
Abstract
The novel combination sacubitril/valsartan represents a new therapeutic approach in the management of heart failure. With the simultaneous blockage of the enzyme neprilysin (by sacubitril) and angiotensin II receptors (by valsartan), this combination reduces the degradation of natriuretic peptides and other counterregulatory peptide systems while avoiding the deleterious effect of angiotensin II receptors activation and thereby encompasses a beneficial impact of 2 important neurohormonal pathways activated in heart failure. As opposed to previously tested neprilysin inhibitors, sacubitril/valsartan represents a more effective method in reducing morbidity and mortality in heart failure, while preserving a safety profile comparable to well-established, standard, angiotensin-converting enzyme inhibitor’s therapy.
Introduction
In a large, multicenter, randomized, double-blind study conducted in patients with heart failure (HF) having reduced ejection function, the new agent sacubitril/valsartan (LCZ696, Entresto; Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA) was found superior to standard therapy with enalapril in improving outcomes. 1 Sacubitril/valsartan represents the combination of angiotensin II receptor blockade and neprilysin inhibition. Here, we describe its mechanism of action, pharmacodynamics and pharmacokinetics, indications, side effects, risks, and contraindications. In addition, we review completed and ongoing contemporary studies shedding more light on the patient population that might benefit most from sacubitril/valsartan use.
Neurohormonal Changes Caused by HF
Heart failure triggers a series of compensatory mechanisms including significant neurohormonal changes. These changes, however, are not straightforward and comprise of simultaneous detrimental and beneficial components that affect the clinical manifestations of this disease.
The activation of the renin–angiotensin–aldosterone pathway causes the cleavage of the nonactive precursor, angiotensinogen, by the enzyme renin, to produce angiotensin I, which in turn transforms into angiotensin II, mostly by the action of angiotensin-converting enzyme (ACE). Although the binding of angiotensin II to the less abundant, angiotensin type 2 receptor stimulates vasodilation, natriuresis, inhibition of cell growth, and bradykinin release, 2 the activation of the dominant angiotensin II type 1 receptor produces numerous deleterious effects, including significant vasoconstriction, increased myocardial hypertrophy and fibrosis, increased vasopressin secretion, increased renal resorption of water and sodium, and also direct stimulation of the adrenal cortex to secrete aldosterone, which further aggravates myocardial fibrosis and sodium retention. 3 On the other hand, other adaptive neurohormonal mechanisms triggered by HF were shown to produce beneficial effects. Atrial and B-type natriuretic peptides (NPs) are neurohormones secreted in response to high tension in cardiac chambers. These peptides exert their physiological function primarily through their binding to NP receptor type A and the consequent production of cyclic guanosine monophosphate (cGMP) by the activation of guanylate cyclase. 4 Through this mechanism, NPs produce vasodilation, increase natriuresis, ameliorate myocardial fibrosis (by inhibiting the growth of fibroblasts and vascular smooth muscle cells), and reduce the secretion of renin and aldosterone as well as catecholamines. 5 Unlike atrial NP (ANP) and brain NP (BNP), the principle source of C-type NP is the vascular endothelium. It performs its function in an endocrine or paracrine manner through binding to the membrane guanylyl cyclase NP receptor B or by signaling through the nonenzyme NP receptor C and promotes vasorelaxation. 6,7 Adrenomedullin, a ubiquitous neurohormone primarily secreted by endothelial cells, was shown to have vasodilatory effect and pro-natriuretic effect and was also found to blunt the secretion of aldosterone in HF models. 8 A more complex player, bradykinin, also participates in HF compensatory mechanisms. The activation of the kallikrein–kinin system, responsible for bradykinin production, can be triggered by the elevation in cytokine levels or the increased levels of aldosterone, both present in HF. This activation produces an elevation in bradykinin levels, which were found to positively affect not only vasodilation and myocardial relaxation but also contractility and myocardial performance. 9 The activation of the B2 receptor by bradykinin might, however, cause an increased tissue permeability and may trigger angioedema. 10
Natriuretic Peptides in Clinical Use
The administration of exogenous neurohormones, mainly NPs, has been shown to have a significant vasodilatory effect leading to beneficial hemodynamic impact in patients with HF. Since these drugs are limited to intravenous approach, studies in the last 2 decades have focused on the attempt to increase endogenous NPs levels by blocking their degradation.
The neutral endopeptidase, neprilysin, is a membrane-bound metalloproteinase widely spread in different tissues including the myocardium, the kidneys, the brain, the vascular endothelium, and the immune system. 11 Neprilysin serves as the chief enzyme not only responsible for the degradation of NPs, adrenomedullin, and bradykinin but also for the degradation of angiotensin II and endothelin. 11 As a result, its action and vice versa, its blockade, produce a complex reaction with mixed effects.
In 1989, Northridge et al reported on the development of the “atriopeptidase” inhibitor, UK 69578, which selectively inhibited the degradation of ANP by kidney endopeptidase in a dog model and was also shown to increase natriuresis and to reduce pulmonary artery wedge pressures in 6 patients with HF who participated in this study. 12 Further studies with the endopeptidase inhibitor, candoxatril, showed, however, a mixed pattern of results. In the acute phase, the drug was found to increase NPs levels and improve hemodynamic profile. 13 Extended exposure to candoxatril showed improved exercise capacity in some patients with HF, 14 while negatively affecting systemic vascular resistance and cardiac index in others. 15 This deleterious hemodynamic effect was attributed to the observed increase in angiotensin II, aldosterone, and catecholamine levels after prolonged therapy with this drug. 16 These results turned the spotlight to omapatrilat, a molecule that acts as both neprilysin inhibitor and ACE inhibitor, and hence, it was expected to capture the favorable effect of neprilysin inhibition (increased NPs, adrenomedullin, and bradykinin levels) while preventing the accumulation of angiotensin II. 17 It was initially shown that omapatrilat improved left ventricular geometry, reduced lung congestion, increased urinary NP excretion, and prolonged survival in animal models of HF, 18 suggesting that this dual blockage produces a greater degree of improvement compared to ACE inhibition alone. However, when tested in clinical trials in patients with chronic HF, omapatrilat failed to show the anticipated advantage over the ACE inhibitor, enalapril. 19 A result that was attributed to the lower dosage and once-daily regimen of omapatrilat therapy in that study. More importantly, as a result of this double blockade of degradation of bradykinin, in addition to the inhibition of aminopeptidase P, another bradykinin degrading enzyme, 20 omapatrilat significantly increased the risk of angioedema. 21
These data showed that the dual inhibition of neprilysin and ACE acted as a 2-edged sword: increasing the levels of protective neurohormones on one side, while placing the patients at an increased risk of angioedema on the other. Nevertheless, the need to counteract the rise in angiotensin II levels, as a result of neprilysin inhibition, was still present and triggered the investigation into the combination of neprilysin inhibition with a compound less likely to increase bradykinin levels, angiotensin receptor blockers (ARBs). The results of these studies led to the development of LCZ696, a combination of the neprilysin inhibitor, AHU377 (sacubitril), with the ARB, valsartan 22 (Figure 1). Further research showed that sacubitril/valsartan was at least as effective as omapatrilat in blood pressure (BP) reduction but without ensuing the increased risk of angioedema. 23,24

The effect of sacubitril/valsartan on the renin–angiotensin system and the natriuretic peptide system. Adopted with permission from Vardeny O, et al. JACC Heart Fail. 2014;2(6):663–670.
The PARADIGM-HF Trial
The result of these accumulating data was the largest study conducted to date in HF, the Prospective Comparison of ARNI [Angiotensin Receptor-Neprilysin Inhibitor] with ACEI [Angiotensin-Converting-Enzyme Inhibitor] to Determine Impact on Global Mortality and Morbidity in Heart Failure (PARADIGM-HF) trial. 1 In this study, 8442 symptomatic (New York Heart Association [NYHA] class II-IV) patients with HF having ejection fraction (EF) below 40% (changed to 35% later in the trial) and elevated levels of NPs (BNP >100 pg/mL or NT-proBNP >400 pg/mL, BNP >150 pg/mL, or N-terminal proBNP (NT-proBNP) >600 pg/mL, for patients with and without a history of HF hospitalization, respectively) were randomized to treatment with sacubitril/valsartan or the ACE inhibitor, enalapril. Mean age was 64 ± 11 years, over 70% of the study patients were males, and around 60% had an ischemic cardiomyopathy. A majority of the patients were treated with other evidence-based HF drug therapies (>90% on β-blockers therapy, >50% on mineralocorticoid receptor antagonists). However, rate of the use of implantable defibrillators and cardiac resynchronization therapy was low.
Only patients who were treated with ACE inhibitors or ARBs prior to the study and maintained systolic BP of ≥100 mm Hg were eligible for the study. In addition, all participants were required to undergo a single-blind, run-in period in which they received enalapril 10 mg twice a day for 2 weeks, then sacubitril/valsartan 100 mg twice a day for 2 weeks, and then 200 mg twice a day for another 2 to 4 weeks. Patients who maintained systolic BP of ≥95 mm Hg at the end of the run-in period underwent double-blind randomization to enalapril 10 mg twice a day versus sacubitril/valsartan 200 mg twice a day (mean systolic BP at study entrance was around 122 mm Hg). Of the 10 513 patients who entered the enalapril run-in phase, 1102 discontinued the study, and of the 9419 patients who entered the sacubitril/valsartan run-in phase, 977 discontinued the study. Reasons for discontinuation of therapy on both arms are shown in Table 1. The study was prematurely stopped after a median follow-up of 27 months due to compelling beneficial effect of sacubitril/valsartan. The primary outcome (death from cardiovascular causes or hospitalization for HF) occurred in 21.8% and 26.5% of the patients in the sacubitril/valsartan and enalapril group, respectively (P < .001), conferring to a relative risk reduction of 20%. Overall death occurred in 17% of the patients treated with sacubitril/valsartan during the study period compared to 19.8% of the enalapril-treated patients (P < .001). Sacubitril/valsartan also reduced cardiovascular mortality from 16.5% to 13.3% (P < .001; relative risk reduction of 16% and 20% for all-cause mortality and cardiovascular mortality, respectively). In addition, compared to the enalapril arm, sacubitril/valsartan-treated patients had a 21% lower rate of hospital admissions (P < .001) and a 30% lower rate of emergency department visits (P = .017). The only adverse event found to be more prevalent in the sacubitril/valsartan arm compared to the enalapril arm was systolic BP below 90 mm Hg (2.7% and 1.4%, respectively, P < .001) and symptomatic hypotension (14% compared to 9.2%, respectively, P < .001), but these events rarely required the discontinuation of therapy (<1% in both arms). Angioedema was reported in 19 patients in the sacubitril/valsartan group and in 10 patients in the enalapril group, the number of patients hospitalized was 3 and 1, respectively, and none of the patients had airway compromise. Other side effects (with higher incidence in patients treated with enalapril) were cough (14% vs 11%; P < .001) and increase in serum creatinine to >2.5 mg/dL (4.5% vs 3.3%; P = .007). Incidence of hyperkalemia was comparable between the 2 groups (17% and 16%, respectively).
Reasons for Discontinuation of Study Drug During the Run-In Phase of the PARADIGM-HF Trial.
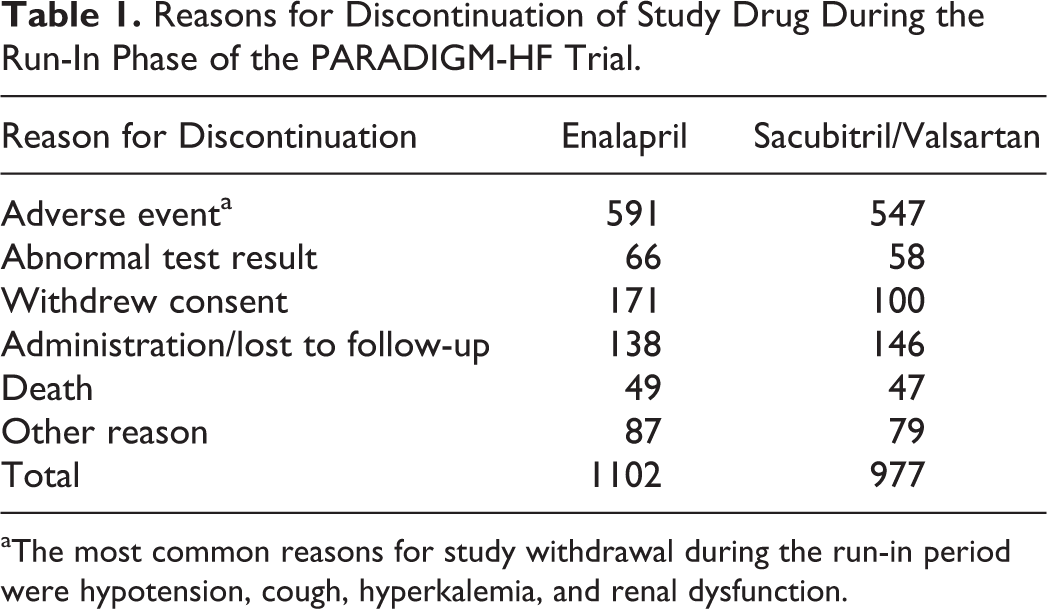
aThe most common reasons for study withdrawal during the run-in period were hypotension, cough, hyperkalemia, and renal dysfunction.
The PARADIGM-HF study has clearly demonstrated the superiority of sacubitril/valsartan combination compared to the well-established, standard HF therapy with enalapril. At the same time, however, there are certain areas of equipoise that need to be taken into consideration when analyzing the results of the trial. Patients with a recent acute coronary syndrome, history of severe pulmonary disease, or hepatic impairment were excluded from the study. The exclusion of patients who did not tolerate sacubitril/valsartan in the single-blind run-in period, probably, resulted in lower rates of side effects during the double-blind period. The underrepresentation of NYHA class IV patients, African Americans, and patients with implantable cardioverter defibrillators and resynchronization devices in the study limits the ability of drawing conclusions regarding the efficacy and safety of the drug in these groups. Similarly, considering the relatively preserved systolic BP in the study population and the fact that only 21% of the patients had an initial systolic BP of <110 mm Hg, the trial results may not be applicable to a significant proportion of severe HF patients who tend to have lower BP. The relatively low incidence of angioedema seen in this trial (0.1%-0.2% as opposed to 0.5%-2% in previous reports) can also be attributed to the exclusion of patients who may have experienced this adverse event during the run-in period and to the low (5%) representation of African American patients, a population at higher risk for angioedema. Finally, the choice of enalapril, rather than a more frequently used once-daily ACE inhibitors, as a comparator in the trial might be questionable, however, enalapril was used as a study drug in many important HF trials 25,26 and as such is considered a well-validated standard of care.
Pharmacodynamics and Pharmacokinetics
Sacubitril/valsartan (LCZ696) contains a complex comprised of sacubitril, valsartan, sodium cations, and water in a ratio of 1:1:3:2.5, respectively. 22 Following oral ingestion, the complex breaks down to valsartan and to the neprilysin inhibitor prodrug, AHU377, which further metabolizes, by nonspecific esterases, to the active neprilysin inhibitor, sacubitrilat (LBQ657). When administered with food, there is a mild decrease in the exposure to valsartan levels, which was found to have no clinical impact, and therefore, sacubitril/valsartan can be administered with food. 22 Cytochrome P450 enzyme-mediated metabolism of the drug is minimal. The plasma half-life of LBQ657 and valsartan is 11.5 and 9.9 hours, respectively. One-half to two-thirds of sacubitril (mostly as LBQ657) is eliminated through urine and up to one-half is eliminated in feces, whereas almost 90% of valsartan is excreted in feces and about 10% in urine. 22 Both sacubitril and valsartan have high volumes of distribution (103 and 75 L, respectively), since both of them are highly bound to plasma proteins (>95%). 27 As discussed later, LBQ657 crosses the blood–brain barrier and it can be found in small levels in the cerebrospinal fluid (0.28% of plasma levels). 27
The target daily dose of sacubitril/valsartan in the PARADIGM-HF study (400 mg) represents 97 mg of sacubitril and 103 mg of valsartan administered twice a day. In open-labeled studies, conducted in healthy participants and in patients with HF, this dose of valsartan was shown to be comparable to a 320 mg daily dose of valsartan, a phenomenon attributed to the higher bioavailability of anionic-form valsartan in this formula as compared to other existing formulas. 22
Kidney Effect
In animal models of renal failure, treatment with omapatrilat or with candoxatril led to increased tubular ANP, increased renal vasodilation, amelioration of proteinuria, and regression in glomerulosclerosis. 28,29 In human trial, omapatrilat was found to delay the deterioration in renal function compared to ACE inhibition alone (6.8% vs 10.1%, respectively). 19
Patients with severely impaired renal function (estimated glomerular filtration rate [eGFR] <30 mL/min/1.73 m2) were excluded from the PARADIGM-HF trial. However, deterioration in renal function (defined as the development of end-stage renal disease, a decrease of more than 50% from baseline eGFR, or a decrease in eGFR of more than 30 mL/min/1.73 m2 to a less than 60 mL/min/1.73 m2) occurred to similar extent in both treatment arms (2.2% and 2.6% in the sacubitril/valsartan arm and the enalapril arm, respectively, P = .28). 1 It should be noted that in a substudy of the prospective comparison of ARNI with ARB on management of heart failure with preserved ejection fraction (PARAMOUNT) trial (investigating the effect of sacubitril/valsartan in patients having HF with preserved ejection fraction [HFpEF]), 36 weeks of treatment with sacubitril/valsartan compared to valsartan alone delayed the deterioration in eGFR (−1.6 mL/min/1.73 m2 vs −5.2 mL/min/1.73 m2, respectively; P = .007). 30
A small-scale study published in 2016 investigated the pharmacokinetics of sacubitril/valsartan in mild (eGFR: 50-80 mL/min/1.73 m2), moderate (eGFR: 30-50 mL/min/1.73 m2), and severe (eGFR <30 mL/min/1.73 m2) renal dysfunction, compared to normal controls, following 1 and 5 days of treatment. 31 Sacubitril and valsartan levels were similar across the different kidney function groups, however, the plasma half-life of the active neprilysin inhibitor, sacubitrilat, was prolonged in parallel with the severity of renal dysfunction (12, 21.1, 23.7, and 38.5 hours in the normal, mild, moderate, and severe renal dysfunction group, respectively). 31 Current recommendations suggest starting sacubitril/valsartan at a dose of 24/26 mg in patients with eGFR<30 mL/min/1.73 m2 and dose increment according to patient’s clinical condition. 27
Effect on Biomarkers
An important tool in the surveillance of patients with HF is the monitoring of NP levels. In the case of patients treated with sacubitril/valsartan, a clinician must take into consideration the effect of neprilysin inhibition, which might produce an elevation in ANP and BNP levels. In the PARADIGM-HF trial, a minor reduction in the levels of both BNP and NT-proBNP was shown in the enalapril-treated group, whereas an elevation in the levels of BNP was observed within the first month of treatment with sacubitril/valsartan and was maintained throughout an 8-month surveillance period. 32 However, since NT-proBNP is not degraded by neprilysin, the levels of NT-proBNP were significantly reduced within the first month of treatment with sacubitril/valsartan and were maintained during the follow-up period compared to enalapril treatment. 32 Similarly, the levels of cGMP, a vasodilating second messenger influenced by the levels of NPs, were significantly elevated in the sacubitril/valsartan-treated group. These findings serve to demonstrate the beneficial effect of sacubitril/valsartan on vasodilation and reduced myocardial wall stress in patients with HF. A current approach toward the implementation of NPs measurement in patients with HF treated with sacubitril/valsartan would be to follow NT-proBNP levels rather than BNP as an indicator for clinical stability.
Ocular and Central Nervous System
Given the abundance of neprilysin in bodily tissues and its ample effect on many protein end products, an issue for future consideration and surveillance is the neprilysin-blocking effect on the accumulation of amyloid β (Aβ) peptide. Both animal and human studies have shown that variations in Aβ homeostasis either due to increased production or decreased clearance were associated with accelerated amyloid depositions in both brain and eye tissues and were related to the development of Alzheimer disease and age-related macular degeneration. 33,34 The importance of neprilysin in these diseases processes was demonstrated in animal models that showed acceleration or amelioration of neurological and ocular injuries with the disruption or overexpression of neprilysin, respectively. 33 Accordingly, concerns were raised as to the potential risks of neprilysin inhibition treatment in humans. 35 Studies attempting to address this issue were done in both nonhuman primates and in healthy human volunteers and showed that short-term (14 days) treatment with sacubitril/valsartan caused a detectable increment in the levels of sacubitrilat in the participants’ cerebrospinal fluid, along with an elevation in the levels of the soluble Aβ isoform but not the levels of the aggregable one. 36 Given these studies have not fully dismissed all concerns, the Food and Drug Administration (FDA) has asked the drug manufacturer to conduct a comprehensive neurocognitive and neuroimaging, multicenter, double-blind study to evaluate the neurological effect of sacubitril/valsartan as compared to valsartan alone in patients with HFpEF. 37 It should be mentioned, however, that though not specifically prespecified, a deterioration in cognitive function was not reported in the sacubitril/valsartan arm during the 27-month follow-up of the PARADIGM-HF trial. 1
Indications and Warnings of FDA
Sacubitril/valsartan is indicated to reduce the risk of cardiovascular death and HF hospitalizations in patients with chronic NYHA class II to IV HF and reduced EF. 27 The product information states that sacubitril/valsartan is usually used in patients receiving other therapies for HF, in place of an ACE inhibitor or ARB.
Sacubitril/valsartan contains a boxed warning for fetal toxicity, with discontinuation of the product recommended as soon as possible once pregnancy is detected. Sacubitril/valsartan is also contraindicated in patients with a history of previous hypersensitivity to the drug or angioedema with an ACE inhibitor or ARB. Concomitant use of sacubitril/valsartan with an ACE inhibitor is also contraindicated, and when switching from ACE inhibitor, it is recommended that sacubitril/valsartan not be initiated within 36 hours from discontinuation of ACE inhibitor. Based on the results of the aliskiren trial in Type 2 diabetes using cardiorenal endpoints (ALTITUDE) study, 38 the concomitant use of sacubitril/valsartan and the renin inhibitor, aliskiren, is not recommended in patients with diabetes or eGFR <60 mL/min/1.73 m2 due to the increased risk of hyperkalemia and hypotension.
Dosing and Titration
Recommended starting dose depends on previous doses of ACE inhibitors or ARBs and renal function. In patients taking a dose of ≥10 mg/d of enalapril or equivalent dose of other ACE inhibitors (lisinopril ≥10 mg/d or ramipril ≥5 mg/d), initial dose of sacubitril/valsartan, starting >36 hours after discontinuation of the ACE inhibitor, is 49/51 mg twice a day uptitrated to the maximum dose of 97/103 mg twice a day 2 weeks later. In patients taking enalapril in a dose of ≤10 mg/d, the starting dose is 24/26 mg twice a day. Similarly, the starting dose of sacubitril/valsartan is 49/51 mg twice a day in patients taking valsartan >160 mg or equivalent ARB (losartan >50 mg/d, olmesartan >10 mg/d) and 24/26 mg twice a day in patients taking ≤160 mg/d of valsartan. Patients naive to ACE inhibitors or ARB should be started on the lowest sacubitril/valsartan dose with uptitration every 2 weeks to the highest dose. In patients with severe kidney disease (eGFR <30 mL/min/1.73 m2), reduced starting dose of 24/26 mg twice a day is recommended with doubling the dose every 2 to 4 weeks to target maintenance dose of 97/103 mg twice a day as tolerated.
The Effect of Sacubitril/Valsartan in HFpEF
The participant of HFpEF draws significant attention since about half of patients with HF have HFpEF and, importantly, since none of the current HF therapies (or other therapies) were found to improve outcomes in this patient population. 39 In the PARAMOUNT trial, 40 a phase 2 study, 301 patients with EF ≥45%, documented history of HF symptomatology, and NT-proBNP levels of above 400 pg/mL were randomly assigned to treatment with sacubitril/valsartan (starting dose 50 mg twice a day, uptitrated to 200 mg twice a day) or valsartan (starting dose 40 mg twice a day, uptitrated to 160 mg twice a day).
After 12 weeks of treatment, NT-proBNP levels were significantly reduced in the sacubitril/valsartan group (baseline: 783 pg/mL, 12 weeks: 605 pg/mL) compared to the valsartan group (baseline: 862 pg/mL, 12 weeks: 835 pg/mL; P = .005). Also, at 36 weeks of treatment, an improvement in NYHA class and in atrial volume was noted in the sacubitril/valsartan group (P = .003, P = 0.05, respectively), although no difference was noted in other echocardiographic parameters. Based on the results of this trial, the efficacy and Safety of LCZ696 Compared to Valsartan, on Morbidity and Mortality in Heart Failure Patients With Preserved Ejection Fraction (PARAGON-HF) trial, aiming to randomize 4300 class II to IV patients with HFpEF, is presently conducted (see below).
Postmarketing Information
In May 2016, results of the initiating sacubitril/valsartan (LCZ696) in heart failure (TITRATION) study, 41 aimed to evaluate the tolerability of patients having HF with reduced ejection fraction (HFrEF) to a rapid uptitration of sacubitril/valsartan, were published. In this trial, 540 patients with HFrEF underwent a run-in period in which all patients received 50 mg twice a day of sacubitril/valsartan for 5 days followed by a double-blind, randomization period in which they were divided to a “conservative arm” (50 mg twice a day for 14 days, 100 mg twice a day for 21 days, and then 200 mg twice a day) and “condensed arm” (100 mg twice a day for 2 weeks followed by 200 mg twice a day). Predefined tolerability criteria (hypotension, renal impairment, hyperkalemia, and angioedema) occurred in 8.4% versus 9.7%, 7.6% versus 7.3%, 4.4% versus 7.7%, and 0.8% versus 0% of the conservative versus the condensed arm, respectively (P = .57), and 84.3% of the patients in the conservative arm and 77.8% of the patients in the condensed arm achieved and maintained target dose of sacubitril/valsartan (P = .078). The authors of the study concluded that the accelerated uptitration of sacubitril/valsartan was well tolerated. 41
Post hoc analyses of the PARADIGM-HF study results focused on specific important characteristics of patients with HF. Lower than target doses of either enalapril or sacubitril/valsartan—analysis showed that this group of patients experienced higher burden of end point events. Nevertheless, the beneficial effect of sacubitril/valsartan over enalapril was maintained in patients in whom a dose reduction (of either enalapril or sacubitril/valsartan) was done throughout the course of the trial. The majority of patients in the PARADIGM-HF study maintained the target dose of sacubitril/valsartan 200 mg twice a day (mean 375 ± 71 mg daily) and enalapril 10 mg twice a day (18.9 ± 3.4 mg daily). During the study, 43% of patients in the enalapril arm and 42% of patients in the sacubitril/valsartan arm reduced their dose at any time after randomization. The strongest multivariate predictors of dose reduction were baseline creatinine, age, heart rate, use of implantable defibrillator, and lower systolic BP. All were similar in the 2 treatment arms. However, in patients actively taking study drug below target dose levels, sacubitril/valsartan remained effective compared to enalapril (hazard ratio [HR]: 0.57, 95% confidence interval [CI]: 0.42-0.78; P < .001). 42,43
Another post hoc analysis examined the effect of sacubitril/valsartan across the range of systolic dysfunction in the PARADIGM-HF trial (mean EF was 29.5%, interquartile range: 25%-34%) and showed that sacubitril/valsartan was effective in reducing outcomes throughout the spectrum of impaired EF. 44
A study examining an important characteristic in HF management, hospital readmissions, showed that the 30-day readmission rate in patients hospitalized during the study period was reduced by 38% in the sacubitril/valsartan-treated group compared to the enalapril-treated group (9.7% vs 13.4%, respectively, OR: 0.62, 95% CI: 0.45-0.87; P = .006). 45
An analyses focused on prespecified measures of nonfatal clinical deterioration showed that in comparison to the enalapril group, fewer sacubitril/valsartan-treated patients required intensification of medical treatment for HF (HR: 0.84; 95% CI: 0.74-0.94; P = .003) or an emergency department visit for worsening HF (HR: 0.66; 95% CI: 0.52-0.85; P = .001). The patients in the sacubitril/valsartan group had 23% fewer hospitalizations for worsening HF (P < .001) and lower need for intensive care admissions (−18%; P = .005), intravenous positive inotropic agents (−31%; P < .001), and implantation of a HF device or cardiac transplantation (−22%; P = .07). 32
Desai et al 46 reported on the mode of death in the patients included in the PARADIGM-HF study. The majority (80.9%) of deaths were cardiovascular, and as indicated above, the risk of cardiovascular death was significantly reduced by treatment with sacubitril/valsartan. Investigating deaths due to cardiovascular (CV) causes, both sudden cardiac death (HR: 0.80, 95% CI: 0.68-0.94; P = .008) and pump failure death (HR: 0.79, 95% CI: 0.64-0.98; P = .034) were reduced by sacubitril/valsartan compared to enalapril. Deaths of other CV causes and noncardiovascular causes were distributed evenly between the treatment groups.
An analysis of the effect of age on the PARADIGM-HF study results 47 revealed an increase in the prespecified safety outcomes of hypotension, renal impairment, and hyperkalemia with age in both treatment groups, and the overall results of the study, including more hypotension but less renal impairment and hyperkalemia with sacubitril/valsartan, were consistent across age groups.
An analysis of the study results in different risk groups as determined by the complete Meta-analysis Global Group in Chronic Heart Failure (MAGGIC) risk score 48 was performed in 8375 of the trial’s patients. The benefit of sacubitril/valsartan over enalapril for the primary end point was similar across the spectrum of risk. Treating 100 patients with sacubitril/valsartan compared to enalapril for 2 years led to 7 fewer patients in the highest risk group experiencing primary outcomes, compared to 3 in the lowest group. 49
The most recent publication by Solomon et al 50 showed that patients included in the PARADIGM-HF study who had recent HF hospitalization were more likely to experience cardiovascular death or HF hospitalization compared to those who had never been hospitalized. At the same time, however, patients who were clinically stable, as indicated by either no HF hospitalization within the last 3 months or by a lack of any prior HF hospitalization, were as likely to benefit from sacubitril/valsartan therapy as more recently hospitalized patients.
Ongoing Trials
Extension, open-label, study of the PARADIGM-HF trial will evaluate the safety and tolerability of sacubitril/valsartan by examining the incidence of angioedema, reduced BP, and serious adverse events (including death) in patients (n = 3700) who safely completed the PARADIGM-HF trial. The study is scheduled to be completed in May 2018. 51
The PARAGON-HF trial—A multicenter, randomized, double-blind study aimed to evaluate the efficacy and safety of sacubitril/valsartan as compared to valsartan alone in 4300 patients with HF having EF ≥45% who are scheduled to be followed for a period of up to 57 months. 52 Almost half of the patients will also undergo repeated measurements of cognitive function.
The comparison of Pre- and Post-discharge Initiation of LCZ696 Therapy in HFrEF Patients After an Acute Decompensation Event (TRANSITION) trial—A multicenter, randomized study designed to compare the safety and effectiveness of the initiation of sacubitril/valsartan in predischarge patients with HF versus postdischarge patients with HF (n = 1000) who were hospitalized due to an acute decompensated HF event.
Cost-Effectiveness Analysis
Since the issues of cost and cost-effectiveness have a significant impact on the implementation and the usage of new drugs, a cost-effectiveness analysis comparing treatment with sacubitril/valsartan versus enalapril has been made in the United States. 53 The authors analyzed data from a population of patients with profile similar to that in the PARADIGM-HF trial and conducted a model estimation with 30-year time horizon, including risk of all-cause mortality, HF hospitalization, quality of life estimation, hospital admission’s costs, and medication’s costs. The model showed that for eligible patients, sacubitril/valsartan will increase quality-adjusted life years (QALYs) at an expense of US$45 017 for every QALY compared to enalapril. Importantly, this estimation is considered within the range of “very good value” (<50 000 per QALY) in accordance with both the American Heart Association/American College of Cardiology and the World Health Organization standards and is comparable to other therapies and interventions. 54,55
Updated Guidelines Recommendations
Recommendations for the use of sacubitril/valsartan have been included in a guideline updates published in 2016 by the American College of Cardiology, the American Heart Association, and the Heart Failure Society of America in the United States 56 and by the European Society of Cardiology in Europe 57 (Table 2).
Current Guidelines Recommendations.

Abbreviations: ACC, American College of Cardiology; ACE, angiotensin-converting enzyme; AHA, American Heart Association; ARB, angiotensin receptor blocker; ARNI, angiotensin receptor neprilysin inhibitor; B-R, from one or more randomized clinical trials (RCTs) or meta-analysis of moderate quality RCTs; ESC, European Society of Cardiology; HFSA, Heart Failure Society of America; HFrEF, heart failure with reduced ejection fraction; NYHA, New York Heart Association.
Footnotes
Author Contributions
O. Havakuk contributed to conception and design, acquisition, analysis, and interpretation of data, and drafted the manuscript. U. Elkayam contributed to conception and design, acquisition, analysis, and interpretation of data, and critically revised the manuscript. Both authors gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.