
Abstract
Inotropes are an integral component of the early stabilization of the patient presenting with cardiogenic shock. Despite years of clinical experience with the 2 most commonly used inotropes, dobutamine and milrinone, there remains limited data comparing outcomes between the two. We conducted a retrospective review to compare the effectiveness and safety of milrinone or dobutamine for the initial management of cardiogenic shock. Adult patients with cardiogenic shock regardless of etiology who received initial inotrope therapy with either milrinone (n = 50) or dobutamine (n = 50) and did not receive mechanical circulatory support were included. The primary end point was the time to resolution of cardiogenic shock. Changes in hemodynamic parameters from baseline and adverse events were also assessed. Resolution of shock was achieved in similar numbers in both the groups (milrinone 76% vs dobutamine 70%, P = .50). The median time to resolution of shock was 24 hours in both groups (P = .75). There were no differences in hemodynamic changes during inotrope therapy, although dobutamine trended toward a greater increase in cardiac index. Arrhythmias were more common in patients treated with dobutamine than milrinone, respectively (62.9% vs 32.8%, P < .01), whereas hypotension occurred to a similar extent in both groups (milrinone 49.2% vs dobutamine 40.3%, P = .32). The use of concomitant vasoactive medications, dosage required, and duration of therapy did not differ between groups. There was no difference in the overall rate of discontinuation due to adverse event; however, milrinone was more commonly discontinued due to hypotension (13.1% vs 0%, P < .01) and dobutamine was more commonly discontinued due to arrhythmia (0% vs 11.3%, P < .01). Milrinone and dobutamine demonstrated similar effectiveness and safety profiles but with differences in adverse events. The choice of milrinone or dobutamine as initial inotrope therapy for cardiogenic shock may depend more on tolerability of adverse events.
Introduction
Cardiogenic shock (CS) is characterized by systemic hypoperfusion and end-organ dysfunction resulting from cardiac pump failure. Early correction of hemodynamic abnormalities may prevent the development of multisystem organ failure and reduce mortality. 1 Despite advances in pharmacological and mechanical circulatory support (MCS), in-hospital mortality remains as high as 40%. 1 -3 Therefore, further clinical data comparing different therapies for CS is still necessary.
The acute management of CS often necessitates the use of inotropic therapy in order to improve cardiac output and restore tissue perfusion. 1 Norepinephrine is the vasopressor of choice in CS based on fewer arrhythmic complications and reduced mortality when compared to dopamine, yet observational data suggest that the addition of an inodilator (a positive inotrope that also reduces afterload) may improve survival. 4,5 Milrinone and dobutamine are the most commonly prescribed inodilators, but they possess distinct pharmacodynamic and pharmacokinetic profiles potentially leading to discordant outcomes. 6
Limited data exist comparing efficacy and safety between milrinone and dobutamine in CS, despite decades of clinical experience with the individual agents. Studies comparing the 2 agents in patients with acute heart failure (AHF) and CS found similar increases in cardiac index (CI), yet no difference in the incidence of adverse events or in-hospital outcomes. 7 -9 Two studies prospectively comparing milrinone and dobutamine in patients with CS following cardiac surgery found divergent effects on the CI, one of which also found that dobutamine was associated with a significantly greater incidence of atrial fibrillation (AF). Neither study reported on clinical outcomes between groups and the duration of follow-up was limited to 4 hours or less. 10,11 Accordingly, major guidelines do not offer firm guidance on which inotrope is preferred for the initial management of CS, 12 -14 and a 2014 Cochrane review of inotropic agents for myocardial infarction (MI) complicated by CS identified a lack of data comparing the different agents. 15 Clinicians routinely prescribe inotropic therapy for CS based on hemodynamics and adverse effect profile, but it is not clear what effect this has on clinical outcomes. We therefore conducted this retrospective review to compare the safety and efficacy of milrinone or dobutamine as the initial inotrope for the treatment of CS.
Materials and Methods
Study Design
We performed a single-center, retrospective chart review of patients receiving milrinone or dobutamine as initial inotrope therapy for CS at NYU Langone Health, a 726-bed tertiary care academic hospital. Institutional review board approval was granted, and a waiver of informed consent was obtained. Patients admitted between January 1, 2013, and February 28, 2015, who received inotrope therapy with either milrinone or dobutamine were identified by a medication use report. All adult patients age greater than 18 who received milrinone or dobutamine as initial inotrope therapy for CS were included. Cardiogenic shock was defined as: (1) hypotension or continuous infusion of at least one vasopressor, (2) evidence of cardiac dysfunction on a pulmonary artery catheter or echocardiography, and (3) signs of systemic hypoperfusion (Figure 1). 14 Patients were excluded if they had no hemodynamic evidence of CS, the presence of a ventricular assist device or intra-aortic balloon pump (IABP), concomitant milrinone and dobutamine therapy at initiation, CS of a mixed or noncardiac origin, or cardiac arrest prior to initiation of inotrope therapy.

Definition of cardiogenic shock. 14 LV indicates left ventricle; MAP, mean arterial pressure; RV, right ventricle; SBP, systolic blood pressure; SvO2, mixed venous oxygen saturation.
Data Collection
Data collection points included baseline patient demographics, the etiology of CS, baseline Acute Physiology and Chronic Health Evaluation (APACHE) II score, daily Sequential Organ Failure Assessment (SOFA) score, hemodynamic data (heart rate [HR], heart rhythm, mean arterial pressure [MAP], and CI), echocardiography studies, laboratory data (mixed venous oxygen saturation [SvO2], serum lactate, serum creatinine, liver transaminases, and platelets), urine output, and dose of all vasoactive and antiarrhythmic agents (inotropes, vasopressors, diuretics, pulmonary vasodilators, β-blockers, calcium-channel blockers, amiodarone, digoxin, propofol, and dexmedetomidine). All data were collected from the electronic health record. Hemodynamic data and doses of inotropes and vasopressors were collected hourly, if charted that frequently, and used to calculate a daily median.
Objectives
Our primary objective was to compare the time to resolution of CS in patients who received milrinone versus dobutamine as initial inotrope therapy. Resolution of CS was defined as (1) CI > 2.2 L/kg/min (if available), (2) SvO2 > 50% and serum lactate < 2 mmol/L, and (3) resolution of hypotension or discontinuation of vasopressors. Secondary outcomes included time to inotrope failure, intensive care unit (ICU) and hospital length of stay (LOS), and mortality. Inotrope failure was defined as discontinuation of inotrope therapy due to ineffectiveness or adverse effects or switch to or addition of an alternative inotrope. Data evaluating the efficacy of the inotrope were collected until resolution or failure occurred. Safety data included adverse events (arrhythmias, hypotension, thrombocytopenia, liver enzyme elevations, and the need for renal dose adjustment) and the rate of discontinuation secondary to adverse events.
Statistical Analysis
Statistical analysis was performed using SPSS Statistics version 22 (IBM, Armonk, NY). Categorical variables are reported as frequencies and percentages and were compared using χ2 test or Fisher exact test. Continuous variables are reported as medians with interquartile range. Continuous variables were compared using the Mann-Whitney U test for nonparametric, nonnormally distributed data. A P value < .05 was considered statistically significant. Patients were consecutively screened for inclusion from a medication use report beginning January 1, 2013. Due to a limited number of medical patients who received inotropes, we first screened all patients from medical units for inclusion. Once all patients from medical units had been reviewed, we then screened patients from surgical services until a final sample size of 50 patients per inotrope was reached. We performed a post hoc analysis of efficacy and safety end points within the cardiac surgery subgroup because of the large number of patients included from this population. We were unable to perform a power analysis for our study because of an absence of prior data that utilized similar end points. A final sample size of 50 patients per inotrope was chosen arbitrarily to allow for a pilot analysis of the utility of the primary end point of resolution of CS. Efficacy analyses were performed only on patients who achieved resolution of CS (milrinone, n = 38; dobutamine, n = 35) to eliminate the impact of confounders on the primary outcome. The safety analysis included all patients who received either milrinone (n = 61) or dobutamine (n = 62) during the evaluation period. Patients who were on concomitant inotrope therapy or had switched to the alternative agent were included in the safety analysis, although they were excluded from the efficacy analysis to provide more robust safety data.
Results
Patient Characteristics
We consecutively screened 622 patients for inclusion (Figure 2). In total, 217 patients who received milrinone as initial inotrope therapy and 405 who received dobutamine were reviewed. The most common reason for exclusion in both groups was failure to meet hemodynamic criteria for CS (Figure 2). The median age of all included patients was 73.5 years, they were 51% male, and were primarily admitted to the cardiovascular surgery service (Table 1 and Supplemental Table S1). Median APACHE II score at the time of initiation of inotrope was 12 in the milrinone group and 12.5 in the dobutamine group. Baseline comorbidities and medications were similar between the 2 groups with the exception of a higher incidence of prior cerebrovascular accidents in the milrinone group (Table 1 and Supplemental Table S2). Median ejection fraction at baseline was relatively normal in both groups due to the large number of cardiac surgery patients included who had preoperative echocardiograms that preceded the CS event (Table 1). The median dose of inotrope at initiation was 0.25 and 2.5 µg/kg/min for milrinone and dobutamine, respectively (Supplemental Table S5). The majority of patients in both groups were admitted for cardiac surgery (Supplemental Table S1). However, patients receiving milrinone were more likely to be admitted for heart valve surgery than those receiving dobutamine (62% vs 40%, P = .03), whereas patients receiving dobutamine were more likely to be admitted for acute decompensated heart failure (ADHF) than those receiving milrinone (20% vs 4%, P = .03). There were also differences seen in the etiology for CS (Table 1). Cardiac surgery with cardiopulmonary bypass was more common in the milrinone group than the dobutamine group (80% vs 62%, P = .05), whereas ADHF was more common in patients receiving dobutamine than milrinone, respectively (28% vs 8%, P = .02).

Inclusion and exclusion.
Baseline Patient Characteristics.a

Abbreviations: ADHF, acute decompensated heart failure; APACHE, acute Physiology And Chronic Health Evaluation; MI, myocardial infarction; NYHA, New York Heart Association.
a All data reported as median (interquartile range), unless otherwise specified.
Clinical Outcomes
Resolution of CS was achieved with the initial inotrope in 38 patients in the milrinone group and 35 in the dobutamine group (P = .50; Table 2). The median time to resolution of shock was 24 hours in both groups (P = .75). Additionally, we did not find a difference in time to correction of specific hemodynamic variables (Table 2). The dose of inotrope at resolution of shock, although not directly comparable, was similar between the 2 groups (Table 2).
Clinical Outcomes.a
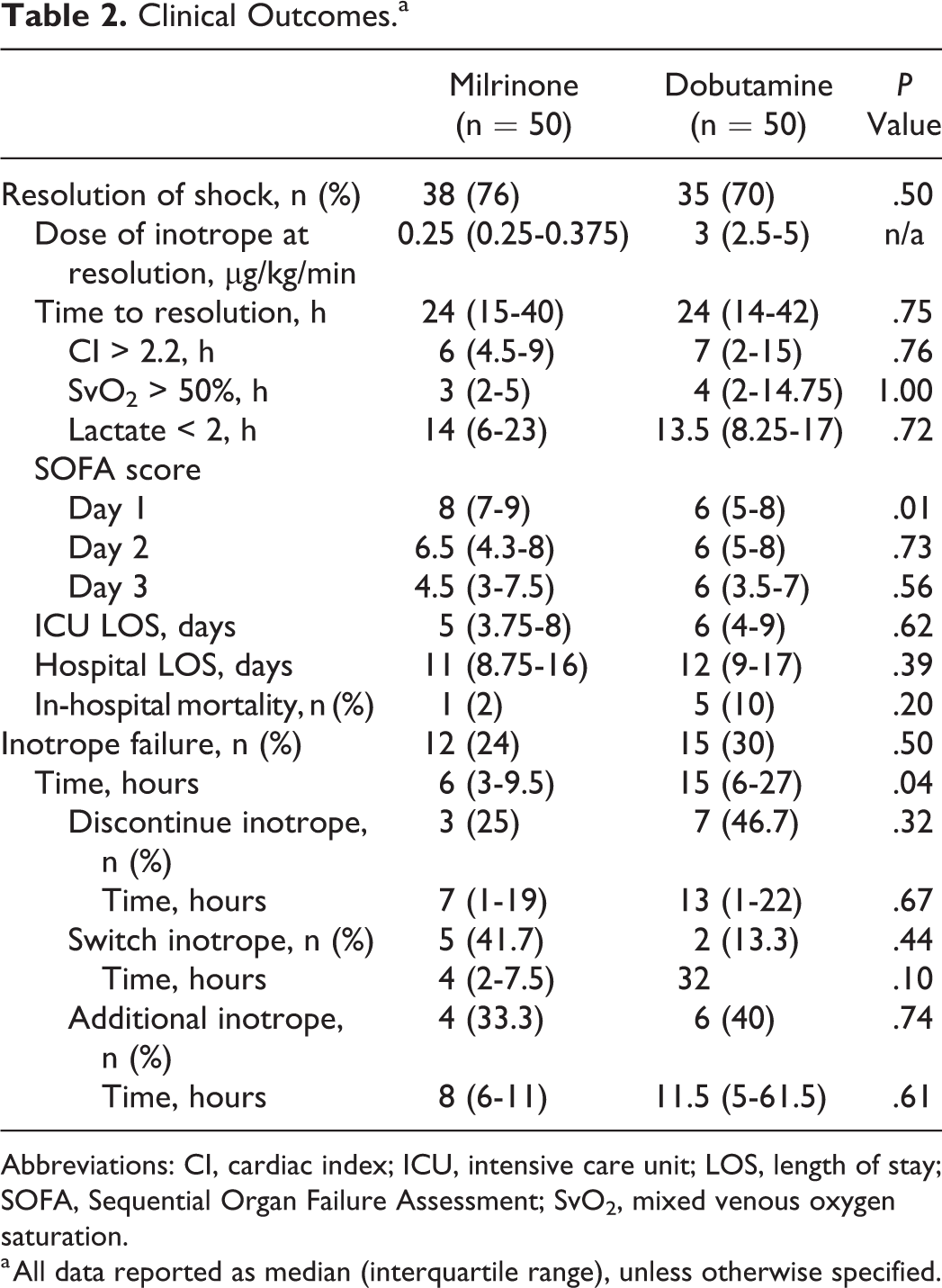
Abbreviations: CI, cardiac index; ICU, intensive care unit; LOS, length of stay; SOFA, Sequential Organ Failure Assessment; SvO2, mixed venous oxygen saturation.
a All data reported as median (interquartile range), unless otherwise specified.
Inotrope failure occurred in 12 patients in the milrinone group and 15 patients in the dobutamine group (P = .50). There were no differences in the reasons for inotrope failure between the 2 groups (Table 2). Overall, time to inotrope failure was significantly shorter in the milrinone group versus the dobutamine group (6 vs 15 hours, P = .04).
The median SOFA score on day 1 of inotrope therapy was significantly higher in patients who received milrinone but were similar on day 2 and day 3 of inotrope therapy (Table 2). Length of ICU and hospital stay were similar between the groups (Table 2). There was no difference observed in in-hospital mortality (Table 2).
Hemodynamics
The median hemodynamic trends over the first 3 days of inotrope therapy in patients who achieved resolution are shown in Tables 3 and Supplemental Table S4. Median values and percentage change from baseline were compared between groups for each day of therapy. Median CI was lower in the dobutamine group at baseline but was consistently higher in the dobutamine group over the course of therapy, with the largest difference being recorded on day 2 (Table 3 and Supplemental Table S4). The percentage change in CI from baseline trended toward statistical significance in the dobutamine group (Table 3). Median HR and MAP for each day of therapy were similar when compared between the groups.
Percent Change in Daily Median Hemodynamics.a
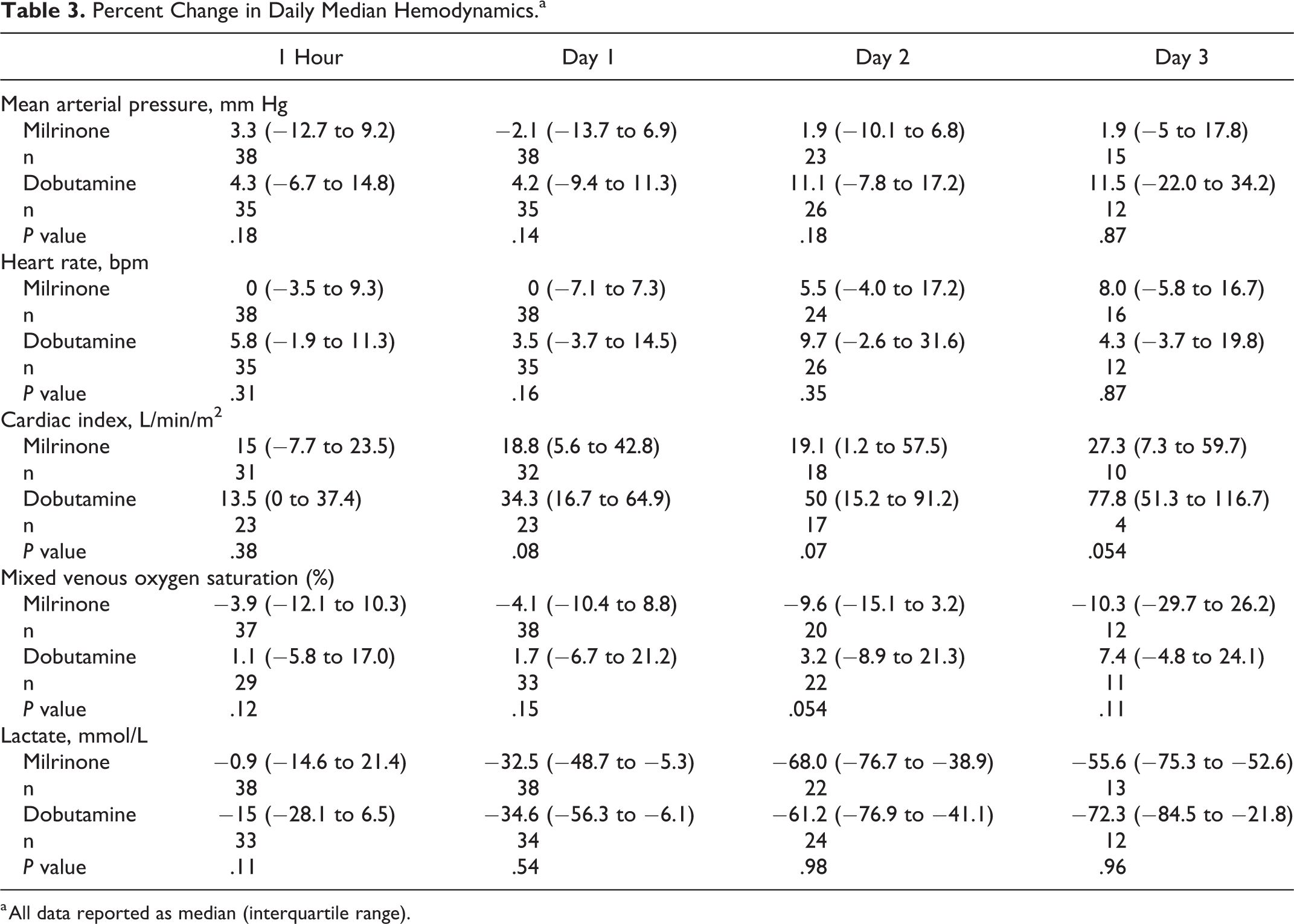
a All data reported as median (interquartile range).
Vasoactive Medications
The use of concomitant vasoactive medications was collected over the duration of inotrope therapy (Supplemental Table S5). There was no significant difference in the utilization of concomitant vasopressors or the maximum and median dose infused. Calcium channel blockers (CCB) were used more frequently with milrinone, but when used the median duration of overlap was similar in each group. Diltiazem and nicardipine continuous infusions were the most commonly used CCB.
Safety
Safety data were evaluated in all patients who received milrinone (n = 61) or dobutamine (n = 62) at any time during the evaluation period regardless of initial inotrope (Table 4). The rate of arrhythmia was significantly higher in those receiving dobutamine compared to milrinone (62.9% vs 32.8%, P < .01). The difference in arrhythmia was primarily driven by a significant difference in sinus tachycardia. The incidence of AF did not differ between the groups. Hypotension was common with both inotropes. There was no difference between the nadir systolic blood pressure or MAP between groups. However, patients receiving milrinone became hypotensive significantly faster than those receiving dobutamine (3.5 vs 8 hours, P = .02). Acute kidney injury occurred more frequently in those receiving dobutamine than those receiving milrinone but did not reach statistical significance.
Safety Outcomes.
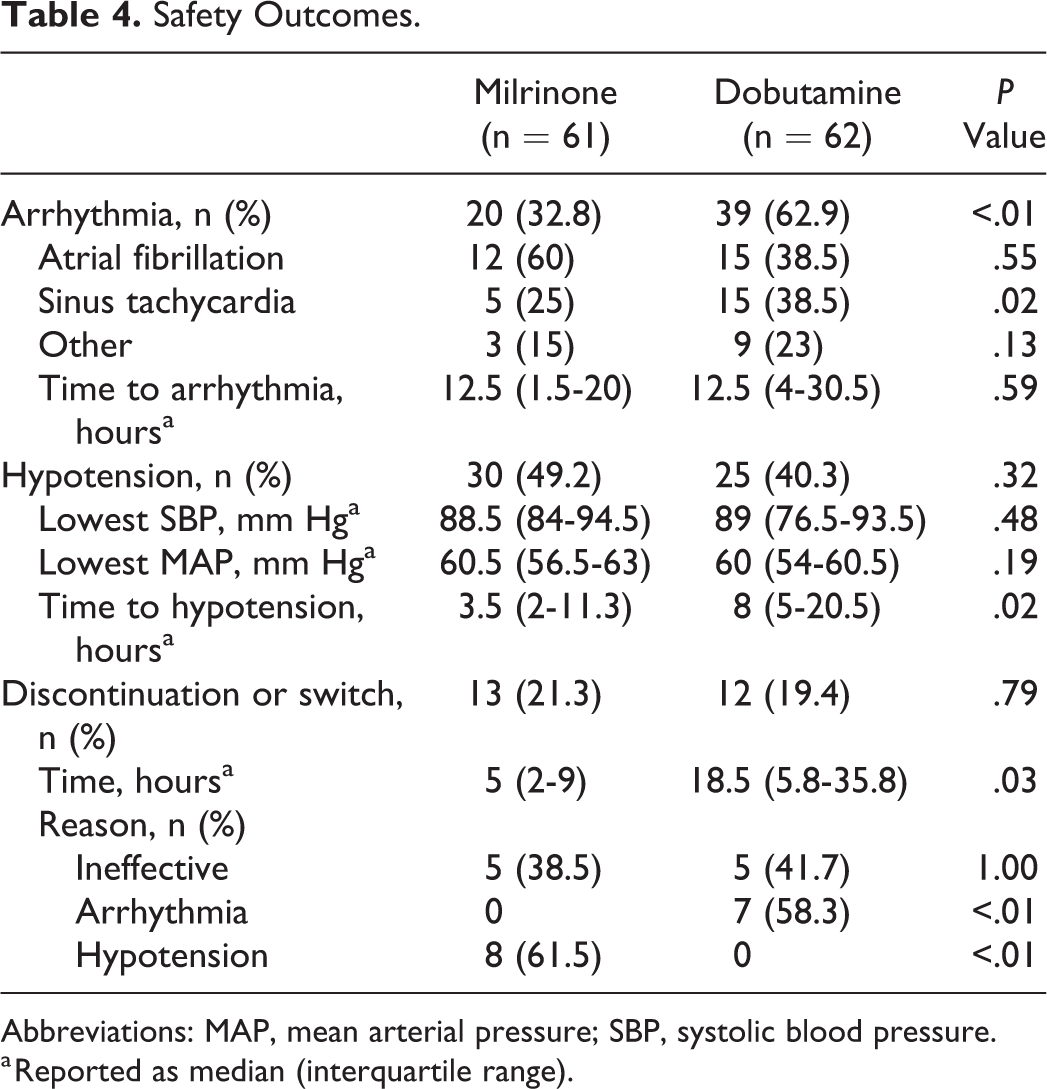
Abbreviations: MAP, mean arterial pressure; SBP, systolic blood pressure.
a Reported as median (interquartile range).
The incidence of discontinuation of inotrope therapy or switch to alternative inotrope therapy was similar between milrinone and dobutamine (21.3% vs 19.4%, P = .79). Milrinone was most commonly discontinued or changed due to hypotension, whereas dobutamine was most commonly discontinued or changed due to arrhythmia. Milrinone was discontinued or changed significantly faster than dobutamine (5 vs 18.5 hours, P = .03).
Cardiac Surgery Subgroup Analysis
Baseline characteristics, reason for admission, and prior-to-admission medications were similar between the 2 groups (data not included). There were no differences between groups with regard to the procedure details (cardiopulmonary bypass time or aortic cross clamp time). The median dose of inotrope at initiation was 0.25 or 2.5 µg/kg/min for milrinone or dobutamine, respectively. There was no difference at baseline in the use of vasopressors or doses administered.
Resolution of CS was achieved with the initial inotrope in 74% of patients in the milrinone group and 63% in the dobutamine group (P = .30). The median time to resolution of shock was 23 and 17 hours for milrinone and dobutamine, respectively (P = .15). There was no difference in time to correction of specific hemodynamic variables (Supplemental Table S6). The reasons for inotrope failure were similar between the 2 groups (Table S6). Time to inotrope failure was shorter in the milrinone group versus the dobutamine group (5 vs 14 hours, P = .12) but was not statistically significant. Daily SOFA score, ICU and hospital LOS, and in-hospital mortality additionally were similar between the groups (Supplemental Table S6).
Safety outcomes mirrored those in the total population with more arrhythmias in the dobutamine group than in the milrinone group (52% vs 29%, P = .02) but a similar incidence of hypotension (milrinone 45% vs dobutamine 32%, P = .19). Similarly, milrinone was discontinued more commonly due to hypotension (14% vs 0%, P = .01), whereas dobutamine was discontinued more commonly due to arrhythmia (16% vs 0%, P < .01) (Supplemental Table S7).
Discussion
Cardiogenic shock is the most extreme manifestation of a critical reduction in cardiac output. Ventricular dysfunction may be the result of many pathophysiological processes (eg, acute MI [AMI], AHF, postcardiotomy shock), but the end result if not urgently treated is multisystem organ failure and death. 1,2 Technological advances have led to an increase in the use of MCS; however, MCS has considerable complications including bleeding, thrombosis, device malfunction, and requires a skilled practitioner for implantation. 16 Medical therapy therefore remains the first-line treatment of CS.
Inotropic agents are an integral component of the initial treatment of CS. They can be further classified based on their effects on systemic vascular resistance (inopressors or inodilators), milrinone and dobutamine being the 2 inodilators approved for use in the United States. 17 Inodilators are of theoretical benefit in CS because, in addition to increasing chronotropy and inotropy, they also reduce afterload on the heart by decreasing systemic vascular resistance and reduce preload by decreasing ventricular filling pressures. Yet, milrinone and dobutamine have key pharmacological differences that suggest they may produce different outcomes, particularly in prespecified patient populations. Dobutamine may be preferred in patients with relative bradycardia or vasodilatory shock because of more chronotropy and less effects on systemic vascular resistance, whereas milrinone may benefit patients with pulmonary hypertension, diastolic dysfunction, or arrhythmias because of its reduction in pulmonary vascular resistance, positive lusitropy, and decreased arrhythmogenicity. 6,17 -19
To date, there are no large randomized controlled trials (RCT) comparing clinical outcomes between different inotrope strategies in CS. In fact, a Cochrane Review from as recently as 2014 identified zero RCTs evaluating outcomes between milrinone and dobutamine in patients with CS complicating AMI. 15 Two prospective, propensity-matched, observational analyses provided modest evidence of benefit of inodilators in CS. 5,20 Still, differences in outcomes between-individual inodilators were not directly compared. Several studies compared milrinone and dobutamine in prospective RCTs in other patient populations, but were limited by sample size and duration of follow-up. In a relatively small study, Aranda and colleagues randomized patients with inotrope-dependent heart failure to either milrinone or dobutamine. 7 They reported similar survival to transplantation and no difference in the requirement of additional inotrope or MCS. As in our study, they found comparable rates of crossover to the alternative inotrope, and the reason for crossover was hypotension or arrhythmia in all cases for milrinone or dobutamine, respectively. Karlsberg et al randomized patients presenting with new-onset heart failure following an MI to milrinone or dobutamine, but only for a 24-hour infusion. They found similar increases in CI but significantly greater reductions in MAP and mean pulmonary capillary wedge pressure (PCWP) in patients treated with milrinone, and more arrhythmias associated with dobutamine. 8 Yet, there were no differences in outcomes between the 2 groups, despite differences in hemodynamic end points and adverse effects.
In contrast to the previous two studies, the majority of the patients in our review presented with CS following cardiac surgery. Two studies compared the effects of milrinone and dobutamine in patients with CS following cardiac surgery, but they were also limited by duration of observation. Feneck and colleagues found that dobutamine was associated with significantly greater increases in CI and HR, and also a higher incidence of new-onset AF, but they only reported results over a 4-hour time period. 10 They initiated and titrated dobutamine to higher doses than was seen in our study, possibly explaining the increased efficacy and adverse events. Carmona et al found no differences in CI, HR, and MAP between milrinone and dobutamine. 11 However, they only evaluated hemodynamic parameters at 30 and 60 minutes after inotrope initiation and they did not titrate the infusion. Though both studies provided excellent hemodynamic comparison between milrinone and dobutamine, neither study reported on clinical outcomes in patients with CS following cardiac surgery. The results of the prior studies suggest that longer follow-up and a primary end point more reflective of clinical outcomes is necessary to provide further comparison of milrinone and dobutamine. To this end, we performed a post hoc analysis of patients who underwent cardiac surgery. Outcomes overall were similar in this subgroup as in the total population. Although resolution of shock was 6 hours faster in the dobutamine group, this did not reach statistical significance.
Our retrospective analysis is the first to compare time to resolution of shock in a broad population of patients with CS treated with milrinone or dobutamine. Resolution of shock and restoration of organ perfusion is critical to survival in CS. 1 Vasopressor requirement and persistent hypotension despite vasopressor support are independent predictors of in-hospital mortality in CS complicating AMI. 21 Additionally, lactate clearance over the first 12 hours of CS portends a higher likelihood of survival, and a lower SvO2 identifies patients with persistent tissue dysoxia and worse survival. 22,23 We thus feel that our primary end point of resolution of shock, which incorporates all of these variables, provides a more accurate surrogate of prognosis than CI or PCWP alone as used in previous trials. 7,9 To this end, we found no difference in the time to resolution of shock between milrinone and dobutamine. Furthermore, we evaluated hemodynamic and clinical variables over 3 days providing a more complete picture of each patient’s clinical course. Dobutamine trended toward a greater increase in CI over the observation period, but there were no differences in hemodynamic variables, including HR and MAP, and there was no difference in the requirement for concomitant vasopressors. It may not be surprising then that we did not find a difference in clinical outcomes such as LOS and mortality because there was little difference in achievement of hemodynamic end points between groups.
In this regard, the adverse effects that arise as milrinone and dobutamine are titrated to achieve hemodynamic end points may be of more consequence. Despite its propensity to decrease systemic vascular resistance, milrinone was not associated with more hypotension or increased vasopressor requirements. However, hypotension was cited as the reason for discontinuation of milrinone therapy in 8 cases. Upon closer analysis of these 8 patients, we found that the nadir MAP at the time of inotrope discontinuation was similar to that of the population as a whole, but the decrease in MAP from the time of initiation of milrinone to the time of discontinuation was 11.5 mm Hg; moreover, the median time to discontinuation of milrinone due to hypotension was 3.5 hours. This suggests that patients who will not tolerate milrinone can be identified early and switched to alternative therapies. Dobutamine, conversely, was associated with significantly more arrhythmias ultimately leading to discontinuation of therapy in 7 patients. This is consistent with previous analyses and is a limiting factor of dobutamine therapy. 8,10 We observed significant differences in the time to change of inotrope therapy due to perceived failure or adverse event. The clinical significance of this observation is uncertain, but may again indicate bias or may be related to the natural history of the development of hypotension and arrhythmias.
Limitations
There are several limitations to our study. This was a retrospective analysis, which introduces numerous biases. We had unbalanced patient populations based on etiology of CS with more patients in the milrinone group undergoing cardiac surgery. Furthermore, because the majority of patients suffered from postcardiac surgery CS, many data points appear normal at baseline (ejection fraction, APACHE II) and are not reflective of the patients’ most critically ill state. Prescribers currently select inotrope therapy based on preference due to a lack of clear guidance and the majority of inotropes were initiated in the operating room. It is presumed that most patients were initially prescribed an inotrope with a favorable hemodynamic and adverse effect profile potentially introducing a selection bias. We did not, however, find any difference in hemodynamics between groups at initiation of inotrope therapy. Finally, although we couldn’t perform a power analysis, our sample is rather small and therefore subject to type 2 error.
Our results were also limited as an indirect result of our inclusion and exclusion criteria, in spite of our attempt to design a novel primary end point reflective of clinical outcomes. First, our population consisted primarily of patients undergoing elective cardiac surgery. The APACHE II scores were abnormally low for a population of patients with CS, but were collected prior to inotrope initiation and thus correlate to a noncritical preoperative state in the majority of patients. In contrast, the SOFA scores, which were collected over the course of inotrope therapy, more accurately reflect the acuity of illness after the onset of CS. The initial SOFA score of 8 in the milrinone group predicts a morality of approximately 33%, and the SOFA score was unchanged over the first 72 hours of therapy in the dobutamine group also predicting a poor prognosis. 24 Still, in-hospital mortality was relatively low, but it is not surprising that the majority of patients recovered given that patients with CS following elective cardiac surgery have significantly better survival rates compared to other etiologies of CS. 25 Second, we further limited the severity of illness of our population by excluding patients with an IABP or other form of MCS. It is common practice at our institution to use MCS in severe cases of CS, especially those presenting with AMI or AHF. The exclusion of these 2 patients groups that have higher baseline mortality rates mean our results may not apply to more critically ill patients.
Finally, we did not find a difference in the incidence of AF among our patient groups. This finding has several potential biases. The incidence of AF while receiving milrinone was lower than that reported in the baseline characteristics, while we saw a similar incidence of AF while receiving dobutamine as that reported at baseline. This is surprising because the majority of patients underwent cardiac surgery, a population with a high incidence of postoperative AF (POAF). 26 Milrinone patients did, however, receive significantly more CCB therapy, and trended toward more β-blocker and amiodarone therapy. These observations suggest that milrinone and dobutamine did not lead to increases in the incidence of AF, but treatment with milrinone allowed for the use of additional medications to better control AF. Additionally, we did not collect race as part of our baseline characteristics and recent data has suggested that African-Americans are at an increased risk of developing POAF while on inotrope therapy when compared to Caucasian patients. 27 Future studies should collect race as this too may influence inotrope choice.
Conclusion
In our retrospective analysis of initial inotrope therapy in patients with CS mostly postcardiac surgery, we did not find a difference between milrinone and dobutamine in the time to resolution of CS. In agreement with previous short-term hemodynamic studies, dobutamine was limited by the development of arrhythmias. However, in contrast to previous reports, milrinone was not associated with more hypotension or an increased need for concomitant vasopressors in the overall population. A subset of patients may not tolerate milrinone hemodynamically, but this intolerance generally presented early in therapy. Based on these findings, we feel that milrinone can be safely considered as an alternative initial inotrope for patients in CS, even in those with tenuous blood pressure. Future prospective trials comparing these 2 agents in patients for the treatment of CS are necessary to further delineate efficacy and tolerability and should focus on distinct subsets of patients with CS.
Supplemental Material
Supplemental Material, 18.07.11_Supplement_Inotropes_Manuscript_FINAL - Comparative Effectiveness and Safety Between Milrinone or Dobutamine as Initial Inotrope Therapy in Cardiogenic Shock
Supplemental Material, 18.07.11_Supplement_Inotropes_Manuscript_FINAL for Comparative Effectiveness and Safety Between Milrinone or Dobutamine as Initial Inotrope Therapy in Cardiogenic Shock by Tyler C. Lewis, Caitlin Aberle, Diana Altshuler, Greta L. Piper, and John Papadopoulos in Journal of Cardiovascular Pharmacology and Therapeutics
Footnotes
Authors’ Note
This article was presented in abstract form at the 45th Annual Society of Critical Care Medicine Congress, Orlando, FL, USA, February 20-24, 2016.
Author Contributions
T. C. Lewis contributed to conception and design, acquisition, analysis, and interpretation; drafted the manuscript; critically revised the manuscript; and agrees to be accountable for all aspects of work ensuring integrity and accuracy. C. Aberle, D. Altshuler, and J. Papadopoulos contributed to conception and design, analysis, and interpretation and critically revised the manuscript. G. L. Piper contributed to analysis and interpretation and critically revised the manuscript. All authors gave final approval to the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.