
Abstract
Background:
Statin therapy has been thought to improve outcomes in cardiac surgeries. We aimed to determine the statin effects on the development of postoperative atrial fibrillation (AF), hospital length of stay (LOS), and inflammatory status in patients undergoing cardiac surgeries.
Methods:
A systematic literature search in databases was performed, until January 2015. Randomized clinical trial (RCT) studies evaluating statin effect on statin-naive patients with sinus rhythm undergoing cardiac surgeries were eligible to be analyzed.
Results:
Twelve RCTs involving 1116 patients, 559 receiving statin and 557 receiving control regimen, were analyzed. Postoperative AF occurred in 17.9% and 36.1% of patients in the statin and control groups, respectively. The statin therapy was associated with decreases in the postoperative AF (risk ratio [RR] 0.50, 95% confidence interval [CI] 0.41-0.61, P < .000010), hospital LOS (mean difference in days, RR −0.44, 95% CI −0.67 to −0.20, P = .0002), and postoperative C-reactive protein (CRP) compared with control (mean difference in mg/L, RR −12.37, 95% CI −23.87 to −0.87, P = .04). The beneficial effects on AF and CRP were more marked in patients receiving atorvastatin compared to other statins. Decrease in postoperative AF was greater in coronary artery bypass graft surgery compared to that in isolated valvular surgery.
Conclusion:
Perioperative statin therapy in statin-naive patients with sinus rhythm undergoing cardiac surgeries was associated with decreases in the development of postoperative AF, the hospital LOS, and the CRP level. However, there were insufficient data to provide evidences regarding statin impacts in patients undergoing isolated valvular surgery.
Introduction
Atrial fibrillation (AF) is the most common heart arrhythmia with an incidence of 0.4% to 1%, increasing with age. 1 It has also been found to be a major complication after cardiac surgeries, occurring in 10% to 65%, varying with surgery type, and developing usually on second or third postoperative day. 2,3 Several risk factors, including advanced age, valvular heart disease, a previous history of AF, chronic lung disease, preoperative digoxin use, and heart failure, have been shown to predict AF after cardiac surgeries. 4,5 The pathophysiologic mechanisms involved in the development of AF after cardiac surgeries have not been clearly elucidated; however, some etiologies, including the electrophysiological remodeling of atrium, inflammatory pathways, and oxidative stress, have been postulated to be the main pathogeneses. 6,7 Given the greater risk of morbidity and mortality attributable to the incidence of postoperative AF and the increased length of hospitalization and cost of care, some therapies, mainly beta blockers, have been recommended for the prevention of AF following cardiac surgeries. 6 On the other hand, the primary prevention of AF with respect to the mechanisms involved in the AF incidence has contributed to using some nonantiarrhythmic agents, which inhibit the progression of substrate for AF by mechanism-based prevention. 8
The 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase inhibitors, named statins, have been shown to have an antiarrhythmic effect against the development of AF in patients undergoing cardiac surgeries, in addition to their lipid-lowering and anti-ischemic properties; 9 however, previous randomized clinical trials (RCTs) have shown inconsistent results, that is, some of those were relatively a small study or underpowered to evaluate this end point. 2,8,10 –19 Moreover, in the latest guideline of AHA/ACC/HRS for the management of patients with AF, the use of upstream statin therapy may reduce postoperative AF in patients undergoing coronary artery bypass graft (CABG) surgery, and it was endorsed in patients undergoing CABG with class IIb recommendation and level of confidence A. 20 Hence, we sought to conduct a meta-analysis of all RCTs published up to the end of 2014 so as to evaluate the effect of perioperative statin therapy on the development of AF in statin-naive patients undergoing cardiac surgeries.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISAM) protocol was used in preparing this report. 21 Two reviewers, YR and MG, independently searched for and assessed RCTs to be included into this meta-analysis.
Data Sources and Search Strategy
In a comprehensive search of databases, the reviewers searched electronic databases through ISI (Web of Science), PubMed, Ovid MEDLINE, Cochrane library, and Scopus for all studies published in English language reporting the effect of statin therapy on AF after cardiac surgery. We used key words consisting of “statin,” “HMG-CoA reductase inhibitor,” “atorvastatin,” “simvastatin,” “pravastatin,” “rosuvastatin,” “lovastatin,” and “fluvastatin” combined with “atrial fibrillation” with or without “cardiac surgery” (Supplement 1). The database search has been carried out in 2 steps: (1) from January 1980 up to July 2014 and (2) an updated search from August 2014 to December 31, 2014. In addition to electronic searching, we manually searched the references of review articles, recent meta-analyses regarding similar topic, and the included RCTs to ensure that we did not miss any relevant studies. All titles and abstracts were uploaded into reference management software database, and all of them were independently evaluated by the reviewers.
Study Selection and Quality Assessment
The RCTs meeting the following criteria were selected: (1) comparing a statin regimen with a placebo or control regimen; (2) patients undergoing cardiac surgeries, including CABG surgery, valve surgery, or a combination of both procedures; (3) the end point of AF reported as an outcome regardless of stating its method of detection and/or monitoring tool; (4) statin-naive patients who have sinus rhythm preoperatively; and (5) availability of the full texts of RCTs.
All selected articles were evaluated by 2 reviewers concerning methodological quality using the Jadad scoring method. 22 Additionally, those were checked for potential biases using the Cochrane Statistical Methods Group, consisting of random sequence generation, allocation concealment, blinding, incomplete outcome data, selective reporting, and any other potential sources of biases, classified into low risk, high risk, and unclear risk of biases.
Data Abstraction and Synthesis
We reviewed the full text of included RCTs and provided basic study features and the perioperative characteristics of patients. The reported AF was identified if it was reported as an outcome or its definition and monitoring methods also had been specified. The main results consisted of pooled risk ratio (RR) with 95% confidence interval (CI) showing the effect of statin therapy on the reviewed outcomes, including postoperative AF, the length of stay (LOS) in hospital and intensive care unit (ICU), intubation time after surgery, and postoperative C-reactive protein (CRP) peak value.
All continuous and dichotomous variables were analyzed using the Mantel-Haenszel method and Inverse Variance Statistical method, respectively. In order to assess the heterogeneity within studies, the I2 statistic was used. All variables were analyzed using the fixed-effects model in the absence of substantial heterogeneity (chi-square test P value > .1 and I2 <50%); otherwise, we used random-effects model. When observing considerable heterogeneity, it was investigated by means of subgroup analysis. In order to address the heterogeneity, 2 subgroup analyses consisting of statin agent type and surgery type were performed. The statin type was divided into 2 groups, including atorvastatin and other statins (rosuvastatin, pravastatin, and simvastatin). Because some differences exist between the CABG and the valvular surgeries regarding the pathophysiology of postoperative AF developing, 8 studies were categorized into the following 2 groups: (1) isolated CABG surgery and (2) hybrid or isolated valvular surgeries. Moreover, sensitivity analyses were conducted by excluding studies with Jadad score <3, RCTs with high or unclear risk of bias, non-placebo–controlled trials (assigned usual care in control group), and those with unspecified method of AF monitoring. A P value less than .05 was considered to be statistically significant. All statistical analyses were carried out using RevMan, version 5.3.5 (The Cochrane Collaboration, Oxford, United Kingdom).
Results
Study Selection and Characteristics
After removing duplicates, a total of 1320 studies were screened to be included in the meta-analysis, of which 12 RCTs comprised of 1116 patients, 559 receiving statin and 557 receiving placebo or control regimen, fulfilled our criteria to be analyzed (Figure 1). Included RCTs 2,8,10 –19 were conducted mainly in European and Asian countries from 2006 to 2014. The study population mainly consisted of patients who underwent elective on- or off-pump CABG surgery (n = 10), combined on-pump CABG and valve surgeries (n = 1), and on-pump isolated valve surgery (n = 1). Comparing statin therapy and control group was made with a placebo (n = 9) or a control regimen (n = 3). All patients were statin-naive at the time of enrollment in all RCTs (Table 1). Other baseline and perioperative characteristics were summarized (Table 1 and Supplement 2). The Cochrane Statistical Method Group revealed a low risk of bias in 5, high risk in 3, and unclear risk in 4 studies. Furthermore, all RCTs received Jadad scores of 2 (n = 2), 3 (n = 5), 4 (n = 2), and 5 points (n = 3; Supplement 3).

Flow diagram showing the selection of included studies.
Baseline Methodological Features of the Studies Included in the Meta-Analysis.

Abbreviations: AF, atrial fibrillation; CABG, coronary artery bypass graft surgery; ECG, electrocardiogram; ICU, intensive care unit; NS, not specified.
Study Measured Outcomes
We calculated the pooled RRs for the measured outcomes, including the postoperative AF, the hospital LOS, the ICU LOS, the intubation time, and the postoperative CRP peak value. Postoperative AF occurred in 17.9% and 36.1% of patients in the statin and control groups, respectively. There was no heterogeneity within studies reported AF (I 2 = 0%, P = .096), and pooled results using fixed-effects model showed a statistically significant reduction in the development of postoperative AF (RR 0.50, 95% CI 0.41 to 0.61, P < .00001; Figure 2). Nine studies reported the hospital LOS following surgery. The statin therapy was associated with a reduction in the hospital LOS compared to control regimen (mean difference in days, RR −0.44, 95% CI −0.67 to −0.20, P = .0002). There was moderate heterogeneity within studies that reported the hospital LOS, I2 = 52% (Figure 3). Seven of included RCTs reported ICU LOS, which did not show any significant difference between the statin and control regimen (mean difference in hour, RR −0.47, 95% CI −2.24 to 1.30, P = .6), depicted in Figure 4. The postoperative change in CRP was reported in 7 of included studies. Pooled results showed that statins significantly decreased the CRP levels compared to control regimen (mean difference in mg/L, RR −12.37, 95% CI −23.87 to −0.87, P = 0.04), although it was associated with considerable heterogeneity, I2 = 99% (Figure 5). The intubation time was not significantly different between the statin therapy and control (mean difference in day, RR −1.01, 95% CI −2.41 to 0.39, P = .16); however, it was associated with substantial heterogeneity, I2 = 74% (Supplement 4).

Effect of statin therapy on the postoperative atrial fibrillation (AF).
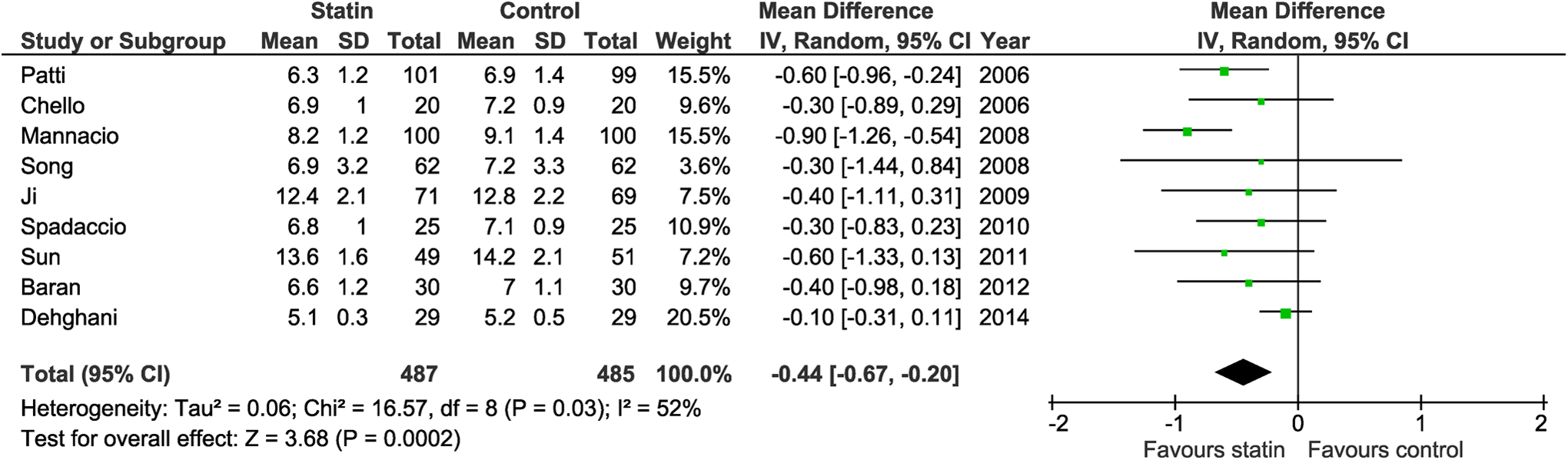
Effect of statin therapy on the hospital length of stay (LOS).

Effect of statin therapy on the intensive care unit (ICU) length of stay (LOS).

Effect of statin therapy on the postoperative C-reactive protein (CRP) peak value.
Publication Bias
Funnel plot was also drawn for mentioned outcomes, of which the hospital LOS, intubation time, and CRP plots were asymmetrical. Therefore, we excluded outlaying studies with large 95% CI; thereafter all plots were symmetric (supplement 5). Neither Begg’s funnel plot nor Egger’s test detected obvious evidence of publication bias, as well.
Subgroup Analysis
For heterogeneity to be addressed, 2 subgroup analyses were performed. Comparing groups based on statin agent used, atorvastatin showed a greater protection against the development of postoperative AF than did other statins (RR 0.49, 95% CI 0.39 to 0.61, P < .00001 vs RR 0.53, 95% CI 0.34 to 0.82, P = .005). Moreover, atorvastatin was associated with a greater decrease in the CRP level (RR −21.91, 95% CI −23.62 to −20.20, P < .00001 vs RR −5.64, 95% CI −6.38 to −4.90, P < .00001) and demonstrated less heterogeneity as well (I2 = 87% vs I2 = 99%). Comparing the outcomes on the basis of surgery type subgroups (CABG vs hybrid or valvular), the effect of statin therapy on AF development seemed to be more marked in CABG compared to hybrid or valvular group (RR 0.45, 95% CI 0.34 to 0.59, P < .00001 vs RR 0.58, 95% CI 0.43 to 0.79, P < .0004). Heterogeneity within studies reported the hospital LOS disappeared in surgery type subgroup analysis, CABG compared with hybrid or valvular (I2 = 0% vs I2 = 82%). Furthermore, when exploring heterogeneity in the intubation time, it disappeared in CABG group. However, heterogeneity within studies reported CRP remained considerable even comparing surgery type groups (Table 2).
Subgroup Analyses Showing Statin Effects on Outcomes.

Abbreviations: AF, atrial fibrillation; CI, confidence interval; CRP, C-reactive protein; ICU, intensive care unit; LOS, length of stay; MD, mean difference; NA, not applicable; RR, risk ratio
Sensitivity Analysis
Sensitivity analyses were conducted to explore the sources of heterogeneities and to identify the effects of various exclusion criteria on the outcomes. After excluding studies with high and unclear risk of bias, there were no significant differences in the effect of statin therapy on the estimated outcomes. In addition, the outcomes were similar when excluding RCTs with Jadad score <3. Upon excluding studies without prespecified AF monitoring method or not being placebo-controlled trial, no significant differences were observed concerning the outcomes, and heterogeneity related to the CRP estimate remained substantial (Table 3).
Sensitivity Analysis Based on Study Bias and Methodological Features.
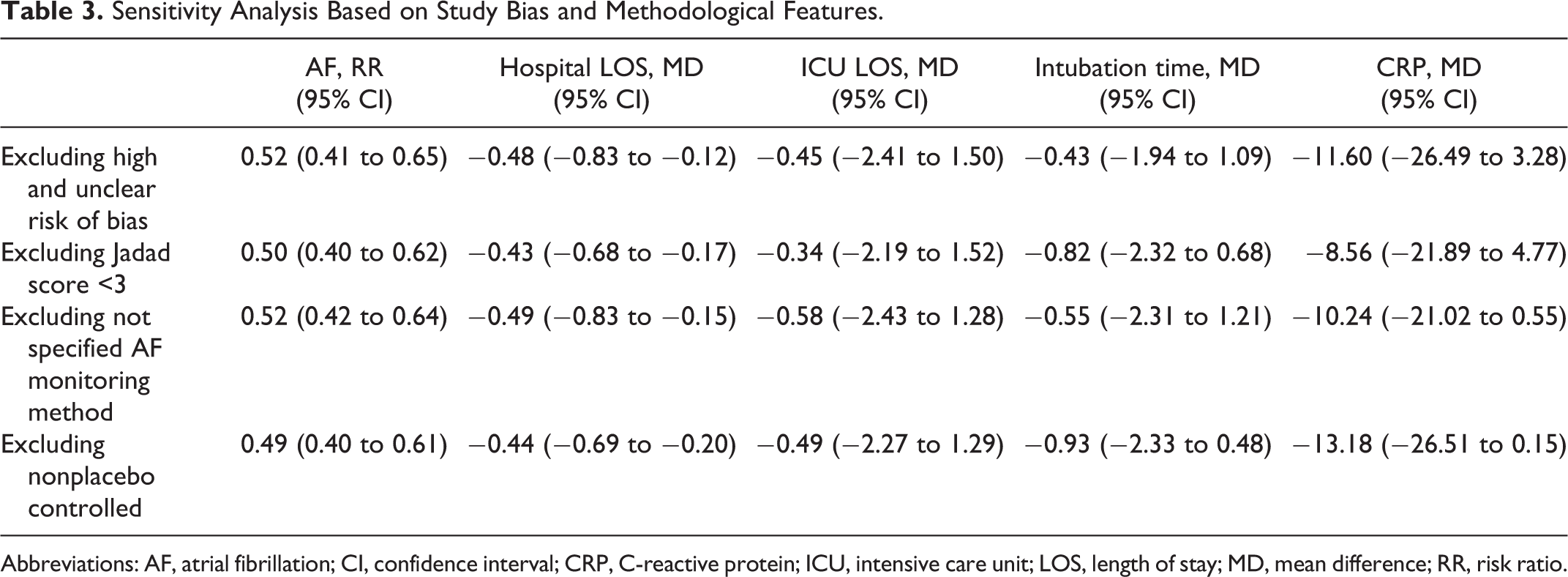
Abbreviations: AF, atrial fibrillation; CI, confidence interval; CRP, C-reactive protein; ICU, intensive care unit; LOS, length of stay; MD, mean difference; RR, risk ratio.
Discussion
This meta-analysis included 12 published RCTs reporting the effect of perioperative statin therapy on the development of AF in statin-naive patients with sinus rhythm undergoing cardiac surgeries. The present study showed that statin therapy reduced the development of AF after cardiac surgeries. Moreover, using statin therapy was associated with decreases in the hospital LOS and postoperative peak CRP values. The beneficial effects of statin on the AF developing seemed to be more marked in the patients receiving atorvastatin than in those taking other statins. Furthermore, the impacts of statin on outcomes were more remarkable in patients undergoing CABG surgery than those in hybrid or valvular surgeries. After subgroup analysis, the heterogeneity in the hospital LOS disappeared in patients undergoing CABG surgery; however, heterogeneity related to the CRP outcome remained substantial even after applying sensitivity analysis.
The findings of this updated meta-analysis are in accordance with those of other previously published meta-analyses, in which has been demonstrated that statin therapy effectively decreased the frequency of postoperative AF. 23 –26 However, reported by Yin et al, 27 no significant effect of statins on reducing postoperative AF in patients undergoing cardiac surgery has been found, underscoring the need for more RCT studies. They concluded that the lack of statin effect should be clarified by future studies focusing on the effect and mechanisms involved in this setting. In our meta-analysis, we showed that the CRP decreased significantly in statin-receiving patients compared to placebo/control group, demonstrating the probable potential role of inflammatory pathways in the pathophysiology of postoperative AF, although this relationship may not be causative one, and more studies are required to prove any relationship. In addition, it is worth noting that the RCTs included relatively small number of patients with each study including no more than 200 patients. Therefore, it seems that the observational data, as previously reported in large populations, become even more important, especially because the findings are in accordance with those of the RCTs.
Statins have long been used as lipid-lowering agents in clinical practice, although its pleiotropic potentials have also been introduced, of which antiarrhythmic property may be of great clinical importance that is a cholesterol-independent action. 28 Statins are divided into low, intermediate, and high dosages based on their antilipid properties. Accordingly, Kourliouros et al 29 retrospectively investigated the dose-dependent effects of statin on the development of postoperative AF, in which they have reported that high-dose statins had greater impact on reducing postoperative AF. In contrast, they have also demonstrated that there was no significant difference between atorvastatin 80 and 10 mg regarding the reduction in AF developing after cardiac surgery. 30 In addition, it has been found that the antiarrhythmic effect of statins did not match their lipid-lowering property. In this case, simvastatin 20 mg, an atorvastatin 10 mg equivalent, showed a significant effect on postoperative AF compared with that in no statins (odds ratio [OR] 2.32, 95% CI 1.30-4.11), whereas atorvastatin 10 mg had no impact on AF (OR 1.05, 95% CI 0.55-1.99). Moreover, the protective effect of simvastatin 40 mg, which is an atorvastatin 20 mg equivalent, was significantly more pronounced than did atorvastatin 20 mg or atorvastatin 40 mg regimen. 31 Besides that, we divided RCTs into 2 groups, including atorvastatin and other statins, in which we found that atorvastatin effects on postoperative AF and CRP level were greater compared with other statins. On the other hand, only 9 of the RCTs used atorvastatin and other statins were used in only 1 RCT each. The doses were different and the study designs and the patient populations were not the same. Given the lack of direct comparison of different statins, definite conclusions need further studies comparing different statins’ regimens.
Postoperative AF has been found to be one of the main factors leading to increase in the hospital and ICU LOS in patients undergoing cardiac surgeries. 5 Borzak et al 32 demonstrated that prolonged hospitalization period was affected by postoperative AF; hence, preventive strategies are of great importance to reduce the cost of care and patients’ morbidity attributed to the postoperative AF. 33 Nine and seven RCTs have reported the effects of statin therapy on the hospital and ICU LOS, respectively. We found that statin therapy decreased the hospital LOS, while it was ineffective to decrease the ICU LOS. Furthermore, the duration of intubation was also significantly reduced in the statin-treated patients compared to control group. The ventilation time has been demonstrated to predict the incidence of postoperative AF after CABG. 34 In this meta-analysis, statin therapy did not significantly reduce the ICU LOS but was associated with a significant decrease in the intubation time that is a main factor influencing the ICU LOS in such a setting. This controversy is likely to be caused by other predisposing factors resulting in the prolonged ICU LOS, including underlying diseases or the standards of caring in ICU wards. Moreover, the heterogeneity related to the hospital LOS and intubation time completely disappeared after excluding the valvular or hybrid surgeries. We think that because patients undergoing isolated valvular surgery, in one RCT, 8 had lower mean age and less cardiovascular risk factors, shorter hospital LOS and intubation time were developed compared with patients undergoing only CABG with older ages and more risk factors. However, since the number of patients undergoing isolated valvular surgery was very small, only in 1 study, we could not conclude that whether statin effects in valvular repair surgeries are beyond the conclusions of the original study.
It has been postulated that inflammation has a prominent role in the initiation and perpetuation of AF developing after cardiac surgery, 35 and on-pump cardiac surgery results in the activation of complement system and subsequent increase in CRP. 36 The anti-inflammatory effect of statins has also been shown in some studies, in which the statin therapy led to decrease in inflammatory markers following cardiac surgery, including CRP, 10,13,14,17 interleukins, 11,12,16,19 and white blood cell count; 8,16 however, despite the increase in postoperative CRP in cases with AF compared with non-AF ones, some studies lacked the statin efficacy in decreasing postoperative CRP. 2,11,15 In this meta-analysis, despite being inconsistent from study to study, the statin therapy led to a statistically significant decrease in postoperative peak CRP values in patients taking statins than those receiving control regimens, although it was associated with considerable heterogeneity. We performed subgroup and sensitivity analyses, but the heterogeneity did not disappear. It seems that this heterogeneity may be caused by clinical heterogeneity because so many factors can be interfered with CRP levels. As a contributor of this hypothesis, the time of CRP peak values was different among studies from 6 hours to 3 days, although their settings were similar in many aspects.
Study Limitations
Despite being a comprehensive meta-analysis including all published RCTs performed on statin-naive patients, there are some limitations in our analysis. First, we did not include unpublished studies, abstract forms, and other languages except for English. Second, we were unable to evaluate the sources of heterogeneity related to the CRP outcome. This heterogeneity may be attributable to various populations in the studies or to different pathophysiologic mechanisms of AF developing. Furthermore, statistical heterogeneity is a correlate of clinical heterogeneity, and this relationship may sometimes be weak. 37 Third, we did not make an analysis regarding the duration of statin therapy. Of note, the most of postoperative AF cases are developed during postoperative second or third day, 3 and all included studies followed the patients at least up to the discharge time or even 30 days postoperatively, these periods of follow-up seem to be sufficient for evaluation of statin effects on postoperative AF. On the other hand, some RCTs have not defined the method of AF monitoring that may lead to a bias in the detection of cases with AF. Regarding this issue, we performed a sensitivity analysis by excluding these RCTs, in which there was no difference in the statin effect on reducing postoperative AF. Fourth, due to lack of data regarding the statin effect on the postoperative lipid status of patients, which has been reported in only 2 RCTs, 10,16 we were unable to evaluate the lipid-lowering properties of statins in our analysis.
Conclusion
In this meta-analysis, perioperative statin therapy in statin-naive patients with sinus rhythm undergoing cardiac surgeries was associated with a decreased risk in the development of postoperative AF, hospital LOS, and postoperative peak CRP levels. Moreover, our meta-analysis provided evidence that the beneficial effects of atorvastatin were more pronounced than those of other statins but underscores the need for more RCTs comparing different statin agents. However, there were insufficient data to provide evidences regarding perioperative statin therapy for patients undergoing isolated valvular surgery.
Footnotes
Author Contributions
Rezaei, Y contributed to conception and design and acquisition, analysis, and interpretation, drafted the manuscript, critically revised the manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy. Gholami-Fesharaki, M contributed to design, acquisition, and interpretation, critically revised the manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy. Dehghani, MR, Arya, A, Haghjoo, M, and Arjmand, N contributed to conception and acquisition, critically revised the manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.