
Abstract
Cardiovascular disease (CVD), principally myocardial infarction (MI) and stroke, is the leading clinical and public health problem in the United States and is rapidly becoming so worldwide. Their primary prevention is promising, in theory, but difficult to achieve in practice. The principal modalities that have demonstrated efficacy include therapeutic lifestyle changes (TLCs) and adjunctive drug therapies under the guidance of the health-care provider and tailored to the individual patient. The prevention and treatment of the pandemic of overweight and obesity and lack of regular physical activity, both of which are alarmingly common in the United States, prevention and treatment of hypertension, avoidance and cessation of cigarette smoking, adoption and maintenance of a healthy diet, and avoidance of heavy alcohol consumption all have proven benefits in decreasing the risks of a first MI and stroke as well as other clinical manifestations of CVD. Although adoption of TLCs would avoid the need for adjunctive drug therapies in many primary prevention subjects, this strategy is difficult to achieve or maintain for most and may be insufficient for many, especially those at high risk with metabolic syndrome. The criteria for metabolic syndrome, affecting over 40% of the adult population older than 40 in the United States, include overweight or obesity, dyslipidemia, hypertension, and insulin resistance, a precursor of diabetes. The adjunctive therapies of proven benefit in the primary prevention of MI and stroke include statins, blood pressure medications, aspirin, and drugs to treat insulin resistance and hyperglycemia. Fortunately, even for patients who prefer prescription of pills to proscription of harmful lifestyles, these drug therapies still have net benefits. The adoption and maintenance of TLCs and adjunctive drug therapies into clinical practice will reduce both the incidence of and mortality from a first MI and stroke as well as other major clinical manifestations of CVD.
Introduction
Cardiovascular disease (CVD) accounts for over 800 000 deaths in the United States each year, and more than 17 million deaths worldwide. In the United States, CVD, which includes, principally, myocardial infarction (MI) and stroke, accounts for over 40% of total deaths. In the United States, CVD is projected to remain the single leading cause of mortality and is becoming so worldwide. In the United States, MI accounts for about 25% and stroke constitutes 16.5% of all deaths from CVD. Stroke alone ranks fifth in all-cause mortality, 1 killing nearly 133 000 people annually in the United States and over 11% of the population worldwide. 2 The vast majority of strokes in the United States are ischemic, and this trend is rapidly becoming globalized. The estimated annual cost of MI in the United States is approximately $11.5 billion and that of stroke approximately $18 billion. 1 The larger cost of stroke is due, at least in part, to the fact that it is one of the most common causes of disability. Despite these sobering statistics, in the United States and most developed countries, there have been consistent declines in mortality from MI and stroke over many decades, although recently these improvements are no longer evident. 1,2 Early declines were attributable mainly to primary prevention but, more recently, to more aggressive diagnoses and treatment. 3 There is an increasingly urgent need for primary prevention, as United States life expectancy is no longer increasing due mainly to the stoppage and possible future reversal of the decreasing trends in mortality from CVD. In addition, sudden cardiac death accounts for 50% of deaths from CVD and is the first symptomatic event in at least 25% of cases. 4 Furthermore, in 76% of patients who experience a first stroke, the initial presenting symptom is the stroke itself. 5
Thus, there are increasing challenges to clinicians to aggressively implement a multifactorial approach to risk reduction with therapeutic lifestyle changes (TLCs) and adjunctive drug therapies in the primary prevention of MI and stroke. In this article, we review the evidence as well as suggest methods that clinicians may wish to consider, including both TLCs and adjunctive drug therapies of proven benefit in the primary prevention of MI and stroke.
Therapeutic Lifestyle Changes
Prevention and Treatment of Overweight and Obesity
The prevention and treatment of overweight and obesity is a major TLC of proven benefit in the primary prevention of MI and stroke. In the United States, over 2 of 3 adults are currently overweight or obese, making the current US society the fattest in the world and, possibly, in its history. 5,6 The morbidity and mortality hazards of overweight and obesity have been drastically underestimated due to 3 major methodologic limitations. The first is the failure to control for cigarette smoking. Smokers tend to be thinner due to their appetite suppression by cigarettes and die as much as 10 years earlier than their nonsmoking counterparts. Thus, the failure to control for this important confounder leads to an underestimate of the mortality hazards of overweight and obesity. Second, some investigators have inappropriately controlled for variables in the same causal pathway such as hypertension, dyslipidemia, and diabetes, which are direct effects of overweight and obesity. Third, there has been a failure to exclude participants at baseline in prospective cohort studies whose low weight is due to subclinical but fatal diseases. 6
The Nurse’s Health Study (NHS) enrolled and followed 121 794 dedicated and conscientious female registered nurses and addressed these methodologic limitations. In that prospective cohort study, women at increased weight, as measured by body mass index (BMI), defined as weight in kilograms divided by height in meters squared, experienced 40% of the coronary events. 7 Further, in the Prospective Studies Collaboration which included 57 studies that had enrolled and followed 894 000 men and women, each increase of 5 kg/m2 in BMI was associated with a 40% increase in mortality from CVD, including both MI and stroke. 8 Numerous observational studies have shown that individuals who achieve even modest weight loss experience decreases in mortality from MI and stroke as well as total CVD. 9 Both the United States Preventive Services Task Force (USPSTF) and the American Heart Association (AHA)/American Stroke Association recommend various TLCs to decrease weight in order to reduce the risk of a first MI or stroke. 9,10
Overweight and obesity, specifically central obesity, even in the absence of elevated BMI, lead to dyslipidemia, hypertension, and insulin resistance. Metabolic syndrome, as defined by the National Cholesterol Education Program, is the presence of 3 or more of the following: abdominal obesity as determined by waist circumference >102 cm (>40 inches [in]) for men and >88 cm (>35 in) for women; triglycerides ≥150 mg/dL; high-density lipoprotein cholesterol <40 mg/dL for men and <50 mg/dL for women; blood pressure ≥135/85 mm Hg; fasting glucose ≥110 mg/dL. 11 In US adults, aged 40 and older, metabolic syndrome has increased in prevalence by 35% from 1988 to 2012, from 34.2% to 40%. 12 Primary prevention participants with metabolic syndrome have a 10-year risk of a first MI of 16% to 18%, and also experience a 2-fold increased risk of stroke. 13,14 These sobering statistics have led to a description of metabolic syndrome as the new silent killer as was the case for hypertension decades ago. The TLCs that should be used for the treatment of metabolic syndrome should include both weight loss and regular physical activity. For overweight participants unwilling or unable to adopt TLCs, clinicians should consider drug therapies and, for obese participants, aggressive drug therapies or even surgical approaches to decrease their high risks of MI and stroke.
Regular Physical Activity
Small amounts of daily physical activity may be the closest TLC to a “magic pill” because of the possibilities to achieve significant reductions in body weight, blood pressure, cholesterol, hyperglycemia, and triglycerides. 14 Enhancements in mood, sleep, energy, and sex life are other added benefits. 15 For adults, current recommendations for regular physical activity include either a minimum of 150 minutes each week of moderate intensity aerobic activity, for instance walking, or 75 minutes each week of vigorous aerobic activity. 16 After accounting for other risk factors, physical inactivity has been estimated to be responsible for 12.2% of cases of MI in the United States. 5
In the NHS, women who engaged in moderate physical activity compared with those in the lowest quintile of physical activity had a statistically significant and clinically important reduction in risk of a first MI and stroke. 17 Further, those who walked for just 20 minutes per day, which is achievable for many, if not most, experienced a 30% to 40% reduction in risk of MI and stroke. 18
Despite the fact that engaging in 20 minutes of regular physical activity daily, specifically, a brisk walk that can be continued even among the oldest old, can have statistically significant and clinically important benefits, only around 20% of US adults actually engage in the recommended levels. 19 Clinicians should discuss current recommendations for physical activity with their patients and attempt to guide and encourage their patients to think about how they may be able to incorporate them into their daily routines based on their individual circumstances.
Avoidance and Cessation of Cigarette Smoking
In the United States, cigarette smoking has long been the leading avoidable cause of premature death. At present, overweight and obesity are beginning to overtake cigarettes due, in part, to remarkable declines in smoking rates in the United States. 6 Nonetheless, in the United States and most developed countries, cigarette smoking accounts for very large numbers of avoidable premature deaths. Worldwide, the alarming increases in cigarette smoking is a major contributor to the alarming global increases in mortality from CVD from fifth to first as a cause of death. 20 The amount currently smoked is a major risk factor for MI and stroke. Thus, a 4 pack per day smoker for 10 years has a far higher risk of MI or stroke than a 1 pack per day smoker for 40 years although each has experienced 40 pack-years of smoking. Further, in general, current smokers have about twice the risk of MI or stroke than nonsmokers, including the elderly population. 21 Finally, for CVD, cessation of smoking leads to declines in risk beginning within a few months and reaches that of a nonsmoker within a few years. In contrast, for lung cancer, duration is a far more major risk factor, and, as a consequence, cessation causes no decrease for several years after quitting, and even after 10 years the risks remain midway between those of a continuing smoker and nonsmoker. Thus, for CVD, it is never too late to quit, even among the elderly population, but for cancer it is never too early. 21
Clinicians should educate patients about the risks of smoking as well as about the benefits of cessation on MI and stroke that begin to accrue even within a few months. The success rate of smoking cessation can be increased by incorporating behavioral and pharmacologic interventions, such as varenicline, which can lead to permanent cessation in about 1 of 5 to 1 of 3 of participants. 22,23
Healthy Diet
In numerous observational studies, both case–control and cohort as well as their meta-analyses, men and women who adopt a healthy diet experience significantly decreased risks of a first MI and stroke. 24,25 Specifically, those who self-select for increased consumption of fruits and vegetables have significantly decreased risks of MI and stroke. Further, individuals who adhere to the Mediterranean diet, when compared to those who consume a low-fat diet, experience a 30% reduction in risk of CVD, principally MI and stroke. 24 In a meta-analysis of 8 observational studies, individuals who consume more than 5 servings of fruits and vegetables per day have further significant reductions in the risk of MI and stroke, compared to those who consume less than 3. In addition, those who consume 3 to 5 servings per day of fruits and vegetables have lower risks than those who consume less than 3. Finally, those who consume less sodium or more potassium also have decreased risks of MI and stroke, due, at least in part, to direct effects on blood pressure. 9
In a multicenter trial in Spain, 7447 patients at high risk of a first MI and stroke were randomized to 3 diets consisting of a Mediterranean diet supplemented with olive oil, a Mediterranean diet supplemented with mixed nuts, or a reduced fat diet. In this randomized trial, patients assigned to both the Mediterranean diet with extra virgin olive oil and those supplemented with mixed nuts both experienced significantly lower risks of major cardiovascular events of 31% and 28%, respectively. 26 Long-term adherence to a healthy diet that includes calorie restriction is vital to the primary prevention of MI and stroke and may avoid the need for adjunctive drug therapies for many US adults. 27 It is important to note that dietary changes pose particular challenges for patients, as they are difficult to achieve as well as to maintain but they do lead to appreciable benefits on MI and stroke risk. Guidance to patients about diet is well worth the clinician’s time to help their patients to set goals and encourage them to reach those goals.
Avoidance of Heavy Alcohol Consumption
In most populations throughout the world, individuals who consume large amounts of alcohol have the highest risks of CVD, including MI and stroke. Most patients seem less aware of this fact but are well aware that those who consume small amounts of daily alcohol tend to have lower risks than teetotalers. In addition, most patients are also less aware that those who consume more than 15 to 30 g of alcohol or ≥1 to 2 standard drinks daily have significantly increased risks of MI and stroke. 28,29
The totality of evidence suggests that any benefits from consuming small amounts of daily alcohol are similar for each type consumed. 28,29 Thus, in most prospective cohort and case–control studies, individuals who self-select to drink a glass of red wine experience the same health benefits as those who self-selected for a glass of white wine, a glass of beer, or shot of whiskey.
Of perhaps greatest importance, clinicians should educate their patients that the difference between drinking smaller and larger amounts of alcohol may mean the difference between preventing and causing premature death since rates of MI and stroke as well as hypertension, hemorrhagic stroke, and breast cancer all begin to rise above 1 drink daily, especially in women. 28 –30
Adjunctive Drug Therapies
Statins
The available evidence indicates clear and conclusive benefits of statins in the primary prevention of MI and stroke. In numerous randomized trials of over 170 000 patients in primary and secondary prevention, as well as their meta-analyses, statins produce both statistically and clinically significant reductions in MI and stroke as well as CVD and total mortality. 31 Further, more versus less intensive statin therapy produces incremental benefits on MI and stroke in the highest risk post-acute coronary syndrome patients as well as moderate-risk patients with chronic stable coronary disease. In primary prevention, perhaps the most conclusive randomized data have emerged from the Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin (JUPITER) trial. 32 In JUPITER, 17 802 apparently healthy men and women, generally not considered candidates for statin therapy, were assigned at random to 20 mg of rosuvastatin daily or placebo for a scheduled duration of 5 years. The participants were chosen based on an elevation of high-sensitivity C-reactive protein, a sensitive marker of inflammation and accurate predictor of future risk of CVD. Those assigned at random to rosuvastatin achieved an average low-density lipoprotein cholesterol of 55 mg/dL compared to 109 mg/dL in the placebo group. After only 1.9 years, an independent Data and Safety Monitoring Board unanimously recommended early termination due to a 44% reduction in the primary prespecified combined end point of major adverse cardiovascular events which included MI, stroke, revascularization, hospitalization for unstable angina, and death from cardiovascular causes (P < .0001). Although the trial was terminated early based on a statistically extreme benefit on the primary prespecified combined end point, after only 1.9 years of treatment and follow-up, there were also significant reductions in 3 of the 5 components, including 54% for MI (hazard ratio [HR] = 0.46; 95% confidence interval [CI]: 0.30-0.70), 48% for stroke (HR = 0.52; 95% CI: 0.34-0.79; P = .002), and 46% for revascularization (HR = 0.54, 95% CI: 0.41-0.72). There was also a statistically significant reduction of 20% for total mortality (HR = 0.80; 95% CI: 0.67-0.97; P = .02). In JUPITER as well as the meta-analyses of all trials of primary prevention, women experience similar benefits to men on MI and stroke. 33
Recommendations are in general agreement that statins should be considered a crucial component of all strategies in the primary prevention of MI and stroke as well as a wide range of other manifestations of CVD. The ACC/AHA guidelines recommend screening patients with the ACC/AHA pooled cohort risk equation, and initiating treatment with moderate or high intensity statin in primary prevention participants with a 10-year risk of coronary heart disease of ≥7.5% 34 (see Table 1).
Moderate and High Intensity Statins.
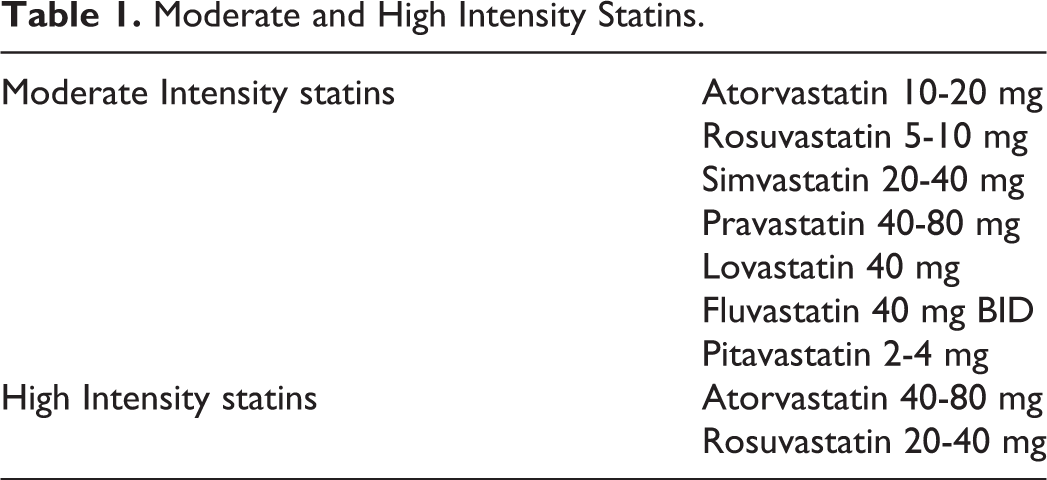
The evidence to support the use of nonstatin lipid-lowering regimens is less robust, but they should be considered in specific situations either as adjuncts or where statins may be contraindicated. At present, the only adjunctive drug therapy to statins of demonstrated additive benefit is ezetimibe, and the magnitude of the added benefit is small. Thus, evidence-based doses of a moderate- or high-intensity statin should be the first-line drug of choice, especially for high-risk patients with metabolic syndrome who constitute 40% of adult men and women in the United States. 9
Multiple Drug Therapies for High Blood Pressure
Hypertension is one of the most common conditions seen in primary care offices and is a major risk factor for MI and stroke as well as other manifestations of CVD. Using the most recent guidelines from the ACC/AHA, which defines hypertension as values ≥130 mm Hg for systolic blood pressure and 80 mm Hg for diastolic, hypertension affects over 45% of the US adult population. 35 In addition to TLCs, patients with hypertension will often need drug therapies to achieve the blood pressure goal. Unlike lipid management with high-intensity statins where a single drug will suffice, most patients with hypertension will require 2 or 3 blood pressure medications to achieve the recommended targets. Drug therapies of proven benefit include diuretics, angiotensin-converting enzyme inhibitors or blockers, and calcium channel blockers. 36 In randomized trials and their meta-analyses in patients with mild to moderate hypertension defined as >140/90, drug therapies produce a 4 to 5 mm Hg reduction, resulting in statistically significant and clinically important reductions in risk of a first MI of 14% and first stroke of 42%. 37 The recently published SPRINT trial of intensive blood pressure lowering was terminated early due to a statistically extreme reduction in risk for the primary prespecified composite cardiovascular end point, of MI, stroke, acute coronary syndrome, congestive heart failure, or CV death. 38
Clinicians should be aware that early detection of hypertension by screening and control through TLCs and usually multiple adjunctive drug therapies are important factors in reducing risks of a first MI or stroke. The USPSTF and ACC/AHA guidelines recommend that patients should have their blood pressure monitored annually. 9,39 The TLCs should be initiated for all patients, especially those above 130/80, and pharmacotherapy initiated for those with blood pressures ≥140/90.
Aspirin
In the randomized trials of primary prevention with aspirin, 30 years ago, the Physicians’ Health Study (PHS) of 22 071 apparently healthy men was the first to demonstrate a statistically extreme benefit on reducing the risk of a first MI, 40,41 and the Women’s Health Study (WHS) of 39 872 apparently healthy women was the first to demonstrate a benefit on reducing the risk of a first stroke. 42 At present, despite the availability of data from numerous trials and their meta-analyses, the totality of evidence remains incomplete. In a comprehensive meta-analysis of 6 major primary prevention trials, aspirin significantly reduced the incidence of major coronary events, strokes, and all serious vascular events. 43 In terms of relative risk reductions, the findings from the meta-analysis of the trials of primary prevention are similar to those in secondary prevention. In secondary prevention, however, the absolute benefit of aspirin is large in relation to the absolute risks, primarily major extracranial bleeding. In primary prevention, if one assumes that the risk of a bleeding event is the same as for secondary prevention, then, based on the evidence from moderate risk primary prevention participants, the benefits will tend to outweigh the risks only when the 10-year risk of a coronary event begins to exceed 10%. In addition, while age is a well-known risk factor for occlusive vascular events, but age is also associated with increased risks of bleeding. Further, until very recently, nearly 80% of participants were low-risk participants randomized in the PHS (10-year risk of 4.8%) and the WHS (10-year risk of 2.5).
Very recently, the results of 3 large-scale trials of aspirin in primary prevention in participants at moderate risk have been reported. The A Study of Cardiovascular Events iN Diabetes (ASCEND) trial randomized 15 480 participants at least 40 years of age with diabetes and showed a statistically significant benefit on major vascular events (RR = 0.88, 95% CI: 0.79-0.97; P = .010). 44 The Aspirin to Reduce Risk of Initial Vascular Events (ARRIVE) trial randomized 12 546 participants older than 55 for men and older than 60 for women with moderate cardiovascular risk and showed no significant reduction in the primary combined CVD event (HR = 0.96; 95% CI: 0.81-1.13). 45 Finally, the Aspirin in Reducing Events in the Elderly (ASPREE) trial randomized 18 117 participants older than 70 and showed no significant reduction in the primary combined CVD end point (HR = 0.95; 95% CI: 0.83-1.08). It may be of importance to note that follow-up rates were far higher in ASCEND than in either ARRIVE or ASPREE. 44 –46 Perhaps of even greater importance, adherence rates were about 70% in both groups in ASCEND and about 60% in both groups in ASPREE. 44,46 The adherence rates at the time of the event is a particularly important issue in all trials of aspirin as the half-life of the platelet is about 8 days which is why those undergoing elective surgery are asked to stop the drug for at least one week. Finally, it might be helpful to understand the interrelationships of aspirin and statin use with adherence and follow-up. All these considerations may have contributed to a failure to detect a small-to-moderate benefit in ARRIVE or ASPREE which had been reported in the previous trials among older adults. All these considerations emphasize the crucial importance to conduct another worldwide meta-analysis of trials using individual participant data which would shed light on whether, and, if so, which of these methodologic limitations influenced the overall results.
When the totality of evidence is incomplete, it is appropriate to remain uncertain. 47 Thus, based on the current evidence, judgments about prescribing long-term aspirin therapy for apparently healthy individuals should only be made on an individual case-by-case basis. General guidelines for the prescription of aspirin in primary prevention do not seem to be justified. Further, the increasing burden of CVD in the United States and other developed as well as developing countries underscores the need for the wider prescription of drug therapies of proven net benefit, such as statins, and multiple drugs, where necessary, to lower blood pressure. 48 This individual clinical decision-making may affect many primary prevention participants that are at particularly high risk of a first MI or stroke, such as those older than 40 with metabolic syndrome, who have a 10-year risk of a first CHD event of 16% to 18%. 13 Finally, clinicians should consider that the benefits of statins and aspirin, are, at the very least, additive. 49
If a clinician decides to prescribe aspirin in primary prevention, it is also important to educate patients since only 50% of patients prescribed the drug are taking it. Furthermore, over 1 in 5 patients who think they are taking aspirin are actually taking either a traditional nonsteroidal anti-inflammatory drug, which has prothrombotic effects or acetaminophen, which has no antiplatelet effects. In primary prevention, the prescription of aspirin should be based on an individual clinical judgment and only when the magnitude of the absolute benefit exceeds the magnitude of the absolute risk, which is chiefly major extracranial bleeding. When the magnitude of benefit is similar to that of risk, patient preference may be considered. Such issues may be relevant to primary prevention participants who feel that the prevention of an MI or stroke is more important than the development of a gastrointestinal bleed.
Insulin Resistance and Hyperglycemia
The pandemic of overweight and obesity has, perhaps not surprisingly, also spawned a pandemic of type 2 diabetes mellitus. Insulin resistance, a component of the metabolic syndrome, is a known precursor of type 2 diabetes mellitus. 50 The development of type 2 diabetes in primary prevention participants with and without metabolic syndrome will increase their risks of CVD about 2- to 3-fold in men and 4- to 6-fold in women. 51 Diabetes leads to macrovascular complications such as MI and stroke and microvascular complications, principally ocular and renal. Nonetheless, MI and stroke are far and away the leading causes of death in patients with type 2 diabetes, and heart failure is also a major cause of their hospitalizations and deaths. 51,52
The American Diabetes Association recommends screening all adults older than 45 years, those with a history of gestational diabetes, and any asymptomatic adult who is overweight or obese with at least one additional risk factor for diabetes. 53 The USPSTF recommends screening patients who are overweight or obese between the ages of 40 to 70 years (see Table 2). 54 The implementation of multifactorial interventions, including TLCs and adjunctive drug therapies, by clinicians for their individual patients and policymakers for the health of the general public can markedly reduce the premature morbidity and mortality associated with diabetes mellitus, especially MI and stroke.
Recommendations for Screening for Diabetes Mellitus.

Abbreviations: CVD, cardiovascular disease; HDL, high-density lipoprotein; USPSTF, United States Preventive Services Task Force.
Conclusions
The AHA has proposed 7 metrics for cardiovascular health, which include avoidance or cessation of smoking, maintenance of a normal body weight, a healthy dietary pattern, regular physical activity, as well as optimal total cholesterol, blood pressure, and fasting glucose in the absence of drug treatment. In the United States, only 0.1% of the population meet all the criteria, 4% meet 6, and 13% meet 5. 5 These sobering statistics pose major challenges to clinicians and their patients in the primary prevention of MI and stroke. The multifactorial interventions of proven benefit in the primary prevention of MI and stroke include TLCs and adjunctive drug therapies. Many of these interventions would be optimally achievable with an interprofessional approach that facilitates patient engagement with resources outside the office visit. The effective implementation of these interventions by clinicians for their individual patients can lead to significant reductions in premature morbidity and mortality from MI and stroke. A sufficient totality of evidence that includes reliable data from large-scale randomized trials designed a priori to test a hypothesis is necessary to develop rational guidelines. 55,56 Guidelines, however, should provide only the framework to the health-care provider who is in the best position to make informed clinical decisions for each of his or her patients. The recognition and implementation of these TLCs and adjunctive drug therapies by health-care providers for their individual patients and policymakers for the health of the general population will contribute to significant improvements in MI and stroke as major causes of premature and avoidable morbidity and mortality in the United States and worldwide.
Footnotes
Author Contributions
All coauthors contributed to the drafting and revisions of this review.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Professor Hennekens also reports that he serves as an independent scientist in an advisory role to investigators and sponsors as Chair or Member of Data and Safety Monitoring Boards for Amgen, British Heart Foundation, Cadila, Canadian Institutes of Health Research, DalCor, and Regeneron; to the Collaborative Institutional Training Initiative (CITI); United States Food and Drug Administration, and UpToDate; receives royalties for authorship or editorship of 3 textbooks and as coinventor on patents for inflammatory markers and CVD that are held by Brigham and Women’s Hospital; has an investment management relationship with the West-Bacon Group within SunTrust Investment Services, which has discretionary investment authority; does not own any common or preferred stock in any pharmaceutical or medical device company.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Drs Martinez, Foster, Sherling and Professor Hennekens report that they are funded by the Charles E. Schmidt College of Medicine of Florida Atlantic University.