
Abstract
Background:
Age is a major predictor of contrast-induced acute kidney injury (CI-AKI). Few studies have focused on CI-AKI in elderly patients with acute coronary syndrome (ACS).
Methods:
We compare the incidence of CI-AKI in patients <75 and ≥75 years enrolled in the Protective effect of Rosuvastatin and Antiplatelet Therapy On contrast-induced acute kidney injury and myocardial damage in patients with ACS (PRATO-ACS) study and explore the impact of high-dose rosuvastatin on CI-AKI and clinical outcomes in the 2 age-groups. Statin-naive patients with non-ST-segment elevation ACS scheduled for early invasive strategy (total 504) were randomized to rosuvastatin (40 mg on admission followed by 20 mg/day) or no statin treatment. Contrast-induced acute kidney injury was defined as creatinine increase ≥0.5 mg/dL or ≥25% above baseline within 72 hours after contrast administration. All patients were stratified in tertiles according to baseline high-sensitivity C-reactive protein (hs-CRP).
Results:
Rate of CI-AKI was significantly higher in patients ≥75 years (15.9% vs 8.7%, odds ratio: 2.001; 95% confidence interval: 1.14-3.53, P = .015). No significant interaction was observed between age and statin treatment (P = .17). Pretreatment with rosuvastatin was associated with 65% relative reduction in CI-AKI rate (22/170 [12.9%] vs 8/177 [4.5%], P = .007) in younger patients and 38% (16/82 [19.5%] vs 9/75 [12%], P = .20) in the elderly individuals. The greatest protective effect of statin treatment was achieved in patients with the highest hs-CRP values in both age-groups.
Conclusion:
Patients ≥75 years with ACS had a higher risk of developing CI-AKI. Early high-dose rosuvastatin is efficacious in reducing kidney injury in all patients, especially those with the highest baseline hs-CRP values.
Background
In the last 2 decades, there has been a remarkable increase in the median age of patients admitted with acute coronary syndrome (ACS) and subjected to diagnostic and therapeutic angiographic procedures that use iodinate contrast medium. 1 –3 This has meant also an increase in the percentage of elderly patients exposed to risk of developing contrast-induced acute kidney injury (CI-AKI). 4 Elderly patients are more prone to develop CI-AKI than the younger patients, owing to the physiologic aging of kidneys, often multiple morbidities, and impaired cell repair responses. 5 –9 Since CI-AKI is an important independent prognostic factor, both short- and long term, there is growing attention to strategies for prevention of CI-AKI. However, to date, very few studies have focused specifically on CI-AKI in elderly patients, and there is limited data on the possible different impact of prophylactic measures against CI-AKI in different age-groups. 4,6,8 The aim of this report was to examine the incidence of CI-AKI in patients ≥75 years with non-ST-segment elevation ACS (NSTE-ACS) enrolled in the randomized Protective effect of Rosuvastatin and Antiplatelet Therapy On contrast-induced acute kidney injury and myocardial damage in patients with ACS (PRATO-ACS) study and explore the relative impact of high-dose rosuvastatin on the development of acute renal damage and short- and mid-term clinical outcome (by age) in this population. 10
Methods
The design and main results of the PRATO-ACS study have been described previously.
10
Briefly, 543 statin-naive patients with NSTE-ACS scheduled for early invasive strategy were enrolled in the trial immediately upon admission. Exclusion criteria were long-term lipid-lowering therapy at the time of the index ACS, high-risk features warranting emergency coronary angiography (within 2 hours), acute renal failure or end-stage renal failure requiring dialysis or serum creatinine ≥3 mg/dL, severe comorbidities that precluded early invasive strategy, contraindications to statin treatment, contrast media administration within the last 10 days, and pregnancy or refusal of consent. Eligible patients were randomly assigned to receive high-dose rosuvastatin (statin group) or no statin treatment (control group). After randomization, 39 patients were excluded from the final analysis for the following reasons: 17 had not undergone angiography and 22 did not complete creatinine determination. Thus, a total 504 patients were analyzed, 252 per group. At the time of randomization, patients in the statin group were administered 40 mg rosuvastatin followed by 20 mg/day (10
The primary end point of the present post hoc analysis was CI-AKI defined as an increase in sCr of ≥0.5 mg/dL or ≥25% over the baseline value within 72 hours after contrast agent administration. Additional end points were (1) degree of renal damage evidenced by the maximum sCr increase over the baseline value in the 72 hours after contrast medium administration (“Delta-Creatinine”); (2) adverse cardiovascular and renal events at 30 days including acute renal failure requiring dialysis, persistent renal damage, all-cause mortality, myocardial infarction, or stroke; (3) all-cause mortality or nonfatal myocardial infarction rate at 6 months. 10
Patients were divided in 2 age-groups: <75 and ≥75 years. 11 Categorical variables were summarized as percentages and continuous variables as mean and standard deviation (SD) or median with interquartile range (IQR). The differences between categorical variables were investigated by chi-square analysis or Fisher exact test. Parametric unpaired t test (with Satterthwaite’s correction for degrees of freedom when necessary) or the analogous nonparametric test (Wilcoxon Mann-Whitney U test) was applied to evaluate differences in continuous variables between the 2 groups. Rates of CI-AKI were compared between groups using chi-square analysis. The multivariate logistic analysis performed to evaluate the association between statin treatment and CI-AKI occurrence in the 2 age-groups (<75/≥75 years) included various potential prognostic and confounding factors such as sex, diabetes, hypertension, low-density lipoprotein (LDL) cholesterol, baseline creatinine clearance (CrCl), left ventricular ejection fraction (LVEF), contrast volume, CI-AKI risk score, and baseline hs-CRP. The association between treatment and CI-AKI was expressed as odds ratio (OR) and 95% confidence interval (CI). An interaction term for statin treatment and age was also introduced into the multivariate models to examine the possible role of age (<75/≥75 years) as effect modifier. The effect of statin pretreatment in the two age-groups was also evaluated by gender, baseline LDL cholesterol (<100/≥100 mg/dL), and tertiles of baseline hs-CRP (<2.7, ≥2.7 to <7.5 and ≥7.5 mg/L). 12 All probability values were 2-tailed, and P value less than .05 was considered significant. All the analyses were carried out using STATA 12 software (Stata Corp LP, Texas).
Results
The entire population included 504 statin-naive patients with NSTE-ACS, 347 (69%) <75- and 157 (31%) ≥75-year-olds. Table 1 summarizes baseline demographic, clinical, biochemical, and procedural characteristics of the 2 groups. As expected, the ≥75-year-old group presented higher prevalence of established cardiovascular risk factors, lower left ventricular and renal function, lower hemoglobin levels, lower cholesterol levels and BMI values, and greater use of diuretics and angiotensin-converting enzyme inhibitors. We emphasize that 85.9% of the ≥75-year-olds had preexisting moderate to severe (CrCl < 60 mL/min) chronic kidney disease compared to only 21.6% in the <75 year olds. Furthermore, hs-CRP was significantly higher in the more elderly group, practically half of whom were in the highest hs-CRP tertile (≥7.5 mg/L). Patients ≥75 years also had more extensive atherosclerosis both in coronary and in extracoronary districts. There were no significant differences in contrast volumes and treatment strategies in the 2 groups. Obviously, estimated CI-AKI risk score was significantly higher in the ≥75-year-olds. We must point out that regarding timing, the lapse between symptom onset and randomization and between randomization and contrast medium exposure were significantly longer in the ≥75-year group, often resulting in longer hospital stay.
Baseline Demographic, Clinical, Biochemical, and Procedural Characteristics by Age-Groups.a
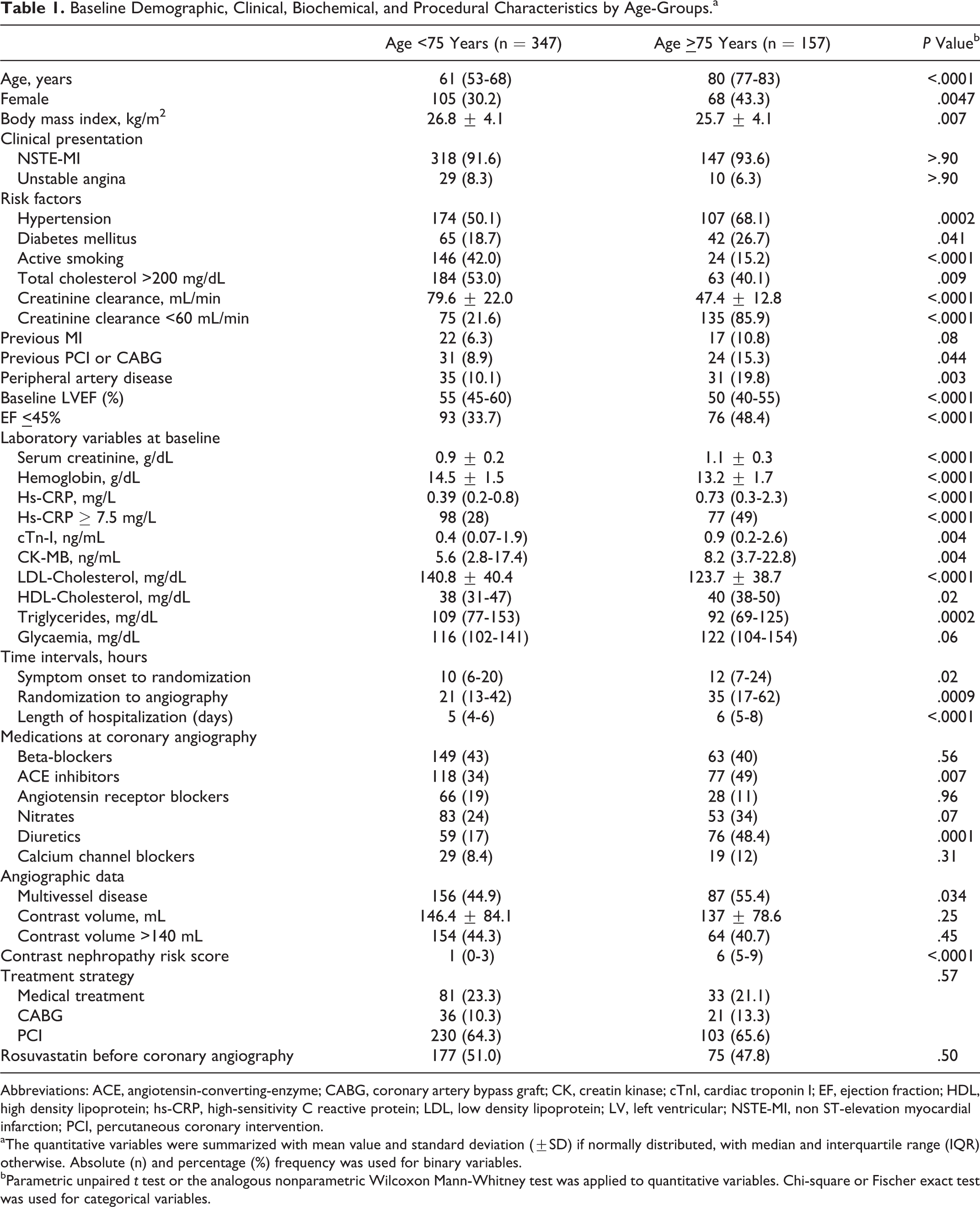
Abbreviations: ACE, angiotensin-converting-enzyme; CABG, coronary artery bypass graft; CK, creatin kinase; cTnI, cardiac troponin I; EF, ejection fraction; HDL, high density lipoprotein; hs-CRP, high-sensitivity C reactive protein; LDL, low density lipoprotein; LV, left ventricular; NSTE-MI, non ST-elevation myocardial infarction; PCI, percutaneous coronary intervention.
aThe quantitative variables were summarized with mean value and standard deviation (±SD) if normally distributed, with median and interquartile range (IQR) otherwise. Absolute (n) and percentage (%) frequency was used for binary variables.
bParametric unpaired t test or the analogous nonparametric Wilcoxon Mann-Whitney test was applied to quantitative variables. Chi-square or Fischer exact test was used for categorical variables.
The primary end point of CI-AKI occurred in 55 patients (10.9%): 30 (8.7%) in the <75 and 25 (15.9%) in the ≥75 group (odd ratio [OR] 2.001; 95% confidence interval [CI]: 1.14-3.53; P = .017; Figure 1, left). Delta-Creatinine was significantly higher in the ≥75-year-olds than in the younger group: 0.11 ± 0.27 vs 0.04 ± 0.23 mg/dL, respectively (P = .008; Figure 1, right).

Contrast-induced acute kidney injury (CI-AKI) rate (A) and mean creatinine increase (Delta-Creatinine; B) in patients <75 and >75 years old.
Incidence of CI-AKI was lower in patients treated with statin than in controls in both groups. In particular, CI-AKI occurrence was reduced by 65% (22/170 [12.9%] vs 8/177 [4.5%], RR 0.349, 95%CI: 0.16-0.76; P = .008) in the <75-year-olds and by 38% (16/82 [19.5%] vs 9/75 [12%], RR 0.615, 95%CI: 0.28-1.31; P = .20) in the ≥75-year-olds (Figure 2, left). After adjustment for confounders, statin pretreatment resulted an independent protective factor against CI-AKI in patients <75 years (adjusted OR 0.24, 95%CI: 0.09-0.60; P = .002) and clinically relevant albeit not statistically significant protective factor in the ≥75-year-olds (adjusted OR 0.67, 95%CI: 0.26-1.78; P = .43). No significant statistical interaction was observed between age (<75/≥ 75) and allocation to statin treatment (P = .17).

Contrast-induced acute kidney injury (CI-AKI) rate (A) and mean creatinine increase (Delta-Creatinine; B) by age (<75/>75 years) and statin treatment.
Mean Delta-Creatinine was lower in statin-treated patients than controls in both the <75 (0.02 ± 0.18 vs 0.07 ± 0.25 mg/dL, P = .049) and ≥75-year-old groups (0.07 ± 0.25 vs 0.13 ± 0.29 mg/dL, P = .18; Figure 2, right).
Division of patients into baseline hs-CRP tertiles evidence that the elderly patients in the highest hs-CRP tertile had a particularly high incidence of CI-AKI compared the younger group (23.4% vs 14.3%, respectively). It is interesting to note that the protective effect of statin pretreatment became significant in the highest tertile of the ≥75-year-olds like in the <75-year-olds (Figure 3). Gender and baseline LDL cholesterol did not affect the results in either age-group.

Contrast-induced acute kidney injury (CI-AKI) rate in patients by age and statin treatment related to baseline high-sensitivity C-reactive protein (hs-CRP) tertiles.
The clinical follow-up was completed in all 504 patients included in the PRATO-ACS study. The incidence of 30-day cumulative adverse clinical events was significantly higher in the ≥75 than in the <75-year-old patients (12.7% vs 2.6%, OR 5.48, 95%CI: 2.44-12.34; P < .001). This difference was mainly driven by the higher rates of death (2.5% vs 0.3%, OR 9.05, 95%CI: 1.003-81.6; P = .05) and persistent renal damage (7.6% vs 1.4%, OR 5.7, 95%CI: 1.96-16.36; P = .001) in the ≥75-year compared to the <75-year-old patients. In both groups, 30-day adverse cardiovascular and renal events were lower in the statin-treated than in the control patients (Table 2). At 6 months, patients ≥75 years old presented a higher rate of death or nonfatal myocardial infarction compared to patients <75 years (8.3% vs 4%, OR 2.15; 95%CI: 0.98-4.68; P = .055), and in both groups the event rate was lower in the statin than in control patients (Table 2).
Adverse Clinical Events at 30 Days and 6 Months by Age and Statin Pretreatment.

aFisher exact test.
Occurrence of CI-AKI (OR 3.13, 95%CI: 1.26-7.78; P = .014), Delta-Creatinine (OR 4.4, 95%CI: 1.5-12.9; P = .008), and 30-day persistent renal damage (OR 4.13, 95%CI: 1.11-15.4; P = .034) resulted significantly associated with 6-month adverse clinical events in the entire PRATO-ACS series of patients.
Discussion
The results of this post hoc analysis of the PRATO-ACS trial show that acute renal damage following contrast medium administration was significantly more frequent, more severe, and more likely to become persistent in ≥75 than in <75-year-old patients. Moreover, elderly patients presented a worse clinical outcome at both 30 days and 6 months. Pretreatment with high-dose rosuvastatin, in addition to routine hydration and NAC administration, was efficacious in reducing renal damage after contrast administration, especially in those elderly patients with the highest baseline hs-CRP levels.
The percentage of elderly patients admitted with NSTE-ACS and scheduled for early invasive strategy is increasing. 1 –3 In the PRATO-ACS trial, patients ≥75 years old account for 31% of all statin-naive patients with NSTE-ACS. The present analysis shows that the incidence of CI-AKI is more frequent in the elderly group confirming a very recent meta-analysis that reported a 2-fold higher incidence compared to younger patients. 8
It is well known that age per se represents an independent risk factor for CI-AKI. 6,13 –15 The higher prevalence of comorbid conditions, age-related cardiovascular and renal changes (structural and functional), and treatment with multiple drugs, especially in the setting of ACS, predispose elderly patients to CI-AKI. 4,5,11,16,17 Our patients present these clinical features of increased vulnerability. In particular, practically 86% of our elderly patients (≥75 years) had a baseline CrCl < 60 mL/min. Reduced GFR, as estimated from the sCr or creatinine-based equations, is highly prevalent in the elderly and strictly associated with both higher risk of CI-AKI and worse short- and long-term renal and cardiovascular outcome. 18 –21
Moreover, in our analysis involving patients with ACS, the elderly patients in particular present high degrees of systemic inflammation due to many interrelated clinical conditions (diabetes, reduced renal and cardiac function, multidistrict atherosclerosis, etc). Increased systemic inflammation, expressed by higher baseline hs-CRP levels, may be an important adjunctive mechanism that contributes to acute renal dysfunction. 22,23 Several studies show links between inflammation and renal damage following contrast medium exposure evidencing a strict relationship between baseline hs-CRP values and CI-AKI rates. 12,24,25
In our series of patients with NSTE-ACS the mean degree of renal damage is mild. However, it is known that even small acute changes in kidney function may cause persistent reduction in renal filtration rate and worsen cardiovascular prognosis. 26 –28 We note that the elderly patients in our study developed more severe (Delta-Creatinine) and persistent renal injury with a 2-fold higher rate of 6-month composite adverse events (death or myocardial infarction) than the younger patients.
The PRATO-ACS study showed that in statin-naive patients with NSTE-ACS scheduled for early invasive strategy, high-dose rosuvastatin, administered immediately on-admission (and always before contrast medium exposure), was associated with a significantly lower incidence of CI-AKI. The kidney protection was adjunctive to standard hydration and NAC administration and was associated with a trend toward a better 6-month clinical outcome. 10
This post hoc analysis evidences that the nephroprotective effect of high-dose rosuvastatin reduces occurrence and severity of acute renal damage after contrast administration even in older patients, albeit generally less pronounced. The relative risk reduction for CI-AKI was 65% in patients <75 years old and 38% in the ≥75 year olds. However, in patients at high risk, such as the elderly individuals, even a less significant reduction in renal damage may have an important clinical impact because even small changes weigh heavily on prognosis. 26,29
Focus on the ≥75-year-olds shows that those with highest baseline hs-CRP values, treated with high-dose rosuvastatin, attained a CI-AKI rate reduction similar to that of the younger group. This confirms that statins work better and more quickly in patients with higher levels of systemic inflammation. 12,30,31
All our patients were treated according to the current guidelines with the same routine prophylaxis (intravenous hydration) and received similar volumes of contrast medium. We wonder if perhaps the elderly (and very high-risk patients in general) might not benefit from more personalized preventive measures even using, for example, bioimpedence-guided or end-diastolic pressure-guided hydration strategies in addition to statins. 32,33
Pooled analysis of clinical trials in older people support use of statins for secondary prevention of cardiovascular events. 34,35 Notwithstanding that current ACS guidelines recommend high-intensity statin administration in all patients with ACS, the role of statin in elderly patients, and in patients with reduced renal function is still debated. 3,36 Our study confirms that also elderly patients with NSTE-ACS scheduled for early invasive strategy can benefit from short-term high-dose statin treatment. In fact, the nephroprotective effect together with reduced myocardial periprocedural damage can contribute to better short-term clinical outcome in statin-naive patients, especially those with NSTE-ACS, consistently reported in several studies and meta-analyses. 37
Limitations
This study is a post hoc analysis with the limitations inherent to its retrospective nature. Due to the small size of the elderly group, there is a likelihood for type I and II errors. The present analysis is hypothesis generating and the results derived cannot be conclusive. Further studies are necessary to demonstrate the clinical impact of the proposed strategy in elderly patients. However, the lack of statistical interaction between age (<75/≥75 years) and statin treatment allocation (P = .17) suggests the favorable renal impact of statin pretreatment in all patients including the elderly individuals even though our numbers are insufficient to permit statistically significant conclusions. Moreover, since all patients were statin naive, most patients who had experienced previous cardiovascular events (generally treated with statins) were excluded from our trial. In addition, as all patients enrolled in the trial had to be able to sign an informed consent, our data may not apply to the frailest of elderly patients.
Conclusions
Patients ≥75 years with ACS had a higher risk of developing CI-AKI. This retrospective analysis confirms the benefit of short-term high-dose rosuvastatin pretreatment in all patients. The reduced frequency, severity, and persistence of kidney injury are of clinical relevance also in the elderly patients.
Footnotes
Author Contributions
Francesco Tropeano contributed to acquisition, analysis, interpretation of data and drafting of the manuscript. Mario Leoncini, Anna Toso and Francesco Bellandi contributed to conception, design, interpretation of data. Mauro Maioli, Laura Dabizzi and Debora Biagini contributed to acquisition, analysis and interpretation of data. Simona Villani contributed to statistical analysis and interpretation of data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.