
Abstract
Background:
Limited data are available on the clinical management of atrial fibrillation (AF) and its outcomes from an Australian perspective.
Objective:
To describe the appropriateness of antithrombotic prescribing for patients who presented with a diagnosis of AF to the Hawkesbury St John of God Hospital, New South Wales, Australia.
Methods:
This retrospective observational study reviewed patients admitted to St John of God Hawkesbury Hospital with AF between June 2016 and June 2017. We calculated stroke risk using the CHA2DS2-VASc score based on medical records and reviewed the appropriateness of oral anticoagulant (OAC) prescribing compared to the 2016 European Society of Cardiology guidelines. Patients were excluded if they had only 1 episode of AF that reverted either spontaneously or upon cardioversion without any documented recurrences.
Results:
A total of 200 patients (18 years) were included, with 180 (90%) deemed eligible for anticoagulation. Of these 72.8% (n = 131) were prescribed an OAC. A total of 40.0% of patients at low risk of stroke and 68.4% at intermediate risk were prescribed an OAC, respectively. Apixaban was the direct OAC of choice with 36.6% of patients prescribed an OAC receiving apixaban. Warfarin was prescribed for 25.1% of the patients who were prescribed an OAC.
Conclusions:
The underutilization of anticoagulant medication in high-risk groups and over utilization in low-risk groups remains an ongoing issue in contemporary AF management, and it highlights the need to improve AF-related stroke prevention in our jurisdiction.
Introduction
Atrial fibrillation (AF) is the most common sustained cardiac rhythm disorder and is associated with reduced quality of life, functional status, cardiac performance, and overall survival. 1 The prevalence of AF increases with age, and it is the most common cause of stroke in the elderly individuals. 2 With an aging Australian population, AF is going to become increasingly prevalent in the future, making it an important health issue to monitor.
The contemporary management of AF is centered on symptomatic improvement, reduction in AF-related emergency department visits or hospitalizations, and reduction in morbidity and mortality, particularly the prevention of stroke and thromboembolism. Nonanticoagulated AF is associated with a 3- to 5-fold increased risk of stroke. These strokes are generally more severe (greater resource utilisation, long-term disability, and mortality) and more recurrent than non-AF strokes. 1 There is strong evidence supporting the efficacy of oral anticoagulant (OAC) in the prevention of AF-associated stroke and systemic thromboembolism. However, their value is limited by under prescription, 3 poor adherence, 4,5 and subtherapeutic dosing. 6
Simple, clinically applicable stroke risk-stratification schemes have been validated in large populations. 7 –9 The CHA2DS2-VASc score was first incorporated into the European Society of Cardiology (ESC) guidelines in 2010 and has simplified the initial decision for OAC in patients with AF. These guidelines recommend that patients without clinical stroke risk factors do not need antithrombotic therapy, while patients with stroke risk factors (ie, CHA2DS2-VASc score of 2 or more for men and 3 or more for women) are likely to benefit from OAC. 10 Oral anticoagulant therapy can prevent the majority of ischemic stroke in patients with AF, can prolong life, 10 –12 and is superior to no treatment or aspirin. 13,14 The net clinical benefit is almost universal, with the exception of patients at very low stroke risk, and OAC should therefore be used in most patients with AF. 10
As with stroke risk calculators, several bleeding risk scores have been developed, mainly in patients prescribed warfarin. The calculator most widely used is the HAS-BLED score. 15 Stroke and bleeding risk factors may overlap. For example, older age is one of the most important predictors of both ischemic stroke and bleeding in patients with AF. 16 A high bleeding risk score should generally not result in withholding OAC. Rather, bleeding risk factors should be identified, recognized, and treatable factors corrected. Balancing the risk of stroke versus the risk of bleeding is an ongoing dilemma for physicians.
Warfarin and other vitamin K antagonists (VKA) were the first anticoagulants used in AF. Vitamin K antagonists therapy reduced the risk of stroke by two-thirds and mortality by one-quarter compared to control (aspirin or no therapy). 11 The use of VKAs is limited by the narrow therapeutic interval, necessitating frequent monitoring and dose adjustments. Three direct oral anticoagulants (DOACs) (apixaban, rivaroxaban, and dabigatran) provide several advantages over warfarin, including their predictable pharmacokinetic profile allowing standardized dosing, no need for routine monitoring, and the incidence of interactions, particularly with food is decreased.
There are limited data on the use of anticoagulants in patients with AF in New South Wales. However, data from other Australian states have identified various levels of discordance between international guideline recommendations and actual prescribing patterns among patients with AF. Data from a recent study conducted in Tasmania estimated that only 54% of patients with AF who were eligible for anticoagulation actually received anticoagulants. 17 The most common reason that high-risk patients without any contraindications were not given OAC was “practitioners’ decision.” 18 Other barriers to the use of anticoagulants described in the literature are increasing age, increasing bleeding risk, previous bleeds, falls risk, comorbidities, and ability to comply with treatment. However, the considerable stroke risk without OAC often exceeds the bleeding risk on OAC, even in the elderly individuals, in patients with cognitive dysfunction, or in patients with frequent falls or frailty. 19 The bleeding risk associated with aspirin is not different to the bleeding risk on warfarin 20 or DOAC therapy 14 ; however, warfarin and DOACs effectively prevent strokes in patients with AF while aspirin does not. 11,14,20
There is currently limited data available regarding the characteristics, clinical management, and outcomes of patients with AF in Australia. The available data, however, correlates with data from international studies that suggest an underutilization of anticoagulant therapy. 21 The Commonwealth Review of Anticoagulation Therapies in AF in Australia identified that stroke prevention in individuals with AF requires improvement. A range of issues were highlighted, including the assessment of patients for stroke and bleeding risk, appropriate choice of antithrombotic agent(s) in patients with multiple comorbidities, and the monitoring of patient. 22 The review stressed the need for local data on which to base recommendations regarding the treatment of AF. This study was designed to contribute comprehensive data describing the outcomes of current stroke prevention strategies in a New South Wales–based hospital as suggested by the Commonwealth review. The aim of this study was to describe the appropriateness of antithrombotic prescribing for patients who presented with a diagnosis of AF to the Hawkesbury St John of God Hospital, New South Wales, Australia.
Methods
This was a retrospective observational study of medical records for patients admitted between June 2016 and June 2017. We included 200 patients aged ≥18 years admitted to the Hawkesbury St John of God Hospital with AF (both valvular and nonvalvular) as their primary (AF was the presenting complaint) or secondary condition (AF was listed as a current illness in the medical history or discharge summary). Patients were identified by the Medical Record Departments using codes I48.0 (Paroxysmal AF) to I48.9 (AF unspecified).
Data collected at baseline included patient demographics, medications on admission, documented previous medical history, relevant laboratory data (ie, estimated glomerular filtration rate [eGFR], international normalization ratio [INR], platelet count, etc.), discharge diagnosis, and discharge medications. From our data, patients were assigned a CHA2DS2-VASc score based on the 2016 ESC guidelines with a score of 0 warranting no therapy and a score of 2 or more in men and 3 or more in women warranting OAC therapy. HAS-BLED was the bleeding risk calculator of choice. An HAS-BLED score of 0 = low risk, 1-2 = moderate risk, and ≥3 = high risk. This allowed us to compare the anticoagulant prescriptions during admission to current guidelines. There have been a number of evidence-based guidelines created to aid clinicians in the management of patients with AF. 23 –26
Patients who presented with only 1 episode of AF that reverted spontaneously or by cardioversion were excluded, as stroke prophylaxis may not be warranted in these patients. We considered an index admission to be a patient’s first admission within our data collection period, with a diagnosis of AF that met the study’s inclusion criteria.
Contraindications (CIs) to OAC are often relative and subject to prescriber interpretation. There remain few consistent, absolute CIs to the use of OACs. We considered absolute CIs to be intracranial hemorrhage, end-stage liver disease, allergies to the specific anticoagulant, and breast-feeding or pregnancy in women. 27 We also considered relative CIs such as dementia, documented labile INR (for warfarin), medication interactions, and bleeding disorders. 27,28 While risk of falls is a strong factor influencing the decision for commencing anticoagulant therapy, 29 it was not included as a CI to antithrombotic therapy as many argue that it is not a valid CI and is also difficult to assess through retrospective data. Physician decision not to prescribe anticoagulant therapy was recorded and taken into account for our analysis. Specific contraindications for the new oral anticoagulants (DOACs) were identified using the Australian Medicines Handbook 2017.
Patients were divided into 4 groups based on the medication they were prescribed on discharge. The “no therapy” group received no antiplatelet or anticoagulant therapy. The “antiplatelet” group received aspirin, clopidogrel, prasugrel, dipyridamole, or ticagrelor either alone or in combination with one another but not in combination with an OAC. The “anticoagulant” group entailed those patients on either warfarin, apixaban, rivaroxaban or dabigatran. The “combination group” were patients receiving any antiplatelet plus any OAC therapy. Our examination of appropriateness of antithrombotic prescribing at discharge of the index admission was based on the 2016 ESC guidelines. We considered underutilization as nonprescribing of anticoagulation, with or without antiplatelet therapy, in patients without documented CIs to anticoagulant therapy and a CHA2DS2-VASc score ≥1 for men and ≥2 for women.
Ethics
This project received ethical approval from the Human Research Ethics Committee (St John of God Health Care) and was conducted in compliance with Institutional Review Board and Human Subjects Research Committee requirements.
Statistical Analyses
Categorical variables were summarized using frequencies and percentages, whereas numeric variables were summarized using the statistics n, mean, and standard deviation.
Comparisons between groups are made using independent t tests for numeric outcome variables and Pearson χ2 tests for categorical outcome variables. The P values for these tests are presented. Data were analyzed using SPSS version 25 (IBM). P values ≤ .05 were considered nominally significant without adjustment for multiple comparisons.
Results
The medical records of 230 patients were reviewed, of who 200 were included. Patients were excluded if they had only 1 episode of AF that reverted either spontaneously or upon cardioversion without any documented recurrence, had any CIs to OAC, or if they died during their admission.
The mean (standard deviation [SD]) age of the included patients was 72.4 (13) years, and 51.0% were male. Hypertension was the most commonly (59.0%) associated comorbid condition. The presentation reviewed was the first presentation of AF for 64.5% of patients. The demographics and clinical characteristics of the patients are summarized in Table 1.
Patient Demographics.

Abbreviations: AF, atrial fibrillation; BP, blood pressure; INR, international normalization ratio; SD, standard deviation; DVT, deep vein thrombosis; PE, Pulmonary embolus; TIA, Transient ischaemic attack.
The mean (SD) CHA2DS2-VASc score was 3.2 (1.8) with 80.5% of patients scoring ≥2. The majority (66.0%) of patients had an intermediate HAS-BLED score.
CHADS2 scores were documented for 5 (2.5%) of the 200 patients, and CHA2DS2-VASc scores were documented for 37 (18.5%) patients. Ten of the documented CHA2DS2-VASc scores were incorrect according to the 2016 ESC guidelines.
Based on the 2016 ESC guidelines, 90% (n = 180) of the 200 patients were eligible for OAC therapy (had a CHA2DS2-VASc score of ≥1). Of these, 72.8% (n = 131) were prescribed an OAC (an antiplatelet). An antiplatelet was prescribed alone to 12.2% (n = 22; Table 2). No OAC agent was prescribed for 31.5% (n = 6) and 26.7% (n = 43) of patients with a CHA2DS2-VASc = 1 and ≥2, respectively. There were 15 patients who had a documented reason for no therapy (Advanced Care Directives, falls risk, excessive alcohol intake, upcoming invasive procedure, and actively bleeding ulcers). This suggests that 18.9% (n = 34) of patients were on suboptimal therapy with no documented reasons. In contrast, 80.0% (n = 16) of patients with a CHA2DS2-VASc score of 0 received either an antiplatelet agent (40.0%) or an anticoagulant (40.0%).
Antithrombotic Changes During Admission for Patients With a CHA2DS2-VASc ≥1.
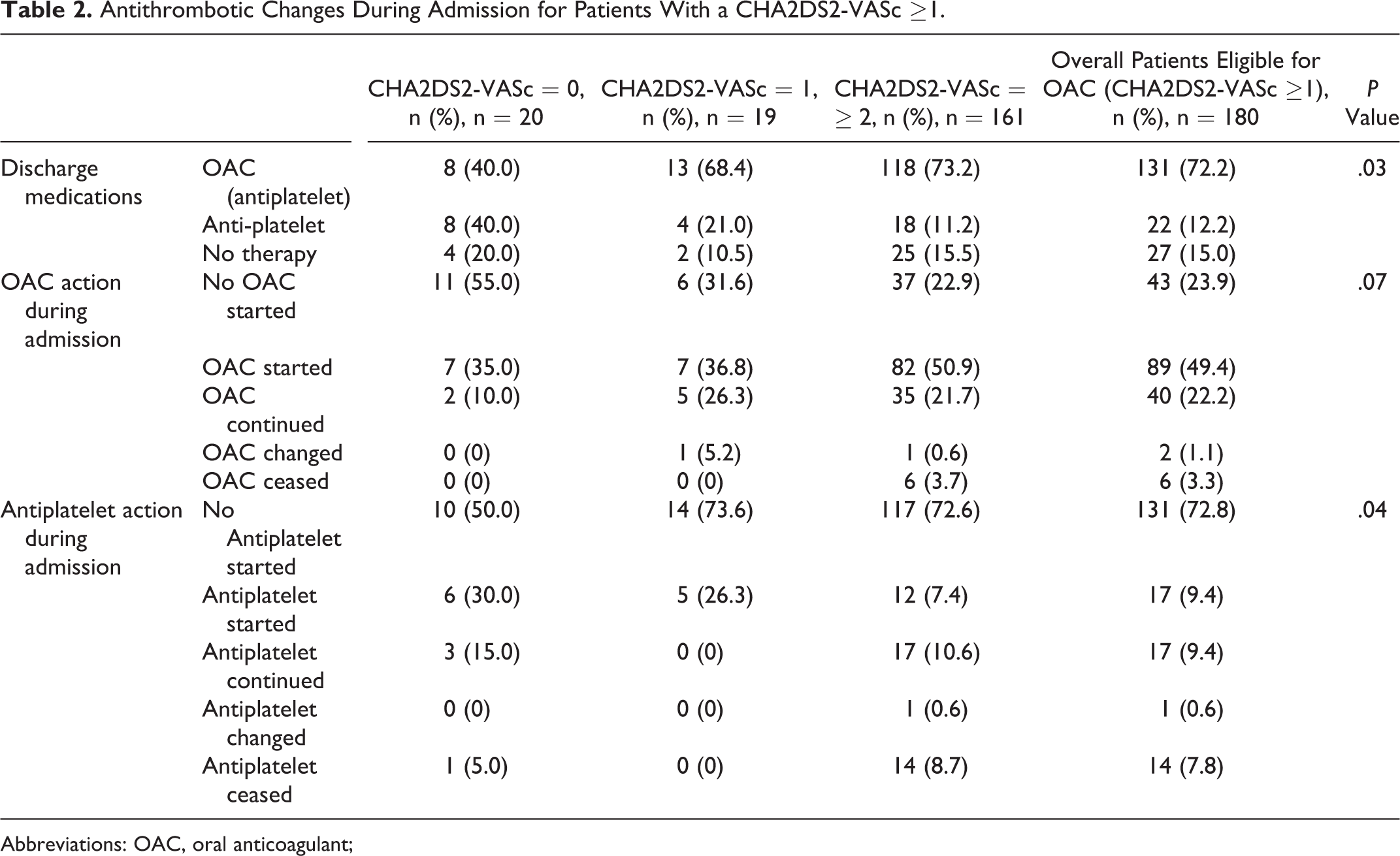
Abbreviations: OAC, oral anticoagulant;
There was an association between the type of discharge medication (including no treatment) and CHA2DS2-VASc score (P = .03; Table 2). The higher the CHA2DS2-VASc score, the more likely the patient received an OAC. A total of 68.4% (n = 13) patients with a CHA2DS2-VASc score of 1 and 73.2% (n = 118) with a CHA2DS2-VASc score of ≥ 2 received an OAC. A total 20.0% (n = 4) of patients with a CHA2DS2-VASc score of 0 received no therapy compared to 10.5% (n = 2) and 15.5% (n = 25) for a CHA2DS2-VASc score of 1 and ≥2 respectively.
The CHA2DS2-VASc score had an impact on whether an OAC was prescribed (P = .02; Table 3). The mean CHA2DS2-VASc score for no prescription was 2.7 (SD 1.9), while the mean CHA2DS2-VASc score for prescription of an OAC was 3.4 (SD 1.7). The HAS-BLED score did not appear to be associated with OAC prescribing (P = .44, Table 3).
Anticoagulation Prescription Based on CHA2DS2-VASc Score.
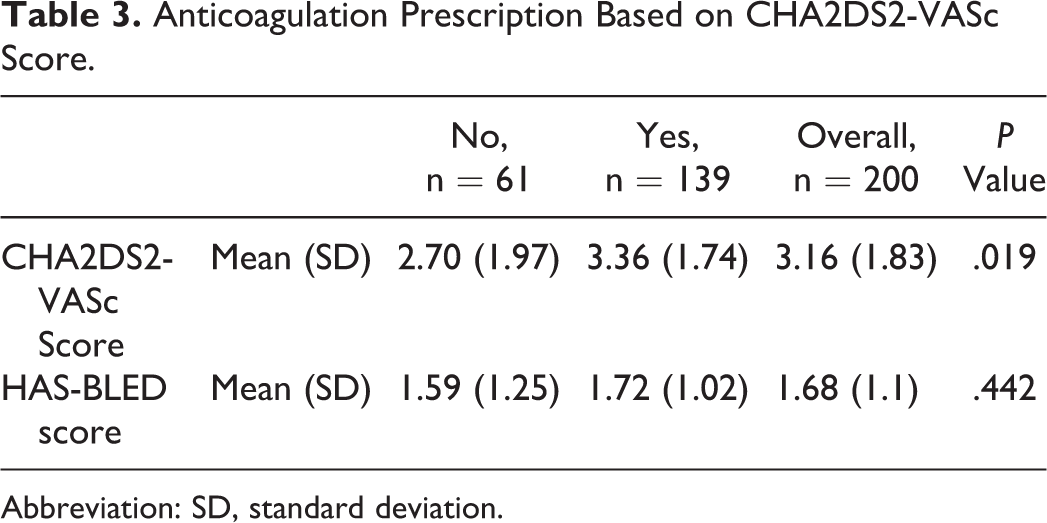
Abbreviation: SD, standard deviation.
Warfarin was the only anticoagulant that had a statistically significant relationship (P = <.0001) with eGFR (Table 5). A total of 66.6% of patients with an eGFR of 15 to 29 mL/min were prescribed warfarin, 8.3% were prescribed apixaban, and the remainder were not prescribed any OAC. A total 77.1% of patient on warfarin had an eGFR of >30 mL/min; 29.0% of these patients had valvular AF.
The mean INR for patients taking warfarin on admission was 3.3 (SD 1.7) with only 52.0% within the therapeutic INR range (Table 4). On discharge for patients taking warfarin, the mean INR was 2.4 (SD 0.6) with 68.6% within the therapeutic INR (Table 4).
INR Ranges for Patients Taking Warfarin.

Abbreviations: INR, international normalization ratio; SD, standard deviation.
Medications on Discharge by estimated Glomerular Filtration Rate (eGFR) (mL/min).

Apixaban was the DOAC of choice with 49.0% of patients prescribed a DOAC receiving apixaban, 26.9% receiving dabigatran, and 24.0% receiving rivaroxaban. Warfarin remained highly prescribed with 25.1% of patients prescribed an OAC receiving warfarin.
Discussion
Observational studies can be valuable in evaluating disease state management and its outcomes in a population. This study provides a snapshot of AF management patterns in a New South Wales hospital serviced by cardiologists who practice in multiple hospitals throughout the state. As such, we feel that it may represent the patterns across the state rather than the 1 hospital we reviewed. The lack of effective large-scale health-care data linkage systems within Australia makes these results even more relevant and should encourage similar reviews in the near future.
In our study, only 52.5% of patients taking warfarin were within the therapeutic range on admission. On discharge, this marginally increased to 68.6%. While this was just a snapshot of their time in therapeutic range, our findings were consistent with recent studies, which suggest that the time in therapeutic ranges for INR is suboptimal. 30,31 The benefits of DOACs’ predictable effects at a standardized dose without the need for regular monitoring should be a strong factor when deciding which OAC to treat patients with AF. The use of DOACs in clinical practice appears to be increasing rapidly. 32,33 A total of 74.8% of our eligible patients were on a DOAC compared to 25.1% on VKA, which is in accordance with recent guideline changes.
According to the ESC guidelines, 180 of 200 eligible patients were recommended to receive an OAC. 10 Of these, 27.2% (n = 49) were not anticoagulated, with only 15 having documented reasons for no therapy. This suggests that 18.9% (n = 34) of patients were on suboptimal therapy with no documented reasons. As this was a retrospective study, it is not possible to know what discussions occurred between the prescriber and the patient unless it was documented. Therefore, the overuse of OAC in low-risk patients may have been intentional, with the patients actually deciding they wanted to maximize their stroke prevention as much as possible. In contrast, as patients who are at higher risk of stroke are also at higher risk of bleeds, it may have been a mutual decision between the patient and the prescriber not to commence OAC. We relied on the documented information that may not have recorded such discussions, which may have an impact on understanding how the prescribing choices were made.
There are a number of studies suggesting that physicians struggle to balance the benefits of OAC in preventing a stroke and the risks of OAC in causing a major bleed. 34 One notion derived from qualitative research of physicians who do not prescribe OACs in high-risk individuals is that a stroke in an untreated patient is a consequence of the condition, whereas a major bleed from OAC is perceived to be the physicians fault. This perspective may help explain the undertreatment for high-risk patients.
There is strong evidence that patients with a CHA2DS2-VASc score of 2 or more in men and 3 or more in women will benefit from OAC therapy. Fortunately, we now have growing evidence base regarding stroke risk in patients with 1 clinical risk factor (ie, CHA2DS2-VASc score of 1 in men, and 2 for women), although this relies largely on observed stroke rates in patients not receiving OAC. 35 –37 It is now recommended that OAC should be considered for men with a CHA2DS2-VASc score of 1 and women with a score of 2, balancing the expected stroke reduction, bleeding risk, and patient preference. Importantly, age (65 years and older) conveys a relatively high and continuously increasing stroke risk that also potentiates other risk factors. While there is conclusive evidence for the “lower risk” (CHA2DS2-VASc of 0) and “higher risk” (CHA2DS2-VASc 2 for men and 3 for women), there remains some uncertainty around best management of the intermediate level of risk. An individualized weighing of risk, as well as patient preferences, should inform the decision to anticoagulate patients with 1 CHA2DS2-VASc risk factor, apart from female sex. Being female does not appear to increase stroke risk in the absence of other stroke risk factors. 38
The evidence supporting antiplatelet monotherapy for stroke prevention in AF is very limited. 10 Despite this, 15.0% (n = 30) in our study were discharged on antiplatelet monotherapy. This could be explained by comorbid conditions such as previous myocardial infarction; however, lack of documentation regarding prescribing decisions made this difficult to assess.
The CHA2DS2-VASc scores were documented for only 37 (18.5%) of our patients. The absence of this score could be a reason that many patients were not prescribed appropriate OAC. Based on the ESC guidelines, 10 of the documented CHA2DS2-VASc scores were incorrect, potentially leading to inappropriate antithrombotic prescribing.
The HAS-BLED score was not recorded for any of our patients. This may have significant implications on OAC prescribing. We know that bleeding is a major concern for practitioners when prescribing an anticoagulant. The considerable stroke risk without OAC often exceeds the bleeding risk on OAC, even in the elderly individuals, in patients with cognitive dysfunction or in patients with frequent falls or frailty. If practitioners are merely noting the risks but failing to assess them objectively, and thereby missing the opportunity to prescribe an OAC, then the patient might be an acceptable candidate for therapy, but stroke prevention therapy might be suboptimal.
The relationship between kidney function (eGFR) and OAC is important. Warfarin and apixaban were the only OACs prescribed to patients with an eGFR <30 mL/min. There was a strong inverse relationship for warfarin prescribing and reduced eGFR. In this instance, it is reasonable that warfarin is prescribed preferentially due to being eliminated by the liver rather than kidneys. Apixaban was not surprisingly the DOAC of choice in reduced renal function due to being only partially renally excreted. No other DOACs were prescribed when eGFR was <30 mL/min.
Understanding how care is delivered, especially through the application of guidelines and policies, can greatly impact patients OAC effectiveness. Assessing compliance with guidelines therapy can be an effective quality measure. One recommendation to improve adherence to guidelines would be to conduct quarterly review meetings with medical directors, prescribers, and staff to review individual site data. These meetings may promote discussion on variations in practice, comparison of prescribers and the sharing of best and most up-to-date practices for stroke prevention in patients with AF. In order to do this efficiently, a simple CHA2DS2-VASc scoring sheet for every AF admission could be implemented. This would ensure that the CHA2DS2-VASc score is considered, and the reasons for or against OAC are documented, allowing for future analyses and more accurate determination of adherence to guidelines. The introduction of this form would also allow pharmacists easier access to clinical information and prescriber choices. They could then review a patients’ file based on the CHA2DS2-VASc form and make recommendations to the prescriber. If a patient is found to have a low-risk CHA2DS2-VASc score and no other indication for OAC, the referring prescriber may be contacted and asked if they wish to continue or discontinue OAC therapy. The same principles can be applied for high-risk patients who are not prescribed an OAC.
Limitations
As data were collected retrospectively, the presence of missing or incomplete data was unavoidable. Specifically, we relied on documented comorbidities to calculate the CHA2DS2-VASc score. If a patient had incorrect/incomplete data recorded, we may have calculated the score incorrectly. However, this should not have influenced our results, as it can be assumed the clinicians were using the same clinical information to guide their management.
Patients were identified using codes I48.0 and I48.9; however, there might be some incorrectly coded patients who were not included in our analysis.
The size of our cohort was small; however, the demographic analyses shows consistencies with larger studies and represents the general population with AF presenting to the hospital.
Our study only included patients with AF who were hospitalized, meaning that they were potentially already at higher risk of AF-related stroke. This could limit the generalizability of our results to the broader Australian population, as many patients with AF are managed as outpatients.
Conclusion
We noted that despite the high risk of stroke and thromboembolic complications, OAC therapy remains underutilized in the high-risk groups and overutilized in the low-risk groups at St John of God Hawkesbury.
DOACs are becoming increasingly prevalent in the treatment of AF. Their role is likely to continue to grow as more data become available regarding their long-term use, drug interactions, and use in specific patient populations.
Warfarin therapy is an ongoing issue for patients with AF. Time in therapeutic INR range remains a challenge and appears to often be suboptimal on presentation to hospital. The benefits of DOACs in this regard should be a high consideration when prescribing a new OAC for AF.
Oral anticoagulant therapy should be patient centered; however, the prescriber has a duty of care to ensure the best advice is given. By establishing interventions such as those discussed earlier, individual institutions may be able to improve the quality use of OAC.
Footnotes
Author Contributions
Graeme Wertheimer contributed to conception and design, acquisition, analysis, and interpretation, drafted manuscript, critically revised manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy; Luke R. Bereznicki contributed to conception and design, interpretation, critically revised manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.