
Abstract
Background:
The most plausible hypothesis for takotsubo cardiomyopathy (TCM) is a catecholamine surge. Direct administration of catecholamines or medications causing catecholamine surge is frequently used in clinical practice.
Methods:
A Medline/PubMed database search was conducted for case reports or series of drug-induced TCM. All reported cases of drug-induced TCM were systemically identified and analyzed.
Results:
We identified 157 cases of drug-induced TCM. Fifty-seven (36.3%) cases were related to the administration of exogenous catecholamines. In 50 (31.9%) other cases, there was potential adrenergic effect. This included drugs with adrenergic vasoconstriction properties (3.2%), hyperadrenergic state due to alcohol or opioid withdrawal (7.7%), inhibitors of catecholamine reuptake (14.7%), anaphylactic reaction that is accompanied by catecholamine release (3.2%), and psychological or somatic stress coinciding with the administration of a drug that was thought to be the culprit (3.2%). Overall, 68.2% of these drug-induced TCM cases were catecholamine related. In 14 (8.9%) cases, the likely etiology of cardiomyopathy was chemotherapy-induced coronary vasospasm.
Conclusion:
Our systematic review showed that over two-thirds of drug-induced TCM cases were due to direct or indirect catecholamine stimulation. The lowest effective dose and shortest duration of catecholamines should be utilized, and alternative therapies should be considered if feasible.
Keywords
Introduction
Transient reversible left ventricular systolic dysfunction is reported with increasing frequency. It may or may not be accompanied by regional wall motion abnormalities, in the form of apical ballooning or other forms. This condition is described in pheochromocytoma, a stress-induced cardiomyopathy, which develops as a result of emotional or somatic stress (takotsubo), and in subarachnoid hemorrhage, cerebrovascular accidents, or other neurologic conditions (neurogenic stunned myocardium). These conditions share the same morphologic substrate known as contraction band necrosis that is characterized by focal hypercontraction and lysis of small groups of myocardial cells, hypercontracted sarcomeres, dense eosinophilic transverse bands, and an interstitial mononuclear inflammatory response. 1 Patients often present with chest pain, heart failure symptoms, or both have electrocardiogram (ECG) changes (ST-T changes or QT prolongation) and mildly elevated cardiac enzymes (often disproportionately low relative to ECG changes). On imaging, both normally and abnormally moving segments have typical perfusion, 2 cardiac catheterization does not reveal critical stenoses of the coronary arteries, and left ventricular dysfunction often normalizes within few weeks. There are several theories on pathophysiology of takotsubo cardiomyopathy (TCM), but catecholamine surge is described as the most plausible mechanism. 3 Because catecholamines are commonly used in clinical practice, similar cardiac abnormality produced by adrenergic drugs could be an additional argument in favor of this pathophysiology, although β-receptor overstimulation may not be the only mechanism responsible for left ventricular systolic dysfunction. 4 In this article, we are systematically reviewing published case reports on drug-induced TCM.
Methods
A Medline/PubMed database search for case reports until October 2016 was performed using the keywords Takotsubo cardiomyopathy, Tako-tsubo cardiomyopathy or stress cardiomyopathy, and iatrogenic or drug induced. We also manually searched references in the articles, the PubMed search returned. All case reports were reviewed for the appropriate TCM diagnosis. Each case was further examined in order to identify the most likely underlying the cause of transient changes in myocardial contractility.
Results
A total 157 cases were reported in the literature as drug-induced TCM. The comprehensive list of the medications reported is summarized in the Tables 1 to 3. In 57 (36.3%) cases, TCM was related to the administration of exogenous catecholamines (Table 1). Epinephrine was the most common drug causing TCM (25 cases) followed by dobutamine (19 cases). In 50 (31.9%) other cases, there was potential adrenergic effect. This included drugs with direct sympathomimetic effect such as midodrine, adrenergic activation due to alcohol and opioid withdrawal, inhibitors of catecholamine reuptake, and anaphylactic reaction accompanied by catecholamine release (Table 2). Overall, 68.2% of cases of drug-induced TCM were catecholamine related. In other 14 (8.9%) cases, the likely etiology of cardiomyopathy was chemotherapy-induced coronary vasospasm (Table 4).
Exogenous Catecholamine-Induced Takotsubo-Induced Cardiomyopathy.
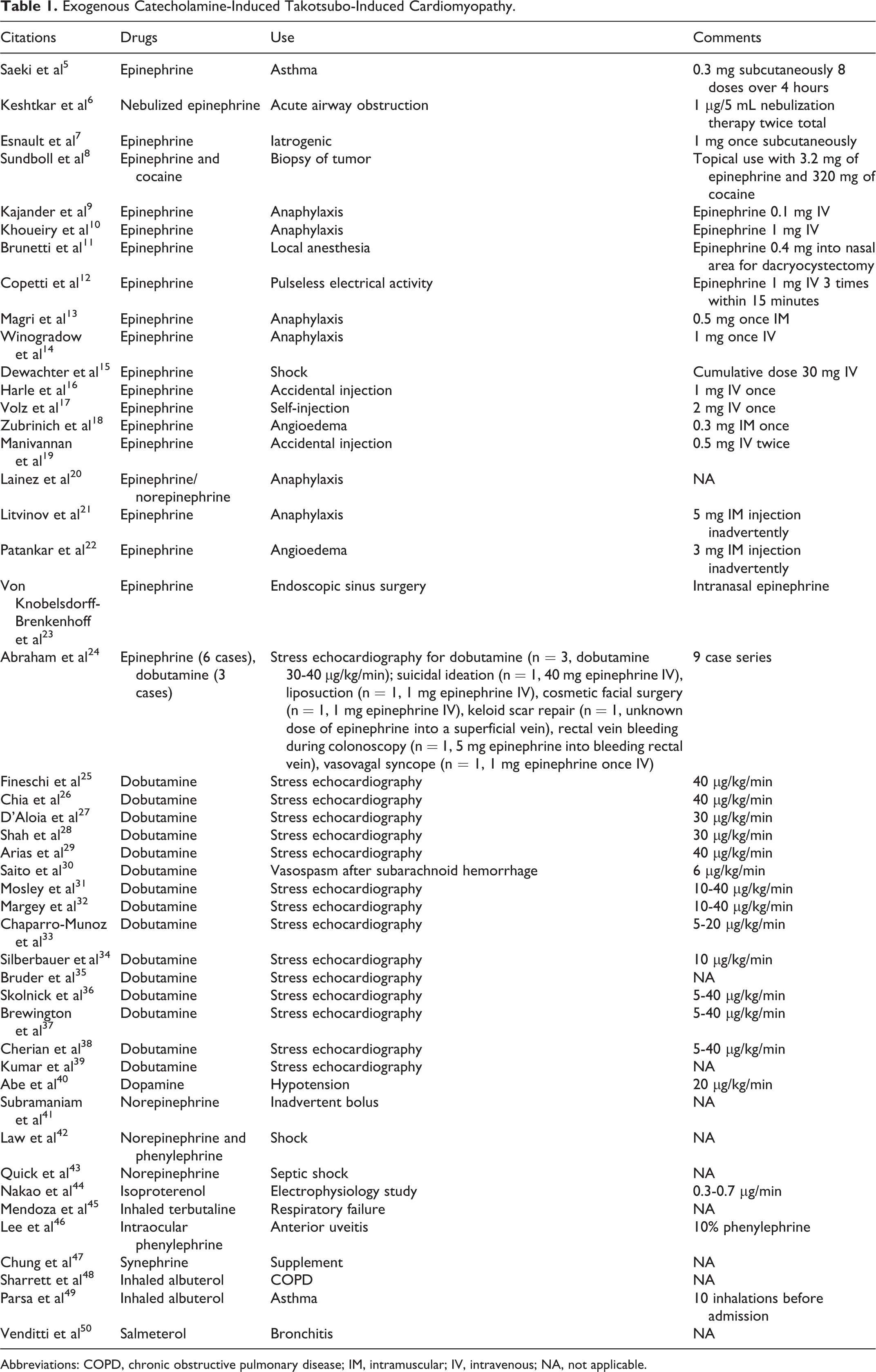
Abbreviations: COPD, chronic obstructive pulmonary disease; IM, intramuscular; IV, intravenous; NA, not applicable.
Other Adrenergic-Induced Takotsubo-Induced Cardiomyopathy (Reuptake Inhibitor, Anaphylaxis, Withdrawal, Adrenergic Vasopressors, and Psycho or Somatic Stress).
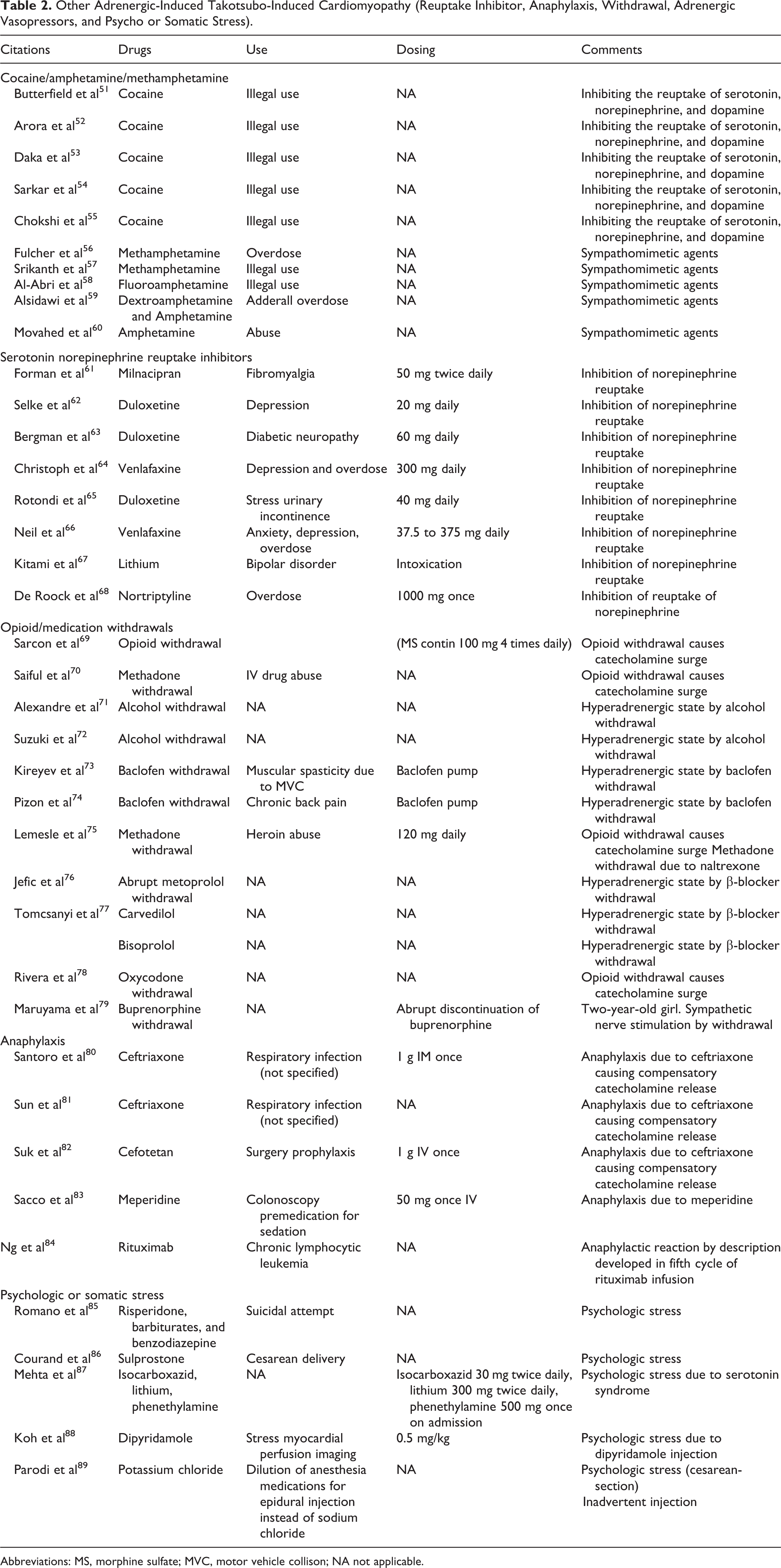
Abbreviations: MS, morphine sulfate; MVC, motor vehicle collison; NA not applicable.
Chemotherapy-Induced Coronary Vasospasm, Noncatecholamine Vasoconstrictors, or Unknown Mechanism.

Abbreviations: COPD, chronic obstructive pulmonary disease; FU, fluorouracil; GABA, gamma-aminobutyric acid; IL-2, interleukin 2; IV, intravenous; NA, not applicable; PDE, phosphodiesterase.
Etiology of Takotsubo-Induced Cardiomyopathy.

Discussion
Cardiodepressive effect of exogenous catecholamines was established long time ago. In 1994, Movahed et al described a dose-dependent reduction in left ventricular ejection fraction in dogs with left ventricular dilation and contraction band necrosis, with complete recovery in several days. 124 Only many years later, when TCM resulting from emotional or physical stress was reported, it became evident that these 2 phenomena may represent, in fact, the same condition. In this review, we collected the cases of drug-induced TCM and showed that 36.3% was due to exogenous catecholamines. Epinephrine was the most common drug associated with TCM followed by dobutamine.
Our systematic review supported that catecolamine surge is the most plausible mechanism for TCM based on 68.2% of drug-induced TCM cases being catecholamine related. This exaggerated sympathetic nerve stimulation theory was validated by the case series with 13 patients with stress cardiomyopathy using neurohumoral assessment. 3 It showed plasma levels of catecholamines (norepinephrine, epinephrine, and dopamine) on hospital stay 1 or 2 in 13 patients with TCM were 2 to 3 times higher than those in 7 control patients with myocardial infarction. By hospital stay 7, 8, or 9, plasma levels of catecholamines went down to one-third to one-half of the peak values. The mean left ventricular ejection fraction on hospital stay 1 was 0.20 but by hospital stay 3, 4, 5, 6, or 7, ejection fraction improved to 0.45. It supports that catecholamine surge is probably central to the mechanism of TCM.
Drugs with direct sympathomimetic effect like midodrine, 107 ergotamine tartrate, 104 ergonovine, 105 oxymetazoline, 112 and pseudoephedrine 108 are also reported causes of drug-induced TCM. In particular, ergotamine, which is structurally similar to endogenous catecholamines and indolamines, exerts some α-adrenergic effects. 104 Midodrine is an α-adrenergic receptor agonist and can also trigger takotsubo syndrome. 107 This mechanism also applies to pseudoephedrine that directly stimulates the adrenergic receptors. 108 Oxymetazoline is a nasal decongestant–stimulating α-receptors. 112 Also, inhibitors of catecholamine reuptake/sympathomimetic amines could cause drug-induced TCM. They include cocaine (5 cases), 51 -54 nortriptyline, 68 lithium, 67,87 and 11 others with the most common drug being venlafaxine (7 cases). 64,66 Takotsubo in the setting of lithium intoxication can be also explained by the fact that lithium causes catecholamine overload by inhibiting the reuptake of serotonin and norepinephrine. 67 In another case, the patient was treated with lithium in combination with phenethylamine that is known to release endogenous catecholamines. 87 Phentermine is an amphetamine derivative used as an appetite suppressant, which is thought to be a sympathomimetic amines that stimulate the release of norepinephrine and dopamine from the storage sites in the presynaptic nerve terminals. 119 Other catecholamine-related causes included indirect adrenergic effects, including parasympathetic block (2 cases), 117,122 sudden withdrawal of β-blockers (3 cases), 76,77 anaphylactic reactions (5 cases), 81 -84,118 withdrawal of opioids (5 cases), 69,70,75,78,79 or alcohol (2 cases). 71,125 Opioid withdrawal is known to cause hyperadrenergic state that leads to catecholamine surge and increased β-receptor sensitivity and subsequently myocardial stunning. Alcohol withdrawal is also accompanied by catecholamine release (in extreme causing delirium tremens). Psychologic or somatic stress was believed to be the catecholamine-related cause of TCM in 8 cases. 121 In 3 of these cases, the interpretations were that 1 patient had suicidal attempt, 85 and another 2 TCM cases were believed to be due to cesarean section. 86,89
Although the majority of drug-induced TCM cases was explainable with catecholamine surge theory, a couple of researches showed that the majority of patients had normal catecholamine levels in patients with TCM. 126 -128 Y-Hassan 126 showed that 89% of patients had normal epinephrine level, and 52% of patients had normal norepinephrine levels. Only 3 of 33 patients had remarkably elevated catecholamine and metabolite levels. Another study also reported that all 6 patients had normal epinephrine levels; 3 patients had normal norepinephrine levels, and the other 3 patients had mild elevation of norepinephrine level. 127 Yoshioka et al also found that mild elevation in catecholamines was not associated with TCM. 128 These results challenged catecholamine surge theory and raised the possibility that other theories may contribute to the development of TCM.
In 17 (11%) cases, the likely etiology of cardiomyopathy was coronary spasm, and in 22 (14.3%) cases, we were unable to explain the origin of TCM. Four capecitabine cases and ten 5-fluorouracil (FU) cases are reported in the literature database as TCM by coronary spasm (Table 3). Zolmitriptan, which increases serotonin release resulting in coronary vasospasm 106,109 and bromocriptine, 111 is also reported to cause vasospasm. In this latter group, chemotherapy-induced takotsubo in the setting of malignancy was the most common. Unlike cases with catecholamine infusions, chemotherapy-induced cases of TCM appear much less uniform and convincing (Table 3).
5-fluorouracil and its prodrug capecitabine are used for the treatment of colorectal, breast, and brain cancers. However, cardiotoxicity is reported in 1% to 18% of patients. 95 Cardiac adverse effects of 5-FU include ischemic events (ST-segment changes) with or without angina and sometimes myocardial infarction. A dose-dependent arterial vasoconstriction was demonstrated in isolated rabbit aortic rings following FU administration. Also, plasma levels of endothelin, a strong vasoconstrictor, are elevated in patients with cancer treated with FU and particularly in those developing cardiotoxicity. 129 Currently, 5 capecitabine cases and eight 5-FU cases are reported in the literature database as TCM (Table 3). The exact pathogenesis of capecitabine or 5-FU-induced takotsubo disease is unknown, but there are a couple of potential mechanisms: coronary vasospasm and direct drug/metabolite-induced toxic action on myocytes. 90 All of cases developed the TCM within 72 hours after the therapy, and in each case, Ejection fraction (EF) recovered to normal within 1 to 2 weeks. Of note, all of capecitabine cases did not have the typical apical ballooning feature in echocardiogram. 90 We cannot exclude that with the similarity of clinical presentation, 5-FU-induced TCM represents some different phenomenon.
Although multiple cases are reported in catecholamine-related literature, there are often a single case report on a certain agent in chemotherapy-induced takotsubo-like syndrome. 130 Millions of women receive trastuzumab, yet there is only 1 case report on trastuzumab-induced TCM. 131 In some cases, repeat cardiac imaging to prove reversal of wall motion abnormality was never performed, and the diagnosis of TCM is therefore not definitive. Moreover, coronary angiography was sometimes delayed, and acute coronary event with spontaneous reperfusion could not be excluded. 131
Also, in chemotherapy-related cases, takotsubo developed in the setting of chemotherapy for malignancy, a stressful situation by itself, and occurrence of such a reaction after the administration of chemotherapeutic agent could be coincidental. 132 When takotsubo developed during the treatment for newly diagnosed acute leukemia 130 or metastatic melanoma 133 and only occurred after the fourth dose of the culprit medication 130 or after 8 weeks of daily intake of pazopanib 134 or even after 4 years of sunitinib exposure, 135 stress can indeed play a greater role than the particular agent.
Other kinds of chemotherapy may have vasospastic effects that create same pattern of cardiac damage as takotsubo. Combretastatin induces cytoskeletal changes in endothelial cells, increases vascular permeability, and inhibits blood flow, causing endothelial cell apoptosis. 136 Vasoconstriction by vasopressin in a patient with already elevated catecholamines levels due to hepatorenal syndrome was also reported to cause TCM. 110
Finally, in number of cases, the role of the pharmacologic agents in the origin of TCM is unclear. 137 Ibuprofen was called a cause of TCM, while the patient described in the case suffered cardiac arrest and underwent extensive cardiopulmonary resuscitation with massive doses of epinephrine. 113 Only handful of cases remain unexplained: androgenic steroids in the setting of hypothyroidism, 114 interleukin 2, 115 entacapone, 116 influenza vaccine, 118 dipyridamole, 88 and convulsions and takotsubo in a 97-year-old patient after levofloxacin and a nonsteroidal anti-inflammatory drug loxoprofen. 123
Conclusion
Our systematic review showed that 68.2% of drug-induced TCM cases were due to direct or indirect catecholamine stimulation. The most common medication associated with drug-induced TCM was epinephrine followed by dobutamine. This further strengthens the argument that excess of catecholamines is the underlying mechanism of TCM.
Footnotes
Acknowledgments
The authors want to thank Tracy Macaulay and Jessica McManus for the contributions to review this manuscript. Without the support, this manuscript would not have been completed.
Authors Contributions
Kido contributed to conception and design; acquisition, analysis, and interpretation; drafted the manuscript; critically revised the manuscript; and gave final approval. Guglin contributed to design, acquisition and analysis, drafted the manuscript, critically revised the manuscript, and gave final approval. Both authors agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.