
Abstract
In the era of the coronavirus disease 2019 (COVID-19) pandemic, acute cardiac injury (ACI), as reflected by elevated cardiac troponin above the 99th percentile, has been observed in 8%-62% of patients with COVID-19 infection with highest incidence and mortality recorded in patients with severe infection. Apart from the clinically and electrocardiographically discernible causes of ACI, such as acute myocardial infarction (MI), other cardiac causes need to be considered such as myocarditis, Takotsubo syndrome, and direct injury from COVID-19, together with noncardiac conditions, such as pulmonary embolism, critical illness, and sepsis. Acute coronary syndromes (ACS) with normal or near-normal coronary arteries (ACS-NNOCA) appear to have a higher prevalence in both COVID-19 positive and negative patients in the pandemic compared to the pre-pandemic era. Echocardiography, coronary angiography, chest computed tomography and/or cardiac magnetic resonance imaging may render a correct diagnosis, obviating the need for endomyocardial biopsy. Importantly, a significant delay has been recorded in patients with ACS seeking advice for their symptoms, while their routine care has been sharply disrupted with fewer urgent coronary angiographies and/or primary percutaneous coronary interventions performed in the case of ST-elevation MI (STEMI) with an inappropriate shift toward thrombolysis, all contributing to a higher complication rate in these patients. Thus, new challenges have emerged in rendering a diagnosis and delivering treatment in patients with ACI/ACS in the pandemic era. These issues, the various mechanisms involved in the development of ACI/ACS, and relevant current guidelines are herein reviewed.
Keywords
Introduction
In the era of the coronavirus disease 2019 (COVID-19) pandemic, new issues and challenges have arisen and/or are newly recognized in the diagnosis and treatment of patients presenting with symptoms of acute cardiac injury (ACI) or acute coronary syndromes (ACS). 1 -3 First, a pattern of ACI, defined as cardiac troponin (cTn) above the 99th percentile in the upper reference limit, has been observed in a variable number of patients with COVID-19 infection dependent on the severity of the infection, which portends an adverse prognosis and increased mortality in these patients 3 -5 ; second, a significant delay has been recorded in patients with ACS attending the emergency room or seeking advice for their symptoms. 6,7 Also, the routine of caring for patients with ACS has been sharply disrupted with regard to urgent coronary angiography and/or the performance of primary percutaneous coronary intervention (PCI) in the case of ST-elevation myocardial infarction (STEMI) vs administering thrombolytic therapy. 8 Thus, new challenges have emerged in delivering treatment for ACI/ACS in the era of the COVID-19 pandemic. 9 All these issues are herein reviewed, modified current guidelines are presented and potential mechanisms involved in COVID-19-induced ACI/ACS are discussed and pictorially illustrated.
Myocardial Injury in COVID-19
Patients with COVID-19 infection can present with acute cardiac injury (ACI) defined as elevated cTn >99th percentile, albeit mostly with stable and unchanging values, or with typical ACS (STEMI or NSTEMI or unstable angina) from atherosclerotic coronary plaque disruption (rupture or erosion) with a rise and fall of cTn in the case of STEMI/NSTEMI, either in the setting of obstructive or non-obstructive coronary artery disease (CAD); the latter group of patients may have angiographically normal-appearing coronary arteries or non-obstructive (<50%) coronary lesions, recently termed ACS with normal or near-normal coronary arteries (ACS-NNOCA) (Figure 1). 10 On the other hand, non-COVID-19 patients may also present with ACS or ACS mimics associated with the COVID-19 pandemic, either triggered by the anxiety related to corona-phobia, 11 or to pandemic-associated financial and other emotional stress. 12,13 Furthermore, many patients with ACS symptoms may avoid or delay their visit to the emergency room for fear of contracting the virus, with ensuing grave consequences. 14

The schema illustrates the potential mechanisms involved in COVID-19-induced acute coronary syndromes (ACS) and acute cardiac injury (ACI), the inter-relationship among them and among the types of typical (atherosclerosis-related) and non-typical (ACS-NNOCA) ACS, and the delayed first medical contact (FMC) observed with its attendant dire consequences (higher complication rate) (see text for discussion). ACE2 indicates angiotensin converting enzyme type 2; ACI, acute cardiac injury; ACS-NNOCA, acute coronary syndrome with normal or near-normal coronary arteries; INOCA, ischemia with non-obstructive coronary artery disease; MINCA, myocardial infarction with normal coronary arteries; MINOCA, myocardial infarction with non-obstructive coronary artery disease; NSTEMI, non-ST elevation myocardial infarction; RAS, renin-angiotensin system; SNS, sympathetic nervous system; STEMI, ST-elevation myocardial infarction; TTC, Takotsubo cardiomyopathy (syndrome); UA, unstable angina.
Acute Cardiac Injury (ACI)
From the outset, it was noted that cTn was marginally elevated in all patients with COVID-19 infection, while values exceeding the 99th percentile in the upper reference limit were observed in
Several systematic reviews and meta-analyses have reported their findings on ACI in COVID-19 patients (Table 1). 4,20 -30 A systematic review of 8 studies comprising 1,229 patients showed that the frequency of ACI was 16% (95% CI: 9%-27%), albeit with high (93%) heterogeneity among the studies. 4 A meta-analysis of 16 studies comprising 2224 patients indicated that the incidence of ACI was 24.4% in hospitalized COVID-19 patients. 20 Subsequently, it was felt that it is more plausible that ACI is attributable mostly to nonischemic causes of myocardial injury or type 2 myocardial infarction (MI) (myocardial oxygen supply–demand imbalance), rather than typical or type 1 MI. 5,31 The point differentiating this increase in cTn from typical MI was the fact that the majority of COVID-19 patients demonstrate stable cTn rather than the dynamically changing values with a rise and fall indicative of an ACS (STEMI/NSTEMI). 32 Nevertheless, this type of ACI has been associated with worse prognosis and increased mortality. 16,22,33 Occasionally, it may follow the course of acute fulminant myocarditis with hemodynamic compromise and cardiogenic shock requiring mechanical support (e.g., with extracorporeal membrane oxygenation-ECMO) for recovery. 34,35 Recently, another review of 26 studies including 11,685 patients indicated that the weighted pooled prevalence of ACI was 20% (range 5%-38% depending on the criteria used). 21
Meta-Analyses of Studies Regarding Acute Cardiac Injury (ACI) and COVID-19 Infection.

Abbreviations: ACI, acute cardiac injury; AKI, acute kidney injury; ARDS, acute respiratory distress syndrome; BNP, brain natriuretic peptide; COPD, chronic obstructive pulmonary disease; cTn, cardiac troponin; CVD, cardiovascular disease; HF, heart failure; hs-cTnI, high-sensitivity cardiac troponin I; HTN, hypertension; ICU, intensive care unit; OR, odds ratio; pts, patients; RR, risk ratio.
ACI and Mortality
As mentioned, evidence that ACI during COVID-19 significantly increases mortality during the infection has been provided by meta-analyses, as well (Table 1). A meta-analysis of 16 studies (N = 2224) indicated that the all-cause mortality in patients with ACI was 72.6% (odds ratio-OR = 17.32) compared to those without ACI (14.5%). 20 Patients who were older with hypertension (HTN) and chronic obstructive pulmonary disease (COPD) were prone to develop ACI. Another meta-analysis of 8 studies (N = 1686 COVID-19 patients; mean age 59.5 years; 387 patients or 23.9% experiencing ACI), indicated that the incidence of ACI was higher among non-survivors (61.6 vs 6.7%, P < 0.0001). 23 Another meta-analysis of 13 studies comprising 2389 patients showed that ACI was associated with higher mortality (risk ratio-RR 7.95, P < 0.001; I2: 65%), higher need for intensive care unit (ICU) care (RR 7.94, P = 0.01; I2: 79%), and severe COVID-19 (RR 13.81, P < 0.001; I2: 0%).22 A meta-analysis of 28 studies including 4189 confirmed COVID-19 patients indicated that more severe COVID-19 infection was associated with higher mean cTn, while ACI was more frequent in those with severe, compared to milder, disease (RR 5.99; P < 0.001). 24 Furthermore, COVID-19-related ACI was associated with higher mortality (RR 3.85; P < 0.001). A meta-analysis of 10 studies, among which 8 reported on ACI, indicated that ACI was associated with an unadjusted odds ratio of 21.15 for in-hospital mortality (I2 = 71%). 25 Finally, a meta-analysis of 49 studies showed that ACI was associated with high odds (odds ratio-OR 10.58) for the adverse composite endpoint of death, severe presentation, hospitalization in the ICU and/or mechanical ventilation; a history of CV disease (CVD) (OR 3.15), acute kidney injury (AKI) (OR 5.13), increased procalcitonin (OR 4.8) or D-dimer (OR 3.7), and thrombocytopenia (OR 6.23) also conveyed high odds for the adverse composite endpoint. 26 Advanced age, male sex, CV comorbidities, ACI or AKI, lymphocytopenia and D-dimer conferred an increased risk of in-hospital mortality.
Shock and malignant arrhythmias have been reported as the most common outcomes of ACI. 36 The risk of in-hospital death among COVID-19 patients with ACI may be predicted by the peak levels of cTn during hospitalization. 37 In addition, advanced age, coagulopathy, acute respiratory distress syndrome (ARDS), and other comorbidities are associated with increased risk of in-hospital mortality in COVID-19 patients with ACI. 30,38 Pre-existence of heart failure and hypertension, and high cardiac biomarkers correlate with worse outcomes. 29
Differential Diagnosis
In addition to possible clinically- and ECG-discernible reasons of ACI, such as STEMI or NSTEMI, other causes, such as myocarditis, Takotsubo syndrome (stress cardiomyopathy), acute heart failure, and direct injury from COVID-19 are important etiologies of ACI; however, noncardiac conditions, such as pulmonary embolism, critical illness, and sepsis need also be considered (Table 2). 5,39 The clinical picture of ACI may be confused with acute MI or an MI mimic, such as Takotsubo cardiomyopathy (TTC) or acute myocarditis, whereby coronary angiography and/or cardiac magnetic resonance (CMR) imaging are most helpful, but in certain cases only endomyocardial biopsy (EMB) could render the correct diagnosis, as it was the case in a patient with COVID-19 who was diagnosed with lymphocytic myocarditis only after an EMB was performed. 40,41 Nevertheless, COVID-19 viral myocarditis, i.e. myocarditis caused by direct virus invasion of the myocardium has not convincingly been demonstrated as yet, 41 with possible rare exceptions, 42 as myocardial injury is more likely related to systemic consequences rather than direct damage by COVID-19. 43,44 Thus, due to the low frequency of COVID-19-induced myocarditis and unclear therapeutic implications, investigators have advised against the use of EMB to diagnose myocarditis in the setting of COVID-19. 45 Anyhow, CMR is suggested as the preferred imaging modality for non-invasive evaluation in acute myocarditis, enabling risk stratification and prognostication. 46
Causes of Acute Cardiac Injury or Acute Coronary Syndrome in Patients With and Without COVID-19 Infection.
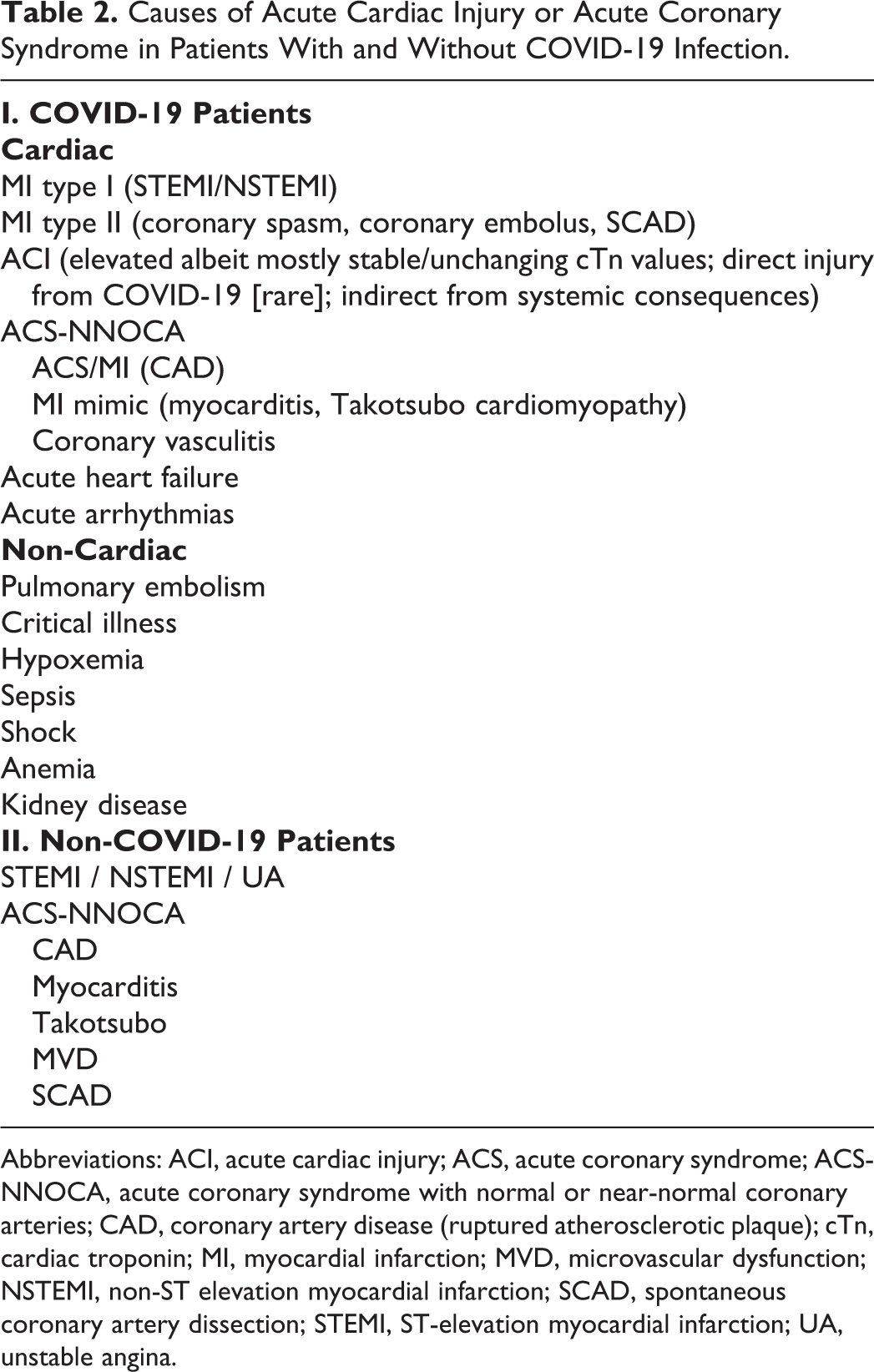
Abbreviations: ACI, acute cardiac injury; ACS, acute coronary syndrome; ACS-NNOCA, acute coronary syndrome with normal or near-normal coronary arteries; CAD, coronary artery disease (ruptured atherosclerotic plaque); cTn, cardiac troponin; MI, myocardial infarction; MVD, microvascular dysfunction; NSTEMI, non-ST elevation myocardial infarction; SCAD, spontaneous coronary artery dissection; STEMI, ST-elevation myocardial infarction; UA, unstable angina.
According to a recent systematic review of CMR imaging findings in 34 studies comprising 199 COVID-19 patients, 79% of the CMRs were abnormal. 47 Myocarditis (40%) was the most prevalent diagnosis. Other findings included perfusion deficits, extracellular volume mapping abnormalities, and pericardial effusion. In the majority of patients, gross left ventricular (LV) function was normal. Kawasaki-like involvement with myocardial edema without necrosis was seen in 4 of 6 children.
A recent review highlights the advantages of chest/cardiac CT and/or CT coronary angiography (CTCA) in evaluating patients with possible ACI vs MI, patients with acute or stable chest pain, patients with pulmonary embolism, patients with possible intracardiac thrombus and patients with valvular heart disease. 48 Thus, appropriate use of a multimodality imaging strategy is most useful to detect ACI and distinguish MI from myocarditis, TTC, pulmonary embolism and other cardiac and chest pathologies in COVID-19 patients. 49,50
Acute Myocarditis
There are case reports of COVID-19 patients presenting with presumed acute myocarditis, many times of the fulminant type, however, there is paucity of confirmatory data via EMB and/or CMR. 51 -56 As mentioned, among 112 COVID-19 patients with ACI, as evidenced by elevated cTn, only 14 (12.5%) patients had abnormalities similar to myocarditis, such as triple elevation in cTnI with values over 0.12 ng/mL, plus abnormalities on echocardiography and/or ECG, albeit without CMR confirmation. 43 A systemic review of 14 patients with COVID-19-related myocarditis (median age 50.4 years) indicated a male predominance (58%), with HTN as the most prevalent comorbid condition (33%). 57 ECG findings were variable, and cTn was reported elevated in 12 cases and creatine kinase-MB in the other 2 cases. Echocardiography, performed in 83% of cases, revealed reduced LV function in 60%. The majority of cases required intubation. Among therapeutic options, glucocorticoids were most commonly used (58%) with a survival rate of 81% (85% for those on steroids). A recent case series reported on 10 patients (8 females) with COVID-19-related myocarditis-like syndrome referred for CMR; 2 patients were diagnosed as TTC and 8 patients had CMR images consistent with myocarditis; all patients fared well with normalization of cTn and recovery of LV function. 58
Recently, in children and adolescents, a Kawasaki-like multisystem inflammatory syndrome with predominant myocarditis associated with COVID-19 infection has been reported. 59 The clinical features of this syndrome overlap with those of Kawasaki disease and toxic shock syndrome. However, myocardial involvement requiring vasopressor support is more common in these patients than in Kawasaki disease (∼50% vs ∼5%), while coronary-artery aneurysms develop less commonly (∼9% vs ∼25%). Data indicate that this syndrome is largely immune-mediated, triggered by COVID-19, with a hyperinflammatory response possibly due to post-infectious cytokine storm, rather than a result of direct myocardial cell injury caused by the virus.
Acute Coronary Syndromes in Patients With COVID-19 Infection
In a prospective multicenter cohort study of 187 patients admitted for acute MI (111 STEMI, 76 NSTEMI), 32 (17%) were diagnosed with COVID-19. 60 GRACE score, Killip classification, and levels of inflammatory markers were significantly higher in COVID-19 patients. Total (25% vs 3.8%; P < 0.001) and CV mortality (15.2% vs 1.8%; P = 0.001) were also higher in COVID-19-patients. GRACE score >140 (OR, 23.45; P = 0.005) and COVID-19 (OR, 6.61; P = 0.02) were independent predictors of in-hospital death.
Another prospective study of 26 STEMI patients admitted during the pandemic reported that 7 (26.9%) of these patients tested positive for COVID-19. 61 Median time from symptom onset to hospital admission was significantly longer in 2020 as compared to the historical cohort (15 vs 2 h; P < 0.01); also, more patients presented late compared with the historical cohort (50% vs 4.8%; P < 0.01). Primary PCI was performed in fewer patients (80.8% vs 100% in the historical cohort; P = 0.06). A multicenter retrospective study of 78 patients with COVID-19 infection and STEMI (median age 65 years, 63% men) reported that during hospitalization, 8 (10%) developed acute respiratory distress syndrome (ARDS), 14 (18%) required mechanical ventilation, 19 (24%) were treated with primary PCI and 59 (76%) were treated with fibrinolytic therapy. 62 A total of 13 (17%) patients required cardiac resuscitation, and 9 (11%) died. Among those treated with PCI (n = 19), a high rate of stent thrombosis (21%) was reported. Finally, a report from Italy of 547 patients hospitalized for ACS (45% STEMI) indicated that the mean admission rate for ACS during the study period was 13.3 admissions per day compared to 18.9 admissions per day during the previous year (incidence rate ratio, 0.70; P < 0.001). 63 The authors also reported a significant increase in mortality during this period that was not fully explained by COVID-19 cases alone.
Thus, in the COVID-19 era, STEMI patients with concurrent COVID-19 infection seem to represent ∼17%-27% of patients admitted with STEMI. Patients admitted with any type of ACS present relatively late to the hospital compared to pre-pandemic periods; fewer patients are submitted to PCI; for a variety of reasons to be discussed later, ACS patients have worse prognosis in the pandemic era compared to the pre-pandemic era.
Acute Coronary Syndromes With Normal or Near-Normal Coronaries
Acute coronary syndromes with normal or near-normal coronary arteries (ACS-NNOCA), comprising MI with non-obstructive coronary arteries (MINOCA) or MI with normal coronary arteries (MINCA) and ischemic syndromes with non-obstructive coronaries (INOCA), 10 are being increasingly reported in patients with COVID-19 infection (Table 2). 64 -66 In a case series of 18 COVID-19 patients presenting with STEMI, 3 of 9 (33%) patients undergoing coronary angiography did not have obstructive coronary artery disease (CAD). 67 In an observational study of 118 consecutive confirmed COVID-19 patients (median age 66 years, all men) undergoing transthoracic echocardiography, 5 (4.2%) patients had features compatible with TTC; however, these patients had no coronary angiography to exclude CAD. 68 There have been several case reports of TTC in patients with COVID-19; 69 -75 one particular case with reverse TTC (akinesia of the LV basal and midventricular wall with apex sparing) was reported to complicate the course of fulminant COVID-19 associated with cytokine release syndrome, whereby inotropic therapy failed, and the patient responded well to therapeutic plasma exchange. 76 In a literature review that yielded 16 COVID-19 patients with TTC (median age 57; 50% male) of which 11/16 patients’ individual data were available, 4 out of 11 (36.4%) patients had cardiac complications such as atrial fibrillation, pericardial effusion, cardiogenic shock, and heart failure. 74 A recent case report described a COVID-19 patient who presented with MINOCA (NSTEMI) and CTCA showed signs of vasculitis with diffuse wall irregularities and focal thickening, which was considered to have triggered endothelial dysfunction and vasospasm. 65
A prospective study enrolled all STEMI patients who underwent primary PCI during the COVID-19 period (83 patients) and compared them with a previous cohort of STEMI patients (2008-2017, n = 1,552 patients); non-COVID-19 patients (n = 72) were also compared with COVID-19 patients (n = 11). 66 Patients during the outbreak period were older, significantly delayed seeking care and sustained a two-fold higher in-hospital mortality. Higher biological markers of inflammation (C-reactive protein), fibrinolysis (D-dimer), and antiphospholipid antibodies in 4 cases were observed in the COVID-19 group. In the COVID-19 group, MINOCA (defined as thrombotic MI non-atherosclerotic coronary occlusion) was observed in 6 of 11 cases (54.5%) vs 5 of 72 cases in the non-COVID-19 group (1.4%) (P < 0.001) and associated with higher post-procedure distal embolization (72.7% vs 30.6%, P = 0.007). The in-hospital mortality was higher in the COVID-19 group (27.3% vs 5.6%, P = 0.016).
Thus, in patients with COVID-19 infection, a garden variety of ACS-NNOCA may be observed ranging from ruptured pre-existing or new atherosclerotic plaques to other ischemic or non-ischemic syndromes, like TTC or acute myocarditis. 57,64,73 -75,77 -79 Importantly, compared with the non-COVID-19 patients, the prevalence of ACS-NNOCA in COVID-19 patients appears to be much higher, reported at ∼33%-55% of patients with COVID-19 presenting with STEMI, 66,67,80 when ACS-NNOCA has been reported to occur in 3.5%-14.5% in non-COVID patients presenting with ACS; 10 the reasons behind this discrepancy have not been elucidated (see discussion on mechanisms below). Notably, the risk of sudden cardiac death (SCD) in patients with ACS-NNOCA remains a major concern; myocardial ischemia, inflammation, and fibrosis are probably at the core of the SCD risk in these patients. 81
Non-COVID-19 Patients
On the other hand, the pandemic may also account for cases of ACS-NNOCA in patients without COVID-19 infection. Interestingly, in these patients, the fear or stress that this pandemic instigates appears to be the trigger for ACS-NNOCA. These may include cases of coronary spasm, TTC, myocarditis, etc. (Table 2). 10,12,65,82,83
A retrospective cohort study of 1914 patients presenting with ACS (1656 in the pre-COVID-19 period and 258 patients during the COVID-19 pandemic period) indicated that there was a significant increase in the incidence of stress cardiomyopathy (TTC) during the COVID-19 period compared with the pre-pandemic period (20 patients or 7.8% vs 5-12 patients or 1.5%-1.8% in the pre-COVID-19 period). 12 Patients with TTC during the COVID-19 pandemic had a longer median hospital length of stay (8 vs 4-5 days; P = 0.006), while mortality was similar (1 patient in each period).
Thus, it becomes apparent that there may be an increase in the numbers of MI/ACS mimickers in the era of COVID-19 and caution is due to render proper diagnosis in patients with or without COVID-19 presenting to the emergency room with chest pain. Multimodality CV imaging including standard and newer echocardiography techniques, CTCA, and CMR may guide diagnosis and management (Figure 2). 84 -86 Cardiovascular imaging may offer several advantages in non-invasively evaluating COVID and non-COVID patients with cardiac symptoms during the COVID-19 pandemic (Figure 2). 48,87,88 Newer echocardiography techniques, such as LV global longitudinal strain, may uncover subclinical myocardial dysfunction in a large proportion (∼80%) of patients hospitalized with COVID-19, while gross LV dysfunction with decreased LV ejection fraction and wall motion abnormalities are less frequent findings (22%-23%). 87 Myocardial strain imaging may detect myocardial dysfunction in almost all critically ill COVID-19 patients. 89 Nevertheless, in the majority, if not all, patients, coronary angiography will be needed to visualize the coronary arteries; in those with non-significant or absent coronary lesions, it would be advisable to perform LV angiography that could hasten and confirm certain diagnoses, like TTC. 10

An algorithm is proposed to investigate the causes of Acute Cardiac Injury (ACI) in patients with COVID-19 infection that includes clinical assessment, ECG, echocardiography and newer strain imaging techniques, high-sensitivity cardiac troponin (cTn), invasive and noninvasive coronary angiography, chest computed tomography and cardiac magnetic resonance (CMR) imaging. N.B.: CMR stands out as the preferred imaging modality for non-invasive evaluation in ACI, also enabling risk stratification and prognostication (see text for discussion). ACS-NNOCA indicates Acute Coronary Syndrome with Normal or Near-Normal Coronary Arteries; CAD, (atherosclerotic) coronary artery disease; CMR, cardiac magnetic resonance imaging; CT, computed tomography; CTCA, computed tomography coronary angiography; cTn, cardiac troponin; ECG, electrocardiogram; LV, left ventricular; MI, myocardial infarction; NSTEMI, non-ST-elevation myocardial infarction; PCI, percutaneous coronary intervention; PE, pulmonary embolism; STEMI, ST-elevation myocardial infarction; TTC, Takotsubo cardiomyopathy; Δs, changes.
Mechanisms for COVID-19-Related ACS and ACI
Acute Coronary Syndrome
Various mechanisms may be involved in the development of
Acute Cardiac Injury
The pathogenesis of COVID-19 infection-related
Another mechanism of myocardial injury may relate to cardiomyocyte damage from severe hypoxemia and hypoperfusion, both complicating COVID-19 infection via pulmonary infection and hemodynamic compromise induced by viral sepsis (imbalance of oxygen supply and demand; type II MI). 109 This mechanism may be accentuated in patients with underlying CV disease such as CAD and heart failure. Finally, as already mentioned, the associated hyperinflammatory state, the cytokine storm, may lead to myocardial damage, as well as to other organ (multi-organ) damage and failure, especially in severe COVID cases with the attendant excessive inflammatory response. 110
In the end, the interplay between the inflammatory, coagulation, complement and endothelial systems in COVID-19 may account for the ensuing CV complications. 111,112 COVID-19-induced inflammation may involve primary vessel inflammation, possible sepsis and a secondary reaction to tissue damage caused by the virus, leading to generation and release of inflammatory mediators. 113 In addition to acute lung injury and multi-organ failure, a cytokine storm, typically associated with concurrent serum ferritin rises and hemodynamic instability, may also lead to vascular damage. 114 Pulmonary thrombosis, not necessarily preceded by deep venous thrombosis, but rather originating primarily in the lungs, may account for the observed “pulmonary embolism” cases. 95 COVID-19 can confer a hypercoagulable state via activation of the contact and tissue factor pathways 115 ; direct viral myocardial and microvascular injury leads to exposure to subendothelium and collagen, producing platelet and possibly contact pathway activation. 111 SARS-CoV-2–platelet interactions result in platelet activation and aggregation in COVID-19, further enhancing the pro-thrombotic vascular milieu. 116 Evidence suggests that COVID-19 leads to excessive production of neutrophil extracellular traps (NETs) (NETosis), especially in patients with severe disease, which is a key mechanism that predisposes to untoward effects including thromboembolic complications and damage to surrounding tissues and organs. 117 COVID-19 microthrombus formation seems to be more closely related to endothelial damage and complement-mediated thrombotic microangiopathy, rather than sepsis-induced coagulopathy or disseminated intravascular coagulation (DIC). 118
Acute cardiac injury in COVID-19 may be due to virus-mediated lysis of myocardial cells, also observed in other viral infections, or as a consequence of COVID-binding ACE2 receptors in the heart, thus reducing the activity of ACE2 and dampening the cardioprotective effects of this enzyme. 119 COVID-19-induced inflammation resulting in substantial cytokine release can also result in atherosclerotic plaque instability, rupture and subsequent arterial thrombus formation, leading to coronary thrombosis and acute MI. 120 Finally, COVID-19-induced endothelial dysfunction may play a key role in the development of micro- and macro-vascular complications in the CV system. 106
Patient Delay in Seeking Care and Visiting the Emergency Department/Re-Emergence of Post-MI Mechanical and Other Complications in the COVID-19 Era
In the era of the COVID-19 pandemic, patients hesitate or are reluctant to seek medical care wishing to avoid hospital admission for their health problems lest they contract COVID. Among them, patients with chest pain delay their visit to the emergency room with resultant significant delay in first medical contact, including patients suffering from acute STEMI. 66,121 Thus, a surge of case reports emerges of delayed presentation of STEMI complicated by ventricular septal or LV free wall rupture or acute mitral regurgitation from papillary muscle rupture, mechanical complications that we used to see in the era when thrombolysis and/or primary PCI were not available. 122 -126 A case series of 10 acute MI patients with delayed presentation reported complications such as heart failure and cardiogenic shock, but also complications rarely seen in the primary PCI era including ventricular septal rupture, LV pseudoaneurysm, and right ventricular infarction. 127 Another series of 4 cases of post-MI mechanical complications also warns about the delayed access to healthcare for fear of contracting COVID-19 which led to excessively high mortality (75%). 128 A case of post-MI pericarditis has also been reported. 129
As mentioned, another case series of 78 COVID-19 positive patients presenting with STEMI found a high rate (76%) of thrombolysis vs primary PCI (24%), a high rate of stent thrombosis (21%), and 11% in-hospital mortality. 62
According to a UK study, during lockdown, a greater than 50% drop was noted in the number of patients presenting to cardiology and those diagnosed with MI. 130 Similarly, a study from China indicated a 51.4% decrease in hospital admissions of STEMI patients during the peak period of COVID-19 epidemic. 131 Importantly, lack of reperfusion therapy for STEMI patients was >10% higher in 2020 than the previous 2 years; 2-3 times more STEMI patients received fibrinolysis in 2020 than the 2 previous years, while the volume of primary PCI dropped by more than half. This led to highest mortality rate recorded in February 2020.
A similar study from Greece indicated a lowest number of acute MI cases in March 2020 compared to the number of MI cases in the same month in the preceding 3-year period (P < 0.001); also, there was a significant 30%-40% reduction in the visits to the cardiac emergency room of the hospital during the first 3 months of the pandemic period. 132
According to a large cohort study from China comprising 28,189 STEMI patients, the COVID-19 outbreak reduced the number of STEMI cases reported to China chest pain centers, the percentage of patients undergoing primary PCI declined, while the percentage of patients undergoing thrombolysis increased. 8 With an average delay of ∼20 min for reperfusion therapy, the rate of in-hospital mortality and in-hospital heart failure increased during the outbreak; the rate of in-hospital hemorrhage remained the same.
In the same context, a recent report of data from 18 hospitals or healthcare systems in the US from January 2019 to April 2020 indicated that the COVID-19 pandemic adversely affected many aspects of STEMI care, including timely access to the cardiac catheterization laboratory for primary PCI. 7 There was a marked reduction in the number of activations for STEMI (29%), which drove a significant decline in the number of activations leading to angiography (34%) and number of activations leading to primary PCI (20%). Similarly, a large US cohort study analyzing 15,244 MI hospitalizations between December 30, 2018, and May 16, 2020 (4955 for STEMI [33%] and 10,289 for NSTEMI [67%]) indicated that beginning February 23, 2020, MI-associated hospitalizations decreased during the early COVID-19 period, while thereafter they started to increase again. 133 The observed to expected mortality ratio for MI increased during the early period, disproportionately associated with patients with STEMI. In the same context, a report from Israel pointed to a resurge of MIs with rebound increase in STEMI hospitalizations coinciding with the fading of the first wave of the COVID-19 pandemic. 134
Finally, a French population-based, observational study assessing the incidence and outcomes of out-of-hospital cardiac arrest (OOHCA) in an urban region during the COVID-19 pandemic, indicated that, compared with non-pandemic periods, the maximum weekly OOHCA incidence increased from 13.42 to 26.64 per million inhabitants (P < 0.0001), before returning to normal in the final weeks of the pandemic period. 135 There was a higher rate of OOHCA occurring at home (90.2% vs 76.8%; P < 0.0001), less bystander cardiopulmonary resuscitation (47·8% vs 63·9%; P < 0.0001) and shockable rhythm (9·2% vs 19·1%; P < 0.0001), and longer delays to intervention (median 10.4 min vs 9.4 min; P < 0.0001). The number of patients with resuscitated OOHCA admitted alive decreased from 22.8% to 12.8% (P < 0.0001) in the pandemic period. COVID-19 infection accounted for about a third of the increase in OOHCA incidence during the pandemic. This is in keeping with the noted higher incidence of life-threatening arrhythmias incurred by COVID-19-associated ACI and ACS. 92 Furthermore, ACS-NNOCA may also trigger malignant arrhythmias and sudden cardiac death. 81
Thus, there is a reduced number of admissions for ACS but also a significant delay in ACS presentation consistently reported during the COVID-19 pandemic era. 7,130,131,136 There is fear supported by important preliminary evidence that this observed pattern may lead to increases in OOHCA, acute mechanical and long-term complications of MI and missed chance to implement secondary prevention therapies for patients with CAD. 127,128,135,136
Coronary Thrombus and Coronary Stent Thrombosis
According to an observational study of 115 consecutive patients admitted with STEMI and managed with primary PCI, those presenting with concurrent COVID-19 infection had higher rates of multivessel thrombosis, stent thrombosis, higher thrombus burden, higher use of glycoprotein IIb/IIIa inhibitors and thrombus aspiration; myocardial tissue perfusion, as reflected by myocardial blush grade, and LV function were significantly lower in patients with COVID-19 with STEMI. 97 Multiple coronary thromboses causing STEMI were reported in a patient with COVID pneumonia who was managed with thrombo-aspiration, coronary stenting and combined antiplatelet and anticoagulant therapy. 137
Furthermore, a recent case report of STEMI indicated the presence of microvascular thrombi accounting for the dismal course of this STEMI patient in the absence of epicardial vessel occlusion. 138 On the other hand, a COVID-19 patient presenting with STEMI was found to have LV thrombus despite receiving anticoagulation; D-dimer levels were excessively elevated and the patient succumbed to his disease. 139
Case reports and series of acute and late stent thrombosis are increasingly being presented in patients with COVID-19 infection. 62,140 -142 In a case series of 78 patients with STEMI, of whom 19 were treated with primary PCI and stenting, 4 patients (21%) developed stent thrombosis. 62
Thus, a heavy thrombus burden involving the coronary macro- and micro-vessels, as well as the cardiac cavities, has been reported in COVID-19 patients presenting with STEMI, who also have a higher risk of stent thrombosis. 95 Whether selective thromboaspiration might improve procedural and clinical outcome in these patients remains to be proven. 143
Guidelines
STEMI/ Mode of Reperfusion in the COVID-19 Era
As mentioned, a high rate of thrombolysis (76%) was reported in an early series of 78 COVID-19 patients presenting with STEMI. 62 Similarly, in a large cohort study from China comprising 28,189 STEMI patients, the percentage of patients undergoing primary PCI declined (OR 0.76; P < 0.001), while the percentage of patients undergoing thrombolysis increased (OR: 1.66; P < 0.001). These results are in accordance with early national STEMI protocols in China and Taiwan that recommended prioritizing thrombolysis. 8,144 However, although a decreasing trend toward primary PCI and an increasing use of thrombolysis as first approach to patients with STEMI had become apparent during the early phase of the pandemic, current guidelines still support primary PCI as the preferred strategy. 145,146
In keeping with objections to thrombolysis as first approach to STEMI in the COVID-19 era and in accordance with the established superiority of primary PCI in managing STEMI patients, a recent European Society of Cardiology (ESC) guidance document recommends primary PCI for all STEMI patients. 147 Specifically, the guidance indicates that primary PCI remains the reperfusion therapy of choice if feasible within the time frame of 120 min and performed in facilities approved for the treatment of COVID-19 patients in a safe manner for healthcare providers and other patients; primary PCI may be delayed during the pandemic (up to 60 minutes) for reasons of logistics; if the target time cannot be met and fibrinolysis is not contraindicated, fibrinolysis should then become first line therapy. 147 They also point out that any STEMI patient should be considered potentially infected since commonly the COVID-19 test results are not immediately available.
Similarly, the American Heart Association (AHA) indicates that in the absence of significant system resource constraints, PCI should remain the primary and preferred reperfusion strategy for patients with STEMI based on superior outcomes with PCI including preservation of LV function and lower rates of reinfarction, stroke, and death. 145 Furthermore, the AHA states that testing for COVID-19 should not delay primary PCI for those with clear STEMI. Fibrinolysis should be considered for patients with STEMI who cannot receive PCI and coronary reperfusion within 120 minutes.
A recent Consensus Statement from the Society for Cardiovascular Angiography and Interventions (SCAI), American College of Cardiology (ACC), and the American College of Emergency Physicians (ACEP) emphasizes the need for primary PCI to remain the standard of care for STEMI patients during the COVID-19 pandemic at PCI-capable hospitals when it can be provided in a timely fashion, with an expert team fitted with personal protection equipment (PPE) in a dedicated catheterization laboratory. 148 They recommend a fibrinolysis-based strategy at non-PCI capable hospitals or in specific situations where primary PCI cannot be performed or is not considered the best option.
Myocarditis
The ESC recommends treating patients with acute myocarditis complicated by cardiogenic shock with inotropes and/or vasopressors and mechanical ventilation. 149 Additionally, in patients requiring longer-term support, extracorporeal membrane oxygenation (ECMO) and LV assist devices should be used.
By and large, glucocorticoids and immunoglobulin therapy are not supported for routine therapy in acute myocarditis, especially in infection-positive forms, as based on prior studies, reviews and the ESC recommendation. 149 -151 However, there are case reports of successful treatment of COVID-19 fulminant myocarditis using antiviral therapy (lopinavir-ritonavir), immune-modulators (interferon alpha-1β, methylprednisolone, immunoglobulin) and supportive measures (inotropes, ECMO). 152 -154 As mentioned, a recent review of 14 patients showed favorable outcomes in COVID-19 patients with myocarditis treated with steroid therapy. 57 In a pediatric series of 20 children presenting with fulminant myocarditis and shock, all children but one received inotropic/vasoactive drug support, all received IV immunoglobulin (with adjuvant corticosteroids administered in 2), and all children survived and were afebrile with a full LV function recovery at discharge from the ICU. 155
Conclusion
Acute cardiac injury (ACI), defined by elevated cTn levels above the 99th percentile, constitutes the most commonly reported CV abnormality in COVID-19 infection, associated with high mortality rates. In addition to clinically and electrocardiographically discernible causes of ACI, such as STEMI or NSTEMI, other causes need to be considered such as myocarditis, Takotsubo syndrome, acute heart failure, and direct injury from COVID-19; furthermore, noncardiac conditions, such as pulmonary embolism, critical illness, and sepsis need also be taken into account (Table 2). ACS-NNOCA appears to have a higher prevalence in both COVID-19 positive and negative patients in the pandemic era, likely due to associated stress incurred by the pandemic, with most data particularly supporting an increased incidence of TTC. Echocardiography with its new strain imaging techniques, chest CT, CTCA or invasive coronary angiography and/or CMR imaging are most helpful in the differential diagnosis (Figure 2), obviating the need for endomyocardial biopsy to render a diagnosis of myocarditis and/or differentiate from other causes of ACI detailed in this review. CMR is singled out as the preferred imaging modality for non-invasive evaluation in ACI, also enabling risk stratification and prognostication. 46
Several studies have now documented a significant reduction of hospital access for patients with STEMI or any type of ACS in the COVID-19 era with an increase in treatment delay, longer hospitalization, higher levels of cTn, higher rates of LV dysfunction, higher rates of thrombolytic treatment of STEMI vs primary PCI and worse clinical outcomes. 6,8,9,60,62,156
Despite a tendency of preferring less invasive approaches in ACS patients during the pandemic, e.g. by administering thrombolysis to more STEMI patients, professional societies still emphasize the need for primary PCI to remain the standard of care for STEMI patients at PCI-capable hospitals when it can be provided in a timely fashion, with an expert team fitted with PPE in a dedicated catheterization laboratory, leaving fibrinolysis-based strategies for non-PCI capable hospitals or in situations where primary PCI cannot be performed within standard timelines.
Perspective
Acute cardiac injury with cTn levels >99th percentile occurs in a considerable percentage of patients afflicted by COVID-19 due to a variety of causes related to this viral pandemic and portends a poor prognosis. Improved understanding of the acute and chronic sequelae of ACI and CV involvement incurred by COVID-19 infection with use of CMR and other CV imaging techniques (e.g., newer echo techniques) may help us to better monitor these patients and devise preventive and therapeutic strategies and finally teach us how to prevent similar calamities in the future. Newer therapies and effective vaccination may hopefully halt a downward spiral and restrain and contain this disease.
In this pandemic era, digital health services, with telemetry via either standard, mobile or wearable monitoring systems, are quickly expanding to protect both patients and health care personnel. 157 However, patient access issues need to be urgently addressed during this pandemic in order to reduce inordinate delays for COVID and non-COVID patients to receive appropriate cardiac (e.g., primary PCI for acute STEMI) and other therapies that may lead to worse clinical outcome with increased morbidity and mortality.
Footnotes
Author Contributions
All authors contributed to the preparation of this manuscript and approved the final version. ASM conceived and designed the project, analyzed the data, wrote the initial draft, and edited the final product; AAM conducted literature search, constructed the Tables and edited/revised the manuscript; TAM conducted literature search, designed the Figures and edited/revised the manuscript; HM analyzed the data, reviewed, revised, and edited the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.