
Abstract
Objective:
Patients with hypertension tend to have a lower health-related quality of life (HRQOL) compared to normotensive patients. This study’s main objectives are to assess (1) HRQOL and factors that might impact it and (2) association between HRQOL and adherence to treatment, trust in physician, and treatment satisfaction among patients with hypertension.
Methods:
A cross-sectional study enrolled 196 patients from medical-care offices in Beirut, North and South Lebanon. Eligible patients signed a consent form and were asked to complete the Trust in Physician Scale, World Health Organization Quality of Life-brief (WHOQOL-brief) questionnaire, and Treatment Satisfaction Questionnaire (TSQM 1.4) as well as questions assessing medication adherence.
Results:
Better antihypertensive medication adherence was significantly and positively correlated with better HRQOL domains except general health where significance was not reached (P = .089). Better adherence was also significantly related to better treatment satisfaction (side effects, convenience, and global satisfaction but not to effectiveness) and an increased trust in physicians (P < .0001). Better treatment satisfaction (TSQM domains) was significantly and positively associated with a better overall HRQOL (P ≤ .001). Increased trust in physician scores were significantly and positively correlated with a better psychological health, environment, and overall HRQOL domains (P = .045, .005, and .006, respectively). Finally, TSQM effectiveness, convenience, and global satisfaction were significantly higher when trust in physician was greater (P = .017, .035, and .002, respectively).
Conclusion:
The results of this study revealed an association between increased adherence to treatment, a higher global satisfaction, and an increased quality of life. An increased patient satisfaction with their antihypertensive treatment and trust in their physician were also correlated with a greater adherence to treatment.
Keywords
Introduction
Hypertension affects 1 billion people worldwide. It is the most important risk factor of cardiovascular and kidney disease and a leading risk factor for mortality. 1
The estimations of the World Health Organization suggest a prevalence of more than 1 in 5 adults worldwide 2 among who 52% have uncontrolled blood pressure (BP). 3 This condition is responsible for around half overall deaths from stroke and heart disease, and complications from hypertension account for 9.4 million deaths worldwide every year. 4
Hypertension is often described as the silent killer disease, with no or few symptoms, and lowering of BP remains far from optimal in spite of current guidelines and therapies available. Adherence to antihypertensive medications varies from approximately 60% 5 to as low as 26% in some studies, 6 and nonadherence have a major impact on clinical outcomes leading to poor BP control. 7
Many factors are incriminated in potentially affecting adherence to antihypertensive medication, including sociodemographic and cognitive factors, the health-care provider–patient relationship, the characteristics of the health-care system, the number of medications, diseases, and the general health profile of the patient. 8 This latter factor can be looked at from the patient’s perspective using self-perceived health-related quality of life (HRQOL) questionnaires. Health-related quality of life as an indicator for health outcome measurements is gaining importance, especially with reference to chronic diseases such as hypertension, 9 and patients with hypertension tend to have a lower HRQOL compared to their normotensive counterparts. 10 The impact of treatment on HRQOL is especially relevant among patients having hypertension, since antihypertensive treatment is lifelong and may itself worsen HRQOL. 11
Moreover, another factor impacting the outcomes of therapy is treatment satisfaction, 12 a patient-reported outcome, and a major component of quality of health care. Treatment satisfaction may provide insight into a patient’s attitude toward hypertension treatment and is associated with higher adherence to antihypertensive drugs 13 and an improved HRQOL. 14
Finally, the relationship between doctor and patient is the center of quality health care. 15 A trusting doctor–patient relationship increases patients’ adherence to hypertensive treatment according to a study published in 2014 by Polinski et al 16 Other studies have also revealed that patients’ trust in physician is associated with patient satisfaction, adherence to treatment, and continuity of care. 17
Given the very limited number of studies exploring relations between trust of patient with hypertension in their doctor, treatment satisfaction, adherence, and HRQOL, the principal aim of this study was to determine adherence to antihypertensive medications and HRQOL among Lebanese patients with hypertension (where cardiologists are the main prescribers of antihypertensive medications) with at least 1 antihypertensive drug.
Our secondary objectives were to explore sociodemographic and clinical factors that might impact both adherence and HRQOL and to examine the associations between HRQOL, adherence to treatment, trust in physician, and treatment satisfaction.
Methods
Ethical Considerations
The institutional review board of Saint-Joseph University approved the protocol of this study (ref USJ-2015-32). This study is observational and was considered to be a less than minimal risk research study with no known emotional, physical, or psychological risks; no special population such as pregnant women, prisoners, or minors were involved. No investigational product was administered. Patients were recruited from medical care offices (cardiologists’ clinics) in Beirut, North and South Lebanon. All participants gave their informed written consent prior to their inclusion in the study.
Participants and Setting
In this cross-sectional study, participants were recruited while they were on a routine visit to their doctor and approached by a trained research assistant. All doctors who helped in the data collection were senior cardiologists. The patient filled the self-administered questionnaire after the end of the visit. Patients’ inclusion was done between May 2015 and September 2016. Inclusion criteria were Lebanese adults (≥ 18 years old), diagnosed with primary hypertension at least 3 months before recruitment in the study, taking at least 1 antihypertensive drug since 3 months or longer. An additional criteria for patients completing the Trust in Physician Scale was being with the same physician for at least 3 months prior to the study and a minimum of 3 visits during this time. Exclusion criteria were a cognitive disease or a secondary hypertension or an inability to recognize their antihypertensive drugs from the other medications they were taking.
Sample Size Calculation
We fixed our expected frequency of high adherence at 16% based on the findings of a previous study 7 and chose a precision level of ±7%. This would allow for adequate power for bivariable and multivariable analyses to be carried out. The Epi-info software version 7.2 (population survey) calculated a minimum sample size of 187 patients to ensure a confidence level of 95% based on a population size of 4 million in Lebanon.
Participant’s Demographic and Clinical Information
Age, sex, level of education, marital status, pathologies other than hypertension, antihypertensive drugs used, treatment duration, and number of antihypertensive drugs (pills per day) were collected through a face-to-face interview performed by a lay person (trained research assistant), independent of the study, who was present at the cardiologists’ clinics and was responsible for applying the criteria, obtaining the written consent, and handing out the questionnaires to the participants and then collecting them. Two hundred forty-two eligible patients were identified during the period of the study. Of those, 38 declined and 8 were excluded because they were not able to really recognize their antihypertensive drugs from the other medications they were taking. One hundred ninety-six patients included completed the study. Blood pressure was measured using a mercury sphygmomanometer (Microlife AG, Widnau/ Switzerland) by a trained nurse. With the patient in sitting position, 2 BP measures were obtained at 5-minute intervals; the BP value was determined using the average of the 2 readings.
Questionnaire Assessment
After collecting basic sociodemographic and clinical information, eligible patients completed the questionnaire consisting of adherence assessment questions, Trust in Physician Scale, the World Health Organization Quality of Life brief (WHOQOL-brief), and Treatment Satisfaction Questionnaire (TSQM 1.4) for Medications.
Adherence Assessment
The adherence to antihypertensive drugs was assessed by asking the patients about the frequency, percentage, and rating response of their hypertensive medications/classes use during the last month. The main pharmacological classes of medications prescribed to the patients were the angiotensin receptor antagonists, nonpotassium and potassium -sparing diuretics, beta-blockers, calcium channel blockers, angiotensin-converting enzyme inhibitors, and centrally acting antihypertensive drugs.
The adherence to antihypertensive drugs was assessed using an adaptation of Lu et al 18 questionnaire by asking the patients about the frequency, percentage, and rating response of their antihypertensive use during the last month. Initially, the questionnaire of Lu et al was validated among patients with HIV and was later used in a population of patients attending general practice. 19 Concerning the frequency, we asked the patient “did you take all your medications all the time?” with the possible responses being divided as follows: 0% for none of the time, 20% for a little of the time, 40% for some of the time, 60% for a good bit of the time, 80% for most of the time, and 100% for all the time. The percent item was checked using the question “what percent of the time were you able to take your medications exactly as your doctor prescribed them?.” The rating item was assessed using the following question “rate your ability to take all your medications as prescribed” with the possible answers being divided as follows: 0% = very poor, 20% = poor, 40% = fair, 60% = good, 80% = very good, and 100% = excellent. The total score was calculated by summing all 3 answers and presented in a percentage. 18 –20 The total score obtained could be presented then as a percentage. 18 –20 The presence or absence of medication adherence was dichotomized in a way where scores <80% reflect low adherence and scores ≥ 80% reflect medium/high adherence. 4
Treatment Satisfaction Measure
It was assessed using the TSQM 1.4 for Medication. This instrument consists of 14-item and is psychometrically robust and validated. It comprises 4 domains: effectiveness items: 1 to 3, side effects items: 4 to 8, convenience items: 9 to 11, and global satisfaction items: 12 to 14. The TSQM 1.4 domain scores range from 0 to 100, with higher scores representing higher satisfaction in that domain. The “Global Satisfaction” scale of the TSQM is used to assess the overall level of satisfaction or dissatisfaction with medications that patients present. 21 The TSQM utilizes the 3 primary dimensions of treatment satisfaction (effectiveness, side effects, and convenience) as well as patient’s overall rating of global satisfaction to compare the relative importance of various medications used to treat a particular illness. 22
Health-Related Quality of Life Measure (WHOQOL-Brief)
The WHOQOL-brief is a 26-item questionnaire that assesses 4 domains of the quality of life: (1) D1-physical (7 items): related to daily living, energy and fatigue, mobility, medical treatment, pain and discomfort, sleep and rest, and work capacity; (2) D2-psychological (6 items): related to body image and physical appearance, positive and negative feelings, spirituality/personal beliefs, self-esteem, and cognition; (3) D3-social relationships (3 items): personal relationships, sexual activity, and social support; and (4) D4-environment (8 items): financial resources, physical security, freedom, accessibility and quality of social and health care, home environment, opportunities for acquiring new information and skills, and participation in and opportunities for recreation, transport, and physical environment. It also includes 2 separate items evaluating the overall quality of life (Q1) and satisfaction with one’s state of health (Q2). 23
It also includes facets assessing overall QOL (first question) and satisfaction with general health (second question). Each item is rated on a 5-point Likert-type scale, and scores are transformed into a 0 to 100 scale. Higher scores indicate a better HRQOL. The WHOQOL-brief is a valid instrument for assessing HRQOL across different languages and cultures and has adequate test–retest reliability, internal consistency, and factor structure within the medical setting.
Trust in Physician Scale
It is an 11-item scale, and each item is scored on a 5-point Likert-type scale ranging from 1 (strongly disagree) to 5 (strongly agree). The unweighted mean of the responses to the 11 questions are summed and value transformed into a 0 to 100 scale. Higher scores mean greater trust. The wording of the 11 questions and the scoring system for each question are presented in Appendix A. This scale was largely used among different participants’ population and across a wide range of pathologies. 24 –27 In order to accurately complete the questionnaire, participants were asked to think of the cardiologist who usually provided their hypertension follow-up and care. Nine patients refused to fill this part of the questionnaire.
Statistical Analysis
The software program used is SPSS for Windows version 23.0. Sociodemographic and disease/drug-related characteristics of the participants were presented using descriptive statistic. Normality of the distribution was tested when appropriate using the Kolmogorov-Smirnov test. Univariate analysis of categorical and continuous variables were performed using the χ2 or the Fisher exact tests and the student t test, respectively. The analysis of variance (ANOVA) test was used to compare means between 3 groups or more. The dichotomized adherence score (presence of medication adherence ≥ 80 [very good/excellent]; absence of medication adherence <80 [other categories]) was analyzed using logistic regression analysis. A multivariate stepwise linear regression was carried out, taking the quality of life score as the dependent variable and using variables that showed a P < .2 in the bivariate analysis as independent variables 28,29 ; potential confounders may be eliminated only if P > 0.2 in order to protect against residual confounding. 30 The correlation coefficient was used to test collinearity among independent variables. The Cronbach α values were recorded for the reliability analysis of all the scales.
Results
In total, 196 (51.5% male) participants were included in this study. Of those 196 participants, 187 filled the Trust in Physician Scale. Missing data were not replaced for this analysis due to their low percentage (<10%): For all questionnaires, except trust in physician, at least 195 answered.
We calculated the reliability of each scale to assess the quality of our data. We obtained a good Cronbach α for the adherence scale (0.783), the TSQM scale (0.902), the WHOQOL-brief scale (0.766), and the Trust in Physician Scale (0.892).
Sociodemographic and clinical characteristics of all the participants are outlined in Table 1. The 4 most frequently observed pathologies (other than hypertension) were hypercholesterolemia (61.7% of participants), coronary artery disease (25.0%), diabetes (24.0%), and elevated triglycerides (20.4%). The clinical characteristics of the patients, the TSQM domains, adherence, WHOQOL-brief domains, and Trust in Physician Scale mean scores are shown in Table 1 as well. Only 46 patients were treated with only 1 antihypertensive drug. The most commonly used classes of antihypertensive drugs were the angiotensin receptors antagonists (56.12% of the patients), the nonpotassium-sparing diuretics (55.10% of the patients), and the β-blockers (52.55% of the patients). The most common combination was an angiotensin receptor antagonist with a nonpotassium-sparing diuretic.
Demographic, Clinical Characteristics of Patients, and Scores of TSQM Domains, Adherence to Treatment, WHOQOL-Brief Domains, and Trust in Physician Scale.a
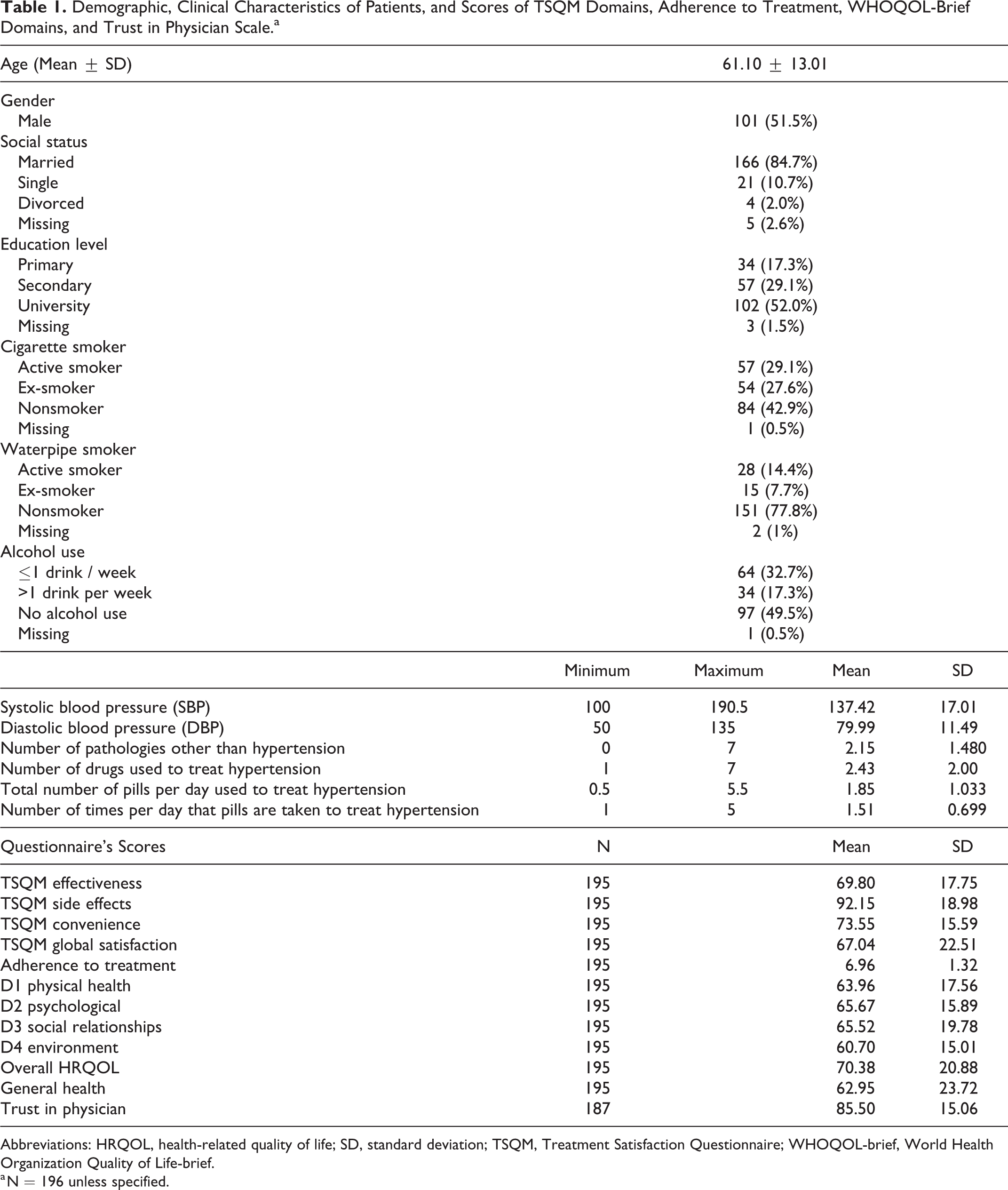
Abbreviations: HRQOL, health-related quality of life; SD, standard deviation; TSQM, Treatment Satisfaction Questionnaire; WHOQOL-brief, World Health Organization Quality of Life-brief.
a N = 196 unless specified.
Bivariate Analysis
Treatment Satisfaction Questionnaire
Older age and taking fewer pills had higher effectiveness. Taking a higher number of drugs, number of times per day that pills are taken as well as a higher SBP had more side effects. A higher number of pills per day and diastolic blood pressure (DBP) had lower convenience. Older age and female gender had more global satisfaction, whereas regular drinkers had lower global satisfaction. Finally, a higher trust in physician score was significantly associated with a higher TSQM effectiveness, convenience, and global satisfaction scores (P = .017, .035 and .002 respectively; Tables 2 and 3).
Correlations Between Patients’ Characteristics and TSQM Domains, MMAS Score, WHOQOL-Brief Domains or Trust in Physician Score.a

Abbreviations: DBP, Diastolic blood pressure; HRQOL, health-related quality of life; SBP, systolic blood pressure; TSQM, Treatment Satisfaction Questionnaire; WHOQOL-brief, World Health Organization Quality of Life-brief.
a Numbers in bold represent significant results; P = P values; N = sample size; P<0.05 were considered significant.
b Antihypertensive drugs only.
Correlations Between the Different Domains of TSQM, WHOQOL-Brief, Adherence to Treatment, and Trust in Physician Scale.a

Abbreviations: HRQOL, health-related quality of life; TSQM, Treatment Satisfaction Questionnaire; WHOQOL-brief, World Health Organization Quality of Life-brief.
a Numbers in bold represent significant P values.
Patients with higher adherence were older, had more pathologies, and were taking more classes of medication, whereas the Trust in Physician score was positively correlated with the number of drugs (r = 0.227), the environment score (r = .296), overall quality of life (r = .292), and adherence to treatment score (r = .412). Moreover, trust was higher among participants with primary education. Adherence was also significantly related to TSQM (side effects, convenience, and global satisfaction but not to effectiveness) and to trust in physician (P < .0001; Table 3).
As for HRQOL, physical health was negatively correlated with the number of pathologies, the number of pills, and to DBP. Males and regular alcohol users presented higher values. The quality-of-life score was significantly and positively correlated with all the TSQM subscales scores, along with the adherence and the trust in physician scores (Table 3). Antihypertensive medication adherence was significantly and positively correlated with all HRQOL domains except general health where significance was not reached (P = .089). Furthermore, the ANOVA test showed no significant difference between the quality of life score and the marital status (P = .314), educational level (P = .110), cigarette (P = .419), waterpipe smoking (P = 0.805), and alcohol drinking (P = .529; data not shown).
Psychological health scores were higher among males, participants with higher education, and regular alcohol drinkers. The lowest values for social relationships domain were observed among patients with primary education, and this domain was negatively correlated with the number of pills.
Environment domain scores were higher among participants with higher education but not correlated with any other variable. General health domain was negatively correlated with number of pathologies and of pills.
Multivariable Analysis
In a linear regression model, taking the health-related quality of life score as the dependent variable showed that adherence to treatment and global satisfaction were associated with a higher quality of life (β = 4.227 and β = 0.341, respectively). Moreover, males had a significantly higher quality-of-life score compared to females (β = 8.326; Table 4).
Multivariable Analysis—Linear Regression Assessing Factors That Would Affect the Quality of Life Score Taken as the Dependent Variable.

a Variables entered in the model: TSQM effectiveness score, TSQM side effects score, TSQM convenience score, TSQM global satisfaction score, total adherence score, trust in the physician score, number of hypertensive drugs taken, gender, educational level.
b Reference group.
Discussion
This study’s main results showed that male gender, adherence to treatment, and treatment global satisfaction were associated with increased quality of life. The importance of patients’ common-sense beliefs or lay perceptions about their illness and treatment is increasingly recognized as determinants of treatment success or failure. 31 In parallel, people’s physical and mental health status definitely plays an irreplaceable role in clinical treatment, and HRQOL has become a multidimensional concept for the comprehensive assessment of this status. 32 To our knowledge, there are few authors who evaluated the association between HRQOL and adherence to antihypertensive treatment or treatment satisfaction. 33 Patients have higher satisfaction with their antihypertensive medication if their BP control is improved and their medication has minimal side effects. 34 The study did suggest that there are differences in adverse events across different antihypertensive medication classes and that those adverse events can affect patients’ satisfaction with treatment. 34
In our study, physical health was negatively correlated with number of pathologies, number of pills, and DBP. General health domain was also negatively correlated with number of pathologies and pills. Male patients showed significantly higher scores of WHOQOL-brief scale, suggesting poorer HRQOL in females compared to males which is in accordance with previous studies. 35,36
Our study also revealed that a better adherence was associated with a better HRQOL, which was somewhat expected, since the treatment of hypertension is usually taken for lifetime, and its success will depend on the effects of the drug regimen on the patient’s quality of life. 37 One simple explanation can be that good adherence prevents hypertensive crisis or hypertension cardiovascular complications, leading to a better quality of life for the patient.
Health-related quality of life domains were significantly and positively correlated with treatment satisfaction in this study: being satisfied with his or her antihypertensive treatment significantly increases the patient’s quality of life. A higher quality of life was also correlated with higher medication adherence.
In addition, treatment satisfaction (side effects, treatment convenience, and global satisfaction) was significantly and strongly associated with hypertensive medication adherence. This was described in a previous study conducted among older patients having hypertension 13 and in another conducted by our research team. 38 Interestingly, adherence was not significantly related to TSQM effectiveness, in opposite to previous findings. 39 –41 A better adherence was found in patients with greater perceived self-efficacy in medication taking.
Adherence to treatment was significantly and positively correlated with age, similar to other studies 42,43 that found that older patients were more compliant than younger ones. In addition, adherence was positively correlated with the number of medications taken per day and the number of pathologies in opposite to the findings of Kamran et al. 44 These variations might be due to a high level of awareness, an increased motivation among the respondents with hypertension in our sample, and because patients were taking combinations of drugs, thus minimizing the number of tablets to be taken daily. The 2013 ESH/ESC Guidelines 45 favor the use of combinations of 2 antihypertensive drugs at fixed doses in a single tablet, because reducing the number of pills to be taken daily improves adherence and increases the rate of BP control.
Treatment satisfaction was previously reported as a reliable indicator of HRQOL in patients presenting with hypertension. 46 Our results confirmed this finding and showed that treatment satisfaction and HRQOL are intimately associated.
Among other factors that could affect positive treatment outcome is the physician–patient relationship. Nonadherence to treatment can be due, among other factors, to patient’s lack of knowledge about the provider’s decision-making process regarding his prescription. 47 Another barrier to adherence and thus to achieving treatment goals is low physician credibility and trust. 16,47 Our results showed that trust in physician scores were higher among participants with primary education compared to higher educated patients. This finding is aligned with published results, among primary care patients, revealing significant relationships between race, education, and patient’s trust of their physicians. 48
Other interesting findings that merit being highlighted are that several QOL domains including overall QOL, treatment satisfaction (effectiveness, convenience, and global satisfaction) as well as adherence were higher when trust in physician was greater. Thus, when aiming hypertension optimal control, prescribers need to consider trust development not only by providing correct treatment but also by creating a respectful and caring relationship with patients through sharing in decision-making and good communication skills.
Limitations
This study is not without some limitations: A relatively small convenience sampling was realized. Participants who presented to medical care offices between May and September 2016 and met the inclusion criteria were included if they agreed to participate; therefore, larger studies are needed to confirm the results, since representativeness of the sample could be an issue. The use of a single self-reported quality-of-life questionnaire is another limitation. Self-report questionnaires should only be used to measure changes and severity of symptoms and should never be used as the single diagnostic tool for a disorder. In addition, self-reported questionnaires may have been subjected to reporting bias. Participants may have forgotten pertinent details or may have overestimated or underestimated them as they may have been too embarrassed to reveal information they consider private. However, external pressures were unlikely to have significantly affected the responses because participants were assured that the results were completely confidential. Another limitation is the possibility that there may be an association between adherence, quality of life, treatment satisfaction, and individual medication classes that were not identified in this study. Furthermore, the trust factor may be deeply influenced by how long a patient has been with a particular physician, a factor that we did not really assess in this study. There is a significant selection bias in that all the included patients had attended their physician on at least 3 occasions in the preceding 3 months. Patients who are nonadherent and who lack trust in their physician are extremely unlikely to have attended in such a regular manner and hence are unlikely to have been adequately represented in the study. This should be acknowledged as a limitation also. Finally, the quality of life of patients with hypertension could vary with the duration of the disease.
However, this study presents some strengths: (1) It combined multiple validated questionnaires and examined various correlations between them, (2) the simplicity of the questionnaires made it easier for the participants to give accurate information, and (c) several major findings are new and unpublished yet.
Conclusion
Up to 50% of patients having chronic illnesses will end up making their own medication-related decisions, without asking for medical advice, and they can eventually become nonadherent. 49 To achieve an optimal control of hypertension, following guidelines in prescribing and providing the correct treatment is not enough. Doctors need to take into consideration patient’s health-related decision-making. This process as showed in this study can be affected by multiple patient’s self-perceived factors such as quality of life under treatment, satisfaction with the treatment prescribed, adherence to treatment, and the relationship with the prescriber (mainly trust).
Footnotes
Appendix A
Trust in Physician Scale Questions.

| Totally Disagree | Disagree | Neutral | Agree | Totally Agree | |
|---|---|---|---|---|---|
| (1) I doubt that my doctor really cares about me as a person. |
|
|
|
|
|
| (2) My doctor is usually considerate of my needs and puts them first. |
|
|
|
|
|
| (3) I trust my doctor so much I always try to follow his/her advice. |
|
|
|
|
|
| (4) If my doctor tells me something is so, then it must be true. |
|
|
|
|
|
| (5) I sometimes distrust my doctor’s opinions and would like a second one. |
|
|
|
|
|
| (6) I trust my doctor’s judgments about my medical care. |
|
|
|
|
|
| (7) I feel my doctor does not do everything he/she should about my medical care. |
|
|
|
|
|
| (8) I trust my doctor to put my medical needs above all other considerations when treating my medical problems. |
|
|
|
|
|
| (9) My doctor is well qualified to manage (diagnose and treat or make an appropriate referral) medical problems like mine. |
|
|
|
|
|
| (10) I trust my doctor to tell me if a mistake was made about my treatment. |
|
|
|
|
|
| (11) I sometimes worry that my doctor may not keep the information we discuss totally private. |
|
|
|
|
1 |
Appendix B
Authors’ Note
All procedures involving human participants performed in this study were in accordance with the ethical standards of the institutional review board of Saint-Joseph University (approval number ref USJ-2015-32) and with the 1964 Helsinky declaration and its later amendments or comparable ethical standards. All individual participants gave their written informed consent prior to inclusion.
Acknowledgments
We would like to thank Dr Nada EL OSTA for her help in the statistical analysis and all the cardiologists that helped us, especially Dr Sani HLAIS, and all the participants.
Author Contributions
Jneid, S. contributed to acquisition, drafted the manuscript, critically the revised manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy; Jabbour, H. contributed to acquisition, critically revised the manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy; Hajj, A., Sarkis, A. and Licha, H. critically revised the manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy; Hallit, S. contributed to analysis and interpretation, drafted the manuscript, critically revised the manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy; Khabbaz, L. contributed to conception and design, contributed to analysis and interpretation, drafted the manuscript, critically revised the manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy. The authors Souheil Hallit and Lydia Rabbaa Khabbaz are last co-authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.