
Abstract
Background:
Low cholesterol levels are associated with a worse outcome in patients with heart failure (HF). Use of statins in HF remains controversial. We aimed to assess whether the prognosis of patients with intrinsically low cholesterol levels differed from that of those with pharmacologically induced low cholesterol.
Materials and Methods:
We conducted a retrospective cohort study on 464 ambulatory patients attending a specialized HF clinic. Patients were cross-classified according to statin therapy and admission total cholesterol level (low cholesterol <150 mg/dL and cholesterol ≥150 mg/dL): (1) low total cholesterol level on statin therapy; (2) low total cholesterol level not taking statins; (3) cholesterol ≥150 mg/dL on statin therapy; and (4) cholesterol ≥150 mg/dL not on statin therapy. Patients were followed up to 5 years and the outcome was all-cause death. A Cox regression analysis was used in prognosis assessment.
Results:
Almost two thirds of the patients were men and the median population age was 69 years; 22.8% of the patients had preserved ejection fraction and 43.5% severe systolic dysfunction. The patients with an intrinsically low cholesterol had a hazard ratio of all-cause death up to 5 years of 2.38 (1.08-7.14) compared to those with low cholesterol induced by statin use. This association was independent of other variables associated with outcome.
Conclusions:
Patients with HF with instrisically low cholesterol levels have a double risk of death up to 5 years compared to patients with pharmacologically induced low cholesterol. Clinicians should not limit the use of statins by fear of lowering the cholesterol levels.
Introduction
The efficacy of statins in reducing morbidity and mortality in patients with documented coronary artery disease (CAD) or those at increased risk of CAD is unquestionable. 1,2 These beneficial effects are probably due to their low-density lipoprotein (LDL) cholesterol-lowering effects and also to cholesterol-independent effects, including improvement in endothelial function, inhibition of neurohormonal activation, decrease in proinflammatory activation, and prevention of ventricular remodeling. 3 –5
In chronic heart failure (HF), evidence regarding the beneficial effects of statin therapy remains contradictory. Various nonrandomized and retrospective studies have suggested improved prognosis in patients treated with statins 6,7 ; however, these results were not confirmed by 2 more recent prospective trials, involving more than 10 000 patients. 8,9 Despite this, as chronic HF and CAD or other compelling indications for statin often coexist, this therapy has become of widespread use in chronic HF.
To further aggravate uncertainty, concern was raised regarding the potential adverse effects of low cholesterol levels. It has been recognized 10,11 that there is a phenomenon of reverse epidemiology with cholesterol in HF, this is, a low cholesterol associates with worse morbidity and mortality in patients with HF. The optimal value of cholesterol to start therapy is not known and neither is known whether there is a value of cholesterol below which is better to suspend and/or not to start statin therapy. To answer these questions, it would be important to know whether patients with intrinsically low cholesterol and those with low cholesterol on statin therapy differ in terms of prognosis.
We aimed to assess whether prognosis of patients with intrinsically low cholesterol levels differed from that of those with pharmacologically induced low cholesterol.
Methods
We conducted a retrospective cohort study on ambulatory patients attending a specialized HF clinic at Hospital São João, a public tertiary care academic hospital. The files were screened sequentially based on the file number order; this is, from the first, in 1997, to the last patient referred to the HF clinic in 2007. Patients’ medical records were screened in order to identify eligible patients. All patients were eligible if weight was recorded in the first appointment and if lipid profile upon referral was known. Knowledge of statin use was also required for study inclusion. Information regarding comorbid conditions and medication started in the first medical visit was abstracted from the charts. Information concerning physical data examination and laboratory parameters was also gathered.
A total of 464 patients were included in the study. Patients on statin therapy and those not were characterized and compared. A total cholesterol level of 150mg/dL was chosen as the cutoff value below which patients were considered as having low total cholesterol. Although arbitrarily defined, it corresponded to the 25th percentile of total cholesterol at admission, so to patients in the lowest range of total cholesterol distribution. Patients with and without low cholesterol were also compared.
According to cholesterol levels (low and not low) and statin use (yes or no), patients were cross-classified in 4 groups: (1) those with low total cholesterol level on statin therapy use; (2) patients with low total cholesterol level and not on statin therapy use, (3) those taking statins and with cholesterol ≥150 mg/dL, and (4) those not taking statins and with total cholesterol ≥150 mg/dL.
Heart failure diagnosis was considered according to the European Society of Cardiology criteria. 12
Severity of systolic dysfunction was classified according to the subjective impression of the operator (all echocardiograms were performed by a cardiologist): severe left ventricular systolic dysfunction (LVSD) corresponded to left ventricular ejection fraction (LVEF) lower than 30%, moderate LVSD to LVEF between 30% and 40% and mild LVSD to LVEF between 40% and 50%. Left ventricular EF above 50% was assumed as preserved systolic function and therefore HF with preserved systolic function.
For prognostic analysis, the single end point of all-cause death was used. Length of follow-up was considered from the date of the first medical visit until the occurrence of death from all-cause or the last contact with the patient, censored at 5 years. Follow-up was based on hospital records and telephone contact.
The study protocol conforms to the ethical guidelines of the declaration of Helsinki and it was approved by the institution’s ethics committee. The authors of this article have certified that they comply with the Principles of Ethical Publishing in the International Journal of Cardiology.
Statistical Analysis
Categorical variables are presented as counts and proportions. Continuous variables are presented as mean (standard deviation) or median (interquartile range) if the distribution is skewed. Comparison between groups of patients under and not under statin therapy as well as between those with and without low total cholesterol level were made using a chi-square test for categorical variables, independent samples t test for continuous variables that were normally distributed, and Mann-Whitney test for continuous variables with a skewed distribution. Survival in the 4 groups created was assessed using the Kaplan-Meier method.
In the subgroup of patients with low cholesterol level (n = 112), a Cox regression analysis was used to identify variables associated with a worse outcome. A multivariate model was built based on the variables that showed prognostic impact in a univariate approach. The use of β-blockers (BB) was also considered in the multivariate model. We used a forward conditional Cox regression analysis in the multivariate model.
All analyses were conducted using the SPSS 18.0 (SPSS Inc, Chicago, Illinois); P < .05 was considered to be statistically significant.
Results
Between 1997 and 2007, 505 patients were referred to the HF clinic. Of these, 10 only attended the first appointment and were lost to follow-up. A total of 464 had known lipid profile in the first visit and the use of statins was recorded. The median (interquartile range) of follow-up was 1124 (622-1800) days. Almost two third of the patients were men and the median age was 69 years. Most of the patients were in New York Heart Association (NYHA) class I or II and 195 (43.5%) of them had severe LVSD. The mean admission total cholesterol was 188 mg/dL and 180 (38.8%) patients were on statin in the first appointment.
Patients on statin use more often had HF of ischemic etiology (88 of 180 [49%] vs 81 of 284 [31%] in those not taking a statin; P value <.001) and more often had LVSD (149 [85.1%] vs 197 [72.2%] in patients not on statin use; P = .002). Patients on statin therapy also had more chronic comorbidities: arterial hypertension (117 [65%] vs 155 [55%]; P = .03), diabetes (77 [43%] vs 71 [25%]; P < .001), and cerebrovascular disease (33 [18%] vs 23 [8%]; P = .001); they also had worse renal function (1.12 [0.95-1.46] mg/L of plasma creatinine in patients treated with statin versus 1.04 (0.90-1.29) in those not on statin; P = .001). The remaining demographic, physical, and laboratory variables showed no significant differences between groups.
The mean population total cholesterol was 188 mg/dL and the median (interquartile range [IQR]) was 186 (150-219) mg/dL. Patients with total cholesterol below and above 150 mg/dL are characterized and compared in Table 1. Patients with admission cholesterol below 150 mg/dL more often had diabetes and a low cholesterol associated with other worse prognostic predictors like a lower systolic blood pressure, lower hemoglobin, and lower serum sodium. Importantly no significant differences existed between groups concerning HF etiology and presence of LVSD.
Comparison Between Patients With Low Admission Total Cholesterol and Those With Admission Total Cholesterol ≥150 mg/dL
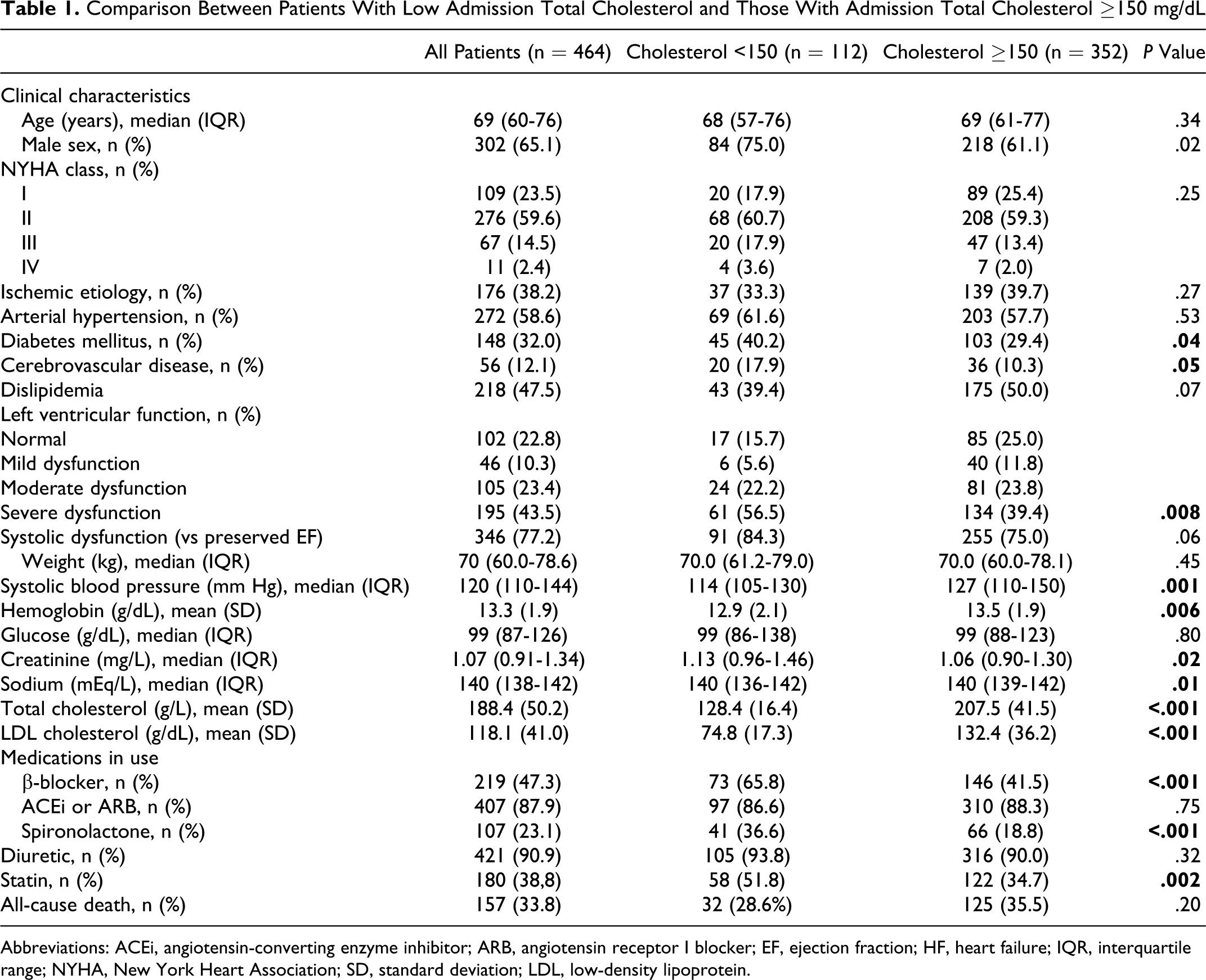
Abbreviations: ACEi, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor I blocker; EF, ejection fraction; HF, heart failure; IQR, interquartile range; NYHA, New York Heart Association; SD, standard deviation; LDL, low-density lipoprotein.
The Kaplan-Meier survival curves up to 5 years of patients cross-classified according to statin therapy and total cholesterol are shown in Figure 1. Nineteen (35.2%) of the 54 patients with low cholesterol level and not on statin compared to 9 (15.2%) of 58 on statin died during follow-up. Among patients with low cholesterol levels, those not on statin use—“naturally” low cholesterol levels—had a significantly worse survival than those taking statin therapy—pharmacologically induced low cholesterol (P = .02). The patients with total cholesterol of 150 mg/dL or higher represented a gray zone and in them statin therapy did not affect prognosis.
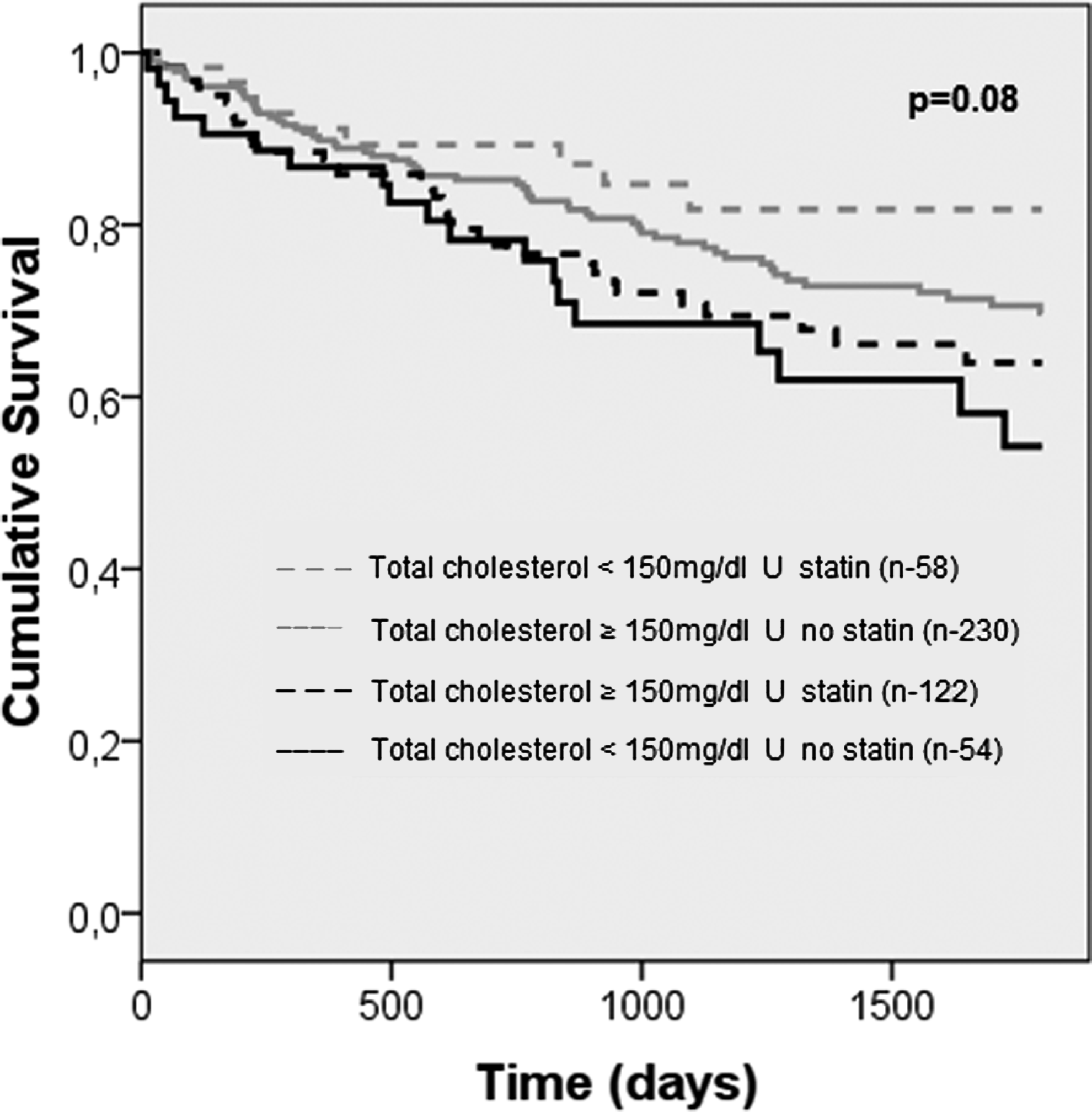
Kaplan-Meier survival curve according to the 4 groups created: patients with low total cholesterol on statin therapy; patients with low total cholesterol not on statin and patients with total cholesterol ≥150 mg/dL not on statin therapy and those with ≥150 mg/dL total cholesterol on statin therapy. Patients with low total cholesterol not on statin therapy had higher all-cause mortality than those with low cholesterol not on statin (P value = .03). Patients with total cholesterol ≥150 mg/dL represented a gray zone, whether or not on statin.
In the subgroup of patients with low cholesterol at admission, the comparison between those on and not on statin use, as well as the analysis of the variables possibly associated with all-cause death up to 5 years in a univariate approach are shown in Table 2. A similar analysis in the subgroup of patients with total cholesterol of at least 150 mg/dL, although not our study’s target population, is shown in Table 3.
Comparison Between Patients With Intrinsically Low Cholesterol and Those With Statin-Induced Low Cholesterol and Possible Variables Associated With Up to 5-Year All-Cause Death in the Subgroup of Patients With Total Cholesterol Below 150 mg/L
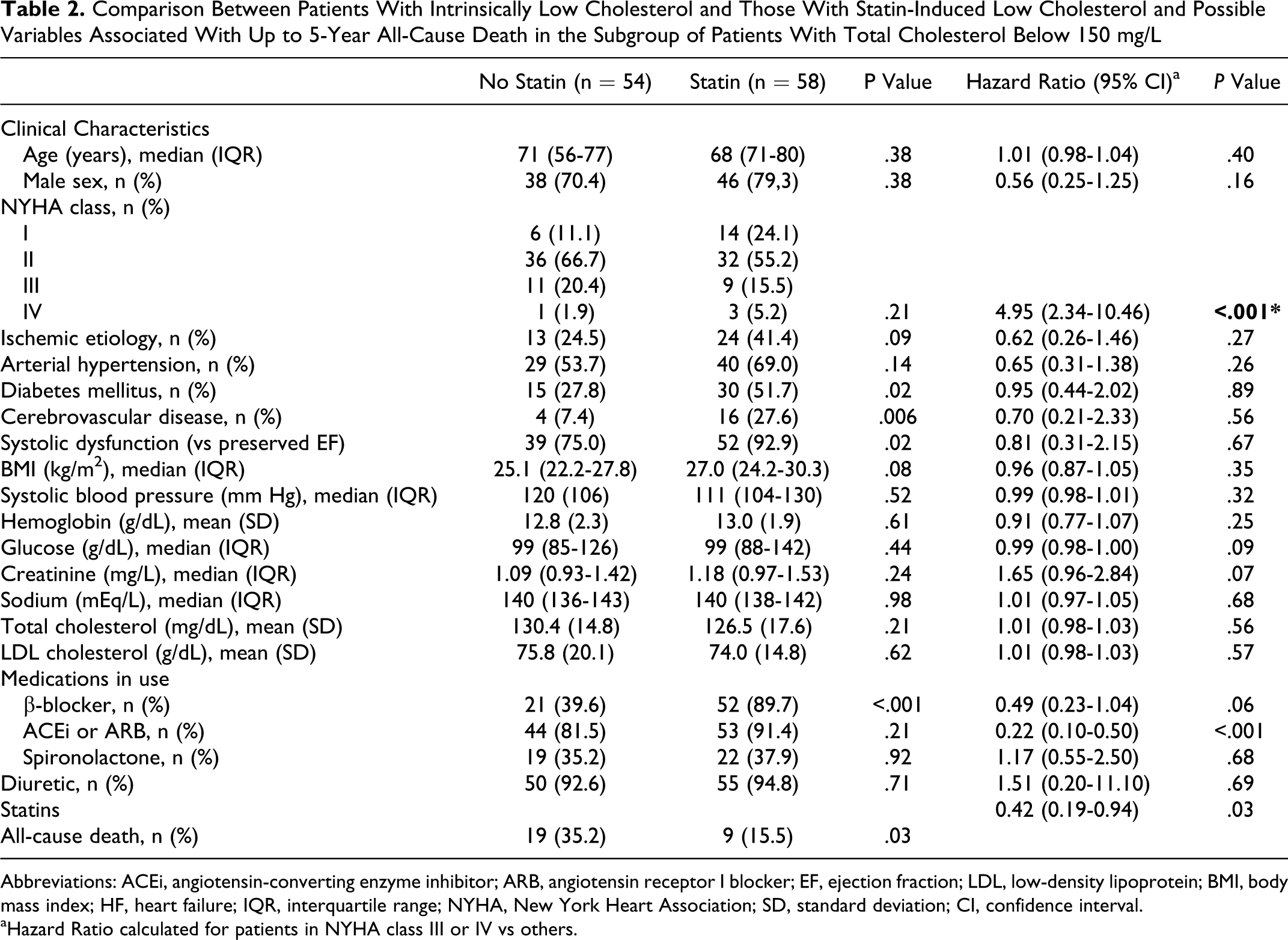
Abbreviations: ACEi, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor I blocker; EF, ejection fraction; LDL, low-density lipoprotein; BMI, body mass index; HF, heart failure; IQR, interquartile range; NYHA, New York Heart Association; SD, standard deviation; CI, confidence interval.
aHazard Ratio calculated for patients in NYHA class III or IV vs others.
Comparison Between Patients on and not on Statin With Total Admission Cholesterol 150 mg/dL or Above
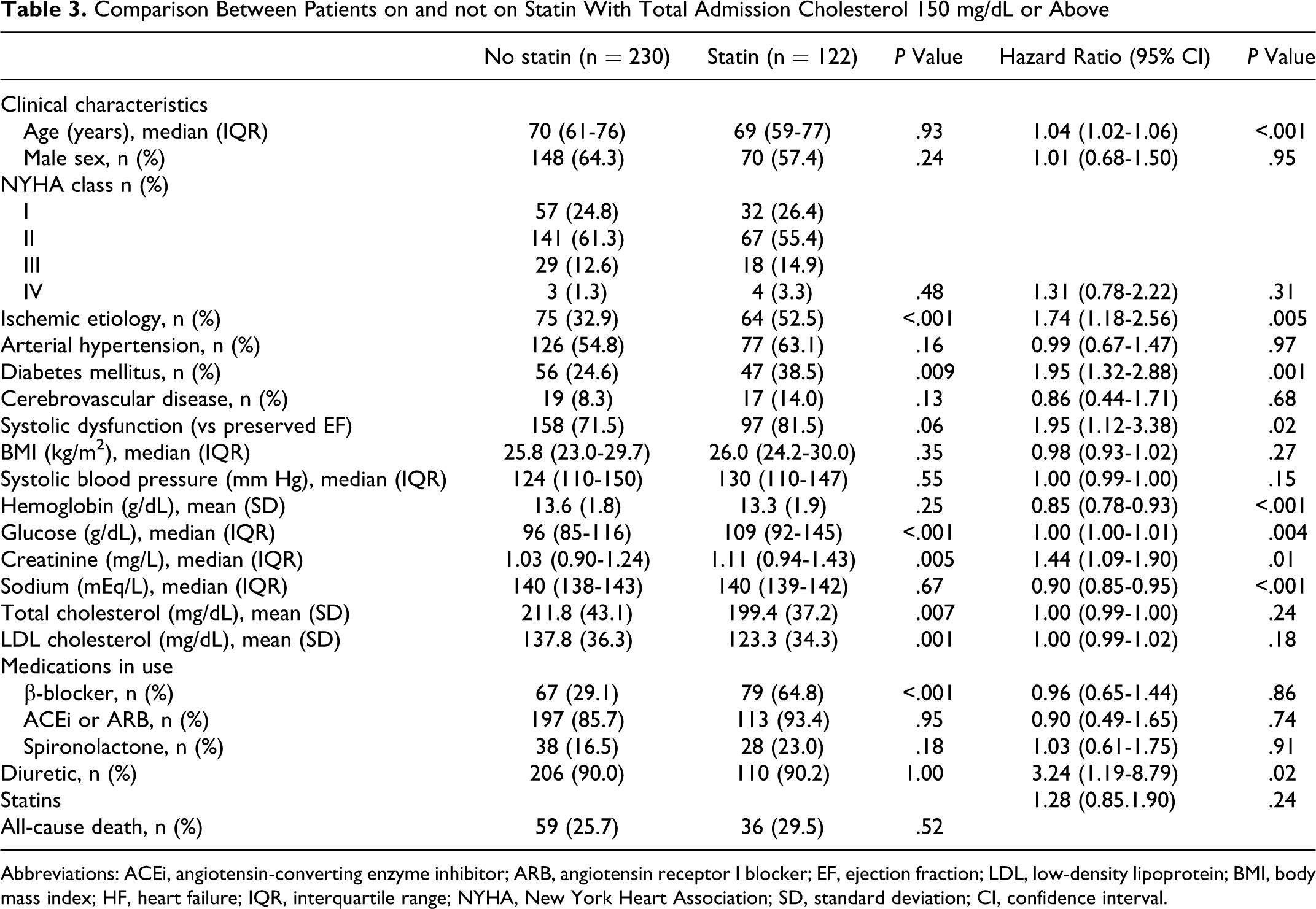
Abbreviations: ACEi, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor I blocker; EF, ejection fraction; LDL, low-density lipoprotein; BMI, body mass index; HF, heart failure; IQR, interquartile range; NYHA, New York Heart Association; SD, standard deviation; CI, confidence interval.
In this subgroup of 112 patients with low total cholesterol, like in the whole group whatever the admission cholesterol, those on statin therapy had higher prevalence of systolic HF and more associated comorbities. Patients with intrinsically low cholesterol were less optimized in terms of BB use. Variables impacting prognosis in a univariate approach were the NYHA class in the first appointment, the use of angiotensin-conversing enzyme inhibitor (ACEi) or angiotensin receptor blockers (ARBs) and statin use. Higher NYHA predicted worse outcome and ACEi or ARBs and statin use had a protective effect. There was also a trend for patients under BB use to have a better prognosis. Table 4 shows the multivariate model built based on these 4 variables. In the specific subgroup of patients with low cholesterol, statin therapy remained associated with all-cause death up to 5 years with a hazard ratio (HR) of 0.42 (0.18-0.93); meaning that the patients with an intrinsically low cholesterol had a HR of all-cause death up to 5 years of 2.38 (1.08-7.14) compared to those with pharmacologically induced low cholesterol. Patients with cholesterol ≥150 mg/dL have an intermediate prognosis as compared with the other groups. They are more likely to survive than patients with instrinsically low cholesterol, but less likely to survive than patients with pharmacologically induced low cholesterol, as shown in Figure 1.
Multivariate Analysis of Prognostic Predictors in Patient With Low Cholesterol
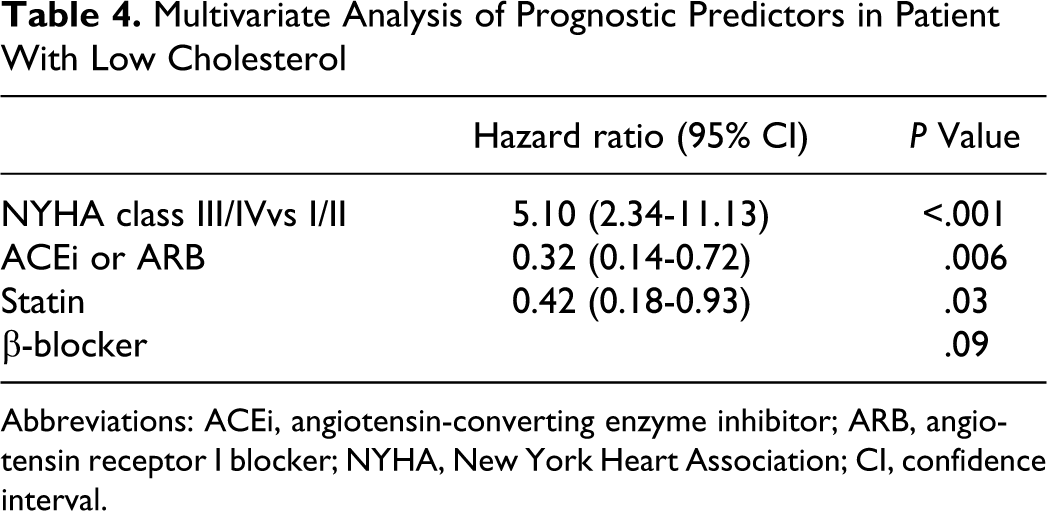
Abbreviations: ACEi, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor I blocker; NYHA, New York Heart Association; CI, confidence interval.
Discussion
In our HF patient population, an intrinsically low cholesterol was associated with a more than double risk of all-cause death up to 5 years when compared with patients with low cholesterol under statin therapy.
To the best of our knowledge, this is the first time that prognosis of patients with low cholesterol is compared between patients under statin therapy or not. Our results suggest that there might be no inferior limit of cholesterol beyond which statins should be suspended; and more importantly they do not argue against the use of statins in this specific patient population.
The role of statins is well established in the CAD setting; however, in HF doubts still persist. Physiological considerations and experimental animal models suggest both beneficial and harmful effects of statins in chronic HF. In small-scale studies and post hoc analyses, a neutral 13 and beneficial 14 effect of statins has been documented in HF and no detrimental effects have been reported. The rational for statin use in HF is in part the same as for CAD with the additional factor that CAD is one of the major diseases that ultimately progress to HF.
For the harmful effects of cholesterol-lowering statin induced in HF, 3 hypotheses have been suggested. The endotoxin lipoprotein hypothesis 15 sustains that lower levels of circulating cholesterol lead to an increase in endotoxins and an upregulation of the inflammatory response with its deleterious effects. The ubiquinone hypothesis 16 sustains that a decrease in cholesterol is followed by a decrease in the ubiquinone production and a consequent decrease in its antioxidant effect and adenosine triphosphate production. The hypothesis based on selenoprotein 17 also links decreased levels of cholesterol with a decrease in antioxidant pathways. The potential beneficial effects of statins are attributed to their pleiotropic anti-inflammatory properties, their counterregulatory actions on the renin–angiotensin–aldosterone and sympathetic systems as well as on the mechanisms of cardiac hypertrophy and fibrosis. 3
If this controversy rises in the whole pool of patients with HF, it is even more pertinent in the specific subgroup of patients with low serum cholesterol levels. In 1998, Vredevoe and colleagues 18 reported that low total cholesterol associated with increased mortality in advanced idiopathic chronic HF patients. Subsequent studies 19,20 showed higher cholesterol levels to be associated with decreased mortality in chronic HF, both ischemic and nonischemic. Growing evidence and interest in this “reverse epidemiology” phenomenon has brought to light the frailty and uncertainty of many aspects of HF pathophysiology and medical management.
The contradictory findings reported in the literature may, at least in part be explained by the difference between intrinsically low cholesterol levels and pharmacologically induced ones. To specifically address this unanswered issue, we tried to assess the prognostic meaning of a patient with HF to have an intrinsically low total serum cholesterol.
Differently from the large rosuvastatin studies in HF—CORONA 8 and GISSI HF 9 —that focused on statin, the focus of our observational study was not on statin, but on cholesterol. The main hypothesis of the large studies cited was that statin, no matter the baseline cholesterol or the cholesterol changes over time, would have beneficial effects in different HF populations. CORONA studied chronic systolic ischemic HF patients over 60 years old and GISSI studied chronic symptomatic HF whatever cause or ejection fraction in patients over 18 years old. We specifically studied the low total cholesterol population and took into account whether such low total cholesterol was or was not statin associated and tried to assess if these two groups had prognostic differences.
In our patient population with HF, an intrinsically low serum cholesterol doubled the risk of death up to 5 years when compared with patients with pharmacologically induced low cholesterol. This may mean that low cholesterol would not associate per se to a worse survival but probably represents a more global process of a somehow poor ill condition in that patients more often had chronic comorbidities—anemia, renal failure, wasting disease, and cardiac cachexia.
In line with our results, it is valid and sustainable to continue statin therapy in patients with HF with a preliminary indication for it, without concerning about the resulting low-cholesterol level obtained, because these patients had no prognostic worsening despite low cholesterol levels.
Our study has several limitations that must be noted. Its retrospective design has inherent and known associated problems, but in this particular study it might have at least had the benefit of not influencing the prescription pattern as would probably occur if it was prospective in nature. It is a single-center study and patients were recruited from a specialized HF clinic; this may limit extrapolation of the results especially for patients with HF treated in primary care centers. However, it is a medium- to long-term follow-up study of a relatively large number of patients with both systolic HF and HF with preserved ejection fraction. The number of patients used for the primary analysis of the prognostic impact of an intrinsically low cholesterol in patients with HF was small; however it was enough to show independent associations with all-cause mortality. A randomized clinical trial would be needed to prove our hypothesis rose from a retrospective, observational approach.
Conclusions
Patients with HF with intrinsically low cholesterol levels have a double risk of death up to 5 years than patients with pharmacologically induced low cholesterol.
Our results support that clinicians cannot limit the use of statins in their everyday clinical practice by concern of lowering the cholesterol levels.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.