
Abstract
Objectives:
The main objective of this study was to evaluate treatment adherence to statin and health-related quality of life (QOL) in Lebanese patients with dyslipidemia. Secondary objectives were to examine associations between treatment adherence, QOL, treatment satisfaction, and illness perception.
Methods:
This cross-sectional study, conducted in 20 community pharmacies from all districts of Lebanon between August 2016 and April 2017, enrolled 247 adult patients taking any statin.
Results:
The mean age of the participants was 52.63 ± 11.92 years (57.5% males); the mean duration of treatment with a statin was 59.72 months. A significant association was found between adherence and marital status (P < .0001), educational level (P = .001), cigarette smoking (P < .0001), and alcohol drinking (P < .0001). A negative but significant correlation was found between the adherence score and the duration of dyslipidemia (r = −0.199). A significant but negative correlation was also found between the side effect score and age (r = −0.137). The monthly salary, the marital status, the educational level, smoking cigarettes or waterpipes, and drinking alcohol were all associated with the Illness Perception Questionnaire scores (P < 0.0001 for all variables). Secondary level of education (β = 13.43), smoking more than 3 waterpipes per week (β = 14.06), global satisfaction score (β = 0.32), convenience score (β = 0.29), and effectiveness score (β = 0.27) would significantly increase the adherence score. Smoking more than 15 cigarettes per day (β = −11.15) and a divorced status (β = −14.81) would however significantly decrease the adherence score. Significant associations were found between the illness perception score, the QOL domains, and the satisfaction domains (P < .05 for all variables).
Conclusion:
This study showed that global satisfaction with treatment, convenience, and effectiveness are important factors that increase treatment adherence. Patient adherence results in patient satisfaction and improved QOL and is an important criterion for achieving desired therapeutic outcomes.
Introduction
Dyslipidemia remains a principal risk factor for cardiovascular accidents/events, with the latter being the principal cause of morbidity and mortality in developed countries and account for 45% of all deaths in Lebanon. 1 A reduction of 0.6 mmol/L of serum total cholesterol in adults older than 60 years is correlated with a 27% decrease in the risk of fatal cardiovascular disease. 2 Because of their significant lowering of low-density lipoprotein cholesterol, statins gained a good reputation as the keystone in the treatment of dyslipidemia 3 and demonstrated marketability in reducing myocardial infarction (MI) and stroke 4 .
Medication adherence is defined by the World Health Organization (WHO) as “the degree to which the person’s behavior corresponds with the agreed recommendations from a health-care provider” (pp 381-390). 5 In real life, adherence to statins is often suboptimal, with many patients discontinuing the treatment, 6 with the all-cause mortality was positively associated with low adherence to statins 7 .
Multiple reasons can explain the lack of patients’ adherence to their prescribed medication regimens, including patient, prescriber, and health-care system factors. 8 An important step is the recognition of both the intentional and the unintentional aspects of nonadherence to medications. 9 Female gender, 10 demographics, 11 patient understanding and perception of medication, and sickness- and treatment-related factors 12 are factors correlated with adherence to medications.
The WHO defines the quality of life (QOL) as the perception of the individuals’ position in life taking into account culture and value systems in which they live and in relation to their expectations, goals, standards, and concerns. 13 The measurement of QOL is particularly relevant in the management of chronic diseases such as dyslipidemia, which are known to be associated with impaired QOL over extended periods. 14 Lalonde et al 15 have shown that patients with dyslipidemia have low QOL; this might be due to rigid dietary restrictions, side effects of medications, and the need for regular medical follow-up. 16
Not only can adherence affect QOL, but QOL may also impact medication adherence. 17 Although no studies examined the association between statin adherence and QOL among patients with dyslipidemia, this association is well documented in a variety of chronic diseases and various treatments. An improved health-related QOL was reported to be a trigger for nonadherence in participants with COPD. 17 Similarly, in patients having psoriasis, QOL impairment lowered treatment motivation. 18
Treatment satisfaction is a patient-reported outcome defined as the patient’s evaluation of the treatment received and its associated outcomes. 19 Treatment satisfaction affects adherence to medication, which in turn impacts the outcomes of treatment. 20 Patients’ lack of belief in medication effectiveness and a bad illness perception are commonly reported barriers to adherence to medications. Consequently, the absence of symptoms linked to an elevation in lipid level does not make the patient feel ill, and they may not realize the importance of lowering their lipid levels. 21 A good illness perception however is believed to increase adherence. 21
The primary objective of this study was to evaluate treatment adherence to statin and health-related QOL in Lebanese patients with dyslipidemia. Secondary objectives were to examine associations between treatment adherence, QOL, treatment satisfaction, and illness perception.
Methods
Study Design and Population
This cross-sectional study, conducted in all 5 districts of Lebanon, was done between August 2016 and April 2017. Our sample was constructed from 20 community pharmacies. A list of pharmacies was provided by the Lebanese Order of Pharmacists. Lebanese participants of both genders, aged 18 years and older, taking any statin were included in this study.
Sample Size Calculation
A sample of 229 patients was targeted to allow for adequate power for bivariable and multivariable analyses to be carried out according to the Epi info sample size calculations with a population size of 5 million in Lebanon, a 54.6% expected frequency of adherence to statins, 22 and a 5% confidence limits. 23 A total of 350 questionnaires were distributed to take refusals into account.
Data Collection
The detailed questionnaire was distributed to patients randomly by the pharmacist on duty in each pharmacy. The pharmacist approached every patient who came to the pharmacy to buy a statin medication, asking him whether he wants to participate in the study. After each pharmacist obtained the authorization from each patient via a written consent, he or she explained the study objectives to each patient. The survey was first tried on 20 patients to see whether the questions were well understood. This process did not lead to any modification in the survey’s questions.
Ethical Aspect
The study protocol was approved by the ethics committee of Saint-Joseph University of Beirut (reference number: USJ-2016-58).
Questionnaire
The self-administered anonymous questionnaire was in Arabic, the native language in Lebanon; it was composed of different sections: sociodemographic, social habits (smoking and alcohol consumption), duration of dyslipidemia, number of associated diseases, duration of statin’s treatment, and drugs associated with the prescribed statin. In addition, the WHOQOL short version (WHOQOL-BREF), Treatment Satisfaction Questionnaire for Medication (TSQM), and the Brief Illness Perception Questionnaire (brief IPQ) questionnaires were used.
Adherence assessment
The adherence to statins was assessed using an adaptation of Lu et al questionnaire 24 by asking the patients about the frequency, percentage, and rating response of their statin use during the last month. Concerning the frequency, we asked the patient “did you take all your medications all the time?” with the possible responses being divided as follow: 0% for none of the time, 20% for a little of the time, 40% for some of the time, 60% for a good bit of the time, 80% for most of the time, and 100% for all the time. The percent item was checked using the question “what percent of the time were you able to take your medications exactly as your doctor prescribed them?” The rating item was assessed using the following question “rate your ability to take all your medications as prescribed” with the possible answers being divided as follows: 0% = very poor, 20% = poor, 40% = fair, 60% = good, 80% = very good, and 100% = excellent. The total score was calculated by summing all 3 answers and presented in a percentage. 25 We calculated the reliability of each scale to assess the quality of our data. We obtained a good Cronbach α (0.776). Initially, the questionnaire of Lu et al was validated among patients with HIV and was later used in a population of patients attending general practice. 25
Quality of life measurement
We used the WHOQOL-BREF, a brief version of the WHOQOL-100. The WHOQOL-BREF questionnaire contains an item for overall QOL and an item for general health, in addition to 24 items divided into 4 domains: 7 items for the physical health domain, 6 items for the psychological health domain, 3 items for the social relationships, and 8 items for the environmental health. Each item is rated on a 5-point Likert-type scale. The raw domain scores obtained were transformed according to guidelines 26 to 4 to 20 scores, which were later transformed linearly on a 0 to 100 scale. 27 Higher scores indicate a better QOL and a better levels of functioning and well-being. The Cronbach α for this scale was excellent (0.915).
Brief Illness Perception Questionnaire
The Brief IPQ is a 9-item questionnaire assessing illness cognitive and emotional representations
28
with a response scale of 0 to 10. The Brief IBQ is divided into several items as follows: - 5 items assessing the cognitive representation of illness (consequences, timeline, personal control, treatment control, and identity) and - 2 items assessing the illness emotional representation (concern and emotions).
One item assesses illness comprehensibility; this item assesses the perceived cause of illness; respondents list the 3 most important causal factors of their illness. This item does not have a response scale and is only qualitative. The Cronbach α for this scale was 0.739.
Treatment Satisfaction Questionnaire for Medications
The TSQM version 1 is a 14-item questionnaire designed to assess treatment satisfaction. 29 The TSQM items’ answers are obtained using a 5- or 7-point Likert-type scale and consists of 4 domains (effectiveness; side effects; convenience, and global satisfaction), corresponding to separate facets of patient’s satisfaction with their current treatment. Each item score is on a 0 to 100 scale, and the total score is obtained for each domain by summing the corresponding items; higher values indicate higher satisfaction, better perceived effectiveness, better convenience, and lower perceived side effects. The Cronbach α for this scale was excellent (0.915).
Statistical Analysis
Questionnaire’s data were collected and processed by Statistical Package for the Social Sciences SPSS, version 23. Categorical variables were presented in frequencies and percentages, and continuous variables as means with standard deviations (SDs). Statistical analysis was conducted using chi-square, Fisher exact test, and analysis of variance (ANOVA). Analysis of variance and Kruskal-Wallis tests were used to compare between 3 groups or more, and Pearson correlation coefficient was used to assess correlations between quantitative variables. Bonferroni adjustment was used for ANOVA post hoc tests of between-group comparisons. In addition, a multivariate regression was conducted to eliminate confounders. A linear regression was performed taking the adherence to treatment as the dependent variable. Variables which gave a P value <.2 in the bivariate analysis were independent variables. A P value <.05 was considered significant.
Results
Sample Description
A total of 247 patients was enrolled. Table 1 summarizes the sociodemographic and clinical characteristics of the participants. The mean age was 52.63 ± 11.92 years, the mean duration of treatment with statins was 59.72 months. A total of 57.5% were males, with 84.6% being married. In addition, 211 (85.4%) took only a statin to control their dyslipidemia (among them 43.3% were using atorvastatin), whereas 36 (14.6%) took a combination of 2 drugs (statin + fibrate or statin + ezetimibe). Table 2 summarizes the scores (mean and SD) observed for each of the questionnaires used.
Sociodemographic and Clinical Characteristics of the Participants.a

aN = 247.
Means and Standard Deviations of all Domains of the Scales.

Abbreviations: IPQ, Illness Perception Questionnaire; TSQM, Treatment Satisfaction Questionnaire for Medication; WHOQOL-BREF, World Health Organization Quality of Life short version.
Factors Affecting Adherence
Mean adherence score was of 73.45%. A significant association was found between adherence and marital status (P < .0001), educational level (P = .001), cigarette smoking (P < .0001), and alcohol drinking (P < .0001; data not shown). Age and body mass index (BMI) were negatively but not significantly correlated with the adherence score, whereas IPQ, TSQM, and WHOQOL-BREF domains’ scores were significantly and positively correlated with adherence (P < .01 for all variables), except for social relationships (Table 3).
Correlation Coefficients of Quantitative Variables Associated With the Adherence Score.
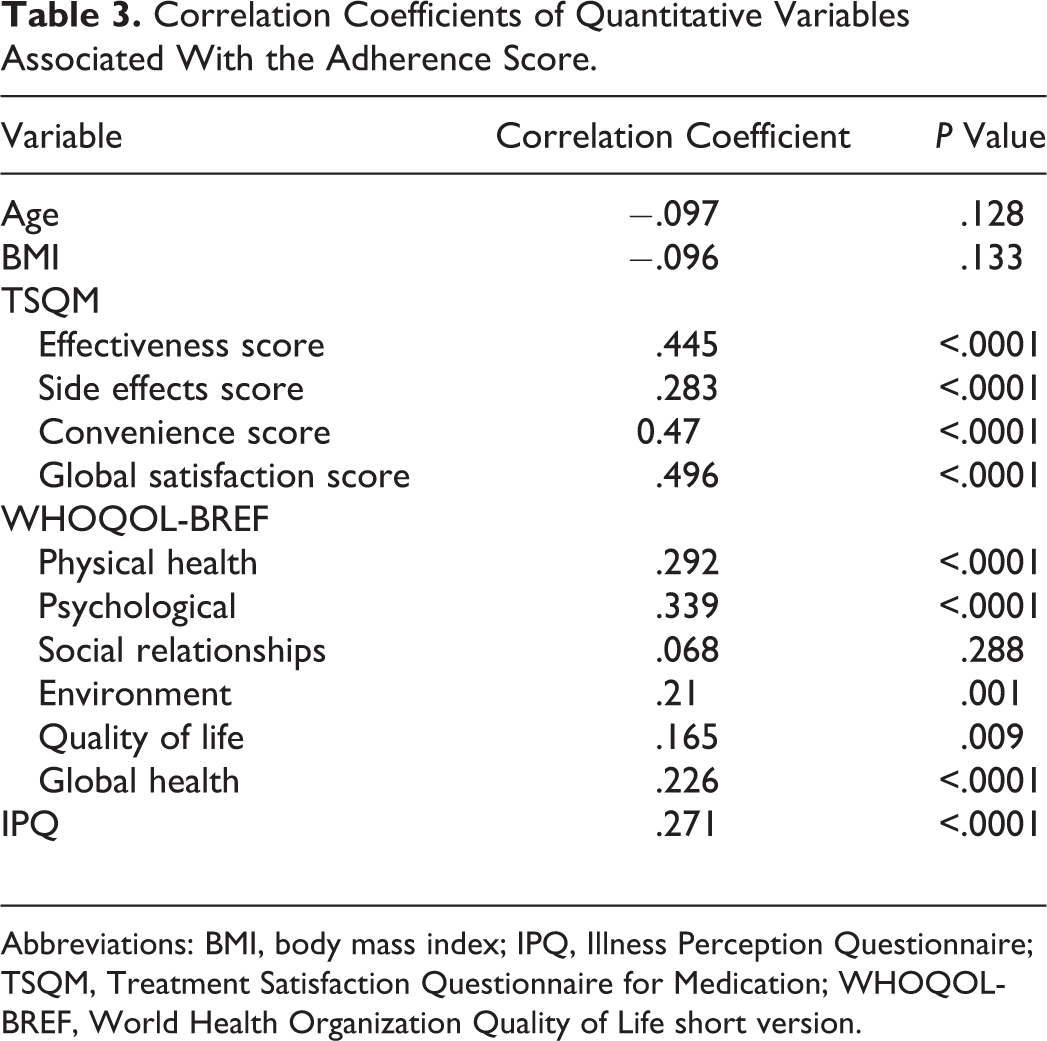
Abbreviations: BMI, body mass index; IPQ, Illness Perception Questionnaire; TSQM, Treatment Satisfaction Questionnaire for Medication; WHOQOL-BREF, World Health Organization Quality of Life short version.
A post hoc analysis showed that married and single patients had a higher mean adherence score (75.02 and 76.31, respectively) compared to divorced/widowed ones (53.28; P < .0001 and P = .018, respectively). In addition, the post hoc analysis revealed that patients with a secondary educational level had a significantly higher mean score than patients with a primary and university level of education (81.03 vs 71.94 and 71.71; P = .031 and P = .042), respectively. As for cigarette smoking, the post hoc analysis showed that a higher mean adherence score was found in nonsmokers versus those who smoke more than 15 cigarettes per day (77.42 vs 62.37; P = .001). Finally, for alcohol, a higher mean adherence score was found for occasional drinkers (≤1 glass per week) compared to those who do not drink alcohol (77.78 vs 68.91; P = .014).
A negative but significant correlation was found between the adherence score and the duration of dyslipidemia (r = −0.199; P = .002). The first cutoff that gave a significant result was that of 60 months; a significantly higher adherence score (77.14) was found in patients with a duration of dyslipidemia <60 months, compared to those having a duration of dyslipidemia longer than 60 months (68.29; P = .011).
It is worth noting that the association between adherence and waterpipe smoking tended to significance (P = .065). Finally, no significant difference was found between adherence scores to the different statin molecules (P = .092).
Factors Affecting QOL
Table 3 shows positive significant associations between adherence and all domains of the WHOQOL-BREF except for social relationships domain. When looking into other factors associated with WHOQOL-BREF domains, the univariate analysis showed that neither gender (P = .257), age (P = .521), marital status (P = .482), educational level (P = .082), and cigarette (P = .363) nor waterpipe smoking (P = .203) were significantly associated with QOL. A significant association was found between alcohol and the QOL (P = .012); however, the post hoc analysis did not reveal any significant differences between the groups.
Factors Affecting Treatment Satisfaction
Table 3 shows significant associations between adherence and TSQM domains’ scores, whereas Table 4 shows significant associations between TSQM domains and participants’ sociodemographic factors. The post hoc analysis showed that a significantly higher mean difference in the effectiveness score was found in single and divorced/widowed patients compared to the married ones (mean difference = 17.04 and 14.41; P < .0001 for both), respectively. A significantly higher difference in the mean side effects score was found in divorced/widowed patients compared to married ones (mean difference = 10.97; P = .042). A significantly higher mean difference in the convenience and the global satisfaction scores was found between the divorced/widowed and the married participants (mean difference = 13.95; P = .001 and mean difference = 12.02; P = .03) respectively.
Factors Significantly Associated to TSQM Domain’ Scores.
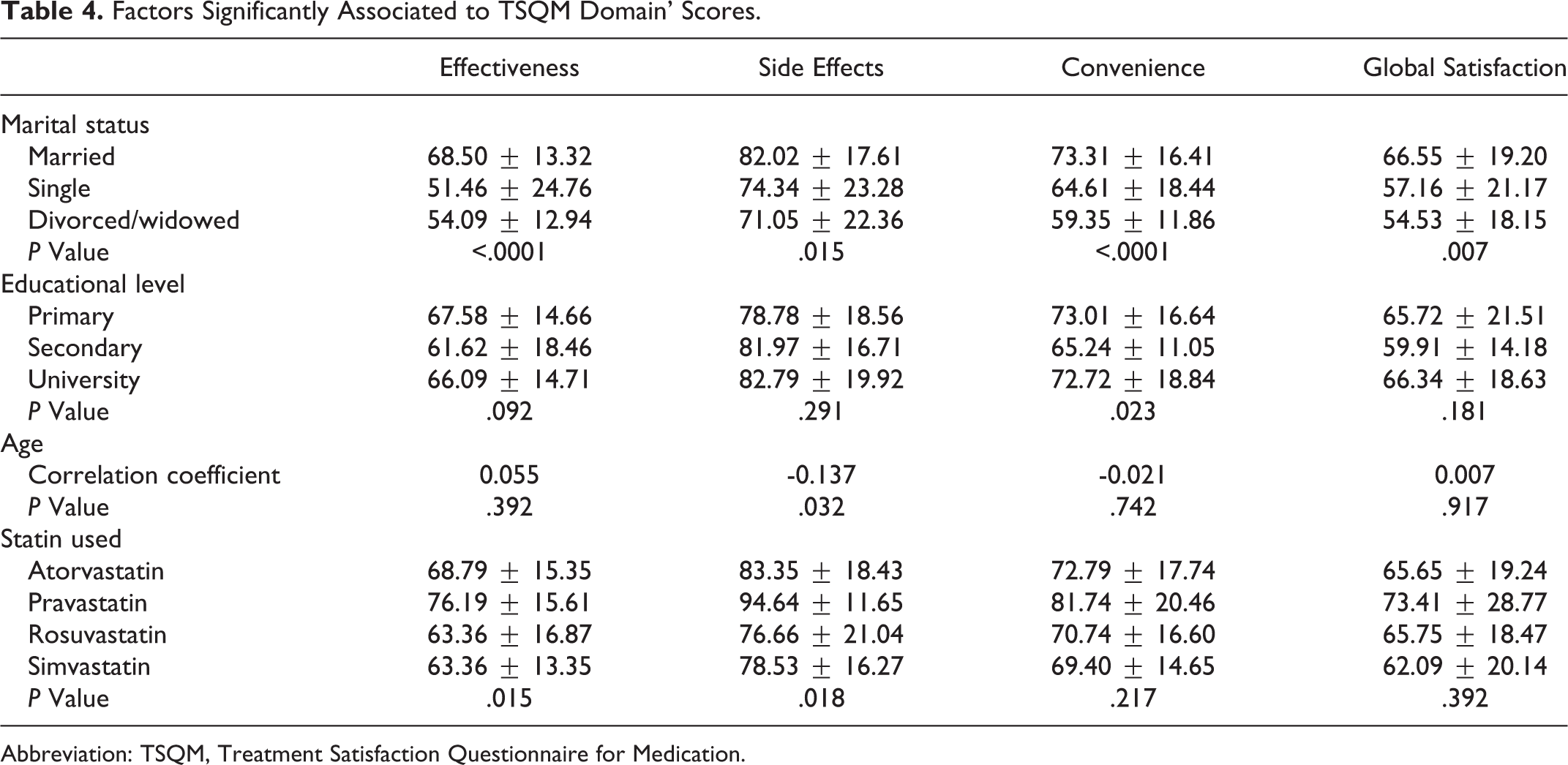
Abbreviation: TSQM, Treatment Satisfaction Questionnaire for Medication.
A significant but negative correlation was also found between the side effect score and age (r = −.137). Treatment Satisfaction Questionnaire for Medication domain’s score showed a significant difference in effectiveness (P = .015) and side effects (P = .018) among statins.
Factors Affecting the Illness Perception
Adherence was positively and significantly associated with IPQ score (P value < .0001; Table 3). Furthermore, when looking into factors affecting the IPQ score, the results showed that the monthly salary, the marital status, the educational level, smoking cigarettes or waterpipes, and drinking alcohol were all associated with the IPQ score (P < .0001 for all variables). In addition, significant correlations were found between the IPQ score, the QOL domains, and the treatment satisfaction domains (P < .05 for all variables; Table 5). It is of note that the IPQ score was not associated with gender (P = .705), age (P = .628), or BMI (P = .703; data not shown).
Significant Associations Between the IPQ Scores and TSQM Domains or WHOQOL-BREF Domains.

Abbreviations: CON, Convenience; EFF, Effectiveness; ENV, Environment; GS, Global Satisfaction; IPQ, Illness Perception Questionnaire; PHY, Physical Health; PSY, Psychological; SE, Side Effects; SR, Social Relationships; TSQM, Treatment Satisfaction Questionnaire for Medication; WHOQOL-BREF, World Health Organization Quality of Life short version.
Multivariable Analyses
The results of the linear regression taking the adherence score as the dependent variable showed that the global satisfaction score (β = 0.32), the secondary level of education (β = 13.43), and the convenience score (β = 0.29) would significantly increase the adherence score, respectively. Furthermore, the effectiveness score (β = 0.27) and smoking more than 3 waterpipes per week (β = 14.06) would also increase the adherence score significantly. On the other hand, smoking more than 15 cigarettes per day (β = −11.15) and a divorced status (β = −14.81) would significantly decrease the adherence score, respectively (Table 6).
Multivariable Analysis.

Discussion
Adherence to treatment is defined as the extent to which patients take their medication in a manner consistent with the prescriber’s recommendations. 30 Multiple factors related to the patient, physician, and health-care system interact together to determine the multifaceted phenomenon of adherence. 31 Nonadherence results in increased hospitalization rates, increased health-care costs, and inadequate therapeutic outcomes. Health professionals have an obligation to provide adequate education regarding the treatment prescribed in order to avoid intentional and nonintentional nonadherence. 32
A recent study among patients who were nonadherent to their statin therapy found a wide range of attitudes and perceptions about statins that contribute to poor adherence including inconvenience, lifestyle preferences, and uncertainty about risks and benefits of statins. 33 Many patients have increased doubts concerning the necessity for statins or more concerns about their potential side effects. 34 There was often worry about and experience of side effects that was found to be associated with increased nonadherence. 35 Our results showed that adherence to the treatment with a statin was significantly and positively associated with the patient’s treatment satisfaction scores (global satisfaction, convenience, and effectiveness) but negatively associated with the side effect score.
Several factors improve adherence to high-intensity statin therapy; these include interaction with the prescriber, participation in cardiac rehabilitation, and elimination of economic barriers. 36 Physicians and patients should work together to establish pharmacological and nonpharmacological goals of therapy, discussing the importance of statin treatment, listening to patients’ concerns, and discussing potential side effects of the treatment, and may have a positive impact concerning the long-term adherence to statin therapy. This applies to the primary prevention and secondary prevention of cardiovascular disease. 37 Statin-associated muscle spasms were shown to be the most common cause of statin discontinuation or dose reduction according to recent findings. 38 In case of the appearance of side effects, the results of a meta-analysis showed that the use of alternate-day dosing of statins (particularly the long-acting statins, atorvastatin, and rosuvastatin) is a reasonable treatment option in patients who are intolerant to more than 1 statin. 39 These implications in the clinical setting were reinforced by a recent study, which demonstrated the importance of patients with coronary heart disease (CHD) to maintain high statin adherence, since statin intolerance was associated with an increased risk of recurrent myocardial infarction and CHD events. 40 Clinicians should avoid discontinuing statin therapy, since it might cause an increase in the atherosclerotic cardiovascular disease. 38 Encouraging more direct dialogue between providers and patients about statin adherence could improve this exchange of information and help identify more patients in need of support to improve adherence. 41 Health-care professionals should also stress on the fact that intolerant patients to 2 or more statins tolerated the statin therapy upon rechallenge, 38 and thus the importance of engaging the patient to overcome their concerns. 38
In our study, we did not assess specific side effects reported for the statin molecule; side effects were only assessed within the treatment satisfaction questionnaire. Further studies are needed to assess the worry-about and patients’ fear of specific statins side effects.
Quality-of-life scores as perceived by the patients in our study ranged from 53.2% (environment) to 64.17% (global health). These numbers are consistent with previously published studies revealing a lower overall QOL score among patients with dyslipidemia (57.9%) compared to controls (76.5%). 42 Positive significant associations were observed between adherence and all domains of the WHOQOL-BREF except for social relationships domain which was not significantly associated to adherence. These new findings emphasize the need for future research to better understand the dynamics between adherence and QOL in patients with dyslipidemia. Such data would be critically important for the optimal management of the patient.
Finally, illness perception is definitely a critical factor when examining adherence in patients with dyslipidemia, since a strong positive association was found between both the scores. A previously published study showed that patients’ illness perceptions were associated with self-reported cholesterol-lowering medication adherence. These associations may be a consequence, rather than a cause, of greater adherence. The authors concluded that given this, intervention strategies aimed at helping patients to establish routines for medication taking may be more effective in increasing adherence than interventions designed to alter perceptions related to taking statins. 43
Our multivariable analysis results showed that patients with a secondary level of education were shown to be more adherent to treatment. In fact, a previous research demonstrated that people with higher education more often want to be involved in decisions about treatment. 44
Patients with a divorced marital status were more likely to be less adherent, in agreement with other findings, which showed that single participants were less adherent to prescribed medication than married ones. 45 Inconsistent results exist concerning the relationship between marital status and medication adherence, 45 with a clear explanation of this relationship remaining unclear. It was hypothesized that spouses facilitate adherence by providing practical support and direct supervision. 46
Smoking more than 15 cigarettes daily was associated with a lower adherence, whereas smoking waterpipes more than 3 times a week was associated with an increased adherence. Greater nicotine dependence was associated with a lower adherence in a recent study, 47 suggesting the importance of nicotine dependence as a barrier to adherence to pharmacological and behavioral cessation treatments. 47 We did not assess the levels of nicotine dependence for cigarettes and waterpipes; further studies are warranted to solidify these findings.
Limitations
Our study has several limitations. The total sample size is small and might not be representative of the whole population. This is a cross-sectional survey with retrospective reports and consequently a low level of evidence. The effect of the recall bias could be differential and lead to the overestimation of effects for some known risk factors. An information bias is also possible, since the use of a questionnaire in a young population or for surrogate responders (parents) may not always be accurate; problems in question understanding, recall deficiency, and over- or underevaluating symptoms may still be possible. In addition, the information about adherence was self-reported, without any information on the refill data. We did not ask the patients about the side effects encountered with statins treatment, which might be an important reason for nonadherence and low perception.
Conclusion
This study showed that patient’s evaluation of their health care is an established component of quality assessment. Global satisfaction, convenience, and effectiveness were associated with a better adherence. Therefore, a good health-care professional–patient communication is a major expectation and an important parameter improving adherence to statins.
Footnotes
Authors’ Contribution
Christine Haddad and Mohammad Salhab contributed to acquisition, drafted manuscript, critically revised manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy; Souheil Hallit contributed to analysis and interpretation, drafted manuscript, critically revised manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy; Aline Hajj contributed to interpretation, drafted manuscript, critically revised manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy; Antoine Sarkis, Eliane Nasser Ayoub, and Hicham Jabbour critically revised manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy; Lydia Rabbaa Khabbaz contributed to conception and design, contributed to interpretation, critically revised manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy. Christine Haddad and Souheil Hallit contributed equally.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.