
Abstract
Introduction
Intra-aortic balloon pump (IABP) has been widely used ever since it was first developed in 1962 and became part of clinical practice in 1968.1,2 Today this circulatory-assist devise is used to treat patients with complications of acute myocardial infarction (AMI) such as cardiogenic shock, 3 refractory left ventricular failure, 4 and for high-risk patients undergoing angioplasty and coronary artery bypass grafting (CABG). 5
Recent results from the Benchmark Counterpulsation Outcome Registry showed that despite IABP insertion, in-hospital mortality in these patients remains high (21.2%). Rate of complications are more in women, elderly patients, and patients with peripheral vascular disease. 6 Prospective analysis of 691 patients revealed that despite technological advances allowing easier IABP insertion, using catheters with smaller diameters and sheathless insertion techniques, complications associated with IABP insertion remain high. The frequency of complications ranges from 12% to 42%, with most series reporting an incidence between 15% and 30%. 7
Another study comparing outcomes of IABP in US and non-US centers found that all-cause, risk-adjusted, in-hospital mortality (20.1% vs 28.7%; P < .001), and mortality with IABP in place (10.8% vs 18.0%; P < .001) were lower at US vs non-US sites. In both US and non-US institutions, IABP-associated complication rates, such as IABP-related mortality (0.05% vs 0.07%), major limb ischemia (0.9% vs 0.8%), and severe bleeding (0.9% vs 0.8%), were low. The reason for the difference in mortality is thought to be more prophylactic use of IABP at early stages of patient’s illness at US centers as compared to non-US centers. 8 On the contrary, a prospective randomized study by Stone et al, demonstrated no difference in mortality with prophylactic use of IABP versus conservative treatment in patients with AMI undergoing percutaneous transluminal coronary angioplasty (PTCA).9–11
Thus, current literature demonstrates a significant variance in terms of indications for using IABP and its outcomes. The aim of this study was to review the existing literature to analyze whether use of IABP offers any cardiovascular benefit to the patients with AMI and the complications associated with the use of IABP.
Materials and Methods
We performed this review in accordance with the Quality of Reporting of Meta-Analysis (QUOROM) statement and the Consolidated Standards of Reporting Trials (CONSORT) Group recommendations. 12
Study Selection
A literature search was done by 2 investigators independently using the PubMed computerized database (1966-2009), Cochrane Controlled Trials Register (1970-2009), EMBASE (1980-2009), and CINAHL (1982-2009). The search was restricted to the articles including human participants. In addition, manual searches were performed through the reference lists of published articles and review articles. Any unpublished studies were excluded. For IABP, the following search terms were used: “Intra-aortic Balloon Counterpulsation, Intra-aortic Balloon Pump, Heart assist device.” For heart disease, the following search terms were used: “Acute myocardial infarction, cardiogenic shock, PTCA.” Study selection process is outlined in Figure 1 .
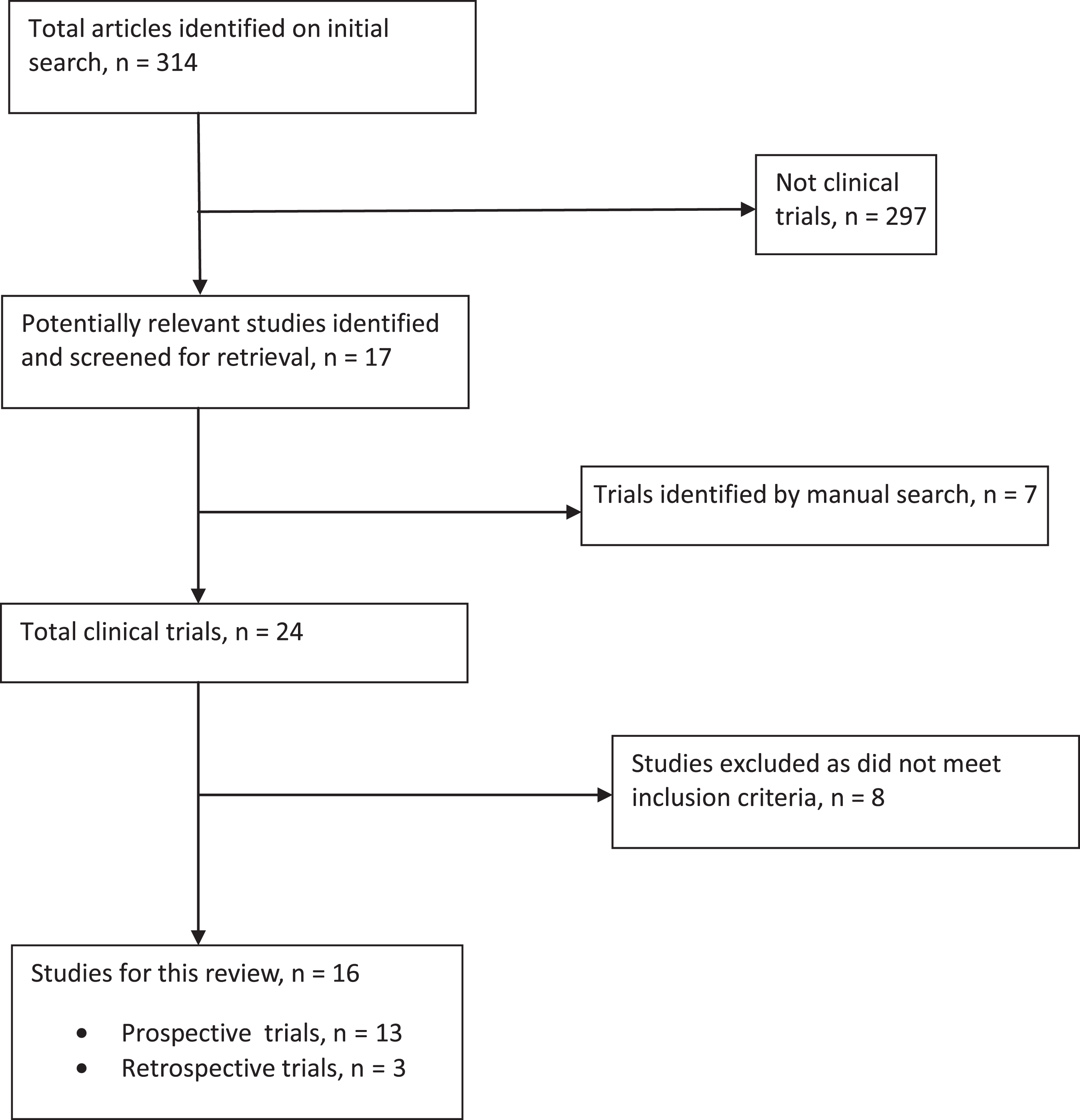
Study selection process.
Inclusion Criteria
Inclusion criteria utilized for the current meta-analysis were as follows: All prospective randomized, nonrandomized studies, and retrospective studies comparing the effects of IABP with no IABP in patients with AMI, with or without cardiogenic shock were included irrespective of the sample size. Studies providing sufficient information for the calculation of relative risk (RR) and odds ratio (OR), as well as those studies that readily provided these or other accepted risk estimates.
Exclusion Criteria
Exclusion criteria were as follows: Studies done on animals. Duplicate studies (Studies originating from same participants by the same investigators but published in different journals). Studies published in a language other than English. Studies comparing prophylactic IABP versus rescue IABP (for intraprocedural complications). Studies comparing the effects of different techniques of IABP (eg, gradual prolonged versus standard balloon inflation). Letters to editors, unpublished articles, and articles providing insufficient information to calculate the RR were excluded.
Two investigators independently reviewed the searched articles. Final decision about inclusion or exclusion was made by mutual agreement.
Data Extraction
Using a standard protocol, the 2 investigators collected the following data from the research articles: name of the authors, name of the journal, date of publication, sample size, study design, demographic characteristics of the population, and outcome of the study. In addition, how well the studies were adjusted for confounding variables and whether the outcomes were measured in a standard, valid, and reliable way were assessed. In the 8 randomized-controlled trials13–20 included in this meta-analysis, the patients with IABP did not differ from patients without IABP in terms of known cardiovascular risk factors such as age, gender, diabetes, hypertension, previous myocardial infarction, and peripheral vascular disease. These trials did not allow for the use of IABP in the control group. The crossover rates were available only for 2 trials.16,18 Five prospective trials were not randomized and had differences in the baseline demographic characteristics, cardiovascular risk factors, and hemodynamic stability. It was unethical according to these studies not to use IABP in hemodynamically compromised individuals and obvious bias in the selection of patients for IABP was observed. Three studies used in our analysis were retrospective and similar bias was observed in these studies.
Therefore, the 2 investigators used criteria developed by the US Preventive Services Task Force (USPSTF) to determine internal validity of the individual studies included in meta-analysis. 21 Studies were rated in 3 categories, “Good, Fair, and Poor” on the basis of the criteria shown in Table 1 .
Study Details
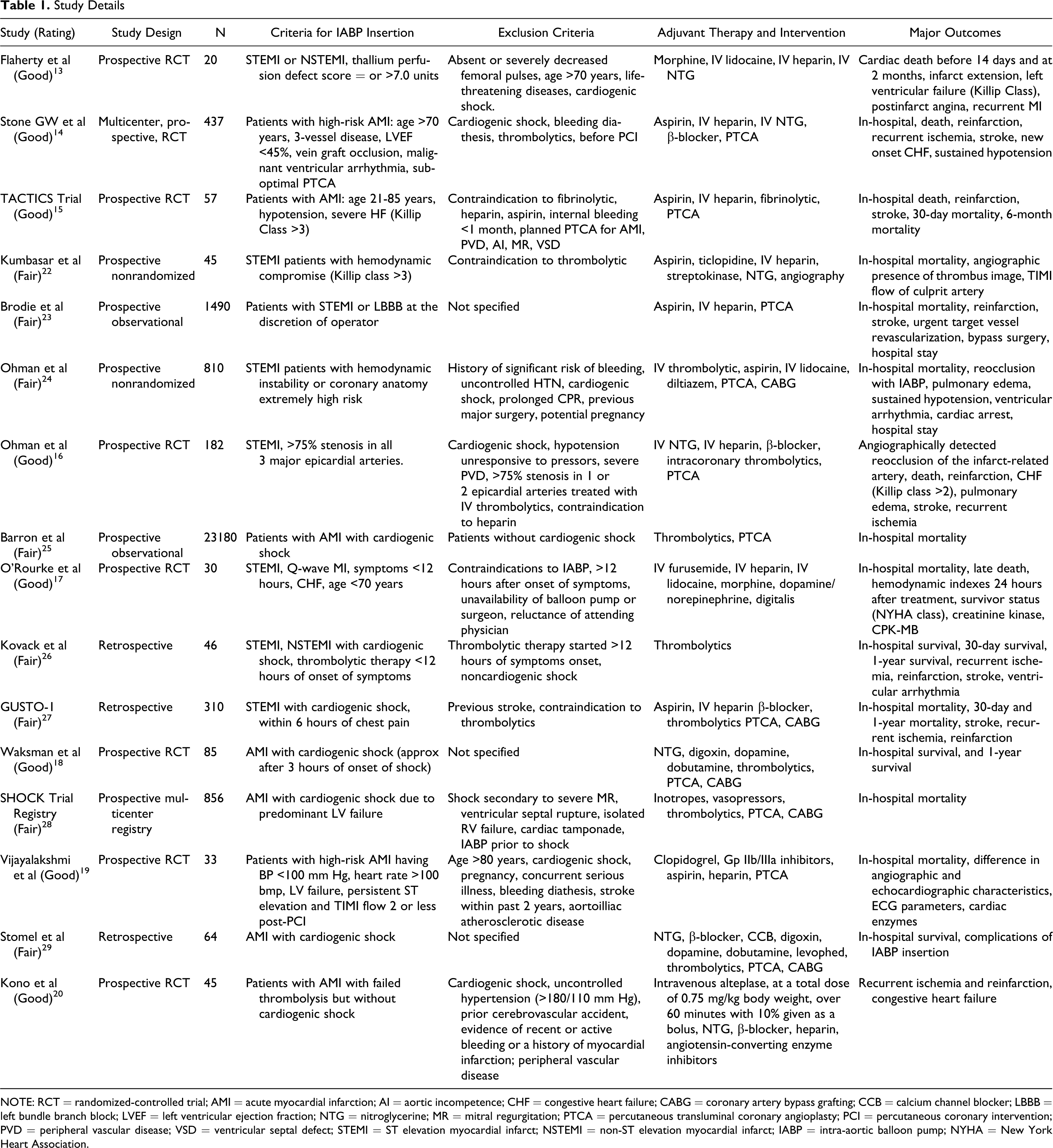
NOTE: RCT = randomized-controlled trial; AMI = acute myocardial infarction; AI = aortic incompetence; CHF = congestive heart failure; CABG = coronary artery bypass grafting; CCB = calcium channel blocker; LBBB = left bundle branch block; LVEF = left ventricular ejection fraction; NTG = nitroglycerine; MR = mitral regurgitation; PTCA = percutaneous transluminal coronary angioplasty; PCI = percutaneous coronary intervention; PVD = peripheral vascular disease; VSD = ventricular septal defect; STEMI = ST elevation myocardial infarct; NSTEMI = non-ST elevation myocardial infarct; IABP = intra-aortic balloon pump; NYHA = New York Heart Association.
On the basis of the above-set criteria, 15 studies in patients with acute ST elevation myocardial infarct (STEMI) or non-STEMI (NSTEMI) with or without cardiogenic shock were identified. We analyzed the primary endpoints (in-hospital mortality, reinfarction, and recurrent ischemia) and secondary endpoint (incidence of moderate and severe bleeding during hospitalization/at 7 days).
Definitions
Acute myocardial infarction included patients with STEMI, NSTMI, new onset left bundle branch block, or Q-wave infarct. Patients experiencing chest pain for more than 20 minutes but less than 12 hours were considered for inclusion in most of the studies. Cardiogenic shock was defined as systolic blood pressure <90 mm Hg for more than 30 minutes that is unresponsive to fluids or a cardiac index of <2.2 L/min per m2. High-risk patients without cardiogenic shock mainly included patients with blood pressure (BP) <100 mm Hg, postprocedure thrombolysis in myocardial infarction (TIMI) risk score 0 to 2, persistent ST elevation postprocedure, left ventricular ejection fraction <45%, vein graft occlusion, and persistent malignant ventricular arrhythmias. Flaherty et al 13 included patients with thallium defect score of 7.0 units or greater, suggestive of extensive myocardium at risk of infarction.
The primary efficacy endpoints were the composite of death from any cause, nonfatal reinfarction, and recurrent ischemia. The definitions of these events were taken from the articles included in our study. Reinfarction was mainly defined by recurrent ischemic symptoms lasting >15 minutes, new ST-T wave changes, new Q-waves, or elevation of cardiac enzymes above its previous nadir. Recurrent ischemia was defined by chest discomfort, electrocardiograph (ECG) changes, new hypotension, or onset of new murmur. The secondary endpoints were incidence of moderate and severe bleeding during index hospitalization or approximately at 7 days. Severe bleeding was defined as intracranial, intraocular, or retroperitoneal hemorrhage, clinically overt blood loss leading to hemodynamic compromise or hemoglobin drop exceeding 3 g/dL (or 10% of hematocrit), transfusion of 2 or more units of packed red blood cells. Moderate bleeding was considered bleeding that needed blood transfusion but did not lead to hemodynamic instability. This definition was not explicitly mentioned in all the studies that reported moderate bleeding.
We did not attempt to reclassify outcome events retrospectively, because such an attempt not only would be impractical but would also create the potential for bias. Since the outcome definitions were the same within a particular trial and the statistical method was based on a comparison of treatment groups within each trial, no material biases would be expected to result from this approach.
Statistical Methods
Meta-analysis was done using RevMan software (Review Manager [RevMan]. Version 4.2 for Windows. Copenhagen: The Nordic Cochrane Centre. The Cochrane Collaboration, 2003). We estimated the proportion of between-study inconsistency (heterogeneity) due to true differences between studies (rather than differences due to random error or chance) using the I2 statistic. Mantel-Haenszel fixed-effect model was used to calculate the combined RRs when studies were homogenous and the random effect model was used when studies were heterogenic. A 2-sided α error of <.05 was considered statistically significant.
Results
Literature Search
Applying the search terms, 1076 articles were identified, of which 24 articles were found to be relevant. After applying inclusion and exclusion criteria, 16 articles remained eligible for meta-analysis, of which 13 were prospective studies and 3 were retrospective studies.13–20,22–29 Eight studies were excluded because no control arm was available, 30 no mortality data were available,31–34 or there was different timing of outcomes.35–37 Thus, the systematic literature search for studies comparing the effects of IABP with no IABP in patients with AMI, with or without cardiogenic shock using aforementioned criteria revealed a total of 16 studies (N = 11 778). Of 16 studies, 1 study provided data only for recurrent ischemia and no mortality data was available. 20 Overview of study characteristics is given in Table 1.
Clinical Outcomes
In-hospital mortality
Meta-analysis revealed that in-hospital mortality of patients with AMI with and without cardiogenic shock did not differ between IABP group as compared to no IABP group (RR: 1.11; CI: 0.69-1.78; P = .67; Figure 2 upper panel). Since the National Registry of Myocardial Infarction 2 (Barron et al 25 ) contributed the maximum number of patients (N = 72 968; 61.78%) in this analysis, which can lead to bias of dominance, we performed another analysis excluding this study. The overall results did not change (RR: 1.10; CI: 0.56-2.14; P = .79).
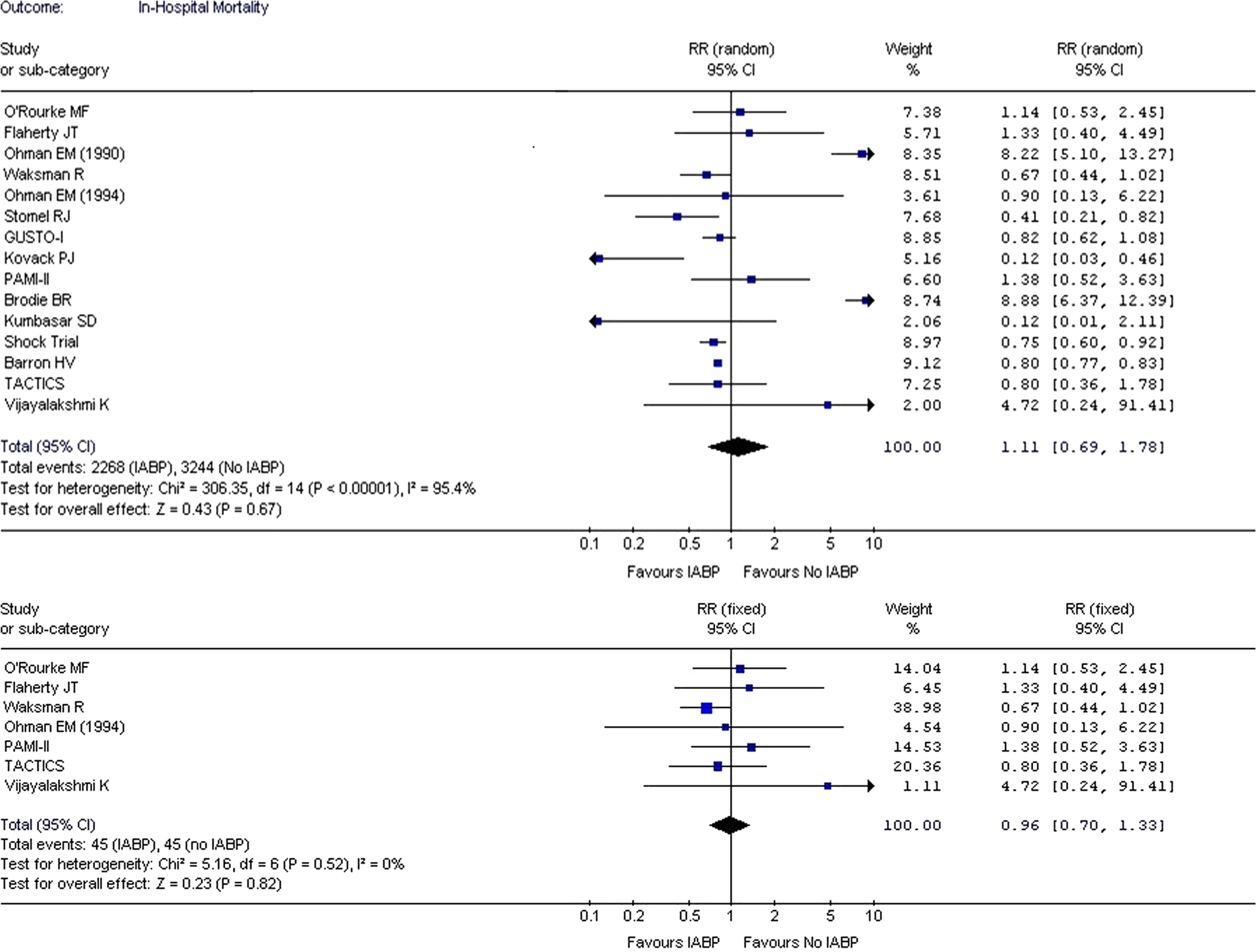
A meta-analysis is generally performed by combining randomized trials since adequate randomization reduces the chance of any bias. Combining such studies in the meta-analysis reduces sampling variation that might occur in individual studies. When the analysis was done using only randomized studies (7 studies),13–19 it did not show any difference in the in-hospital mortality between IABP and no IABP group (RR: 0.96; CI: 0.70-1.33; P = 0.82; Figure 2 lower panel).
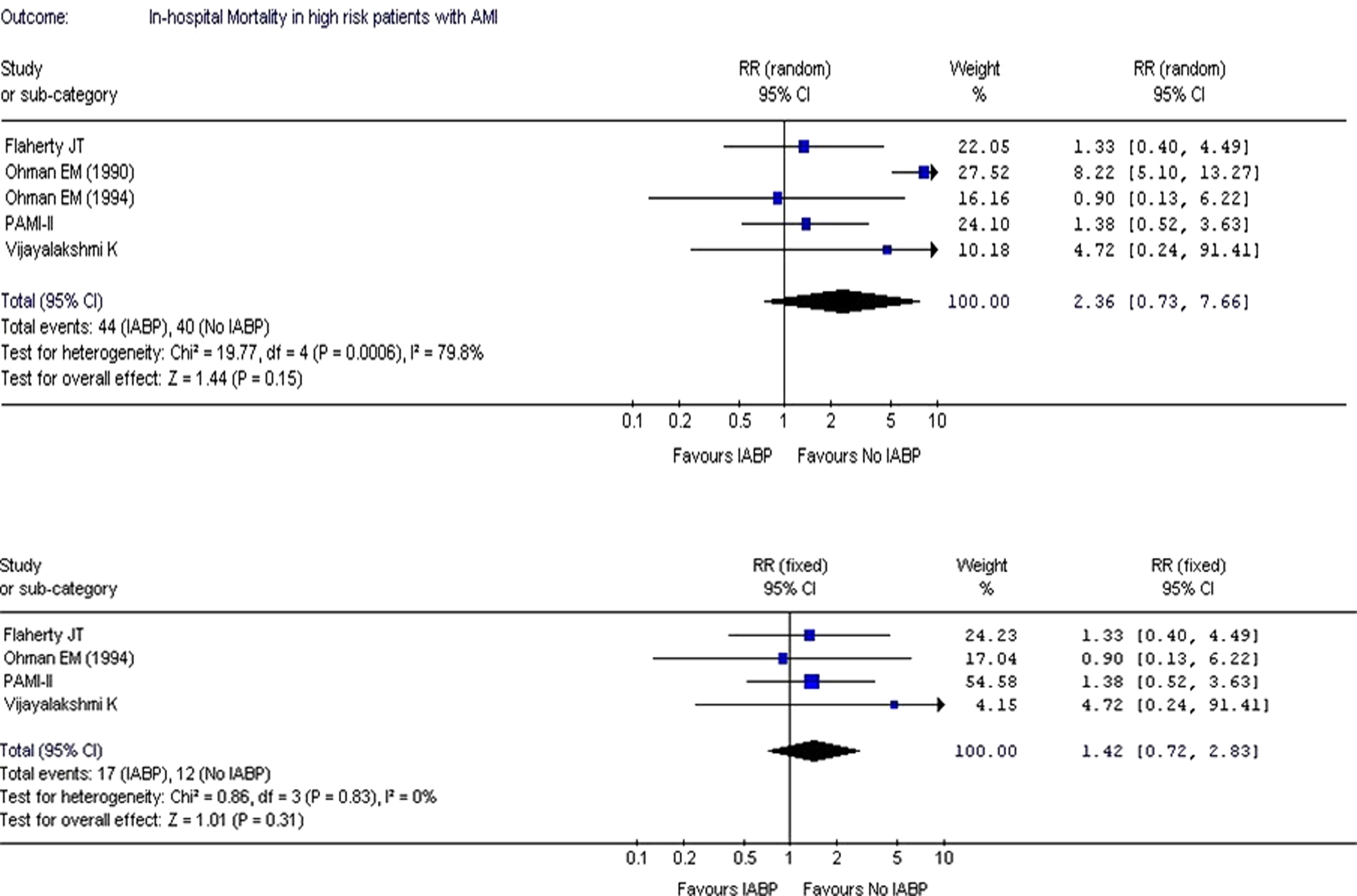
The in-hospital mortality did not improve (RR: 2.36; CI: 0.73-7.66; P = .15) when the analysis was performed on studies that included patients with high-risk AMI without cardiogenic shock (Figure 3 upper panel)13,14,16,19,24. Restricting the analysis to only randomized-controlled trials (4 studies)13,14,16,19 did not change the results (RR: 1.42; CI: 0.72-2.83; P = .31; Figure 3 lower panel).
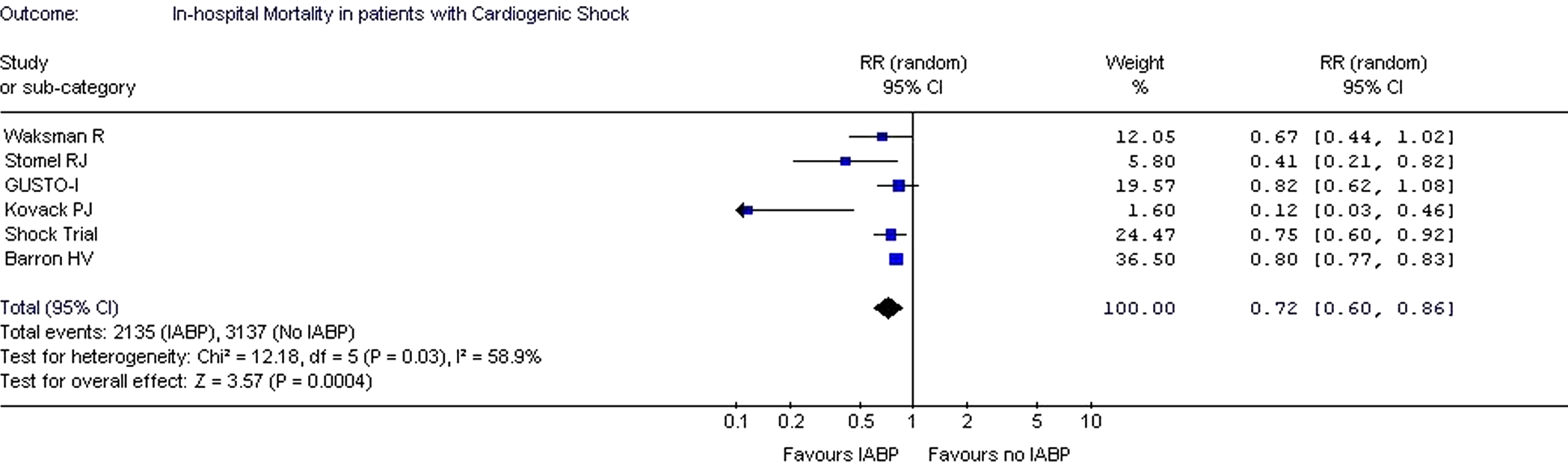
As seen in Figure 4 , when analysis was restricted to the patients with AMI with cardiogenic shock, significantly improved outcome in terms of in-hospital mortality was observed in the IABP group (RR: 0.72; CI: 0.60-0.86; P < .0004).18,25,26–29
Recurrent Ischemia and Reinfarction
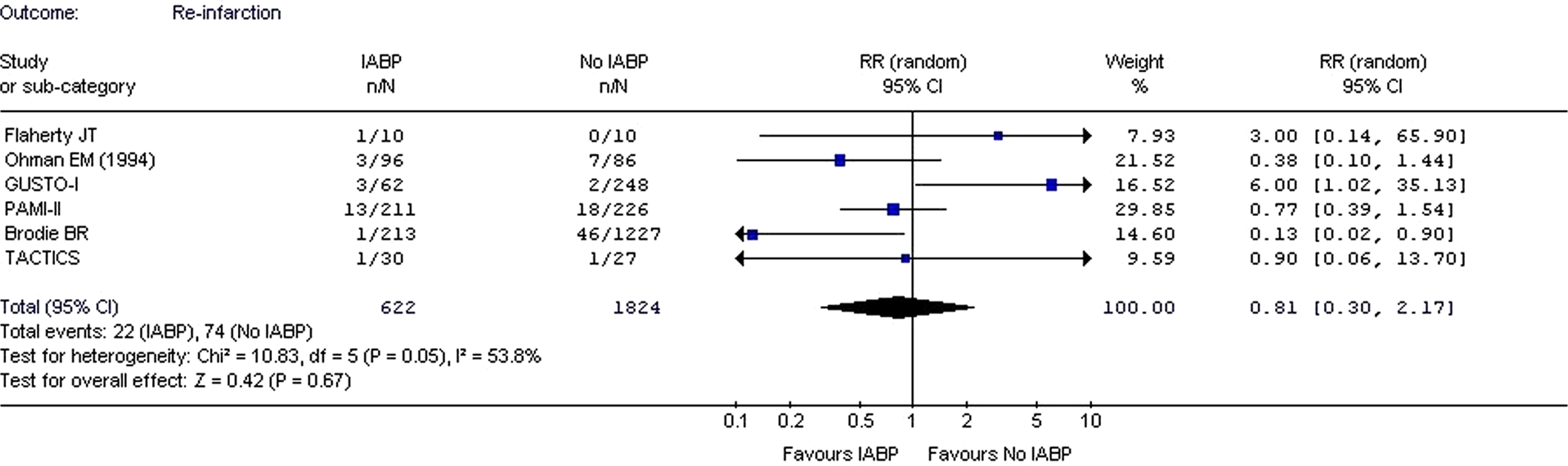
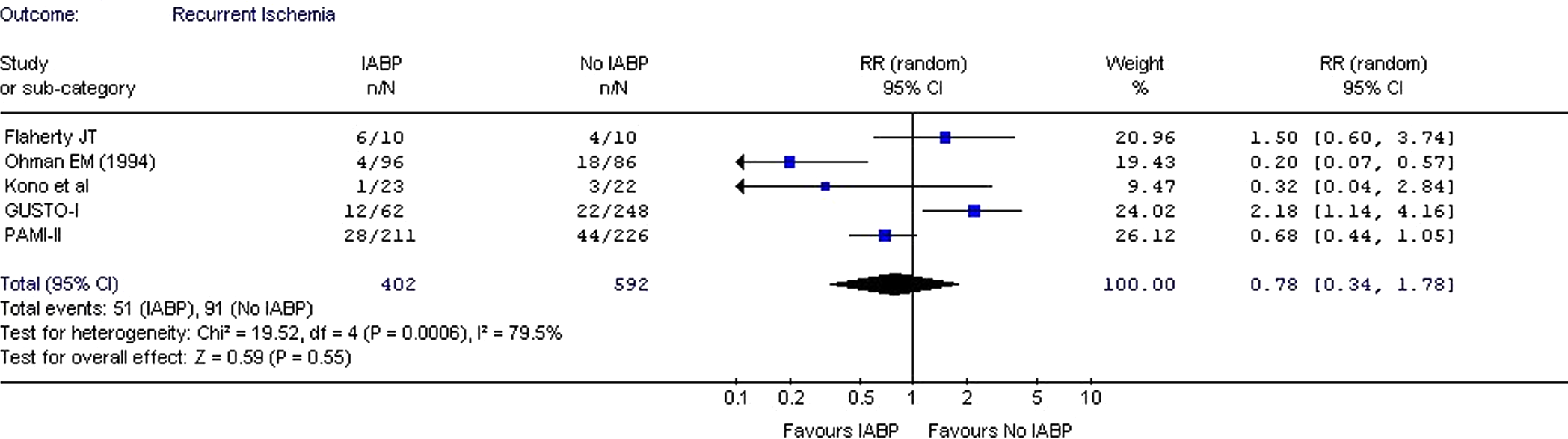
A total of 6 studies provided the data on reinfarction13–16,23,27 and 5 studies provided data on recurrent ischemia.13,14,16,20,27 Analysis of these studies failed to demonstrate significant decrease in the rate of reinfarction (RR: 0.81; CI: 0.30-2.17; P = .67) or recurrent ischemia (RR: 0.78; CI: 0.34-1.78; P = .55) using IABP (Figures 5 and 6 ).
Bleeding Complications
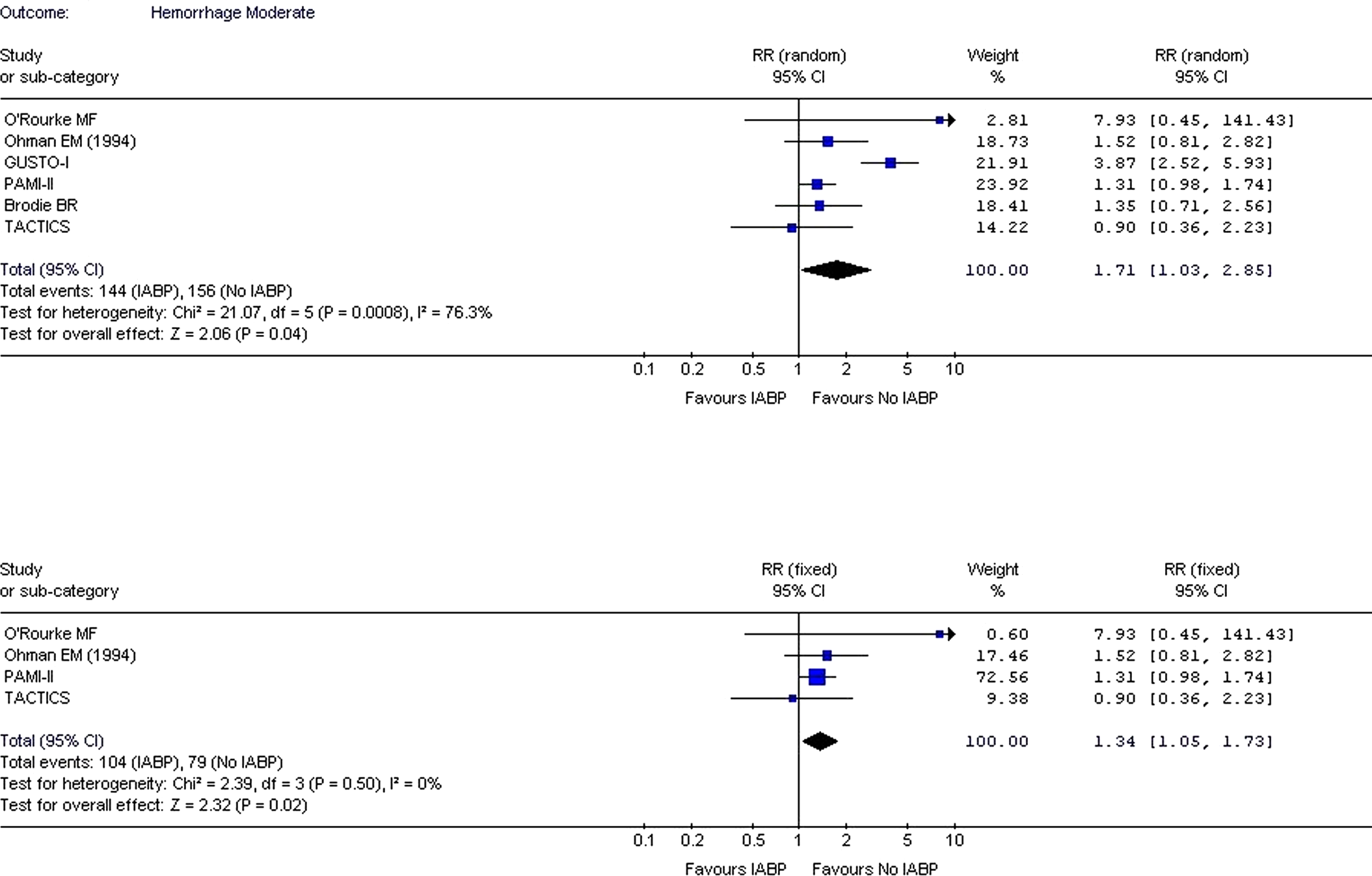
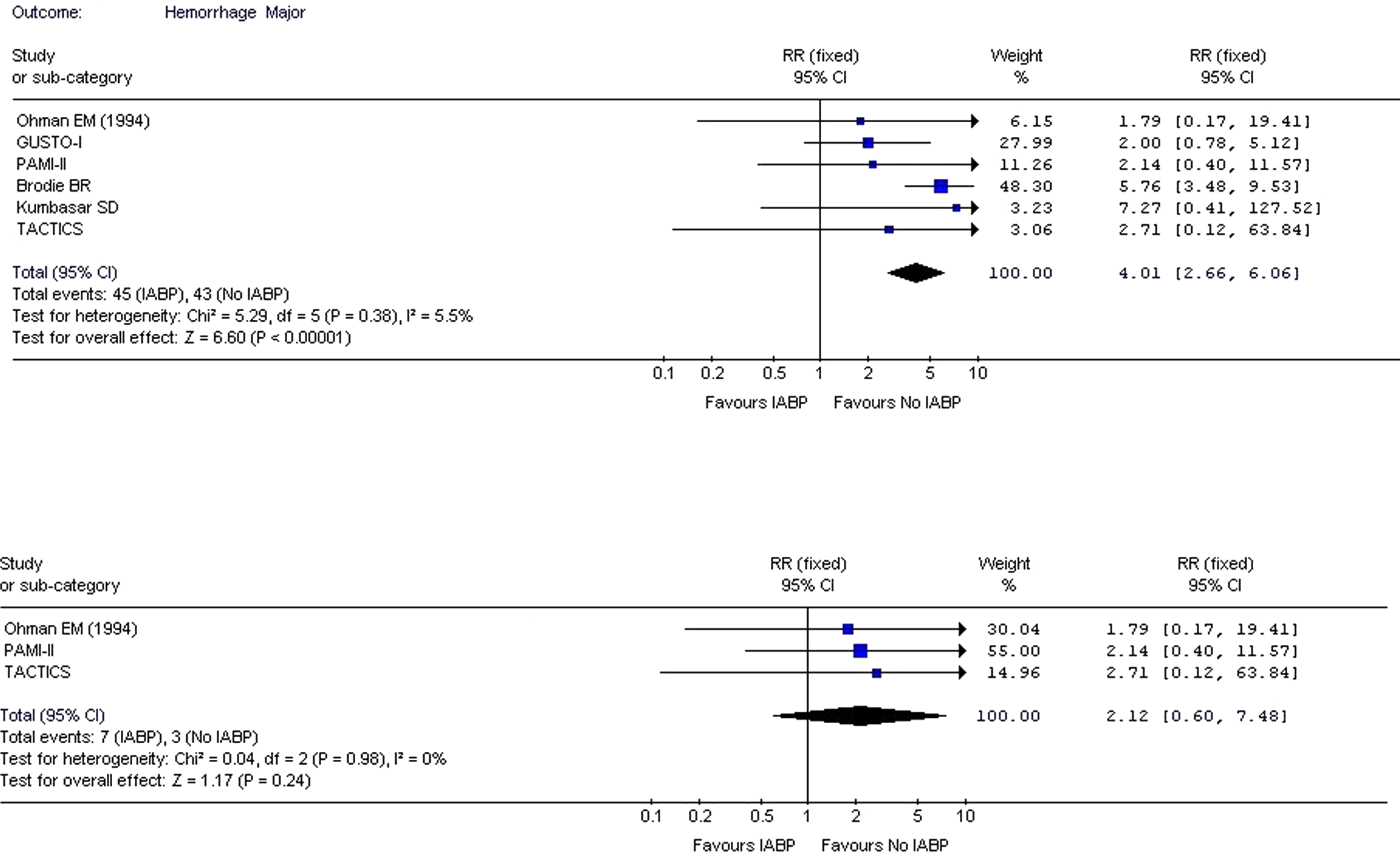
Seven trials14–17,22,23,27 provided data on moderate and major bleeding complications with IABP. The overall risk of moderate and major bleeding was found to be elevated when IABP was used (Figures 7 and 8 ). Intra-aortic balloon pump was found to significantly increase the risk of moderate bleeding (RR: 1.71; CI: 1.03-2.85; P = .04; Figure 7 upper panel)14–17,23,27 and major bleeding (RR: 4.01; CI: 2.66-6.06; P < .0001; Figure 8 upper panel).14–16,22,23,27When analysis was performed using only randomized controlled trials,14–17 the risk of moderate and major bleeding remained high (RR: 1.34; CI: 1.05-1.73; P = .02; Figure 7 lower panel) and (RR: 2.12; CI: 0.60-7.48; P = .24; Figure 8 lower panel), respectively, in the IABP group.
Discussion
Intra-aortic balloon pump is a circulatory-assist device that helps to increase cardiac output by decreasing systolic arterial pressure and increasing diastolic arterial pressure, thereby reducing the myocardial oxygen demand and subsequently myocardial ischemia. 38 However, the effect of IABP on cardiac output is modest. 39 It has been also shown to reduce afterload and increase proximal coronary blood flow velocity, reducing myocardial oxygen demand in hypotensive patients. 40 Magnetic resonance imaging studies of canine models have shown that the use of IABP after reperfusion can help reduce the extent of no-reflow phenomenon and improve the functional recovery of stunned myocardium.41,42 Augmentation of diastolic pressure by IABP has been shown to enhance the onset of coronary artery reperfusion after thrombolytic therapy 43 as well as to improve the late patency of the occluded coronary artery in patients with early failure of thrombolytic therapy. 44
Intra-aortic balloon pump use is widely accepted in the management of patients with cardiogenic shock. In addition, it is also used in situations such as hemodynamic support during angioplasty, post-MI refractory angina, and mechanical complications of AMI. 45 The role of IABP support in management of high-risk patients with AMI remains controversial.
The results of our analysis suggest that there is no benefit in terms of in-hospital mortality, rate of reinfarction, and recurrent ischemia when IABP is used in patients with AMI. In fact, the use of IABP has been shown to increase the rate of moderate-to-severe bleeding. Similar results were observed when the analysis was restricted to only randomized controlled trials.
When a subanalysis was performed including only those studies that evaluated the use of IABP in high-risk patients with AMI, the in-hospital mortality did not improve. Although the outcome appears to favor no use of IABP, the result is not significant. Studies by Flaherty et al, 13 Ohman et al (1991), 24 Stone et al (PAMI II investigators), 16 and Vijayalakshmi et al 19 failed to show any benefit of using IABP in high-risk patients with AMI. Stone et al 14 mentioned that the population included in their study was older and had more triple vessel disease than Ohman et al 16 which is the only study that showed benefits of using IABP. In the study by Flaherty et al, 13 the IABP failed to show improvement in myocardial perfusion, overall left ventricular function, and clinical outcomes including, early mortality, and prevention of infarct expansion. Although the study done by Ohman et al (1994) 16 showed improved in-hospital mortality with the use of IABP, the event rate and sample size was smaller when compared to the earlier study by Ohman et al (1991). 24 Studies done by Kumbasar et al, 22 Brodie et al, 23 and O’Rourke et al 17 were not considered in this subanalysis as they did not exclude patients with cardiogenic shock.
Analysis of studies restricted to patients with AMI complicated with cardiogenic shock revealed significantly decreased RR of in-hospital mortality in patients with IABP use. These results are in accordance with all the studies included in this subanalysis. Despite the fact that thrombolytic therapy has been shown to limit infarct size and decrease mortality, it failed to show benefit in the treatment of patients with AMI with cardiogenic shock. Elevated left ventricular end-diastolic pressure in combination with low perfusion pressure in cardiogenic shock prevent coronary reperfusion in such patients despite restoration of infarct artery patency. 46 Studies in canine models have shown that the use of IABP in combination with thrombolytics appears to have synergistic effect by unloading the left ventricle and increasing aortic diastolic pressure, thereby increasing the rates of coronary thrombolysis. 47 All the studies considered in our analysis had used thrombolytics and revascularization therapy such as PTCA or CABG.
Barron et al 25 also observed that the use of IABP was not associated with a reduction of mortality in patients who are treated with primary PTCA. In fact, it was associated with higher in-hospital mortality rates (OR: 1.26; 95% CI: 1.07-1.50). This was explained by the more intensive medical treatment in patients treated with IABP and thrombolytic therapy. Waksman et al 18 found similar survival rates in IABP patients with early revascularization and IABP patients with no or delayed revascularization. Similarly the SHOCK trial 28 comparing the emergency revascularization versus medical management with thrombolytics in patients with AMI and cardiogenic shock did not show significant overall benefit of early revascularization at 30 days. One of the possible explanations given was lower than expected mortality in initial medical stabilization arm. However, follow-up results from this study showed a lower mortality from all causes at 6 months, 1 year, and long term.43,48 Thus, the reason for no benefit in terms of in-hospital mortality using IABP in patients treated with primary PTCA is not very clear.
Nevertheless, the results from our analysis support the findings of previous studies that show benefit of using IABP in addition to thrombolytics in the treatment of patients with AMI complicated by cardiogenic shock.
Despite the development of sheathless catheter insertion techniques, development of smaller diameter catheters, and other technological advances, the use of IABP has a high rate of complications. Results of our analysis show significantly increased incidence of severe bleeding with the use of IABP. A prospective evaluation of catheter-related complications by Patel et al 7 found that both the sheathless insertion and smaller size catheters are associated with a higher complication rate. Their study also revealed female gender, peripheral vascular disease (PVD), cardiac index, and diabetes are independent predictors of risk of catheter-related complications. Similarly results from the Benchmark registry revealed that in addition to female gender and PVD, factors like body surface area (<1.65 m2) and age (>75 years) are the independent predictors of serious IABP complications. 6
All the studies included in our analysis except the one by Brodie et al 23 have adjusted for most of these factors. The study by Brodie et al 23 had patients with IABP who were older and more often women. Moreover, they used larger French sheaths with longer sheath time and high heparin dose. So we performed an analysis excluding this study. The risk of moderate (RR: 1.81; CI: 0.97-3.36; P = .06) and severe bleeding (RR: 2.38; CI: 1.14-4.95; P = .02) remained high in IABP group.
Our findings indicate a more conservative strategy for use of IABP in patients with AMI. The fact that there was no benefit in moderately hypotensive patients (systolic blood pressure [SBP] 90-100 mm Hg) but mortality reduction was seen in those with SBP < 90 mm Hg indicates benefit in sicker patients and calls for more judicious use of IABP. This conclusion is particularly relevant in the current era of advanced PCI and modern antiplatelet therapy, reserving IABP insertion for a particular group of the sicker patients with cardiogenic shock.
A careful interpretation of meta-analysis results is advised since it is based on the combined analysis of randomized control trials, prospective and retrospective observational studies which have different study designs, and prone to inherent biases. But the analysis of available randomized controlled trials also showed similar results. Although the current analysis provides a general overview of the risks and benefits of IABP use, the availability of a larger number of randomized-controlled trials would have provided more strength to the current analysis. Another limitation of this analysis is that studies did not adjust for body surface area which is an independent risk factor for IABP complications. 6 Also there exists a significant variation in terms of duration of IABP use from 48 hours to 11 days, and some of the studies did not mention the duration of IABP use. A general consensus on the timing of IABP insertion and duration of IABP treatment cannot be drawn from existing literature. A longer duration of IABP may increase the risk of bleeding and possible infection. Also in nonrandomized studies, obvious bias in the selection of patients was observed that may have confounded the results by putting higher-risk patients in the IABP group as compared to the control group. This bias was clearly evident in the SHOCK registry where the difference in mortality in the IABP group was no longer significant after adjustment for ventilator use and revascularization. Moreover, no uniform definitions of moderate and severe bleeding were found among the included studies. We did not attempt to reclassify the bleeding categories according to the current guidelines.
Conclusion
The present meta-analysis suggests that patients with high-risk AMI without cardiogenic shock do not seem to benefit from the use of IABP as measured by outcomes of in-hospital mortality, rate of reinfarction, and recurrent angina. However, in patients with AMI with cardiogenic shock (SBP < 90 mm Hg), there was a significant reduction in mortality with IABP use. The use of IABP increases the rate of both moderate and severe bleeding.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.