
Abstract
Background:
Anticoagulation therapy is recommended for stroke prevention in high-risk patients with atrial fibrillation (AF). This study aimed to estimate the time to switch from warfarin to a direct oral anticoagulant (DOAC) and identify the factors associated with it.
Methods:
By using claims data, we studied 7111 warfarin-using patients with nonvalvular AF who were aged ≥65 years. The Kaplan-Meier analysis was performed to estimate the time to switch from warfarin to a DOAC, and Cox proportional hazard regression analysis was used to estimate the influencing factors.
Results:
Approximately one-third of the patients (2403, 33.8%) switched from warfarin to a DOAC during the study period. Female sex, aged between 75 and 79 years, having a Medical Aid or Patriots and Veterans Insurance, hypertension, and history of prior stroke, and transient ischemic attack or thromboembolism (prior stroke/TIA/TE) were associated with a significantly shorter time to switch. The odds of switching to a DOAC were increased by approximately 1.2-fold in the women and 1.4-fold in the patients with prior stroke/TIA/TE.
Conclusions:
Approximately one-third of the warfarin-using patients switched from warfarin to a DOAC within 6 months after the change in the DOAC reimbursement criteria. In the Cox proportional hazard regression analysis, the factors that affected anticoagulant switching from warfarin to a DOAC were female sex and history of prior stroke/TIA/TE.
Introduction
Atrial fibrillation (AF), the most common arrhythmia, is characterized by a grossly disrupted atrial electrical activity that causes an abnormal heart rate and rhythm. 1 The prevalence of AF increases rapidly with age, by <0.5% in young adults, 1% to 5% in patients aged 40 to 70 years, and ≥10% in patients aged >70 years. 1 -4 In Korea, the prevalence of AF in the population aged ≥65 years was approximately 3% in the study that used claims data from 2011 to 2014 5 and has been gradually increasing like the global trend. 5 -7
Atrial fibrillation is independently associated with an increased risk of mortality 8,9 and augments the risk of stroke by up to 5 times. 10 -12 Stroke due to AF is caused by an embolism originating from the atria, and its occurrence increases as the duration of AF increases. 11
Stroke risk can be largely mitigated by anticoagulant therapy. Adjusted-dose warfarin use reduces the risk of stroke by approximately 60%. 13 Therefore, anticoagulant therapy is recommended for patients with one or more stroke-risk factors without a high risk of bleeding. 14 -19
To assess stroke risk, the CHA2DS2-VASc (congestive heart failure, hypertension, age of ≥75 years [doubled], diabetes mellitus, prior stroke or transient ischemic attack [doubled], vascular disease, age of 65 to 74 years, and sex) score has been used. 14 -16,18 -21 Various bleeding risk assessment tools have been proposed, such as HAS-BLED (hypertension, abnormal renal and liver function, stroke, bleeding, labile international normalized ratio [INR], elderly, drugs or alcohol), ATRIA (anticoagulation and risk factors in AF), HEMORR2HAGES (history of bleeding, hepatic or renal disease, alcohol abuse, malignancy, older age, reduced platelet count or function, hypertension, anemia, genetic predisposition, excessive fall risk, and stroke), and ORBIT (outcomes registry for better informed treatment of AF). 22 -24
Anticoagulant therapy had been limited to warfarin until direct oral anticoagulants (DOACs) became available in the past decade. 25 The efficacy and safety profiles of DOACs are comparable with, if not better than, those of warfarin. 26 -29 Moreover, according to Asian subanalyses and a meta-analysis of the pivotal DOAC randomized controlled trials, Asian patients have superior stroke reduction and major bleeding reduction as compared with non-Asian patients. 30
For several years, DOACs were the second-line thromboprophylactic agents to prevent stroke in high-risk patients with nonvalvular AF (NVAF) in Korea. According to the previous reimbursement criteria, DOACs were allowed in patients verified as having a hypersensitivity or contraindication to warfarin or failed control of INR with warfarin. On July 1, 2015, the benefit criteria were changed to allow DOACs as the first-line drug for stroke prevention in patients with NVAF. Although several studies have examined increased use of DOACs and sociodemographic factors that influence the anticoagulant selection, 31 -36 few studies have been conducted on the anticoagulant switch to a DOAC in patients taking warfarin in a real-world setting.
Switching from warfarin to a DOAC may suggest that some patients had a high level of dissatisfaction with warfarin therapy and high demand for alternative anticoagulant therapy in usual clinical practice. The aim of this study was to compare the time and patterns of switching between warfarin and a DOAC in patients with NVAF and to identify potential confounding factors associated with the switching.
Methods
Study Data
Aged population sample data of approximately 1 million individuals aged ≥65 years in Korea that were collected by the Health Insurance Review and Assessment Service in 2015 (HIRA-APS-2015-0052) were used. Korean Classification of Diseases, Sixth Revision, codes (KCD-6 codes, the Korean version of International Classification of Diseases, Tenth Revision [ICD-10]) were used to identify patients with a specific disease or condition. The ingredient code was used to identify 3 DOACs (apixaban, dabigatran, and rivaroxaban) and warfarin. Edoxaban was not included in the present study because it was not licensed in Korea until 2016 (Appendix A).
Three types of health insurance programs are available in Korea. The National Health Insurance (NHI) covers approximately 97% of the population and imposes a duty on income, while Medical Aid (MedAid) is a guaranteed system for low-income people and the Patriots and Veterans Insurance (PVI) is for national veterans. 37 All types of health insurance programs have the same benefit criteria, but patients’ copayments on prescription drugs range from 0% to 30%. 37
Study Subjects
Patients with AF or atrial flutter as the main diagnosis were identified. Then, patients who received warfarin as outpatients between January 1, 2015, and June 30, 2015, and remained medicated on July 1, 2015, the index date, were included. Patients with valvular heart disease were excluded. While the definition of valvular heart disease slightly differs between guidelines, it generally means valve replacement or rheumatic valve disease. In this study, we identified patients with valve replacement or valve disease on the basis of the KCD-6 codes (Appendix A). To estimate the patients’ stroke and bleeding risks, we used the CHA2DS2-VASc and ATRIA bleeding scores, respectively. Among the various bleeding assessment tools, we selected the ATRIA bleeding score.
Statistical Analyses
The patients’ baseline characteristics are presented using frequency analysis for categorical variables and mean ± standard deviation for continuous variables. The time to switch from warfarin to a DOAC was calculated as time (in days) from July 1, 2015, to the first DOAC prescription. Patients who continued warfarin or were not prescribed any oral anticoagulants since the index date were censored when the follow-up ended (December 31, 2015). A Kaplan-Meier curve analysis was used to compute the time to switch, while a Cox proportional hazard regression analysis was used to estimate the influencing factors. SPSS 23 (IBM Corporation, New York) was used for the statistical analysis, and the significance level was set at P < .05.
Results
Characteristics of the Study Subjects
A total of 7111 patients were finally included in the analysis (Figure 1). Their mean age was 75.0 ± 5.9 years. Male patients dominated the population (55.8% vs 44.2%). The mean CHA2DS2-VASc score was 4.5 ± 1.5, while the mean ATRIA bleeding score was 2.3 ± 1.6. The characteristics of the study subjects are presented in Table 1.
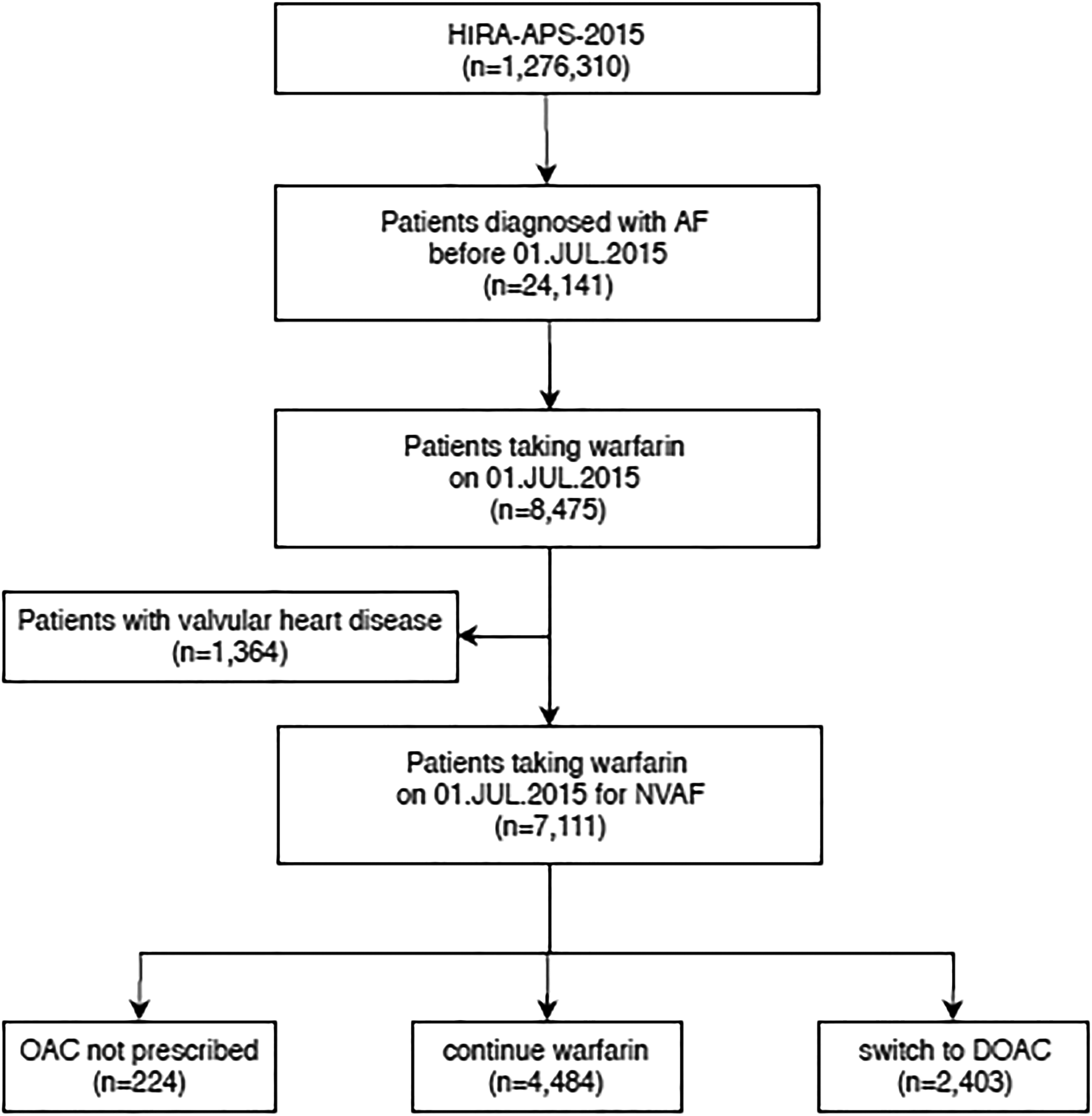
Case extraction diagram. AF indicates atrial fibrillation; DOAC, direct oral anticoagulant; HIRA-APS, Health Insurance Review & Assessment Service-Aged Patient Sample; NVAF, non-valvular atrial fibrillation; OAC, oral anticoagulant.
Characteristics of the Study Subjects.

Abbreviations: ATRIA, anticoagulation and risk factors in atrial fibrillation; CHA2DS2-VASc, congestive heart failure, hypertension, age ≥75 years, diabetes mellitus, stroke (or transient ischemic attack), vascular disease, age 65-74 years, and sex; CHF, congestive heart failure; DOAC, direct oral anticoagulant; MedAid, Medical Aid; NHI, National Health Insurance; PVI, Patriots & Veterans Insurance; SD, standard deviation; TE, thromboembolism; TIA, transient ischemic attack.
Descriptive Survival Analysis
Of the 7111 study subjects, 2403 (33.8%) were switched from warfarin to a DOAC during the study period; the other 4708 patients (66.2%) were censored. The most selected DOAC was rivaroxaban (976, 40.6%), followed by dabigatran (853, 35.5%) and then apixaban (574, 23.9%). The estimated event rate was calculated as 2.37 per 1000 person-days (Table 2). Figure 2 shows the differences among the survivor curves of age group, sex, insurance type, hypertension status, and history of prior stroke/transient ischemic attack or thromboembolism (TIA/TE).
Switching Rate (95% Confidence Interval) from Warfarin to a DOAC.

Abbreviations: CHF, congestive heart failure; CI, confidence interval; DOAC, direct oral anticoagulant; MedAid, Medical Aid; NHI, National Health Insurance; PVI, Patriots & Veterans Insurance; SE, standard error; TE, thromboembolism; TIA, transient ischemic attack.

Kaplan-Meier curves of cumulative probability of switch to DOAC. (A) Age group, (B) sex, (C) insurance type, (D) hypertension, (E) prior stroke or TIA or TE. TIA indicates transient ischemic attack; TE, thromboembolism.
Results of the Cox Proportional Hazards Model
Table 3 presents the results of the Cox proportional hazard regression analysis that examined the association between patients’ characteristics and the time to switch from warfarin to a DOAC. The hazard ratio (HR) of the female patients for the switch to a DOAC was higher than that of the male patients (HR: 1.20; 95% confidence interval [CI] 1.11-1.30, P < .001). The HR of prior stroke/TIA/TE was 1.36 (95% CI: 1.25-1.48, P < .001).
Cox Proportional Hazard Regression Analysis of Baseline Variables Associated With Switch to a DOAC.

Abbreviations: CHF, congestive heart failure; CI, confidence interval; DOAC, direct oral anticoagulant; MedAid, Medical Aid; NHI, National Health Insurance; PVI, Patriots & Veterans Insurance; TE, thromboembolism; TIA, transient ischemic attack.
Discussion
A retrospective cohort analysis was conducted to evaluate anticoagulant switch patterns among patients who were already receiving warfarin therapy. The stroke and bleeding risks of the study population were estimated to be high and low, respectively. Of the study subjects, 33.8% (2403) switched from warfarin to a DOAC during the study period.
We found significant differences in the tendency to switch from warfarin to a DOAC by age group, sex, insurance type, hypertension status, and history of prior stroke/TIA/TE. According to the survival analysis, apparent differences in the time at which the curves begin to separate were observed (Figure 2). While the separation appears immediate for the history of prior stroke/TIA/TE, the separation seems to occur after around 40 days for sex and hypertension.
The Cox proportional hazards regression analysis result indicated that female sex and history of prior stroke/TIA/TE were significant influencing factors of anticoagulant switching behavior from warfarin to a DOAC. Among those with NVAF, women were already known to use less warfarin than men. 38 -40 Underestimation of female stroke risk and fear of bleeding are the most common reasons for warfarin underuse in this population. 38,41 After the introduction of DOACs, sex-based differences in thromboprophylactic treatment diminished or were even eliminated. Loikas et al reported that while fewer women used oral anticoagulants in 2011, this trend had disappeared by 2015. 42
In a prospective observational cohort study of sex-related differences in the management of NVAF, DOAC use was more prevalent in women than in men, although insufficient DOAC dosing was more common in women than in men. 35
Our study results also showed that prior stroke/TIA/TE was a significant factor in drug conversion, parallel to previous findings. In a paper that compared sociodemographic factors of continuing warfarin and transitioning to a DOAC, a new thromboembolic event while on warfarin was the strongest predictor of DOAC switching status. 33 Studies that compared DOACs with warfarin in patients in Asian countries showed that DOACs, except rivaroxaban, significantly reduced the risk of major bleeding as compared with warfarin. 43 -46 Patients in Asia reportedly have a higher incidence of intracranial hemorrhage when taking warfarin than patients in other regions, 43,45 while the incidence of intracranial hemorrhage was higher in patients with previous stroke. 47 -50 Therefore, the result of drug modification with a DOAC in the presence of prior stroke/TIA/TE is considered valid. Seiffge et al compared the antithrombotic effects of DOACs with those of warfarin in patients with AF and a recent cerebral ischemia and concluded that DOAC treatment was associated with a reduced risk of poor clinical outcomes as compared with warfarin, which is mainly attributed to lower risks of intracranial hemorrhage. 51 According to the recommendation of the Asia Pacific Heart Rhythm Society guidelines for the prevention of stroke in patients with AF in 2017, DOACs are preferred to warfarin for patients with a history of ischemic stroke or TIA. 30
It is reasonable to continue warfarin instead of anticoagulant switching for some patients with NVAF. Ikeda et al conducted a survey to investigate reasons for continuing warfarin therapy in Japanese patients with AF and reported that the reasons for continuing warfarin therapy were the high price of DOACs (47.2%) and long-term positive experience with warfarin (31.7%). 52 A prospective cohort study identified white race, married status, and higher median household income as sociodemographic factors associated with a patient’s likelihood of switching to a DOAC rather than remaining on warfarin therapy. 33
Female sex and prior stroke/TIA/TE history are risk factors of stroke and major bleeding. This study showed that both risk factors prompted the patients who were receiving warfarin to switch to a DOAC with similar efficacy but a lower bleeding risk than warfarin when the reimbursement criteria were changed.
This study has several limitations. First, we used claims data collected for reimbursement purposes, not for clinical or research purposes; therefore, the diagnosis may be inaccurate and likely subjected to upcoding by providers looking for higher reimbursement rates. 53 Second, these claims data did not include clinical data such as laboratory test results or physical assessment findings. For example, we were not able to calculate the time in the therapeutic range (an INR between 2.0 and 3.0) to assess the quality of warfarin therapy without INR data. Third, socioeconomic characteristics such as income, education, and health behaviors were not available.
Even with the above mentioned limitations, our study filled a gap in the literature by demonstrating anticoagulant switching patterns from warfarin to a DOAC after the change in the reimbursement criteria and the associated patient characteristics by using real-world data.
Conclusion
This study found that approximately one-third of patients changed oral anticoagulant use from warfarin to a DOAC since the change in the reimbursement criteria. The factors that influenced the anticoagulant switch were female sex and prior stroke/TIA/TE.
Footnotes
Appendix A
Acknowledgment
The authors used Aged Population Sample data from 2015 that were collected by the Health Insurance Review and Assessment Service (HIRA-APS-2015-0052) for this study, but the results have no connection with the Ministry of Health and Welfare or HIRA.
Author Contributions
Susin Park contributed to the design, analysis, and interpretation; drafted the manuscript, critically revised the manuscript; and gave final approval, Nam Kyung Je contributed to conception and design, acquisition, and interpretation; drafted the manuscript; critically revised the manuscript; and gave final approval. Both authors agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.