
Abstract
Background:
Little is known about ivabradine in cardiac rehabilitation in patients with coronary artery bypass graft (CABG).
Methods:
In this prospective, randomized study, suitable patients admitted for cardiac rehabilitation after recent CABG were randomized to ivabradine 5 mg twice a day + standard medical therapy including bisoprolol 1.25 mg once daily (group I-BB, n = 38) or standard medical therapy including bisoprolol 2.5 to 3.75 mg once daily (group BB, n = 43). Patients were evaluated at admission, discharge, and 3 months. The primary end point was improvement in functional status, and other end points were improvement in diastolic function and recovery of systolic function. End points were assessed by distance covered in 6-minute walking test (6MWT), percentage with normal diastolic function, and percentage increase in left ventricular ejection fraction (LVEF).
Results:
Cardiac rehabilitation improved functional capacity in both groups. In group BB, distances covered in the 6MWT at admission, discharge, and 3 months were 215 ± 53, 314 ± 32, and 347 ± 42 m, respectively. Corresponding distances in group I-BB were 180 ± 91, 311 ± 58, and 370 ± 55 m. Normal diastolic function was restored in I-BB patients, increasing from 24% at admission to 50% and 79% at discharge and 3 months; in BB patients, it decreased from 23% to 19% and 16%. The LVEF improved in I-BB patients, from 57% ± 3% at admission to 62% ± 4% at discharge and 66% ± 3% at 3 months, while remaining unchanged in BB patients (57% ± 3%, 59% ± 4%, and 59% ± 3%).
Conclusion:
Adding ivabradine to low-dose bisoprolol during cardiac rehabilitation in patients with CABG improved functional capacity, enhanced recovery of systolic function, and reduced diastolic dysfunction.
Keywords
Introduction
Heart rate is a risk factor in the general population 1 and in patients with coronary artery disease 2,3 or heart failure. 4 The reduction in mortality associated with beta-blockers is likely to be due to their effect on heart rate, in both ischemic heart disease 5,6 and chronic heart failure. 7,8 Low heart rate reduces myocardial oxygen demand while simultaneously improving oxygen supply by prolonging diastole, which improves coronary flow and myocardial perfusion. These benefits have been demonstrated in patients with stable coronary artery disease and in patients with chronic heart failure. 9,10
Accordingly, heart rate reduction has been proposed as a therapeutic target in ischemic heart disease. 11,12 The use of a “pure” heart rate-lowering drug such as ivabradine would be useful for assessing benefit related to heart rate reduction alone. 3,12 With currently available drugs, it is difficult to isolate the effect of heart rate reduction from other pharmacological effects. Furthermore, adherence might be improved if beta-blocker dosage could be reduced and adverse effects avoided. 13 Finally, European Society of Cardiology guidelines for myocardial revascularization endorse adequate medical therapy, other secondary prevention strategies for risk factor modification and permanent lifestyle changes as goals to achieve after myocardial revascularization. Cardiac rehabilitation is an integral part of the management strategy after revascularization, because such measures reduce future morbidity and mortality in a cost-effective way and can further ameliorate symptoms. In this sense, even though not clearly specified by guidelines, rate control might have an added value in revascularized patients, even in the presence of normal ejection fraction (EF). 14 The rate of patients with coronary artery bypass graft (CABG) discharged with beta-blockers from heart surgery ranges from 67.4% and 83%, 15,16 and beta-blockers are especially useful in patients with previous acute myocardial infarction or heart failure; however, according to American College of Cardiology Foundation/American Heart Association (ACCF/AHA) Guidelines for CABG 2011, 17 beta-blockers should be prescribed to all patients with CABG without contraindications at the time of hospital discharge. In a recent multicenter study, cardiac rehabilitation was useful for increasing the rate of patients on beta-blockers, from 67.4% to 88.8% at discharge. In patients admitted for cardiac rehabilitation after myocardial revascularization, heart rate lowering is a useful objective, even if in most of cases the target dose of beta-blocker is not easily achievable because of high susceptibility of these patients to hypotension, mainly because of unstable hemodynamic and diuretic therapy to reduce fluid retention due to cardiopulmonary bypass. Moreover, in first postoperative months, there is high heart rate variability due to transient loss of autonomic control, so these patients are more prone to pass from tachycardia to bradycardia. Here, the use of a higher dose of beta-blocker might be dangerous compared to ivabradine, whose effect on f-channels is frequency dependent and thus the risk of bradycardia is lower. Hence, the aim of this study was to assess the effects at admission, discharge, and 3-month follow-up of adding ivabradine to standard therapy including low-dose bisoprolol in patients who had undergone a recent CABG.
Materials and Methods
Study Population
For this prospective, randomized study that ran between June 2012 and June 2013, we selected patients admitted to our cardiac rehabilitation unit in Lecce, Italy, after recent CABG. Criteria for inclusion were recent CABG, left ventricular ejection fraction (LVEF) ≥50%, stable clinical condition, standard cardiovascular therapy, sinus rhythm, and a heart rate >70 bpm. Patients were excluded if they had atrial fibrillation, uncontrolled cardiac arrhythmia, physical limitation to the 6-minute walking test (6MWT), or chronic obstructive pulmonary disease. The study protocol was authorized by the local ethics committee. All patients gave written informed consent, and blinded data were analyzed by 2 external physicians.
At admission, all patients took bisoprolol 1.25 mg and were randomized to treatment with ivabradine 5 mg twice a day on top of standard therapy including bisoprolol 1.25 mg once daily (group I-BB) or to therapy including bisoprolol 2.5 (38 patients) or 3.75 mg (5 patients) once daily (group BB).
In addition to the beta-blocker (bisoprolol), standard therapy included statin, angiotensin-converting enzyme inhibitor or angiotensin receptor blocker, and antiplatelet agents. All the patients underwent the same program of physical training, which was usually carried out in our hospital. The first phase consisted of respiratory training and gradual mobilization in the early days of hospitalization, followed by a phase of calisthenic (II) training and a dynamic phase (III) on a stationary bike (Appendix A). None of the patients reduced or stopped ivabradine or beta-blockers during the study.
Patients underwent several tests—6MWT, transthoracic echocardiography, and blood sampling—at admission, discharge, and 3 months.
6-Minute Walking Test
A 6MWT was used to assess exercise capacity in the cardiac rehabilitation program. 16 Exercise was assessed by distance walked in the 6MWT (in meters) and double product. 18 Blood pressure was measured at the beginning and the end of the test by auscultation. Heart rate and oxygen saturation were measured by oximetry. Symptoms were assessed by means of the 10-point Borg scale rating.
Echocardiography
A complete resting 2-dimensional echocardiogram and Doppler ultrasound examination (Vivid 3 Pro; GE Healthcare, Buckinghamshire, United Kingdom) including all standard views was performed at admission, before discharge, and after 3 months. Left ventricular end-diastolic volume (EDV) and end-systolic volume (ESV) were obtained from apical 2- and 4-chamber views, via a modified Simpson rule, from which EF was automatically calculated as the difference between EDV and ESV normalized to EDV. Diastolic function was assessed by pulse wave Doppler of the mitral valve (E = PW Doppler E-wave, A = PW Doppler A-wave, E/A, and DTE = deceleration time of E-wave) and tissue Doppler imaging of the mitral annulus (Em = TDI (tissue Doppler imaging), Am = TDI A-wave, and E/Em), which assessed the different types of diastolic dysfunction. 19 –23 All echocardiograms were performed by the same echocardiographist (SM).
Study End Points and Statistics
The primary end point was the improvement in terms of functional status from admission to 3-month follow-up (covered distance in 6MWT) between the 2 groups. Secondary end points were improvement in diastolic function (defined by the percentage of patients with normal diastolic function) and recovery of systolic function (defined by an increase in LVEF).
On the basis of the results of the study by Amosova et al, 24 taking into account the above-mentioned primary end point, the minimal size of each group was 32 patients, in order to have a statistical power of 80% with α below .05. Randomization was performed using software. Categorical data were expressed as numbers and percentages; continuous data were evaluated by means of Kolmogorov-Smirnov test to assess the normality of the distribution. Normally distributed data were expressed as means and standard deviations, while nonnormally distributed data were expressed as medians and interquartile ranges. Independent comparison was performed using a chi-square test and t test or Mann-Witney U test. Pairwise comparison was performed using pairwise t test or Wilcoxon test. Relationships were investigated using linear regression. Statistical significance was defined as P < .05. The software used was SPSS (IBM, Armonk, New York).
Results
Of the 150 patients admitted to the cardiac rehabilitation unit, 81 fulfilled the selection criteria and were randomized to treatment (Figure 1). In all, 43 were randomized to standard therapy including bisoprolol (group BB) and 38 patients to ivabradine 5 mg twice a day + bisoprolol 1.25 mg once daily (group I-BB). In group BB, the high dose of bisoprolol achievable without hemodynamic effect of blood pressure was 3.75 mg in 3 cases and 2.5 mg in 40 cases. No higher doses of bisoprolol were reached due to reduced blood pressure (systolic blood pressure below 100 mm Hg). Patients were admitted to the cardiac rehabilitation unit 10 ± 3 days after CABG, and the early rehabilitation phase (admission to discharge) lasted 9 ± 5 days. Many (77% [n = 62]) of these predominantly normotensive patients with CABG had mild or moderate (grade I or II) echocardiographic diastolic dysfunction. 60% [n = 49] of patients had previous myocardial infarction, without difference between groups. Most (86% [n = 70]) of the patients were men. Characteristics of the 2 groups were comparable at admission (Table 1).

Study flowchart. CABG indicates coronary artery bypass graft.
Baseline Characteristics of Patients With CABG at Admission.a
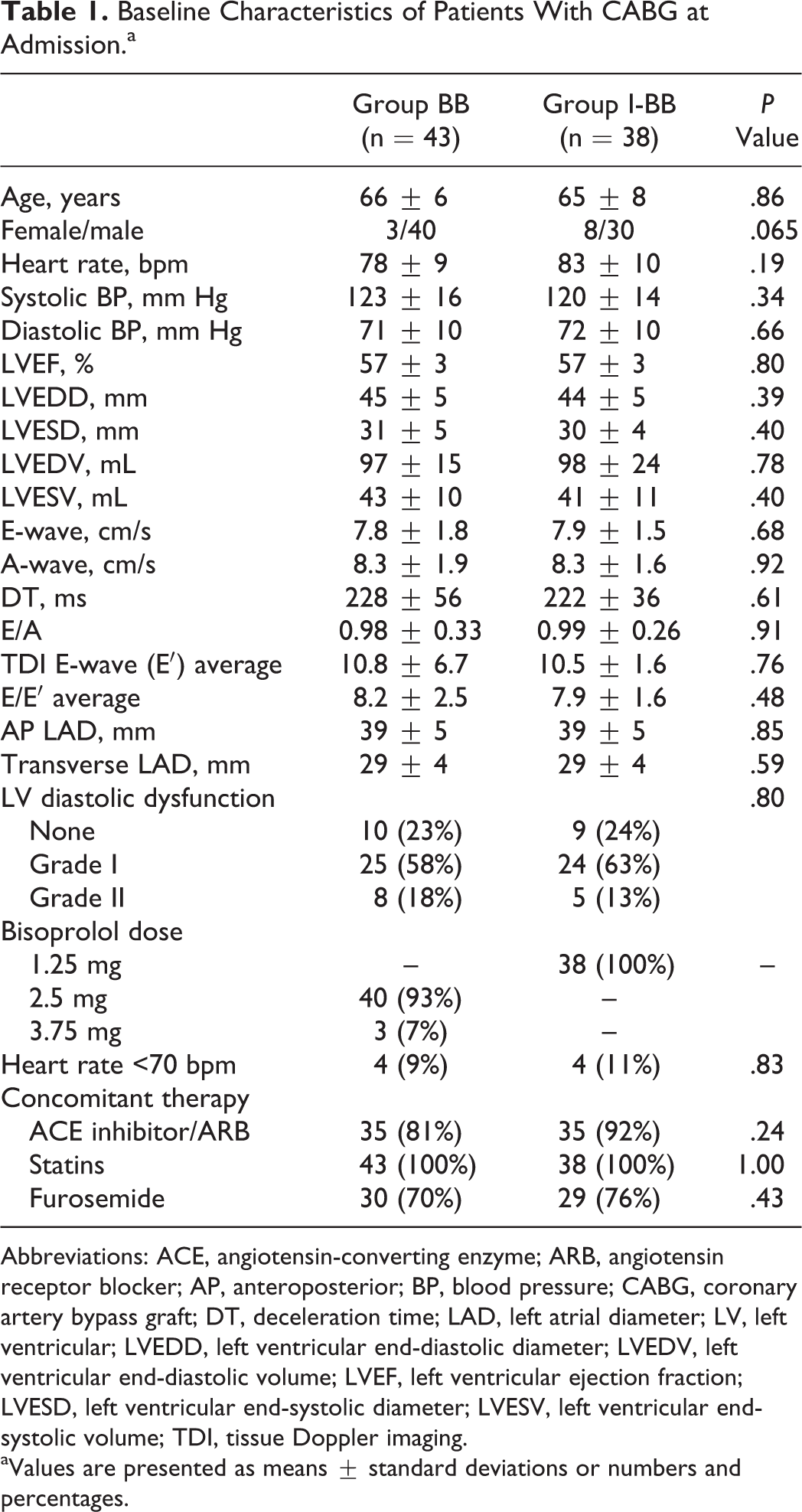
Abbreviations: ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; AP, anteroposterior; BP, blood pressure; CABG, coronary artery bypass graft; DT, deceleration time; LAD, left atrial diameter; LV, left ventricular; LVEDD, left ventricular end-diastolic diameter; LVEDV, left ventricular end-diastolic volume; LVEF, left ventricular ejection fraction; LVESD, left ventricular end-systolic diameter; LVESV, left ventricular end-systolic volume; TDI, tissue Doppler imaging.
aValues are presented as means ± standard deviations or numbers and percentages.
Rate of improvement in exercise capacity was faster in group I-BB than in group BB. At admission, bisoprolol patients covered significantly more distance during the 6MWT than ivabradine/bisoprolol patients (215 ± 53 vs 180 ± 91 m; P < .05; Figure 2). The distance covered by both groups increased progressively over time throughout the study. At discharge, both groups covered similar distances (314 ± 32 vs 311 ± 58 m). Conversely, at the 3-month follow-up, patients in group I-BB covered greater distances than those in group BB (370 ± 55 vs 347 ± 42 m; P = not significant; Figure 2).

Distance covered by patients with coronary artery bypass graft (CABG) in group BB (light gray columns) and patients with CABG in group I-BB (dark gray columns) during the 6-minute walking test at admission, discharge, and 3-month follow-up. *P < .05 (between BB and I-BB). Standard deviation is plotted.
In group BB, the median distance covered increased by 100 m (range 80-130 m) from admission to discharge, by 40 m (range 0-60 m) from discharge to follow-up, and by 135 m (range 80-177 m) from admission to follow-up. The corresponding increases in the group I-BB were 120 m (range 80-170 m), 40 m (range 8-88 m), and 170 m (range 130-235 m; P < .05 vs other group; Figure 2).
Baseline heart rate decreased over time in both groups (Table 2), as did myocardial workload as measured by the double product. There was no difference in mean exercise heart rate between the groups during 6MWT at admission or discharge (Figure 3). However, at the 3-month follow-up, the heart rate at each of the 6 minutes of the 6MWT was significantly lower in I-BB patients than in BB patients (all P < .05).
Exercise Capacity, Diastolic Function, and Systolic Function in Patients With Coronary Artery Bypass Graft, at Admission, Discharge, and 3-Month Follow-Up, According to the 2 Different Therapies.

Abbreviations: BB, bisoprolol; I-BB, Ivabradine/bisoprolol; LVEDD, left ventricular end-diastolic diameter; LVESD, left ventricular end-systolic diameter; LVIVS, left ventricular interventricular septum; LVPWT, left ventricular posterior wall thickness; 6MWT, 6-minute walking test; LVEF, left ventricular ejection fraction.
a P < .05.
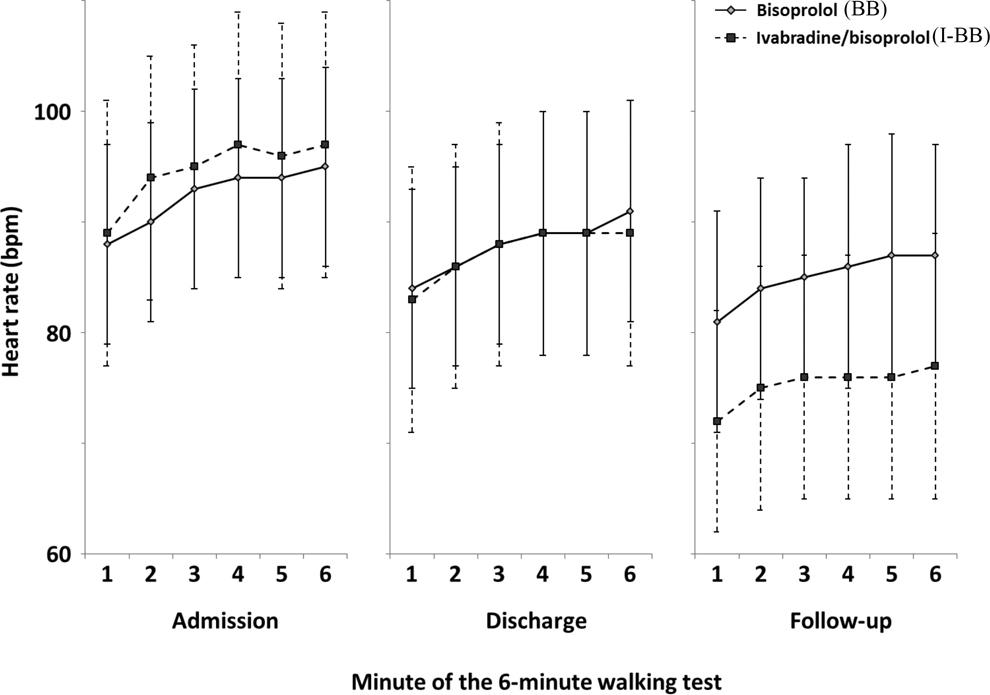
Heart rate at each minute of the 6-minute walking test at admission, discharge, and follow-up of patients with coronary artery bypass graft (CABG) in group BB (light gray diamonds, solid lines) and patients with CABG in group I-BB (dark gray squares, dotted lines).
At admission, both groups had similar distribution patterns of diastolic function status (normal, altered, and pseudonormal patterns). In I-BB patients, normal diastolic function was progressively restored. Normal diastolic function was observed in 24%, 50%, and 79% of patients at admission, discharge, and follow-up, respectively (Table 2). The opposite occurred in BB patients, with normal diastolic function observed in 23%, 19%, and 16% of patients at equivalent time points.
Both groups had similar EF at admission (57% ± 3%). The I-BB patients had significantly higher EFs than BB patients (62% ± 4% vs 59% ± 4%) and at follow-up (66% ± 3% vs 59% ± 3%; P < .05; Table 2).
Discussion
Beta-blockers are commonly used in patients with CABG having previous myocardial infarction or heart failure; indeed, in 65% to 89% of all patients with CABG, beta-blockers are an integral part of secondary prevention. Beta-blockers should be prescribed soon after surgery, as suggested by ACCF/AHA Guidelines, to prevent supraventricular arrhythmias. Furthermore, it seems to be useful to reduce ischemic burden, especially in patients with incomplete myocardial revascularization due to very small target vessels. Finally, the use of postoperative beta-blockers seem to reduce mortality even up to 74 months, also in patients without heart failure or previous myocardial infarction. 17
Our study showed that the addition of ivabradine to low-dose bisoprolol (1.25 mg once daily) in patients who underwent cardiac rehabilitation after recent CABG had further benefits compared with standard medical therapy including bisoprolol 2.5 to 3.75 mg once daily. The administration of the ivabradine/bisoprolol regimen shortly after CABG was associated with improved functional status, enhanced diastolic function, and increased LVEF, with no negative cardiovascular effects. The improvement in response to stress following a minor increase in heart rate for equivalent load allows workload to increase. Our study confirms previous findings that the addition of ivabradine to standard therapy including bisoprolol can improve exercise capacity in angina. 24
Cardiac surgery and cardiopulmonary bypass are triggers for inflammation and apoptosis. 25 Transient myocardial ischemia and the ischemia–reperfusion phenomenon lead to myocardial stunning. There are 2 main determinants of this phenomenon: local production of free oxygen radicals and disturbance of myocyte calcium homeostasis. Inflammatory response, operative trauma, cardioplegia and priming volume, and nonpulsatile flow during cardiopulmonary bypass may impair both systolic and diastolic function in the postoperative period.
Ivabradine has previously been shown to reduce heart rate after myocardial stunning, which may also occur after percutaneous coronary intervention for ST-segment elevation myocardial infarction (STEMI). 26 In eValuation of the IntraVenous I f inhibitor ivabradine after ST-segment elevation mYocardial infarction (VIVIFY), the use of intravenous ivabradine in STEMI produced a rapid and sustained reduction in heart rate, which was safe and well tolerated without affecting blood pressure or hemodynamics. 26 Optimization of hemodynamic parameters (ie, heart rate, ventricular filling pressure, and mean arterial pressure) is crucial in the postoperative phase.
Beta-blockers have well-documented direct effects on cardiovascular and pulmonary function, causing symptoms such as fatigue and dizziness. 27 Because of these effects and other adverse effects—hypotension, dyspnoea, cardiac decompensation, and excessive bradycardia—target dose of beta-blockers may be difficult to achieve. 28 Adverse effects like fatigue and dyspnoea may also help explain why beta-blockers have been shown to limit exercise capacity in healthy individuals. 29 Ivabradine could play a crucial role in the setting of cardiac rehabilitation, as it is devoid of inotropic, lusitropic, or vasoactive effects. 12 The different mechanisms of action of ivabradine and beta-blocker responsible for reducing heart rate mean the combination of ivabradine with low-dose bisoprolol appears to be a valuable option in patients with CABG undergoing cardiac rehabilitation. 12,30
Limitations
As resting heart rate reduction may not be a class effect of beta-blockers, 9 caution should be used in interpreting our findings with the beta-blocker bisoprolol more generally. Our study examined several efficacy parameters, but data on the safety and tolerability of the combination are lacking. However, the efficacy findings are clinically pertinent and the satisfactory short-term safety and tolerability of ivabradine and bisoprolol in combination have been observed elsewhere. 24
Conclusion
In patients undergoing cardiac rehabilitation after a recent CABG, the addition of ivabradine to standard therapy including low-dose bisoprolol 1.25 mg resulted in better improvement in exercise capacity, diastolic function, and recovery of systolic function compared with standard therapy including low-dose bisoprolol 2.5 to 3.75 mg.
Footnotes
Appendix A
Cardiac Rehabilitation Program.

| Phase II | Phase III | |
|---|---|---|
| Frequency | Once per day | 3-5 times per week |
| Entity | 60%-80% of maximal theoretical heart rate | 70%-80% of maximal theoretical heart rate |
| Duration | 20-60 minutes | 30-60 minutes |
| Type of exercise | Treadmill, cycle ergometer | Jogging, cycle, noncompetitive activities |
Author Contributions
Stefania Marazia and Michele Di Mauro contributed to conception or design; acquisition, analysis, or interpretation; drafted the article; critically revised the article; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy. Lucia Urso contributed to acquisition, analysis; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy. Marco Contini, Salvatore Zaccaria, and Filippo M. Sarullo contributed to conception, critically revised the article, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy. Marco Pano contributed to acquisition, analysis, or interpretation; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy. Vincenzo Lenti contributed to conception or design, drafted the article, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.