
Abstract
Purpose:
According to the literature, estradiol has a direct vasodilator action by means of endothelium-derived relaxing factor synthesis. The present study aims to evaluate the acute hemodynamic effects of intranasal 17-β-estradiol on cerebral and lower limb arterial circulation in postmenopausal women.
Methods:
Sixteen healthy women in natural menopause (mean age: 54 ± 3 years) were investigated for at least 6 months, each receiving 300 µg of intranasal 17-β-estradiol. We evaluated the heart rate, systolic/diastolic blood pressure, peak systolic velocity, end-diastolic velocity, and velocity–time integral (VTI) at the level of internal carotid and posterior tibial arteries, before and after 30, 60, and 180 minutes of drug administration.
Results:
After intranasal 17-β-estradiol administration, the internal carotid artery VTI showed statistically significant (P < .05) variations at all the time intervals after administration of the drug (30, 60, and 180 minutes) when compared with “time zero” (T0, ie, the speed recorded at baseline before drug administration). No significant variation was found at the posterior tibial artery. The systolic/diastolic blood pressure and heart rate did not significantly differ before and after drug administration.
Conclusions:
The administration of a single intranasal dose of 17-β-estradiol in healthy postmenopausal women increased cerebral perfusions, whereas the effect on peripheral circulation was much more limited.
Introduction
Studies in cellular, animal, and human models suggest a potential role of estrogens in cardiovascular protection, which occurs through nongenomic rapid effects and genomic long-term effects. 1 Epidemiologic studies show that women in premenopause have a lower risk of experiencing cardiovascular disease events than men of similar age. 2
In 1996, Clarkson showed that estrogens are able to promote primary prevention of arteriosclerosis in female monkeys when given immediately after oophorectomy. 3
The cardiovascular protection provided by estrogens is partly exerted by inducing antiatherogenic serum lipid profile variations.1,4 However, the main site of the estradiol (E2) cardioprotective mechanisms is related to direct endothelial effects. The E2 influences on the endothelium are complex. 5 The vasomotor effect depends on the genomic action of β-estrogen receptors, which activate nitric oxide (NO) synthase and consequently increase NO production, thus modulating vasoreactivity. 5 Both acetylcholine-induced and flow-dependent vasodilation are preserved or potentiated by estrogen treatment in both animal models and humans.5,6 Indeed, E2 increases the endothelial production of NO and prostacyclin and prevents early atheroma through endothelium-mediated mechanisms. 6 Increased NO production elicits vasodilatation in arteries with a normal endothelium and might attenuate or even abolish it in arteries with endothelial dysfunction. 7
The E2 also acts on the endothelium and vascular smooth muscle cell calcium channels, promoting short-term vasodilatation immediately after its administration. 8 The E2 treatment inhibits voltage-dependent type 2 calcium (Ca2+) channels and controls potassium (K+) flow through the membrane, opening voltage-activated cyclic adenosine monophosphate-dependent K+ and Ca2+ channels. 8 This action has recently been shown and is mediated by α-estrogen receptors present in smooth muscle cells of the coronary vascular wall. 8
The nasal route is an effective and well-established route of E2 delivery. 9 Nasal administration produces a pulsed profile of plasma E2, with systemic plasma levels rising rapidly and returning to preadministration levels within 12 hours. 10
We have already shown that after transvaginal administration, steroids may be distributed preferentially to the uterus due to the existence of local distribution mechanisms.11,12 After vaginal administration of progesterone, the endometrial levels of the hormone were markedly higher than those expected, based on the systemic levels reached. 11 Similarly, vaginal administration of micronized E2 resulted in preferential absorption of E2 in the endometrium, consistent with a “uterine first pass” effect. 13
The aim of the present study was to evaluate whether, after intranasal administration of E2, a local preferential distribution of the hormone takes place. For this purpose, the acute hemodynamic effects of intranasal 17-β-estradiol administration on head circulation (internal carotid artery) and systemic vessels (posterior tibial artery) in postmenopausal women were compared. The hemodynamic evaluation was based on the comparison of the arterial velocity–time integral (VTI) in different districts.
Materials and Methods
A total of 16 healthy women volunteers in menopause for 3.2 ± 2.7 years, aged 54 ± 3 years (mean ± standard deviation [SD]), and attending the Section of Cardiovascular Diseases, Department of Emergency and Organ Transplantation, Bari University General Hospital (Italy), were enrolled in the study. The average weight of the patients was 70.4 ± 14.4 kg. Table 1 presents the general characteristics of the study population according to the findings of our research. Recruitment was performed on an outpatient basis, and the diagnosis of menopause in all patients, based on anamnestic data of amenorrhea for at least 6 months, had been confirmed by laboratory findings of serum levels of E2 < 30 pg/mL and follicle-stimulating hormone > 40 mIU/mL. None of the women recruited practiced hormone replacement therapy for menopause or took drugs or substances that act on the cardiovascular system or cause vasomotor alterations.
General Characteristics of the Study Population.a

a Data are presented as mean values ± standard deviation or as number and/or percentage.
The exclusion criteria were obesity, defined as a body mass index (calculated as weight (kg)/height2 (m)2) > 30; hypertension, defined as a systolic blood pressure > 140 mm Hg or a diastolic blood pressure > 90 mm Hg, or a pharmaceutical history of antihypertensive drug use; history of headaches; history or presence of thrombotic disease or hormone-sensitive cancers; severe alterations in glucose, lipid, and liver enzyme serum concentrations; severe nasal obstruction; and allergic rhinitis.
The study was approved by the Institutional Review Board of Bari University General Hospital and done in accordance with the principles of the Helsinki Declaration. The patients were informed about the aim of the study, and their signed consent was obtained.
All patients received 17-β-estradiol through a nasal spray formulation containing a cyclodextrin carrier (Sprediol; Stroder, Florence, Italy).
Each patient received 2 sprays (1 per nostril) of a dose of 300 µg of E2; intranasal applications were done in all patients by 1 health care professional.
Before and after 30, 60, and 180 minutes of administration, the patients were assessed for hemodynamic parameters: heart rate, systolic and diastolic blood pressure, Doppler analysis of the internal carotid artery and the posterior tibial arteries with the evaluation of peak systolic velocity (PSV) and end-diastolic velocity (EDV), and VTI.
Doppler analysis was done in spectral analysis mode with the HP Agilent Sonos 1000, using a probe of 5-MHz CW as follows: For the internal carotid artery, the recording was done at the level of the jugular vein with an angle of incidence < 20°; for the posterior tibial artery, the recording was done at the level of the medial malleolus with an angle of incidence < 20°.
Statistical Analyses
The data are expressed as mean values ± SD, except for the category-specific variables, which are expressed in percentages. The analysis of variance was used for repeated measures. All the variables were normally distributed. A value of P < .05 was considered statistically significant.
Results
The VTI, that is, the parameter that best expressed the velocity temporal variations at the level of the arteries investigated showed statistically significant variations (P < .05) in velocity (cm/s) in the vessels of the cerebral district (internal carotid artery) when compared with T0 (the speed recorded at baseline before drug administration). These significant results were maintained during all the assessments at 30, 60, and 180 minutes after administration of the drug. No significant variation was found at the posterior tibial artery (Table 2).
The VTI Values in Various Districts Expressed as Mean ± Standard Deviation.

Abbreviation: VTI, velocity–time integral.
Note: Each value at 30, 60 and 180 minutes had been compared with baseline. Thus, p < 0.05 is related to the comparison between the values 30, 60 and 180 minutes of internal carotid artery VTI and baseline internal carotid artery VTI.
aP < 0.05.
In the cerebral district, compared with T0 the speed variations were in the positive range; that is, the values tended to increase after drug injection. In particular, the peak velocity in the internal carotid artery was recorded at 60 and 180 minutes after spray application. After this period, the speed was still moderately higher than that at the baseline (Figure 1).
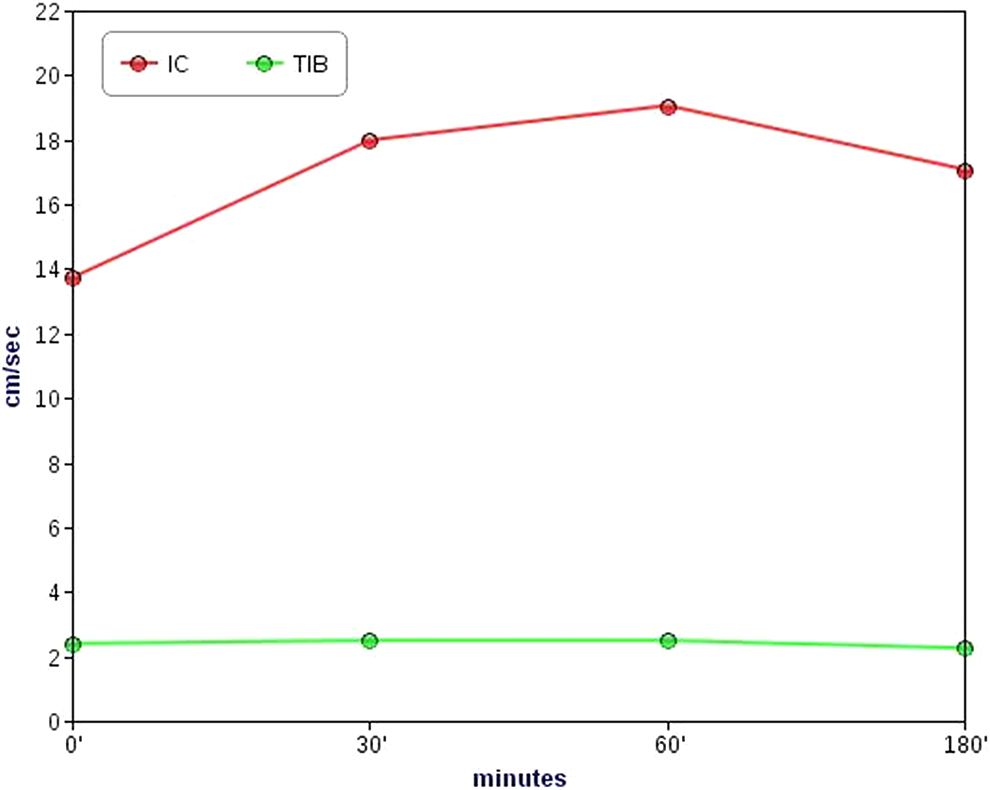
Variation in the velocity–time integral of the internal carotid (IC) artery and posterior tibial (TIB) artery.
After 30 minutes, a 35% increase in the VTI was recorded at the level of the internal carotid artery; this value was higher than the approximately 3% speed variation calculated at the level of the posterior tibial artery. After 60 minutes, the percentage increase for the internal carotid artery was 43%, whereas at 180 minutes, a flow velocity 20% higher than the baseline value at the level of the internal carotid artery was recorded.
However, the PSV and EDV showed a trend toward amelioration and improvement in vascular function similar to that observed in the VTI (data not shown).
Finally, because the heart rate and systolic and diastolic blood pressure did not differ significantly after drug administration, we could exclude the influence of these systemic hemodynamic parameters on the flow variations recorded at several arterial districts considered in our analysis.
Discussion
The data in this study showed that after acute intranasal E2 administration, there was a more pronounced change in the vascular hemodynamics of the cerebral vessels (internal carotid) than that of the peripheral vessels (posterior tibial artery). This result seemed to suggest the possible existence of a preferential distribution of the E2 to the head circulation, perhaps due to the passage of drug through the nasal mucosa. This indicates the possibility of considering the nasal route as an effective pathway for improving the vasodilatory effects of drugs in the head districts.
In particular, 30 minutes after administration, the posterior tibial artery flow increased by only 3%, whereas in the cerebral district, a 35% increase in internal carotid artery flow was recorded.
These results could have at least 2 explanations. It can be speculated that the arteries of the cerebral district have a higher sensitivity to E2 than the tibial artery, and therefore, the effects of the administration could be different. However, to our knowledge, there are no existing data about the different distributions of E2 receptors and the type of receptors among the arteries investigated in this study. Alternatively, it can be speculated that after intranasal administration, a preferential distribution of E2 takes place in the cerebral districts according to the neighborhood relationship between the latter and the nasal pathway of drug infusion.
The nasal route is, effectively, a known preferential route for delivering drugs to the brain and overcoming the blood–brain barrier (BBB). 14 Drugs may reach the brain by transethmoidal absorption through areas not protected by the BBB and then be transported through the perineurium of the olfactory nerve, thus reaching the olfactory lobe and the base of the brain.14,15 Through a pinocytosis process, the drug could run throughout the internal axons of the olfactory nerves, adopting a retrograde direction.14,15 The final distribution of the E2 is due to its fat solubility into the lipid field of the brain. Another possible explanation may lie in the vascular-mediated mechanism of countercurrent distribution of drugs based on different gradients from blood, veins and arteries. 15
The nasal route and the fast delivery of the drug to the brain territories allow an optimal route of drug administration in case of brain diseases. Furthermore, it can be speculated that nasally administered 17-β-estradiol could influence the development or reduction in symptoms related to menopause. Naturally, further studies are needed to examine this hypothesis. Nevertheless, we observed the acute effect of 17-β-estradiol on cerebral vessels; the preferential distribution pattern of such a drug would be worth studying to better observe the cerebral zones that are influenced by its administration and, thus, determine its clinical effects on the physiology of normal women.
Our research, which is based on an international literature review,16–18 seems to reveal original findings considering that limited data exist about the effect of E2 distribution, particularly on postmenopausal women. Krejza et al16,17 tried to explain such considerations in their works, in which they analyzed the cerebrovascular impedance during the menstrual cycle in women after 17-β-estradiol infusion. The findings of their research demonstrate the effects of estrogen on vascular districts, although, unlike our research, they considered only women who were not in menopause. However, similar to our work, their study was also limited by the small sample size. One of the limitations of our study is, in fact, the small group of patients considered for our analysis, which led us to hypothesize, rather than making definitive conclusions, about a complex problem, such as the effects of sexual hormones on cerebral districts.
It is interesting to point out the role of hormones on brain circulation. In fact, Liu et al 18 underlined the difference in sexual hormone influence on brain circulation between women and men. It actually appears that women are protected from cerebrovascular disease more than men; however, the authors presumed that this consideration was not entirely due to the involvement of sexual hormones, because sex differences in brain injuries still remain after menopause or even in the pediatric population. For this reason, the dimorphism related to such an argument could only be the surface of a deeper mechanism that is not well understood at all and is worthy of further assessment and research.
Furthermore, one could speculate that the arteries involved in our study are of different kinds; the internal carotid artery is an elastic type, whereas the tibial artery is a muscular type. This could be considered as a bias in the evaluations done in our research. In the literature, we found no study comparing the parallel effects of E2 administration on different kinds of arteries. Nevertheless, we found that E2 could act on epicardial coronary arteries (ie, muscular types, such as the tibial artery) by increasing their diameter due to an overall increased production of NO.19–21 The consequence of this assumption is that even muscular arteries would have no significant differences compared to elastic arteries, in terms of dilating behavior. Nevertheless, this assumption deserves further investigation from specific research. In the present study, it is quite difficult to consider whether or not our choice was a bias due to the lack of information about this argument in the literature.
Another limitation of our study is the lack of a control group for comparing the results. Nevertheless, the original hypothesis of evaluating the changes in the VTI of the same arteries before and after drug administration made the presence of a control economically difficult. Future works could certainly include a placebo or control group to better define their results.
Finally, we can state that in our population and despite the small sample considered, 17-β-estradiol injection within nasal cavities actually improved brain circulation. This result opens the way to new developments, and 17-β-estradiol could possibly be used to acutely improve the cerebral vascular bed for the evaluation of treatment for cerebrovascular diseases related to vasculature damages. However, further studies are needed to validate the results.
Conclusions
The data in this study show that intranasal 17-β-estradiol administration at a dose of 300 µg induces a significant dilating effect on cerebral vessels, whereas the effect on peripheral vessels is much more limited. This finding could possibly provide a glimpse of the potential implications for the prevention of and therapy for brain disorders with vascular or chronic degenerative etiology, such as Alzheimer disease and multi-infarct encephalopathy. Nevertheless, further studies and trials should be done to confirm our results.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.