
Abstract
Objectives:
We sought to investigate the experimental therapeutic effects and mechanisms of iptakalim, a new adenosine triphosphate (ATP)-sensitive potassium channel (KATP) opener, on monocrotaline (MCT)-induced pulmonary arterial hypertension (PAH) and right heart ventricle remodeling in rats.
Methods:
Rats were injected with a single dose (50 mg/kg, ip) of MCT and given iptakalim (1, 3, and 9 mg/kg·per d, orally [po]) or saline for 28 days. The hemodynamic and morphometric parameters were assessed. Tissue and plasma samples were collected for histological and molecular analysis.
Results:
Treatment with iptakalim at daily oral doses of 1, 3, and 9 mg/kg from the day of MCT injection attenuated the high right ventricle systolic pressure (RVSP) and the increased weight ratio of right ventricle (RV) to left ventricle (LV) plus septum (S) (RV/(LV+S)), decreased heart rate (HR) and decreased mean arterial pressure (MAP), inhibited the RV myocardial tissue cell apoptosis, and the RV myocardial cell B-type natriuretic peptide (BNP) protein expression. Iptakalim also decreased the serum levels of nitric oxide (NO), endothelin 1 (ET-1), BNP, and the levels of NO, ET-1, and tumor necrosis factor-alpha (TNF-α) in the lung tissue.
Conclusion:
These results indicate that iptakalim prevents MCT-induced PAH and RV remodeling and its mechanisms are related to inhibiting the pathological increases in NO, ET-1, BNP, and TNF-α, and Iptakalim may be a promising candidate for the treatment of PAH.
Introduction
Pulmonary arterial hypertension (PAH) is a group of chronic and progressive diseases characterized by a sustained elevation of pulmonary vascular resistance, leading to right ventricular (RV) failure and premature death. 1,2 The exact pathogenesis of PAH is not fully understood, but recent evidence demonstrates that elevated pulmonary artery pressure is the result of vasoconstriction and structural remodeling of pulmonary vessels. 3,4 There are multiple and complex mechanisms involved in the progression of PAH, including proliferation of pulmonary arterial smooth muscle cells, endothelial dysfunction, and inflammation. 5 –8
Iptakalim, 2,3-dimethyl-N-(1-methylethyl)-2-butanamine hydrochloride, is a new structural type of adenosine triphosphate–sensitive potassium channel (KATP) opener, preferentially activating SUR2B/Kir6.1 subtype, without activation of SUR1/Kir6.2. 9 –11 Its antihypertensive effects have been demonstrated in spontaneously hypertensive rats, renal hypertensive dogs, and patients. 12 –14 Our previous studies showed that iptakalim inhibits the remodeling of the pulmonary artery in hypoxic pulmonary hypertensive rats and prevents progression of cardiac hypertrophy to failure induced by a pressure overload, via augmenting the release of nitric oxide (NO) and inhibiting the endothelin 1 (ET-1) system during endothelial dysfunction, thereby resulting in endothelial protection. 15,16 Iptakalim also inhibited the ET-1-induced proliferation of cultured human pulmonary arterial smooth muscle cells and rabbit pulmonary arterial smooth muscle cells, which suggested that iptakalim might be a promising candidate for the treatment of pulmonary arterial remodeling in PAH. 17,18
Chronic hypoxia and injection of monocrotaline (MCT) can establish PAH animal models, but the mechanism of the 2 models is different. Moreover, the performance of both models and the degree of damage are also different. Hypoxic PAH is usually only moderate and limited to medial hypertrophy with varying degrees of adventitial change, but may progress to extensive remodeling in some species. However, MCT-induced PAH is severe with endothelial degeneration or hyperplasia, hypertrophy of medial smooth muscle, and adventitial edema, which is used as a standard model for PAH. 19 –21
Thus, we hypothesize that iptakalim might be effective in the treatment of PAH induced by MCT.
Materials and Methods
Reagents
Iptakalim was synthesized by Thadweik Academy of Medicine (Beijing, China). Monocrotaline was purchased from Sigma-Aldrich (St Louis, Missouri). All other chemicals and materials were obtained from local commercial sources.
Experimental Protocol
All procedures were performed in accordance with the protocol outlined in the Guide for the Care and Use of Laboratory Animals published by the US National Institute of Health (NIH publication no. 85-23, revised 1996) and approved by the local animal care and use committee. To assess preventive effects of iptakalim on MCT-induced PAH, adult male Wistar rats (180-220 g) were randomly divided into 5 groups (n = 10 per group): model group, 3 iptakalim treatment groups, and the control group. In the model group and the 3 iptakalim treatment groups, rats were given a single intraperitoneal injection of MCT (50 mg/kg), while the rats in the control group received an equal volume of physiological saline. The rats in the iptakalim treatment and model groups were further assigned at random to receive either iptakalim (1, 3, and 9 mg/kg per d, orally [po], respectively) or an equal volume of physiological saline from the day of the MCT injection up to the 28th day. Iptakalim was dissolved in saline and administered orally via a gastric tube. Iptakalim or vehicle was orally administered once a day in 2 mL/kg.
Hemodynamics and Cardiac Remodeling Index
On day 28, all animals were weighed and anesthetized with a mixture of xylazine (5 mg/kg) and sodium pentobarbital (15 mg/kg, intraperitoneal injection). After stable anesthesia was obtained, 2 polyethylene catheters were inserted into the RV through the right jugular vein and the left carotid artery, respectively, for hemodynamic measurements. 6,22 Right ventricle systolic pressure (RVSP), systemic blood pressure, and heart rate (HR) were measured with a polygraph system (RM-6000, Nihon Kohden Kogyo Co, Ltd, Japan). Thereafter, blood samples were collected and animals were killed by exsanguination. The thoracic cavity was opened to expose the still beating heart. The heart and lung were rapidly removed, rinsed in ice-cold 0.9% NaCl solution, blotted, and then the heart was weighed. The heart weight (HW) index was calculated by dividing HW by body weight (HW/BW). The left ventricles ([LVs] including interventricular septum, LV + S) and RV free walls were collected separately and weighed. The RV weight index (RV/(LV+S)) was calculated. The right lung was dissected into pieces, frozen in liquid nitrogen, and then stored at −80°C until biology assay.
Histological Analysis
Right ventricle and left lung samples were immersion fixed in 10% buffered formalin and embedded in paraffin. Sections (4 μm) were cut and stained with hematoxylin and eosin. The structural changes in tissues were investigated using a light microscope. Intra-acinar vessels were analyzed to assess the distribution and the degree of muscularization according to the accompanying airway such as terminal bronchiole. The medial thickness and external diameter were recorded and assessed microscopically for the degree of arterial muscularization. The medial wall thickness was measured at 2 locations of each artery and was expressed as the summation of the 2 points of (medial thickness/external diameter)×100 (in percentage).23
Measurement of Serum NO Production, Plasma B-Type Natriuretic Peptide, and ET-1 Levels
Within 30 seconds after collection, heparinized blood was centrifuged for 10 minutes at 3000 rpm, and all samples were stored at −70°C until they were assayed. Because of its instability in physiological solutions, most of the NO is rapidly converted to nitrite (NO2 −) and further to nitrate (NO3 −). Serum levels of NO2 −/NO3 − were measured using NO Detection Kit (Nanjing Jiancheng Bioengineering Institute, Nanjing, China), according to the manufacturer’s instruction. Briefly, nitrate was converted into nitrite with aspergillus nitrite reductase, and the total nitrite was measured with the Griess reagent. The absorbance was determined at 540 nm with a spectrophotometer according to the instructions provided by the manufacturer. Both ET-1 and B-type natriuretic peptide (BNP) were measured using commercial radioimmunoassay kits (Eastern Asia Radioimmunity Research Institute, Beijing, China).
Measurement of NO, ET-1, and Tumor Necrosis Factor-α in Lung Tissue
Freeze-stored lung was thawed, weighed, and homogenized in 0.8 mL of physiological saline per 200 mg of tissue. After homogenization on ice, the tissue samples were centrifuged (15 minutes, 4000 rpm at 4°C). The supernatant was used for measuring NO, ET-1, and tumor necrosis factor-α (TNF-α). The NO level in lungs was measured using NO Detection Kit (Nanjing Jiancheng Bioengineering Institute, Nanjing, China). The levels of ET-1 and TNF-α in lung tissues were measured using commercial radioimmunoassay kits (Eastern Asia Radioimmunity Research Institute).
Assessment of the RV Myocardial Tissue Cell Apoptosis
In situ terminal deoxynucleotidyl transferase dUTP nick end labeling (TUNEL) was performed using an apoptosis detection kit (DeadEnd Colorimetric TUNEL System; Promega, Madison, Wisconsin). The RV myocardial tissues were immersion fixed in 10% formalin and embedded in paraffin. Paraffin sections of 4-μm-thick were cut and stained according to the manufacturer’s instructions. The number of TUNEL-positive cardiac myocyte nuclei was expressed as percentage of the total number of cardiac myocyte nuclei and called the apoptosis index. Five rat hearts in each group were randomly selected and 2 fields in each rat heart were analyzed (light microscopy, 400 magnifications).
B-Type Natriuretic Peptide Protein Expression in the RV Myocardial Tissue
The RV myocardial tissues were immersion fixed in 10% formalin and embedded in paraffin. Paraffin sections of 4-μm-thick were cut, deparaffinized, and dehydrated. The streptavidin–peroxidase conjugate (SP) method was performed in sections stained with a primary polyclonal antibody (ab19645, abcam) to BNP. The degree of BNP expression was assessed by the mean optical density. Five rat hearts in each group were randomly selected and 2 fields in each rat heart were analyzed (light microscopy, ×400 magnifications).
Statistical Analysis
Data are expressed as mean ± standard deviation (SD). Differences between groups were assessed by analysis of variance (ANOVA) and Student Newman–Keuls post hoc test for multiple comparisons. Statistical significance was accepted at P < .05.
Results
Hemodynamic Effects of Iptakalim
As shown in Table 1, on day 28 after MCT administration, RVSP, a reflex of PAH, in MCT-induced model group was elevated markedly compared with that in control group. However, HR and mean arterial pressure (MAP) in MCT-induced model group decreased significantly compared with the control group. Iptakalim at the daily oral doses of 1, 3, and 9 mg/kg for 28 days ameliorated the increase in RVSP and reduction in HR and MAP.
Effects of Iptakalim on RVSP, HR, and MAP in the Pulmonary Arterial Hypertensive Ratsa
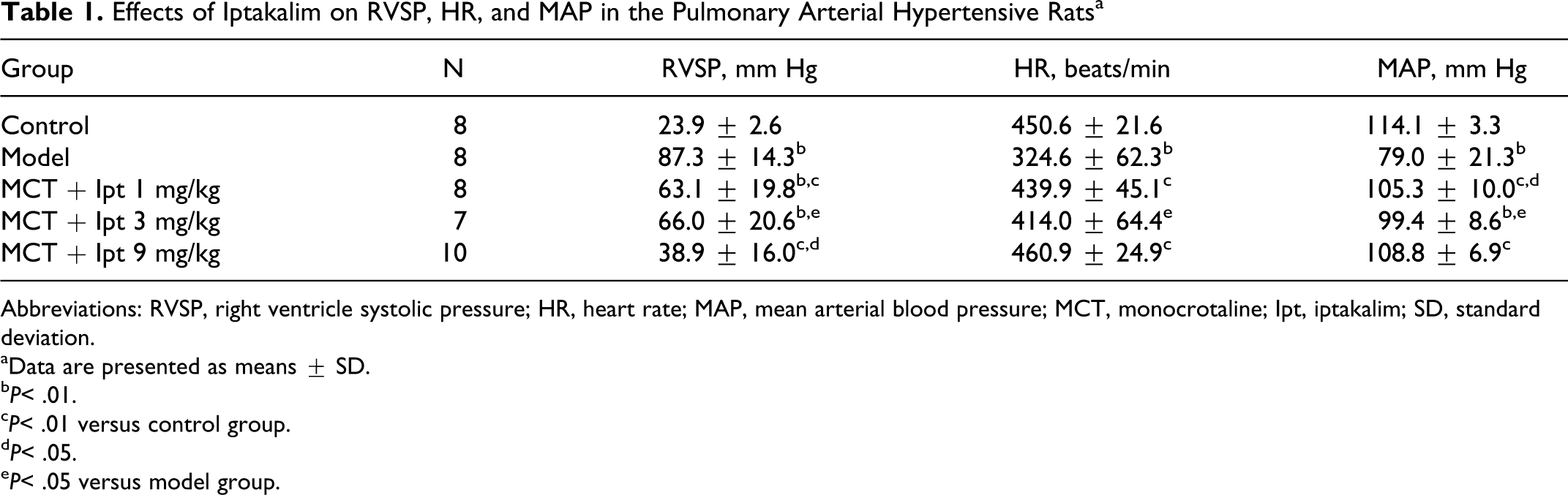
Abbreviations: RVSP, right ventricle systolic pressure; HR, heart rate; MAP, mean arterial blood pressure; MCT, monocrotaline; Ipt, iptakalim; SD, standard deviation.
aData are presented as means ± SD.
b P< .01.
c P< .01 versus control group.
d P< .05.
e P< .05 versus model group.
Iptakalim Reduces the RV Hypertrophy Induced by MCT
As shown in Table 2, on day 28 after MCT administration, HW, HW/BW, ratio of RV weight to LV plus septum (S) weight (RV/LV+S) in MCT-induced model group were elevated markedly compared with control group values; however, body weight (BW) in MCT-induced model group was decreased significantly compared with the control group. Iptakalim at the daily oral doses of 1, 3, and 9 mg/kg for 28 days ameliorated the increase in HW, HW/BW, and RV/LV+S. In addition, the body weight of the MCT-injected group did not differ from control with iptakalim treatment at the daily oral doses of 1, 3, and 9 mg/kg for 28 days.
Effects of Iptakalim on BW, HW, HW/BW, RV/(LV+S) in the Pulmonary Arterial Hypertensive Ratsa
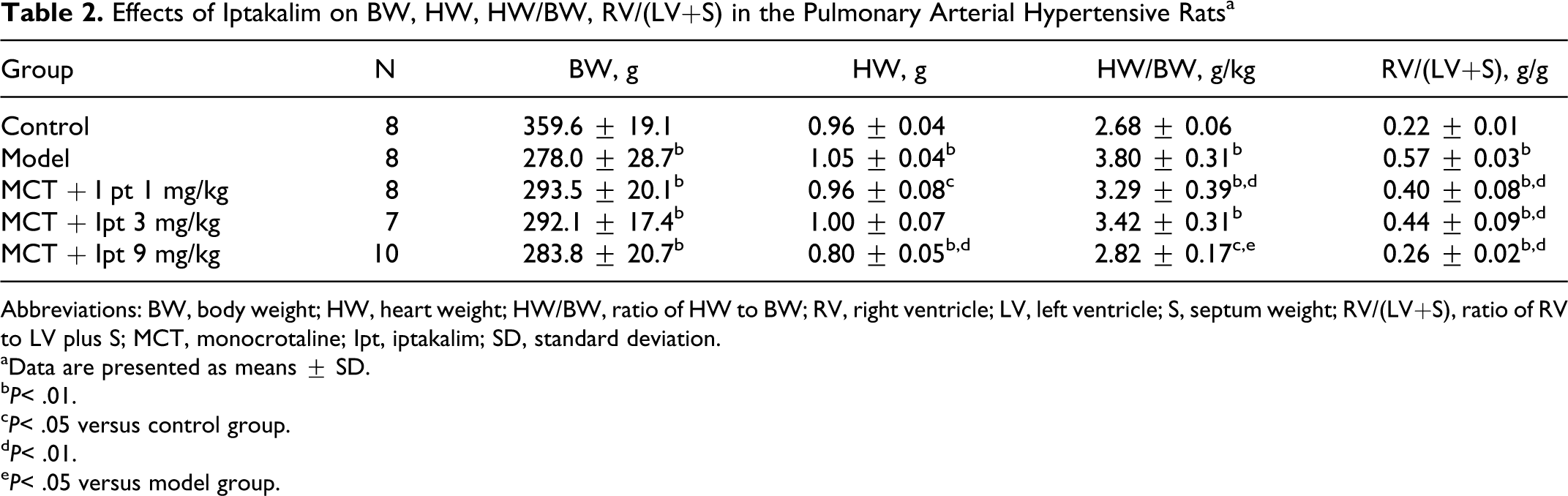
Abbreviations: BW, body weight; HW, heart weight; HW/BW, ratio of HW to BW; RV, right ventricle; LV, left ventricle; S, septum weight; RV/(LV+S), ratio of RV to LV plus S; MCT, monocrotaline; Ipt, iptakalim; SD, standard deviation.
aData are presented as means ± SD.
b P< .01.
c P< .05 versus control group.
d P< .01.
e P< .05 versus model group.
Iptakalim Downregulates BNP Protein Expression in the RV Myocardial Cells
Because it was well recognized that BNP is a molecular marker of heart failure, we determined the effects of iptakalim on the expression of BNP in myocardial cells. As shown in Figure 1, in the model group, the mean optical density of RV myocardial cell BNP protein expression dramatically increased when compared to control rats. These changes could be prevented significantly by treatment with iptakalim at the dose of 9 mg/kg per d for 4 weeks.
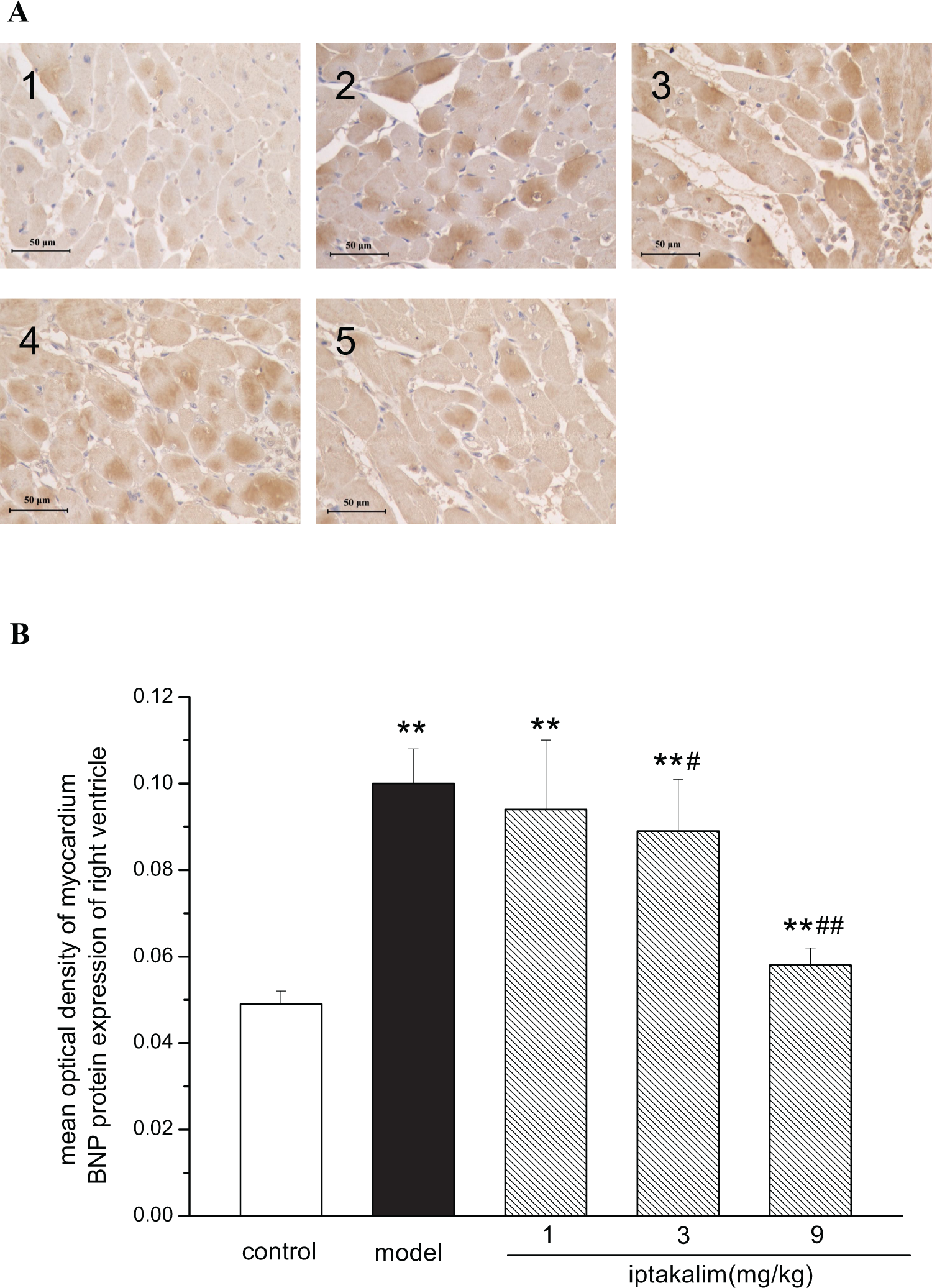
Effect of iptakalim on B-type natriuretic peptide (BNP) protein expression in right ventricular tissues of pulmonary arterial hypertensive rats induced by monocrotaline. A, Representative figure of BNP protein expression in right ventricular tissues (×400). B, Statistic results of BNP protein expression in right ventricular tissues. 1 indicates control; 2, model; 3, iptakalim 1 mg/kg group; 4, iptakalim 3 mg/kg group; 5, iptakalim 9 mg/kg group. Data are expressed as mean ± standard deviation (SD), n = 10. **P < .01 versus control group; # P < .05, ## P < .01 versus model group.
Iptakalim Inhibits Pathological Changes in Lung Tissues and RV Tissues
On day 28 after MCT administration, alveolar mononuclear cell infiltration was observed in lung tissue in areas of consolidation and fibroblasts. The wall of the pulmonary artery was thickened, and intimal smooth muscle cell disorder, hyperplasia, stenosis, and occlusion were also observed. The capillaries in lung tissues were expanded slightly and congested. The secretions of bronchia were increased, and necrotic epithelial cells, red blood cells, and edema fluid were found in the bronchial cavity (Figure 2A). Histological examinations demonstrated that fibrosis of the heart occurred in the RV myocardium. The numbers of monocytes and lymphocytes increased in myocardial interstitial tissues. Scattered, small sheets of multiple foci of myocardial necrosis were also observed in the RV myocardium derived from the model group (Figure 2B). The above mentioned pathological changes in lung tissues and RV tissues could be improved by treatment with iptakalim at the dose of 9 mg/kg per d for 4 weeks.

Effects of iptakalim on histological changes of the lung tissues and the right ventricles in pulmonary arterial hypertensive rats induced by monocrotaline (hematoxylin and eosin stain, ×200). A, Representative figure of the lung tissues. B, Representative figure of right ventricles. C, The medial thickness of pulmonary arteries accompanying terminal bronchiole. 1 indicates control; 2, model; 3, iptakalim 1 mg/kg group; 4, iptakalim 3 mg/kg group; 5, iptakalim 9 mg/kg group. Data are expressed as mean ± standard deviation (SD), n = 5. *P < .05, **P < .01 versus control group; # P < .05 versus model group.
The MCT-treated rats had significantly increased medial wall thickness of muscular pulmonary arteries corresponding to terminal bronchioles compared with that of the control group. Iptakalim at the dose of 9 mg/kg per d treatment could reduce the MCT-induced increase in medial wall thickness significantly (Figure 2C), suggesting that iptakalim at the high dose could attenuate MCT-induced pulmonary vascular remodeling.
Iptakalim Attenuated the RV Myocardial Tissue Cell Apoptosis Induced by MCT
In the model group, the rate of the RV myocardial tissue cell apoptosis dramatically increased compared with the control rats (Figure 3A). The cell apoptosis induced by MCT could be attenuated by treatment with iptakalim at the dose of 9 mg/kg per d for 4 weeks. But no obvious effects were observed in iptakalim 1 and 3 mg/kg per d treatment groups (Figure 3B).

Effects of iptakalim on myocardium cell apoptosis of the right ventricle in pulmonary arterial hypertensive rats induced by monocrotaline (terminal deoxynucleotidyl transferase dUTP nick end labeling [TUNEL] stain, ×400). A, Representative figure of myocardium cell apoptosis in right ventricular tissues. B, Statistic results of myocardium cell apoptosis in right ventricular tissues. 1 indicates control; 2, model; 3, iptakalim 1 mg/kg group; 4, iptakalim 3 mg/kg group; 5, iptakalim 9 mg/kg group. Data are expressed as mean ± standard deviation (SD), n = 10. **P < .01 versus control group; ## P < .01 versus model group.
Iptakalim Downregulated Serum NO Production, Plasma BNP, and ET-1 Levels
We assessed the concentrations of serum NO, plasma BNP, and ET-1 in pulmonary arterial hypertensive rats and found they were increased at the end of 4 weeks after MCT administration. After treatment with iptakalim at the doses of 1, 3, and 9 mg/kg per d for 4 weeks, these parameters were reduced significantly (Figure 4A-C).
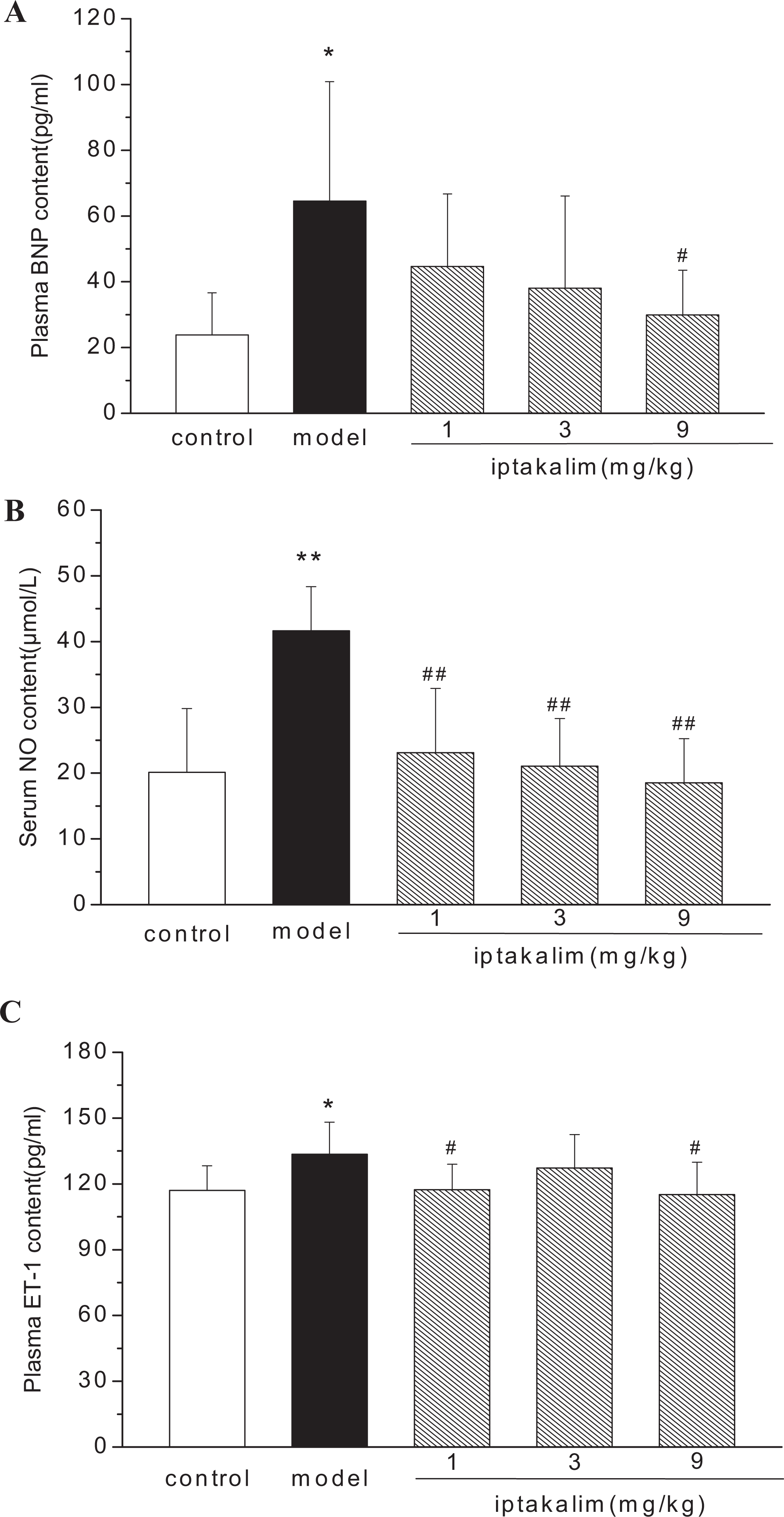
Effects of iptakalim on serum levels of NO and plasma levels of BNP and ET-1 in monocrotaline-induced pulmonary arterial hypertensive rats. Data are expressed as mean ± SD, (A) n = 5-10; (B) n = 7-8; (C) n = 7-10. *P < .05, **P < .01 versus control group; # P < .05, ## P < .01 versus model group. BNP indicates B-type natriuretic peptide; NO, nitric oxide; ET-1, endothelin 1; SD, standard deviation.
Iptakalim Suppressed TNF-α, NO, and ET-1 Levels in Lung Tissues
Accumulating evidence indicated that TNF-α, NO, and ET-1 play important roles in lung injuries induced by MCT. As shown in Figure 5, the lung TNF-α, NO, and ET-1 levels of the model group were increased significantly compared with those of the control group. These changes could be prevented by treatment with iptakalim at the dose of 1, 3, and 9 mg/kg per d for 4 weeks (Figure 5A-C).

Effects of iptakalim on TNF-α, NO, and ET-1 levels in lung tissues of monocrotaline-induced pulmonary arterial hypertensive rats. Data are expressed as mean ± SD, (A) n = 8-10; (B) n = 5-10; (C) n = 8-10. *P < .05, **P < .01 versus control group; # P < .05, ## P < .01 versus model group. NO indicates nitric oxide; ET-1, endothelin 1; SD, standard deviation; TNF-α, tumor necrosis factor-α.
Discussion
The MCT-induced rat has been widely used as an experimental model of PAH. 23 Monocrotaline is a pyrrolizidine alkaloid found in the plant species Crotalaria spectabilis. When injected into rats with a single subcutaneous or intraperitoneal administration, MCT undergoes hepatic transformation from the action of the cytochrome P450 monooxygenase system in the liver to form the MCT pyrrole (MCTP), which injures vascular endothelium of pulmonary vessels within several hours, activates platelets within 1 week, and causes enhanced reactivity of pulmonary vessels to vasoconstrictive substances and muscular hypertrophy of the media of pulmonary vessels, and then leads to PAH and RV hypertrophy. This model mimics the clinical pathological and physiological conditions of idiopathic PAH (IPAH). 24 The effects of iptakalim on pulmonary hypertension induced by hypoxia or ET-1 had been demonstrated in previous studies. 16 –18 The KATP subtypes found in the endothelium are mainly SUR2B/Kir6.1, which contribute to the maintenance of the resting membrane potential and regulate intracellular Ca2+ levels that in turn affect the production and release of NO. 25 Iptakalim, a newly selective KATP opener, activates SUR2B/Kir6.1 preferentially and is a promising drug that could protect against endothelial dysfunction through activating KATP channels in endothelial cells. 10,11,13,15,26 The purpose of this study, therefore, was to investigate the potential effects of iptakalim on PAH and RV hypertrophy progression using the MCT-induced PAH rat model.
In the present study, on day 28 after MCT administration, the rat model of PAH was established successfully and RV remodeling was characterized by elevation of RVSP, HW, HW/BW, RV/(LV+S). The overexpression of myocardial cell BNP proteins in RV accompanied by elevation in plasma BNP level indicated that PAH progressed gradually to right heart failure, and confirms that BNP is a potentially important clinical biomarker of heart failure. 27,28 Elevation in the levels of lung TNF-α, NO, and serum NO were accompanied by decreases in MAP and HR in PAH rats induced by MCT with a feature of time dependence. The lung injuries were similar to those reported by Speyer et al and Markovic et al. 29,30
Iptakalim alleviated pulmonary artery pressure and reversed pulmonary arterial modeling in animal models induced by hypoxia or ET-1. 16 –18 It restored the balance between the NO and ET signaling systems during endothelial dysfunction, by augmenting the release of NO and inhibiting the ET-1 system, resulting in endothelial protection. 26 Its therapeutic effects on pulmonary hypertension might be related to its endothelial protective effects.
Our current data showed that all doses of iptakalim-treated PAH rats (1, 3, and 9 mg/kg per d) induced by MCT for 28 days suppressed the development of PAH, pulmonary vascular remodeling, and RV remodeling, which were accompanied by reduction in the levels of the lung TNF-α, NO, ET-1, blood BNP, NO, and ET-1 compared with the MCT-induced rats. Meanwhile, the mean optical density of RV myocardial cell BNP expression and the rate of the RV myocardial tissue cell apoptosis markedly decreased compared with the MCT-induced rats. Whereas, after treatment with iptakalim, the MAP and HR in model rats were increased significantly. However, in the iptakalim-treated animals, 3 mg/kg per d of the iptakalim-treated group showed mixed effects. There were no dose–response effect on RVSP, MAP, HR, HW, HW/BW, RV/(LV+S), and ET-1 levels in the plasma or lung tissues; the mechanism of iptakalim on PAH induced by MCT needs further experimental research. In addition, although the increases in pulmonary artery pressure and RV hypertrophy were comparable in the rat hypoxia and MCT model, the NO levels in plasma or lung tissues reveal major differences between the 2 models. The levels of TNF-α in lung tissues implied that inflammatory cytokines might play an important role in the development and progression of MCT-induced PAH.
In MCT-induced PAH rats, endothelial dysfunction was characterized by increased levels of NO and ET-1 both in lung tissues and in blood plasma. The change in NO was different from those reported for endothelial dysfunction induced by hyperuricemia or pressure overload. 10,11,15 In these 2 animal models, the serum levels of NO were decreased significantly, which could be reversed by iptakalim treatment. But in MCT-indiced PAH rats, the MCTP mediates its effects through interaction with receptors on the surface of a variety of host cells. These interactions result in the production and release of numerous biochemical mediators including inflammatory cytokines, NO, and toxic oxygen radicals. 31 Inflammatory cytokines, such as TNF-α and interleukin 1 (IL-1), induced the overexpression of inducible NO synthase (iNOS) in vascular endothelial cells and myocardial cells, which increased the NO concentration levels in circulating blood multiple times higher than the normal physiological levels. Thus, the soluble guanylate cyclase (sGC) of vascular smooth muscle cells was activated, leading to the production of large amounts of cyclic guanosine monophosphate (cGMP), which caused the relaxation of vascular smooth muscle and decreased the systemic circulation blood pressure. 32 –34 The excessive NO produced combined with superoxide anion (O2 -) to produce peroxy nitrite (ONOO-). ONOO- could enhance cardiovascular endothelial cell and cardiac cell inflammatory damage and mediate histiocyte apoptosis, resulting in RV remodeling, pulmonary vascular remodeling, and PAH. 35 –44 In this PAH model, iptakalim treatment for 4 weeks not only decreased the high RVSP that is a reflex of PAH, but also reversed the pathological increase in levels of NO and ET-1.
In conclusion, our data suggests that MCTP, a dehydromonocrotaline metabolite, activates monocytes/macrophages to produce cytokines such as TNF-α and then induces excessive release of NO which in turn depresses cardiac function and causes injury of vascular endothelial cells directly and/or indirectly. All of these changes induce PAH, low systemic blood pressure, and HR. Iptakalim, a new KATP channel opener, prevented MCT-induced PAH, reduced RV remodeling, increased the MAP and HR, inhibited pathological NO release, ET-1 secretion, and TNF-α release in MCT animals. Results of this study suggest that iptakalim might be a promising candidate for the treatment of PAH.
Footnotes
Authors' Note
JunShan Li, ChaoLiang Long, WenYu Cui, and Hai Wang designed the research; JunShan Li performed the research; JunShan Li and ChaoLiang Long analyzed data; JunShan Li and ChaoLiang Long wrote the paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from National New Drug Research and Development Key Project (2010ZX09401-307, 2008ZXJ09004-018 and 2009ZX09301-002).