were somewhat more likely than nonveterans to receive outpatient treatment for psychological symptoms (36.1%, [CI = 34.4%-37.8%] vs. 28.9% [CI = 28.2%-29.6%], respectively; CIs not shown in figure). Additionally, among those with high-risk substance use and psychological symptoms comorbid with heart disease/risk, veterans were more likely than nonveterans to receive mental health medication (63.9% [CI = 60.9%-66.9%] vs. 55.2% [CI = 53.7%-56.8%], respectively).

Regression-adjusted probabilities of past-year behavioral health treatment receipt. a All models were adjusted for sex, age, race/ethnicity, education, marital and employment status, income, chronic conditions, and receipt of ≥2 office/clinic visits in the year prior to the interview. All models except the mental health medication model were also adjusted for sensory or daily living impairments. Models limited to respondents with psychological symptoms (past-year major depressive episode, serious psychological distress, or suicidality) were further adjusted for high-risk substance use; models limited to respondents with high-risk substance use were further adjusted for psychological symptoms. b For those with psychological symptoms, any treatment indicates a “yes” response to questions about receiving “treatment or counseling for any problem you were having with your emotions, nerves, or mental health,” excluding “treatment for alcohol or drug use,” in any of the following settings: general or psychiatric hospital, residential treatment center or other facility, outpatient mental health or medical center or clinic, therapist or physician’s office, day treatment program, or group therapy; or a “yes” response when asked about taking “any prescription medication that was prescribed for you to treat a mental or emotional condition.” For those with high-risk substance use, treatment includes either mental health treatment, excluding medication, or a “yes” response to the question “have you received treatment or counseling for your use of alcohol or any drug, not counting cigarettes,” and treatment was delivered in any of the following: hospital, including rehabilitation hospital or facility; outpatient rehabilitation; mental health center; physician’s office, prison or court-ordered setting; group (e.g., AA, NA); or methadone, buprenorphine/suboxone/subutex clinic. Excludes treatment rendered in emergency rooms, from home or family, or as “spiritual influence,” but includes formal faith-based treatment programs. c Complex samples t-test of between-group difference in adjusted predicted values, comparing veterans with nonveterans among respondents with heart disease/risk.
Discussion
This retrospective analysis of validated survey data for a nationally representative sample produced several key findings. First, among those with heart disease/risk, serious psychological distress trended higher among veterans compared with nonveterans; however, this nonsignificant difference did not appear to be explained by between-group differences in use of behavioral health treatment, as veterans with psychological symptoms or high-risk substance use were treated at rates similar to or higher than those of their nonveteran counterparts. Second, rates of high-risk substance use and binge drinking were much higher among younger than older adults and, in bivariate analysis but not tested in adjusted analyses, in both veterans and nonveterans without heart disease. Third and as expected, 15 both veterans and nonveteran respondents with heart disease/risk experienced poorer functioning, evidenced by increased health care service utilization and decreased self-reported overall well-being, than did veterans without heart disease.
Limitations of our work should be noted. First, the NSDUH represents self-reported data that may be affected by biases or inaccurate perceptions. Mitigating this limitation are design elements incorporated in the NSDUH, including use of computer-assisted self-interviewing; measurement of behaviors and symptoms, rather than respondent-reported diagnoses, for psychological and substance use concerns; and use of pictures, rather than names only, when asking patients about prescription medications. 31 Moreover, in a previous analysis of NSDUH data, the diabetes prevalence rate for veterans matched closely with that reported by another national source, suggesting accurate reporting by respondents. 15 Second, we incorporated CVD risk factors into the definition of heart disease; however, a sensitivity analysis in which risk factors were not considered produced similar findings.
Third, study results do not have external validity for persons who are institutionalized, homeless, or active-duty military, as these groups are excluded from the NSDUH sampling frame. 31 Exclusion of those who are institutionalized or homeless may have resulted in underestimated rates of substance misuse or distress. Similarly, because most veterans are male, 15 we were not able to address important questions about women’s cardiometabolic health, currently recognized as an understudied topic, 47 although we did control for sex in the logistic regression analyses.
Fourth, because the NSDUH does not measure whether respondents received care from the VHA, no definitive statements can be made about whether respondents in this sample received multidisciplinary care from VHA or non-VHA sources. Our measures of treatment utilization among those needing services could have been affected by this issue, especially among the estimated 1-quarter of veterans who reside in rural areas, where access to VHA-provided services may be limited. 48
Fifth, although logistic regression analyses controlled for measured confounding factors, the possibility of residual confounding remains in this research, as in all observational designs, and might have affected the outcomes reported here. Selection bias toward better mental or physical health among military personnel, due to the eligibility criteria for entrance into service, 49 is a possibility. Additionally, we were not able to control for military service-related factors that could have affected health status, such as draftee versus recruit status, service branch, or service duration.
Overall, results of this study should be seen as descriptive, intended to suggest potential challenges and policy implications for at-risk patient populations and demographic groups that could not have been studied with a randomized design. Despite the descriptive nature of the study, the impairments in physical and psychological functioning observed in this research have potentially concerning implications for those with or at high risk of heart disease, given evidence that impaired health-related quality of life increases risk of death and cardiovascular complications in patients with CVD. 50 Also concerning are the observed rates of binge drinking, especially in the more than 1-quarter of veterans without heart disease/risk who reported recent binge drinking in the previous month. Presumably, a portion of this group will develop CVD or CVD risk factors in the coming years, making them an appropriate target for lifestyle intervention now.
Although veterans were not less likely than nonveterans to receive treatment for mental health and substance use problems, the generally low rates of treatment for sampled respondents with heart disease/risk—55%-56% among respondents with psychological symptoms, 19% among those with high-risk substance use, and 55%-63% psychotropic medication use among those with both high-risk substance use and psychological symptoms—suggest potential barriers to treatment. These low rates of treatment have been observed in previous research, especially in persons with substance use disorder, and may be due to stigma; treatment access or cost challenges; the desire to continue using substances of abuse; a perception that treatment is unnecessary; and, among older adults, lack of age-appropriate treatment venues for persons with mobility or sensory impairments. 51 -54 Our findings are also consistent with national survey data on veterans of the wars in Afghanistan and Iraq, suggesting gaps between knowledge of heart disease risk factors and engagement in preventive activities, such as stress reduction or healthy blood pressure maintenance. 55
Coupled with that body of work, our findings highlight the potential value of querying adults regarding psychological symptoms and substance use behaviors in routine health care encounters, consistent with the recommendations of the US Preventive Services Task Force. 56,57 Similarly, the American Heart Association and American College of Cardiology Foundation (AHA/ACCF)’s guidance for management of high-risk conditions following an acute myocardial infarction were expanded beginning in 2011 to include a recommendation specifically focused on screening for depression. 58
The present study finding of elevated high-risk substance use among younger adults aligns with previous research on age-related substance use patterns in both veterans and nonveterans, and with evidence of high rates of substance misuse among recent-era veterans. 15,59,60 The present study finding of reduced rates of high-risk substance use in those with heart disease/risk is consistent with AHA/ACCF guidance that providers should encourage patients to moderate alcohol consumption 58 and with known risks of illicit drugs, especially for persons with chronic illnesses. 61
The age-related differences in high-risk substance use and serious distress also suggest a potentially important outreach opportunity to use new technologies, such as mobile applications and telehealth, in helping patients self-manage cardiovascular event risk and psychological symptoms. The VHA provides mobile applications for a variety of preventive services intended to improve health-related quality of life and health outcomes, including smoking cessation, MOVE!, PTSD symptom tracking, mindfulness, stress reduction, and relationship coaching. 62 Its online “app store” may serve as a model for other organizations. 63 For example, variations on its PTSD Coach app have been used by multiple European nations and Canada. 63
The present study finding of a nonsignificant upward trend in serious distress for veterans compared with nonveterans with heart disease/risk is difficult to interpret, especially in light of veterans’ approximately equivalent physical functioning and behavioral treatment utilization. In the previous comparative study of veterans and nonveterans with diabetes, veterans appeared to have equivalent or slightly better psychological functioning than nonveterans, possibly because of the VHA’s multidisciplinary care models for patients with diabetes. 15 In the present study, psychological functioning measures were equivocal. Nonetheless, the combination of impairments and comorbidities associated with heart disease, and generally low rates of treatment for psychological symptoms and high-risk substance use, suggests a need for future study of shared appointments and similar multidisciplinary interventions in patients with heart disease or other chronic conditions associated with impairments in psychological functioning. In a patient population that may face barriers to care, such as a lack of age-appropriate interventions or reluctance to access care, 51 -54 the peer support provided by group interventions like shared appointments or MOVE! may be helpful. Additionally, the holistic focus of these programs is intended both to mitigate disease-related distress and to reduce risk of future cardiovascular events. 24,25 However, other than in diabetes, rigorous evidence on the outcomes of shared appointment programs is limited. 64
Conclusion
Among those with heart disease/risk in a nationally representative sample, impaired physical functioning was evident in both veterans and nonveterans. Among those with heart disease/risk and symptoms of psychological distress or high-risk substance use, rates of treatment were low, although veterans and nonveterans were approximately equally likely to receive treatment. Consistent with treatment guidelines, findings highlight a need for continued expansion of access to mental health treatment and services among those with heart disease/risk, possibly using multidisciplinary care models and peer support.
Supplemental Material
Supplemental Material, sj-docx-1-cpt-10.1177_10742484221091015 - Association of Cardiovascular Disease and Military Veteran Status With Impairments in Physical and Psychological Functioning: Retrospective Cross-Sectional Analysis of US National Survey Data
Supplemental Material, sj-docx-1-cpt-10.1177_10742484221091015 for Association of Cardiovascular Disease and Military Veteran Status With Impairments in Physical and Psychological Functioning: Retrospective Cross-Sectional Analysis of US National Survey Data by Nicole K. Early, Kelsey Buckley, Nana Entsuah and Kathleen A. Fairman in Journal of Cardiovascular Pharmacology and Therapeutics
Footnotes
Author Contributions
Concept and design by NKE, KB, and NE, with assistance of KAF; data acquisition and analysis by KAF; data interpretation, writing draft, and revising for important content by all authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.