
Abstract
Purpose:
This study aims to analyze the treatment patterns and goal attainment of low-density lipoprotein cholesterol (LDL-C) among patients with atherosclerotic cardiovascular disease (ASCVD) and diabetes mellitus (DM) in the real-world setting in Fuzhou, China.
Methods:
Patients aged ≥20 years with a valid LDL-C measurement (index date) in 2016 were selected from National Healthcare Big Data in Fuzhou, China. Patients were stratified into mutually exclusive cardiovascular risk categories: ASCVD (including recent acute coronary syndrome [ACS], chronic coronary heart disease [CHD], stroke, and peripheral arterial disease [PAD]), and DM alone (without ASCVD). Lipid-modifying medication and LDL-C attainment at the index date were assessed.
Results:
A total of 21 989 patients met the inclusion criteria, including 17 320 (78.8%) with ASCVD and 4669 (21.2%) with DM alone; 47.7% of patients received current statin therapy in the overall cohort (53.5% in ASCVD, 26.5% for DM); 20.5% ASCVD population achieved LDL-C target with the highest in patients with recent ACS (33.8%), followed by chronic CHD (21.2%), PAD (20.9%), and ischemic stroke (17.3%); 49.0% of patients with DM achieved LDL-C target. Higher LDL-C attainment was observed in high-intensity statin and a combination of statin and nonstatin groups. Atorvastatin was the most commonly used statin with the highest LDL-C attainment, followed by rosuvastatin.
Conclusion:
Compared with previous studies in China, our study found a relatively low statin use and LDL-C target attainment, but higher than similar studies in Europe. Guidelines should be well complied and more prescription of high-intensity statin or statin and nonstatin combination should be advocated.
Introduction
Cardiovascular diseases (CVDs) are the single largest cause of mortality in the world, 1 accounting for more than 40% of deaths in China. 2 Although age-standardized mortality rates for CVDs in China have declined between 1990 and 2016, the prevalence of age-standardized CVDs increased by 14.7% and prevalent cases of CVD doubled since 1990, reaching nearly 94 million in 2016. 3,4 Reducing low-density lipoprotein cholesterol (LDL-C) levels with statin therapy has been shown to reduce all-cause mortality and the occurrence of major cardiovascular outcomes among patients with and without atherosclerotic cardiovascular disease (ASCVD). 5 -8 The Dyslipidemia International Study (DYSIS)-China showed that the achievement rate of LDL-C target (<1.8 mmol/L) was 26.1% in very high risk (having acute coronary syndrome [ACS], ischemic stroke or coronary heart disease [CHD] plus diabetes mellitus [DM]) patients with metabolic syndrome and 27.4% in patients without metabolic syndrome. 9 Various studies had been carried out in the European countries on the lipid management among very high-risk population, the LDL-C achievement of less than 1.8 mmol/L was 13.9% in French, 10 8.5% in Germany 11 among population with ASCVD, and 16.0% in Italian among overall ASCVD and DM cohort. 12
Statins are currently the first choice for lipid-lowering therapy (LLT). Their effectiveness and safety in reducing secondary coronary artery events have been fully demonstrated. 6,13 -15 Furthermore, high-intensity statin therapy is more effective than traditional therapy in lowering LDL-C level and improving cardiovascular risk. 16 -19 Low-density lipoprotein cholesterol is the primary intervention target for LLT. 4 Guidelines for the prevention and treatment of adult hyperlipidemia in China (2016 Revision) show that LDL-C <1.8 mmol/L (<70 mg/dL) or a ≥50% reduction from baseline LDL-C would be the target for patients with very high cardiovascular risk (defined as established ASCVD). 20 For patients with high cardiovascular risk (defined as LDL-C ≥4.9 mmol/L or total cholesterol [TC] ≥7.2 mmol/L; patients with DM (LDL-C at 1.8-4.9 mmol/L [or TC 3.1-7.2 mmol/L] and age ≥40 years old); a 10-year risk ASCVD ≥10%), LDL-C treatment targets were < 2.6 mmol/L (<100 mg/dL) or a 30% reduction from baseline LDL-C. 20
Literature describing the use of statins and the achievement of lipid targets in patients with high-risk CVD in China is limited. 21,22 Using electronic medical record (EMR) in Fuzhou, we aim to reveal the status of statin used in LLT and the achievement of LDL-C target in the Chinese population within ASCVD: recent ACS, chronic CHD, ischemic stroke, peripheral arterial disease (PAD), and DM.
Methods and Material
Data Source and Study Population
A retrospective cross-sectional study was performed by retrieving data from an existing electronic health record database (National Healthcare Big Data, Fuzhou, China). This database contains over 23 million patients (from September 2001 to January 2018 in 37 hospitals) with more than 2 billion medical records in this city. These data sets contain the major clinical information systems such as hospital information system, laboratory information management system, EMR, picture archiving and communication systems, surgical information, and medical record information.
Based on the unified database platform, the clinical information data adopt the platform management, including the data processing and operation services of the IIIa hospitals, so as to realize the structured and standardized integrated management. In addition to the above data sources, Synyi artificial intelligence company employs natural language processing techniques on diagnosis and structured data from EMR. Diagnostic and clinical data are coded using International Classification of Diseases, 10th Revision Procedure Coding System. Recent ACS was defined as myocardial infarction (MI) or unstable angina requiring hospitalization within the 12 months before the index date. Chronic CHD was defined as a history of MI or unstable angina >12 months prior to the index date and within the baseline period, stable angina, coronary revascularization, or other chronic ischemic heart disease. Ischemic stroke was defined as a history of ischemic stroke within 1 year prior to the index date. Peripheral arterial disease was defined as peripheral vascular disease by noncoronary atherosclerotic disease, abdominal aortic aneurysm, and carotid artery stenosis within 1 year prior to the index date. Diabetes mellitus included both type 1 DM and type 2 DM within 1 year. This study was approved by China Ethnic Committee of Registering Clinical Trials (ChiECRCT-20190003). All procedures performed in the study conform to the ethical guidelines of the 1975 Declaration of Helsinki. The present study retrospectively analyzed data abstracted from the medical chart and national health database; thus, informed consent was not required.
Inclusion criteria were age ≥20 years; at least 1 valid LDL-C measurement in 2016, the last measurement day was defined as the index date; ≥1 high/very-high CV risk condition; and ≥2 years enrollment in the database.
Lipid-Lowering Therapy
Patients with evidence of drug prescription record within 30 days before the index date were considered as receiving current LLT. Patients with a prescription for LLT more than 30 days before the index date within 2 years were considered the previous LLT. Patients with no evidence of any drug prescription were considered no LLT. Lipid-lowering therapies were classified into statins LLT (individual or combined use of other drugs) and nonstatins LLT. Furthermore, statins LLT were stratified into high-intensity statins LLT (atorvastatin ≥40 mg once dose, rosuvastatin ≥20 mg once dose, and simvastatin ≥80 mg once dose), and low- to moderate-intensity statins (all other statins and doses). Nonstatin LLT included ezetimibe, niacin (nicotinic acid), fibrates (gemfibrozil, fenofibrate, fenofibric acid, ciprofibrate, and bezafibrate), and bile acid sequestrants (cholestyramine, colesevelam, and colestipol). The treatment pattern was considered high-intensity therapy if only one record of high-intensity statin LLT was available.
Statistical Analysis
Demographic and clinical characteristics, the most recent LLT drug use before the index date, LLT utilization among each type of ASCVD, and stratified LDL-C levels were summarized via proportions and mean ± standard deviation (SD), as appropriate. All analyses were conducted with SAS software, version 9.4 (SAS Institute, Cary, North Carolina).
Results
Patient Demographics and Clinical Characteristics
Overall, 21 989 patients met the inclusion criteria (Supplemental Figure 1.), including 17 320 (78.8%) patients with ASCVD and 4669 (21.2%) patients with DM alone. Specifically, the patients with ASCVD-stratified classification were 346 (1.6%) ACS, 12 498 (56.8%) chronic CHD, 4285 (19.5%) ischemic stroke, and 191 (0.9%) PAD. The mean (SD) age of patients included in this study was 68.8 ± 12.2 years in the whole cohort and ranged from 61.9 ± 12.4 years in patients with DM to 70.8 ± 11.4 years in patients with chronic CHD. The mean (SD) LDL-C ranged from 2.39 ± 1.09 mmol/L in patients with ACS to 2.73 ± 0.99 mmol/L in patients with ischemic stroke (Table 1).
Baseline Characteristics for the Overall Study Cohort and Hierarchical CV Risk Subgroups.
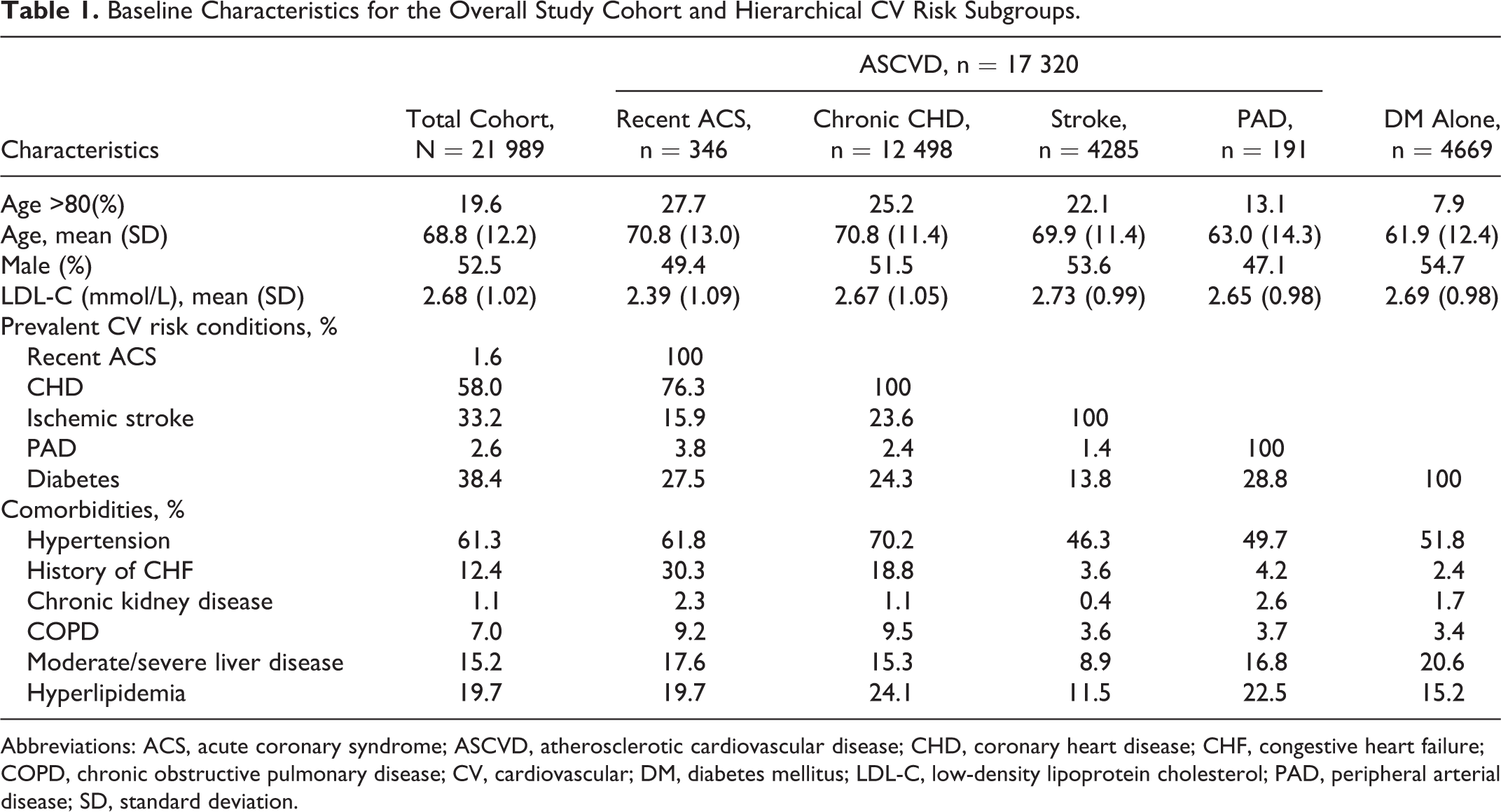
Abbreviations: ACS, acute coronary syndrome; ASCVD, atherosclerotic cardiovascular disease; CHD, coronary heart disease; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; CV, cardiovascular; DM, diabetes mellitus; LDL-C, low-density lipoprotein cholesterol; PAD, peripheral arterial disease; SD, standard deviation.
Lipid-Lowering Utilization
Total cohort
Overall, 48.5% of patients were prescribed LLT within 30 days prior to the index date; 47.7% of patients received statins (3.6% high-intensity statins and 44.2% low- to moderate-intensity statins); 0.8% received nonstatin LLT (Table 2). A total cohort of 19.4% had evidence of prior LLT (but not currently treated); 32.1% of the patients had no evidence of prior LLT.
Use of LLT Overall and By Hierarchical Disease Categories.

Abbreviations: ACS, acute coronary syndrome; ASCVD, atherosclerotic cardiovascular disease; CHD, coronary heart disease; DM, diabetes mellitus; LLT, lipid-lowering treatment; PAD, peripheral arterial disease.
Atherosclerotic cardiovascular disease population
Among patients with ASCVD, 54.2% of the patients were prescribed any LLT as of the index date within 30 days (4.3% high-intensity statins, 49.2% low- to moderate-intensity statins, and 0.7% nonstatin LLT). 20.3% of the patients were prescribed prior LLT and 25.5% of the patients had no evidence of any LLT prescription within 2 years before the index date. The current statin treatment rate (78.9%) was the highest among patients with recent ACS, followed by stroke (60.5%), chronic CHD (50.7%), and PAD (33.0%). Patients with recent ACS also had the highest high-intensity statin treatment rate both in the current treatment (26.0%) and prior treatment (39.0%). Chronic CHD had the highest proportion of prior LLT (22.1%; Table 2).
Diabetes mellitus alone
Only 27.5% of the patients with DM alone received LLT treatment, 1.0% were high-intensity statin treatment and 25.5% were low- to moderate-intensity statin treatment (Table 2). Also, 56.5% had no evidence of prior LLT (Table 2).
Low-Density Lipoprotein Cholesterol Goal Attainment (2011 Chinese Adult Dyslipidemia Prevention Guidelines)
Total cohort
The mean (SD) LDL-C was 2.68 (1.02) mmol/L in the total cohort at the index date (Table 1); 19.9% and 50.6% of the overall patients achieved LDL-C target of <1.8 and <2.6 mmol/L, respectively; 26.6% of patients at high or very high risk achieved the LDL-C attainment.
The goal achievement of LDL-C < 1.8 mmol was higher among currently prescribed with high-intensity statin and low- to moderate-intensity statin (26.4% and 25.6%, respectively), the other 3 groups (currently prescribed with nonstatin prescription, previous LLT, and no evidence of LLT) had a relatively lower goal achievement of about 15%. The same result was obtained among patients with LDL-C <2.6 mmol/L (Table 3).
Achievement of Lipid Goals by Cardiovascular Risk Category and Treatment Type.

Abbreviations: ACS, acute coronary syndrome; ASCVD, atherosclerotic cardiovascular disease; CHD, coronary heart disease; DM, diabetes mellitus; LDL-C, low-density lipoprotein cholesterol; LLT, lipid-lowering treatment; PAD, peripheral arterial disease.
Atherosclerotic cardiovascular disease population
Among ASCVD population, LDL-C goal achievement of less than 1.8 mmol/L was highest in patients with recent ACS (33.8%), followed by chronic CHD (21.2%), PAD (20.9%), and ischemic stroke (17.3%). Mean LDL-C of patients with recent ACS was also the lowest among patients with ASCVD (Table 1). The proportion of patients with 1.8 mmol/L < LDL-C < 2.6 mmol/L varied little among stratified patients with ASCVD (Table 3).
Diabetes mellitus alone
Among patients with DM alone, mean (SD) LDL-C was 2.69 (0.98) mmol/L for patients at the index date. Goal achievement of LDL-C < 1.8 and <2.6 mmol/L was 17.6% and 49.0%, respectively. The target achievement (LDL-C < 2.6 mmol/L) rate of high-intensity statin treatment was notably higher than that of low- to moderate-intensity statin treatment (68.1% vs 54.0%; Table 3).
Low-Density Lipoprotein Cholesterol Goal Achievements by Treatment Pattern and Statin Type
The average level of LDL-C in statin-treated high-risk and very high-risk patients was significantly lower than that in the past treatment group and nontreatment group. Among the current statin treatment groups, combined statin was associated with lower LDL-C average level and higher LDL-C target achievement (<1.8 mmol/L) compared with monostatin therapy (Table 4).
LDL-C Goal Achievements By Treatment Pattern.
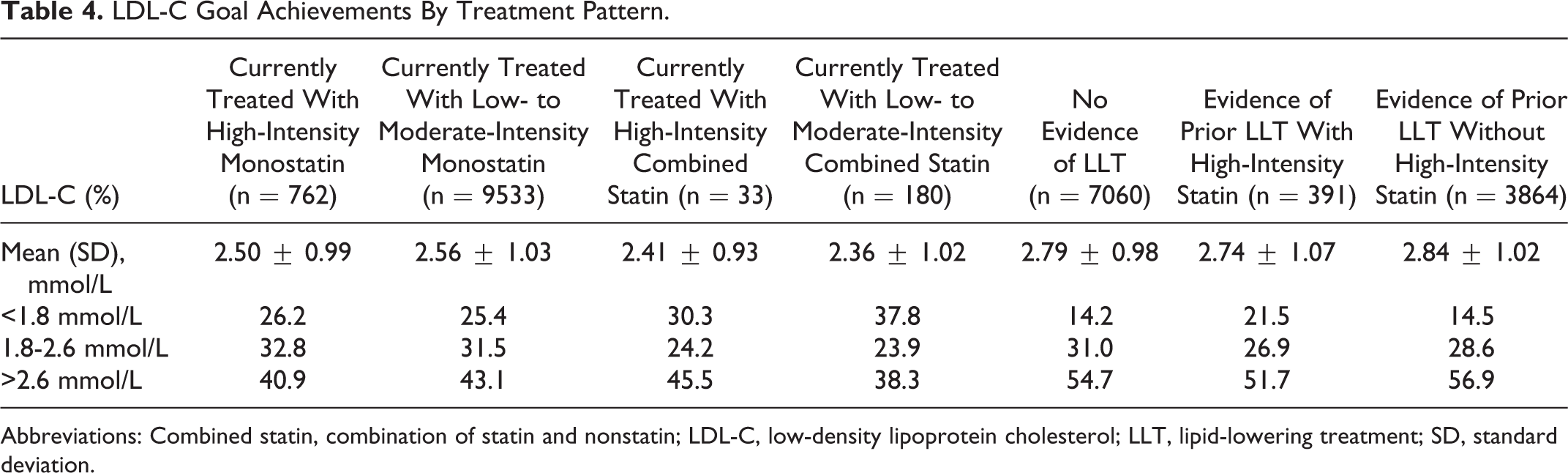
Abbreviations: Combined statin, combination of statin and nonstatin; LDL-C, low-density lipoprotein cholesterol; LLT, lipid-lowering treatment; SD, standard deviation.
Atorvastatin group had the lowest average level of LDL-C (2.45 ± 0.98 mmol/L) and the highest goal achievement both in LDL-C < 1.8 mmol/L (28.4%) and in LDL-C < 2.6 mmol/L (61.2%). Rosuvastatin group followed closely with the second lowest average level of LDL-C (2.57 ± 1.08 mmol/L) and the second highest goal achievement both in LDL-C <1.8 mmol/L (26.9%) and in LDL-C <2.6 mmol/L (57.1%; Table 5).
LDL-C Goal Achievements By Statin Type.

Abbreviations: LDL-C, low-density lipoprotein cholesterol; SD, standard deviation.
The Latest Medication Type Among Patients With Current LLT
Among patients with current LLT, atorvastatin (40.0%) was the most commonly prescribed lipid-lowering drug, followed by rosuvastatin (31.6%), fluvastatin (14.5%), pravastatin (7.4%), and simvastatin (3.9%). The treatment rate of atorvastatin in patients with recent ACS was much higher than that in other patients with ASCVD and DM alone (Supplemental Table 1).
Discussion
This study summarized the use of lipid-lowering drugs among patients with ASCVD and DM in China in 2016 and evaluated the target achievement of LLT for different types of treatment patterns and diseases. Although Chinese and European guidelines strongly recommend statins for the treatment of high-risk cardiovascular patients, 4,23 our study found that only 53.5% of patients with ASCVD and 26.5% of patients with DM were prescribed statins within 30 days prior to the index date. These findings highlight the huge gap between clinical practice in the real world and existing practice guidelines. 4,23
Compared with similar studies in European countries, 24,25 we observed relatively low prescription rates of lipid-lowering drugs in patients at high or very high risk of CVD. Despite the heavy burden of CVD in China, 2 25.5% of patients with ASCVD and 56.5% of patients with DM alone did not receive any LLT within 2 years prior to the index date. Besides, this study found that only 3.6% of patients with ASCVD and 1.0% of patients with DM alone received high-intensity statin therapy within 30 days prior to the index date. It may be related to the recommendation that moderate-intensity statin should be used at the beginning of clinical treatment for the sake of medication safety in Guidelines for the Prevention of Cardiovascular Diseases in China. 4
The Chinese guidelines for the prevention of CVDs point out that statins are the first choice for LLT at present. Relevant studies have shown that the statin use rate in China has increased in recent years. 26 A survey of 1.7 million people in China shows that 9.5% of respondents are at high risk of CVD. Only 0.6% of the respondents in the high-risk cardiovascular group took statins for secondary prevention. 27 Another hospital-based study including 51 972 patients found that 58.8% of the discharge diagnosed patients with ASCVD were prescribed statins between 2008 and 2014, which is consistent with 53.5% current statins prescription rate among patients with ASCVD in our study. 26
In this study, ACS was associated with the highest statin use. The Improving Care for Cardiovascular Disease in China (CCC)-ACS project between 2014 and 2017 demonstrated that 33.9% and 12.7% of patients with ACS with and without a history of ASCVD had been prescribed statins before hospitalization. 28 Another study from the Improving Care for Cardiovascular Disease in China project found that 50.8% of patients with ACS with a history of MI or revascularization were receiving LLT before hospitalization (statin monotherapy in 98.4%, combination in 1.2%). The proportion of patients receiving statin monotherapy reached 91.8%, of which 90.7% were at moderate doses. 29 The CCC-ACS project found that the statin prescription rate of patients with non-ST-segment elevation ACS before discharge was 93%. 30 One previous study in 14 large comprehensive hospitals in Beijing shows that 96.3% of patients diagnosed with acute myocardial infarction were prescribed statin 22 and 80.5% of the patients discharged alive from 53 hospitals across China were prescribed statins. 31 These studies show that for the same group of patients with the same disease, statin treatment rates may vary greatly due to different research designs and procedures. Generally speaking, the prescription rate for statins in the hospital is much higher than that before admission. At the same time, the utilization rate of statin in population epidemiological survey is much lower than that in the hospital-based study. Different criteria for classifying high-risk CVD groups may be the main reason for the above differences. Besides, recall bias and disease concealment in epidemiological surveys, severe illness, more attention on self-health care among patients in the hospital are all potential reasons for different statins utilization as secondary prevention in high-risk CVD groups.
About 82% of patients with CHD discharged from 52 hospitals in 6 cities in China received statin treatment between 2006 and 2007. 32 The statin treatment rate of patients with PAD was much lower than that of patients with CHD (61% vs 22%), which is consistent with our findings. 33
Research from China National Stroke Registry shows that 43.6% of patients with ischemic stroke without a history of prestroke statin treatment were receiving statins during hospitalization after stroke. 34 For patients with noncardiogenic ischemic stroke or transient ischemic attack, long-term treatment with high-intensity statins is recommended to reduce the risk of stroke and cardiovascular events, regardless of other evidence of atherosclerosis. It is recommended that LDL-C be reduced to less than 1.8 mmol/L (70 mg/dL). 4 Our study also found that patients with stroke had a current statin treatment rate of 60.5% (7.2% high-intensity statin), followed by only to patients with ACS among all patients with ASCVD.
Research from 11 community hospitals in Nanjing between 2005 and 2014 shows that 20.9% of patients with DM without CVD history took statins for LDL-C management, which is very close to the result of 26.5% in our study.
The recommendation of moderate-intensity statins for the primary treatment in the Chinese Guidelines may be the underlying cause of the low achievement rate of China’s LDL-C target. Only 20.5% of the patients with ASCVD and 17.6% of the patients with DM alone achieved the LDL-C target of less than 1.8 mmol/L. About 49.0% and 50.9% of the patients with ASCVD and DM alone fail to achieve the target of LDL-C less than 2.6 mmol/L, respectively. Other studies showed similar or higher compliance rate with regard to LDL-C target achievement. For example, 24.7% of patients with ACS with a history of ASCVD achieved the LDL-C target of less than 1.8 mmol/L. 28 The CCC in China project indicated that 30.1% of patient with ACS had LDL-C <70 mg/dL at admission. 29 Diabetic patients of 38% met the target goal and 37.3% of patients who took lipid-lowering agents met LDL-C target goal in 11 hospitals in Naniing. 35
Similar studies on statins utilization and LDL-C achievement among patients with ASCVD and DM alone have been conducted in several European countries, but few have been conducted in Asia. The LDL-C achievement of less than 1.8 mmol/L was 13.9% in French, 10 8.5% in Germany 11 among ASCVD population, and 16.0% in Italian among the overall cohort. 12 Our result of 26.6% attainment in the overall cohort or 20.5% in the patients with ASCVD shows that our lipid control among high-risk population was better than that in Europe, despite relatively low prescription rates of lipid-lowering drugs. The global DYSIS throughout 30 countries worldwide also demonstrated better performance on LDL-C target achievement in China compared with the Europe/Canada/Israel group (31.4% vs 24.7%). 36 However, it must be noted that the basal cholesterol levels in Chinese population are much lower than that in the Europeans.
In terms of the latest drug use, atorvastatin was the most frequently used statin, followed by rosuvastatin, fluvastatin, pravastatin, and simvastatin. The atorvastatin treatment group also achieved the highest rate of lipid-lowering goals, followed by rosuvastatin. The Bayesian network meta-analysis by Lu et al also found that atorvastatin was the most effective in blood-lipid level modification as well as in reducing the risk of CHD mortality and all-cause mortality. 37
Studies have shown that high-intensity statin therapy is more effective in reducing lipid and cardiovascular events. 6,38 However, high-intensity statin treatment had a slightly higher risk of rhabdomyolysis 39 and DM 40 as well as higher rates of toxicity. 6 Thus, the combination of statin and other lipid-lowering drugs has been extensively studied, from which they found that combination therapy is not only safer but also more effective. 41 -44 Studies have confirmed that proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors can be used as a new lipid-lowering drug when statin alone is ineffective for lipid lowering. 45,46 Therefore, more and more evidence show that the combination of statin and nonstatin drugs will be the key of lipid control. 47
Limitations
As the hospitals involved in this study are concentrated in Fuzhou, China, rather than nationwide sampling, the results cannot be generalized to the whole country. Secondly, the selected population is patients with LDL-C records in 2016. It cannot represent all the high-risk or extremely high-risk patients in the hospital, let alone all the population. Thirdly, guidelines for the prevention and treatment of adult hyperlipidemia in China in 2016 indicate, in addition to LDL-C numerically less than 1.8 mmol/L, also a ≥50% reduction from baseline LDL-C for patients with very high cardiovascular risk and a 30% reduction from baseline LDL-C for patients with high cardiovascular risk would meet the target achievement. As the cross-sectional study cannot measure these data, our study may underestimate the LDL-C attainment rate. Fourthly, drug use was based on doctors’ prescription, not on whether the patient actual drug-taking, so the actual drug use would be less than what we reported, and patients may be classified as exposed when they didn’t take the medicine. Finally, when comparing the frequency of different drug usage, we use the latest medication to estimate the total drug proportion. In fact, there may be drug conversion and combination, and our estimates may be biased.
Conclusion
Our study shows that there was suboptimal use of statins among patients with ASCVD and DM alone in Fuzhou, China, especially excessively small proportion use of high-intensity statins and combined medication with other nonstatins, although our study revealed that high-intensity statin and combination therapy were more effective on lipid lowering. Thus, guidelines should be well complied and more prescription of high-intensity statin or statin and nonstatin combination (including newer therapeutic options, such as PCSK9 inhibitors) should be advocated. Besides, atorvastatin should be used more widely, because it’s relatively cheaper due to the expiration of patent protection and more effective in reducing lipids and mortality.
Supplemental Material
Supplementary_file - Lipid-Lowering Therapy and Low-Density Lipoprotein Cholesterol (LDL-C) Goal Achievement in High-Cardiovascular-Risk Patients in Fuzhou, China
Supplementary_file for Lipid-Lowering Therapy and Low-Density Lipoprotein Cholesterol (LDL-C) Goal Achievement in High-Cardiovascular-Risk Patients in Fuzhou, China by Xing Wang, Yan He, Tao Wang, Chunming Li, Zihui Ma, Heng Zhang, Handong Ma and Hongxin Zhao in Journal of Cardiovascular Pharmacology and Therapeutics
Footnotes
Acknowledgment
The authors thank China Electronics Corporation (CEC) data for granting access to the National Health database.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.