
Abstract
Introduction
Central and Eastern Europe (CEE) has the second highest death rate attributable to cardiovascular diseases (CVD) in the world. 1 This high rate of CVD is associated with the complex social and political developments after the fall of the iron curtain combined with prevalent alcohol and tobacco use. 1 However, this does not seem to be true for the region as a whole. After plateauing in the 1980s and 1990s, cardiovascular (CV) death rates in those aged 30 to 69 years in the Czech Republic, Hungary, Poland, Romania, and Slovakia have declined to Western European levels, while CV death rates in those aged ≥70 years remain elevated. 2
Among the modifiable risk factors underlying local and regional mortality trends, smoking cessation and the lowering of serum cholesterol levels have been identified as those that could have an immediate effect on CV risk and potentially even reverse ischemic heart disease. 2 The European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS) recognize the importance of dyslipidemia management and provide periodically updated guidelines on the topic, the most recent iteration of which was in 2019. 3 These guidelines help clinicians to estimate the 10-year risk of fatal CVD based on individual CV risk factors, such as age, sex, smoking status, and total serum cholesterol levels. Based on the individual risk level, goals for serum low-density lipoprotein cholesterol (LDL-C) levels are also defined, that is individuals with high CV risk should aim at attaining an LDL-C level <1.8 mmol/L; those with very high CV risk, which includes all patients with established atherosclerotic CV disease (ASCVD), have an LDL-C goal of <1.4 mmol/L. 3 The pan-European DA VINCI study showed that across the participating CEE countries, only 24% of patients attained these 2019 ESC/EAS LDL-C goals, which was markedly less than goal attainment rates in countries from Northern (34%) or Western (40%) Europe. It should be noted that at the time of study conduct, clinicians were utilizing the less stringent 2016 ESC/EAS LDL-C goals, and that these goals were attained by only 44% of patients from participating CEE countries 4 ; additionally proprotein convertase subtilisin/kexin type 9 inhibitor (PCSK9i) were not available at the time.
There are two main factors that affect the attainment of LDL-C goals: (a) the serum LDL-C level at which treatment is initiated and (b) the intensity of lipid-lowering therapy (LLT) used.5,6 Both factors are highly regulated in clinical practice through reimbursement criteria, which commonly define LDL-C thresholds at which LLT can be initiated and intensified and regulate which products are reimbursed and how. The LDL-C threshold for PCSK9i reimbursement impacts the types of patients who have access to high-intensity combination therapy. Among the CEE countries included in the present report, PCSK9i reimbursement in Bulgaria is limited to those patients who have heterozygous familial hypercholesterolemia (HeFH) with a Dutch Lipid Clinic Network (DLCN) score ≥6 and highly elevated LDL-C, with (>2.6 mmol/L [≥2 events] or >3.6 mmol/L [1 event]) or without (>5 mmol/L) a prior CV event, who are refractory to statin treatment. In the Czech Republic, primary prevention is limited to patients with familial hypercholesterolemia (FH) and highly elevated LDL-C (>3.1 mmol/L), while secondary prevention is limited to patients with LDL-C >2.6 mmol/L. In Slovakia, reimbursement is limited to those patients who do not reach LDL-C goals using statins ± ezetimibe and have highly elevated LDL-C, the exact level being defined by the setting. In primary prevention, reimbursement is limited to patients with HeFH plus LDL-C >5 mmol/L after 6 months of statin plus 1 month of statin ± ezetimibe treatment. In secondary prevention, patients with LDL-C >4 mmol/L after 1 CV event, LDL-C >3.5 mmol/L after ≥2 events or those with HeFH and LDL-C >3.5 mmol/L after any number of events are eligible. 7
The international HEYMANS study aimed to describe the characteristics of patients receiving evolocumab in clinical practice in various European countries and to longitudinally observe lipid profiles, lipid management patterns, and LDL-C goal attainment. It was found that the LDL-C level at which evolocumab was initiated varied between the 12 participating European countries and was sometimes higher than the nationally defined LDL-C level for PCSK9i reimbursement. Additionally, differences in the proportions and types of patients who did not receive statin ± ezetimibe-based LLT prior to evolocumab initiation were noted. 7 Presented here are the data for the Bulgarian, the Czech Republic, and Slovakian cohorts of HEYMANS.
Methods
A full description of the HEYMANS study design and cohort is provided in the publications of the overall study cohort.7,8
Study Design and Participants
HEYMANS was a pan-European observational cohort study conducted in 12 European countries. Bulgaria and Slovakia started to enroll patients in July 2017, while the Czech Republic initiated enrollment in March 2019. In all three countries, the last patient visit occurred in the second quarter of 2021 (Supplemental Figure S1).
Eligible patients were adults who were prescribed evolocumab according to the local reimbursement criteria (Figure 1), who had received at least one evolocumab dose, and who had provided informed consent. Patients pretreated with a PCSK9i within 12 weeks prior to evolocumab initiation, either in routine clinical practice or as part of an interventional trial, were excluded.

PCSK9i reimbursement criteria and enrolled patient population, by country. ASCVD, atherosclerotic cardiovascular disease; CV, cardiovascular; DLCN, Dutch Lipid Clinic Network; FH, familial hypercholesterolemia; HeFH, heterozygous familial hypercholesterolemia; LDL-C, low-density lipoprotein cholesterol; PCSK9i, proprotein convertase subtilisin/kexin type 9 inhibitor. Reimbursement criteria adapted from Ray et al. 7
Retrospective patient data were collected from medical records from 6 months prior to the initiation of evolocumab. Prospective data collection was conducted via electronic case report forms (eCRF) for up to 30 months after evolocumab initiation, irrespective of the duration of evolocumab treatment. The core study observation period was for 12 months after evolocumab initiation; the period from month 13 to month 30 was added as an amendment of the original study protocol. Only patients still in the study at the time of approval of the protocol amendment were eligible for the extension period. Supplemental Figure S1 provides an overview of the core time points and patient flow in this study.
Outcome Measures
The primary outcome measure was the clinical characteristics of the patients receiving evolocumab, by country. Additional outcomes were to observe lipid profiles and lipid management patterns over time. LDL-C goal attainment was assessed for patients who had at least one post-baseline LDL-C value. CV risk was classified according to the 2019 ESC/EAS guidelines. 3
Evolocumab persistence, defined as the proportion of patients who continued to receive evolocumab and remained in the study at specified time points, was analyzed for two periods: 0 to 12 months and 12 to 30 months. The persistence analysis excluded patients who stopped the study before these time points but who were still receiving evolocumab. Patients were considered to have discontinued evolocumab if they permanently stopped therapy during the observation period.
No formal analysis of safety outcomes was planned; suspected treatment-emergent adverse drug reactions (ADRs) were summarized as reported and coded using Medical Dictionary for Regulatory Activities (MedDRA) version 24.0.
Statistical Analysis
Categorical data were provided as patient numbers and percentages with their 95% confidence intervals (CI), where appropriate. Continuous data were provided as means and standard deviations (SD) or medians and first and third quartile (Q1, Q3). Missing data were not imputed and the number of patients with missing data was displayed. Statistical analysis was conducted using SAS version 9.4 (SAS Institute, Cary, NC, USA).
Ethical Conduct
This study was conducted according to the Declaration of Helsinki and was registered in ClinicalTrials.gov (Identifier: NCT02770131). The study protocol and the protocol amendment were reviewed by an independent ethics committee in each participating country. All participants provided written informed consent.
Results
Patient Disposition
The CEE cohort included 333 patients, 88 from Bulgaria, 120 from the Czech Republic, and 125 from Slovakia. Of these, 325 completed the core period. Subsequently, 272 patients were eligible to enter and 200 completed the extension period.
Patient Characteristics
Across all the participating CEE countries, most patients had very high CV risk and were treated in the secondary prevention setting (Figure 1). In Bulgaria, the largest proportions of patients were those with established ASCVD and FH (67%, n = 59/88) and those with FH without ASCVD (19%, n = 17/88). In the Czech Republic, 41% of patients (n = 49/120) had ASCVD without FH, 33% (n = 40/120) had ASCVD and FH, and 21% of patients (n = 25/120) had FH without ASCVD. In Slovakia, most patients (70%, n = 88/125) had ASCVD without FH and 17% (n = 21/125) had ASCVD with FH. There were some imbalances between countries in the proportions of ever smokers (Bulgaria: 47%, n = 41/88; Czech Republic: 48%, n = 58/120; Slovakia: 23%, n = 29/125) and patients with hypertension (Bulgaria: 80%, n = 70/88; Czech Republic: 58%, n = 69/120; Slovakia: 81%, n = 101/125). Table 1 shows patient characteristics at baseline by country.
Patient Characteristics at Baseline.
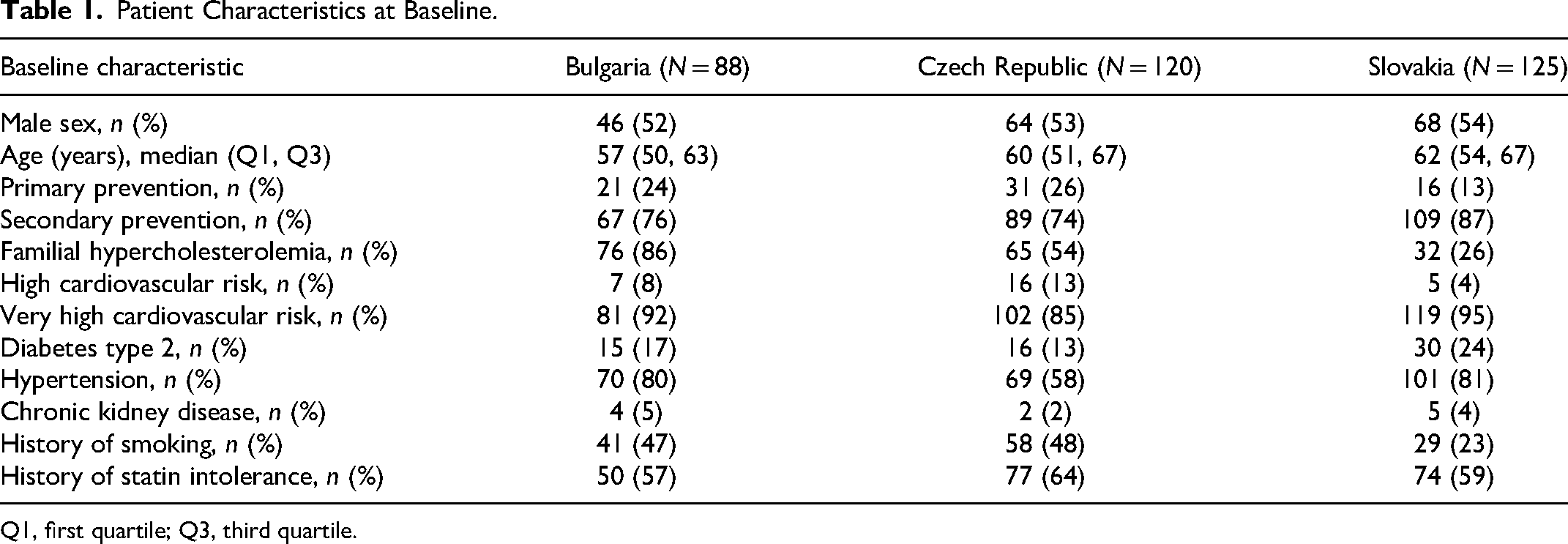
Q1, first quartile; Q3, third quartile.
Dyslipidemia Treatment Over Time
The percentage of patients not receiving LLT prior to evolocumab initiation differed between countries and was relatively low in Bulgaria (19%) and relatively high in the Czech Republic (67%) (Supplemental Figure S2A to S2C). In Bulgaria there appeared to be a trend that the number and types of background LLT (ie, statin, ezetimibe or both) decreased during the first months of evolocumab treatment but varied in the extension phase (Supplemental Figure S2A). In the Czech Republic, the proportion of patients with no background LLT decreased after the initiation of evolocumab, in parallel to an increase in the proportion of those receiving statin ± ezetimibe (Supplemental Figure S2B). In Slovakia, the proportion of patients without any background LLT slightly increased by month 6 after evolocumab initiation and remained stable thereafter (Supplemental Figure S2C).
Evolocumab Use
Across the three CEE countries, nearly all patients received evolocumab at a dose of 140 mg once every two weeks (98%, n = 86/88 in Bulgaria; 99%, n = 119/120 in the Czech Republic; 100%, n = 125/125 in Slovakia). Persistence with evolocumab at month 12 was high: 95% in Bulgaria, 89% in the Czech Republic, and 94% in Slovakia; persistence at month 30 was similar to that seen at month 12 (Figure 2).

Persistence with evolocumab at month 12 and month 30, by country. Persistence was defined as the percentage of patients receiving evolocumab among those with known evolocumab status at month 12 and at month 30. *Ns are the numbers of patients whose evolocumab status was known at month 12 and month 30, respectively. The number of patients entering the extension phase, that is, month 13 to month 30, was 58 in Bulgaria, 117 in the Czech Republic, and 97 in Slovakia.
LDL-C Levels Over Time
At initiation of evolocumab, LDL-C levels were markedly elevated in all three countries, with a median (Q1, Q3) LDL-C of 5.2 (4.0, 6.6) mmol/L in Bulgaria, 4.5 (3.8, 5.8) mmol/L in the Czech Republic, and 4.7 (4.0, 5.6) mmol/L in Slovakia. Within the first 3 months of evolocumab treatment, LDL-C levels were reduced by a median (Q1, Q3) of 61% (44%, 72%) in Bulgaria, 64% (45%, 74%) in the Czech Republic, and 53% (36%, 65%) in Slovakia. LDL-C levels remained low throughout the remaining period of observation (Figure 3).

LDL-C levels over time, by country. LDL-C, low-density lipoprotein cholesterol; Q1, first quartile; Q3, third quartile. *In case of more than one indicated LDL-C levels, these apply to one CV event or more than one CV event or HeFH in secondary prevention (one or more than one event).
Attainment of LDL-C Goals
The 2019 ESC/EAS guideline-recommended risk-based LDL-C goals of <1.8 mmol/L for high-risk and <1.4 mmol/L for very high-risk patients were attained by 46% of patients in Bulgaria, 59% in the Czech Republic, and 43% of patients in Slovakia (Figure 4A). There was a marked difference in goal attainment between patients receiving and not receiving a statin ± ezetimibe-based background therapy, whereby patients receiving combination therapy had a higher goal attainment rate (Bulgaria: 55%, Czech Republic: 71%, Slovakia: 51%) than those receiving evolocumab alone (Bulgaria: 19%, Czech Republic: 49%, Slovakia: 34%) (Figure 4A). Risk-based goal attainment by disease setting differed by country (Figure 4B).

Attainment of risk-based LDL-C goals. A. Attainment of risk-based LDL-C goal by country. B. Attainment of risk-based LDL-C goal by disease setting. ASCVD, atherosclerotic cardiovascular disease; FH, familial hypercholesterolemia; LDL-C, low-density lipoprotein cholesterol; LLT, lipid-lowering therapy, ie statin ± ezetimibe. N = Patients with non-missing values. Goal attainment was defined as attaining an LDL-C level of <1.8 mmol/L for patients with high cardiovascular risk and <1.4 mmol/L for patients with very high cardiovascular risk at least once during the observation period. In the Bulgarian cohort, 8% (n = 7) of patients had high and 92% (n = 81) of patients had very high cardiovascular risk. In the Czech cohort, 13% (n = 16) of patients had high and 85% (n = 102) of patients had very high cardiovascular risk. In the Slovak cohort, 4% (n = 5) of patients had high and 95% (n = 119) of patients had very high cardiovascular risk.
Summary of Safety Events
In Bulgaria, two patients (2%) reported ADRs; no serious ADR occurred. In the Czech Republic, 4 patients (3%) reported ADRs and 3 patients (3%) reported serious ADRs. All 3 patients with serious ADRs discontinued evolocumab. In Slovakia, 3 patients (2%) reported ADRs; no serious ADRs occurred. Supplemental Table S1 provides a summary of ADRs.
Impact of COVID-19
In Bulgaria, 180 LDL-C assessments occurred before 29 February 2020, that is, prior to the coronavirus disease 2019 (COVID-19) pandemic, and 34 assessments occurred between 1 March 2020 and the end of observation, that is, during the COVID-19 period. The number of post-baseline LDL-C measurements per patient-year in the pre-COVID-19 period was 1.4 and during the COVID-19 pandemic it fell to 0.75, representing a halving of the frequency of measurements. In the Czech Republic, 362 LDL-C measurements occurred prior to the COVID-19 pandemic and 279 occurred during the pandemic; the number of LDL-C measurements per patient-year was 2.6 pre-COVID-19 and 2.3 during the COVID-19 pandemic. In Slovakia, 553 LDL-C measurements were conducted before the pandemic and 75 were conducted in the COVID-19 period; the number of LDL-C measurements per patient-year were 2.4 and 1.9, respectively.
Discussion
The HEYMANS CEE cohort reinforced findings from DA VINCI CEE cohort, 4 which showed insufficient LDL-C control in the real-world clinical practice due to underutilization and/or lack of availability of more potent LLTs. In the HEYMANS CEE cohort, the LDL-C level at which evolocumab is initiated, is higher than recommended by guidelines, which suggests that the treatment focus is on patients at extremely high CV risk, neglecting a large proportion of patients with very high or high CV risk. Unless there is a re-evaluation of current barriers to availability of basic and injectable therapies, CV event rates will remain high in a high-risk region of Europe.3,9
The characteristics of the patients receiving evolocumab, as well as the treatment patterns observed in the present study, reflect the local reimbursement criteria for PCSK9i. Outcomes during PCSK9i treatment have been shown to be strongly impacted by a combination of several factors: the LDL-C level at initiation of PCSK9i treatment, the disease characteristics of the patients being treated with PCSK9i, the use (or not) of statin ± ezetimibe-based background LLT, along with other confounding factors that are difficult to discern in smaller patient cohorts.7,8
In the present study, the median (Q1, Q3) LDL-C level at which evolocumab was initiated was highest in Bulgaria (5.2 [4.0, 6.6] mmol/L), and was 4.5 (3.8, 5.8) mmol/L in the Czech Republic and 4.7 (4.0, 5.6) mmol/L in Slovakia. Patients in Bulgaria also achieved the largest absolute LDL-C reduction of these three countries (median [Q1, Q3] reduction of −3.0 [−4.1, −2.2] mmol/L vs −2.8 [−3.5, −2.0] mmol/L in the Czech Republic and −2.5 [−3.0, −1.6] mmol/L in Slovakia). Interestingly, in all three countries patients were started on evolocumab treatment at LDL-C levels higher than those required by the local reimbursement criteria, a trend which was observed throughout the countries participating in HEYMANS. 7 The main reason for evolocumab treatment initiation at LDL-C levels higher than recommended in the guidelines is limited resources of the local healthcare systems, more complex and slower process of patients’ individual reimbursement approval; it does not necessarily reflect non-compliance to the guidelines among the local cardiology community. Clinical practice in the corresponding countries is not adequately suited to allow reasonable access to intensive lipid-lowering treatment for very high-risk patients.
When looking at the disease characteristics of the patients with access to PCSK9i in the present study, most of those from Bulgaria (86%) had FH and had a median baseline LDL-C level of 5.2 mmol/L; ASCVD was already established in most of these patients. Due to a lack of screening and a high reimbursement LDL-C threshold for PCSK9i use in primary prevention, FH thus appears to be treated too late. In the Czech Republic, PCSK9i are reimbursed in primary prevention for patients with FH and elevated LDL-C, and in secondary prevention for all patients with elevated LDL-C, hence a mixed population was enrolled with 54% of patients having FH with or without established ASCVD and 41% having established ASCVD without FH. In Slovakia, where PCSK9i are reimbursed in patients with HeFH and elevated LDL-C and also in dyslipidemic, statin/ezetimibe-refractory patients (as per reimbursement criteria definition) after one or more CV events, most patients had ASCVD without FH (70%). In the overall HEYMANS dataset, 7 which comprised 1951 patients, some tendencies with regards to the treatment patterns in patients with different disease backgrounds could be observed. Patients with ASCVD but without FH (median 3.7 mmol/L) tended to start evolocumab therapy at a similar LDL-C level than those with ASCVD and FH (median 4.0 mmol/L). Both groups showed a similar percentage decrease in LDL-C within the first 3 months of treatment with evolocumab (∼60% reduction), which was subsequently maintained. Patients with FH but without ASCVD (median 5.2 mmol/L) and patients with neither FH nor ASCVD (median 5.2 mmol/L) tended to have evolocumab treatment initiated at a higher LDL-C level; these patients had an approximate 50% LDL-C reduction within the first 3 months of treatment, which was also maintained over time. 7
Both the HEYMANS7,8 and DA VINCI4,10–14 studies showed a consistent pattern of improved LDL-C goal attainment in patients receiving PCKS9i in combination with statins ± ezetimibe compared with those receiving less intensive treatment regimens. In the present CEE cohort, risk-based LDL-C goal attainment was also higher in patients receiving evolocumab combination therapy (Bulgaria: 55%, Czech Republic: 71%, Slovakia: 51%) compared to those with evolocumab alone (Bulgaria: 19%, Czech Republic: 49%, Slovakia: 34%). Bulgaria had the highest proportion of patients receiving statin ± ezetimibe-based LLT at evolocumab initiation (81%) and throughout the observation period (between 62% and 84%), while in the Czech Republic and Slovakia, only between 38% and 49% of patients received background LLT at any time after evolocumab initiation. However, the precise mix of LLT used differed between countries. Although Bulgaria had the highest proportion of patients receiving background LLT, evolocumab was mostly combined with only statin without ezetimibe (36% [month 3, not shown in the figure] to 49% post-baseline). In the Czech Republic and Slovakia, the use of background LLT was generally lower, but when used, approximately one-fifth to one-quarter of patients received statin with ezetimibe and approximately 10% received ezetimibe alone. In all countries slightly more patients used background LLTs in the extension phase, compared to the core phase. This suggests a higher discontinuation rate at month 12 among patients not using background LLTs compared to those using background LLTs, although it needs to be noted that the extension phase was only available to those patients still on study at the time of the approval of the protocol amendment. Persistence with evolocumab therapy was very high with 95% in Bulgaria, 89% in the Czech Republic, and 94% in Slovakia at month 12, and 94%, 85%, and 90%, respectively, at month 30. In the overall HEYMANS cohort, persistence was 93% at month 12% and 92% at month 30. 8
Taken together, LDL-C at evolocumab initiation, underlying disease subtype, ie ASCVD and FH alone or in combination, as well as overall treatment intensity varied among the participating countries, and LDL-C results were different. The following patterns were observed: In Bulgaria, the low rate of LDL-C goal attainment (46%), despite a high proportion of patients receiving combination evolocumab plus statin ± ezetimibe therapy (81%) might be due to the very high LDL-C levels at evolocumab initiation combined with the fact that only patients with FH can get PCSK9i treatment reimbursed in Bulgaria. The highest rate of LDL-C goal attainment among these three CEE countries was observed in the Czech Republic (59%), although this country also had the lowest use of background LLT. The Czech Republic has the broadest reimbursement criteria for PCSK9i of these three countries. In line with this, patients from the Czech Republic were mostly initiated at an LDL-C level lower than in the other CEE countries and had a variety of different CVD profiles. The Czech Republic had the highest proportion of high-risk patients for which the LDL-C goal is more easily attainable than for very high-risk patients. The lowest rate of LDL-C goal attainment among these three CEE countries was observed in Slovakia (43%). The Slovakian population included mostly secondary prevention patients without FH who were initiated on evolocumab treatment at an LDL-C level markedly above the threshold recommended by both the 2019 ESC/EAS guidelines and local reimbursement criteria. Only approximately 40% to 50% of Slovakian patients received combination therapy. Slovakia also had the highest proportion of patients with diabetes (24%; Bulgaria: 17%, Czech Republic: 13%). Such patients are known to have poor adherence to LLT15–18 and LDL-C goal attainment is low even in diabetic patients who are adherent to LLT. 19
Importantly, however, in the HEYMANS CEE cohort, LDL-C goal attainment rates during evolocumab therapy were substantially higher than those seen in the DA VINCI study, 4 which assessed a CEE cohort that did not yet have access to PCSK9i. In the Czech Republic cohorts from the DA VINCI and HEYMANS studies, respectively, 24% versus 59% of patients attained the 2019 ESC/EAS risk-based LDL-C goals. In the Slovakian cohorts from these studies, 18% versus 43% of patients, respectively, attained these LDL-C goals. Bulgaria did not participate in the DA VINCI study.
Especially in Bulgaria and the Czech Republic a considerable proportion of patients in the present cohort had FH, mostly with already established ASCVD. There are initiatives calling for FH screening to improve the early identification of individuals at risk.20,21 All three countries participate in Screen Pro FH (http://screenprofh.com/), 22 which aims to develop a network of centers of excellence for patients with FH in the region of Central Eastern and Southern Europe and to harmonize and unify diagnostic and therapeutic approaches in participating countries. According to data from Screen Pro FH, patients frequently remain undiagnosed with a diagnostic rate among Screen Pro FH participants of 0.1% to 31.6%. 23 In Bulgaria, an institution-based pilot cascade screening program is ongoing. 24 In the Czech Republic, an opportunistic testing and cascade screening program based on the Make Early Diagnoses to Prevent Early Deaths (MedPed) project has been set up in 1998, and a pilot universal screening program in neonates exists. 24 In Slovakia, a nationwide universal screening in children aged 11 and 17 years exists. 24 Slovakia has also set up a MedPed initiative in 1998, similar to the Czech Republic.
Interestingly, in the present study there was a substantial difference between countries in the number of LDL-C measurements taken in routine clinical practice. The number of LDL-C measurements by patient-year in the Czech Republic and Slovakia was higher than for patients in Bulgaria, with measurements being taken approximately once every 5 months versus once every 9 months, respectively, in the pre-COVID-19 period. During the COVID-19 pandemic, the number of LDL-C measurements taken was reduced in all countries, but this change in measurement frequency affected more patients in the Czech Republic because study enrollment started later there. Nonetheless, the Czech Republic was the most successful in maintaining their frequency of measurements among the three CEE countries included in HEYMANS. It is important to note that persistence with evolocumab was very high in the present study, even throughout the extension phase, despite the challenges of the pandemic.
The present study has some limitations. Due to the circumstances of the protocol amendment, the number of Bulgarian and Slovakian patients participating in the extension phase was lower than the number of patients that were initially enrolled from these countries; the Czech Republic only started to enroll patients after the protocol amendment was approved. The COVID-19 pandemic, which started in February 2020 impacted the scheduling of routine clinic visits and so the number of available LDL-C measurements was lower during the pandemic period (01 March 2020 to end of study), compared with the pre-pandemic period (first evolocumab administration to 29 February 2020). Persistence with evolocumab may have been overestimated. In CEE, 108 patients were receiving evolocumab for >6 months before enrollment. Long-term users may have been more likely to continue with their treatment than those who initiated treatment more recently. In addition, centers participating in the HEYMANS study included specialized lipid centers, where healthcare professionals may be likely to encourage persistence with treatment. Nevertheless, our results are similar to those of previous studies on evolocumab persistence.25,26
Conclusions
In the CEE cohort of the HEYMANS study, evolocumab was used mainly in very high-risk patients and treatment was initiated at LDL-C levels >3× higher than 2019 ESC/EAS guideline-recommended thresholds for PCSK9i. Although LDL-C levels were reduced by >50% within 3 months of evolocumab initiation, lowering the LDL-C reimbursement thresholds for PCSK9i initiation and educating clinicians on the importance of lipid management would allow more patients to receive combination therapy, which could improve LDL-C goal attainment and thus clinical outcomes. Early and adequate lipid management with high-intensity combination therapy should be made available to a broad population of individuals in primary and secondary prevention in order to reduce the burden of CVD to society.
Supplemental Material
sj-docx-1-cpt-10.1177_10742484231172847 - Supplemental material for Evolocumab is Initiated in Central and Eastern Europe at Much Higher LDL-C Levels Than Recommended in Guidelines: Results from the Observational HEYMANS Study
Supplemental material, sj-docx-1-cpt-10.1177_10742484231172847 for Evolocumab is Initiated in Central and Eastern Europe at Much Higher LDL-C Levels Than Recommended in Guidelines: Results from the Observational HEYMANS Study by Vladimír Blaha, Roman Margoczy, Ivo Petrov, Arman Postadzhiyan, Katarína Rašlová, Hana Rosolová, Ian Bridges, Nafeesa N. Dhalwani, Marie Zachlederova and Kausik K. Ray in Journal of Cardiovascular Pharmacology and Therapeutics
Footnotes
Acknowledgements
Margit Hemetsberger of Hemetsberger medical services, Vienna, Austria, provided medical writing support and third-party submission with the listed authors’ authorization, funded by Amgen GmbH.
Author Contributions
NND designed the study. KKR served on the study's advisory panel. VB, RM, IP, AP, and HR were study investigators for the Central and Eastern European study cohort and acquired the data. IB conducted statistical analysis of the data. All authors substantially contributed to the interpretation of the study results. All authors were involved in drafting of the manuscript, provided critical revisions for important intellectual content, approved the final version submitted for publication, and agreed to be accountable for all aspects of the work.
Consent to Participate
Written informed consent was obtained from all individual participants included in the study.
Consent for Publication
Not applicable.
Data Availability
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: VB received personal fees from Amgen and Sanofi/Regeneron. RM has received speaker fees from Amgen and Sanofi/Regeneron. IP received research grants from Novartis, Amgen and Boehringer, consulting fees from Amgen, Actavis, Novartis, Medtronic, MSD, Boehringer and Pfizer and speaker honoraria from Amgen, Contego Medical and Medtronic. AP declares grants and personal fees from Amgen, AstraZeneca, Bayer, Gedeon Richter, Novartis, and Teva. KR received lecture fees from Amgen, Novartis, Sanofi, Novo Nordisk, Mylan, Boehringer Ingelheim; HR received lecture fees from Amgen, Novartis and Sanofi; KKR reports grants and personal fees from Abbott, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Cargene, Daiichi Sankyo, Esperion, Kowa, Lilly, NewAmsterdam Pharma, Novartis, Pfizer, Sanofi/Regeneron, Scribe Therapeutics and Silence Therapeutics; IB is an employee of Amgen Ltd and stockholder of Amgen; MZ is an employee of Amgen s.r.o. and stockholder of Amgen; NND is an employee of Amgen Inc. and stockholder of Amgen.
Ethical Approval
This study was conducted according to the Declaration of Helsinki and was registered in ClinicalTrials.gov (Identifier: NCT02770131). The study protocol and the protocol amendment were reviewed by an independent ethics committee in each participating country.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Amgen (Europe) GmbH.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.