
Abstract
Introduction
The role of surgery in stage III non-small cell lung cancer (NSCLC), particularly in the presence of ipsilateral mediastinal lymph node involvement (N2), remains controversial. Criteria for resectability differ among existing clinical guidelines and are particularly difficult to apply in countries with limited access to advanced diagnostic and therapeutic resources. Accordingly, this Colombian expert consensus aimed to define resectability criteria for stage III NSCLC within real-world resource-limited contexts.
Methods
This expert consensus statement was developed by a multidisciplinary panel of Colombian experts following the European Society for Medical Oncology (ESMO) Standardized Operating Procedures. A structured literature review was conducted to inform structured clinical questions addressing resectability across different stage III NSCLC scenarios. Recommendations were formulated through iterative discussion and anonymous voting, with levels of evidence and grades of recommendation assigned according to ESMO methodology.
Results
Consensus was achieved for resectability in selected scenarios of single-station, non-bulky N2 disease, particularly in T1–2 tumors and T3 satellite lesions. Multi-station or bulky N2 disease was more frequently classified as potentially resectable in T1-2 tumors, with greater variability in expert agreement. For T4 disease, resectability depended on the pattern of invasion, nodal burden, and the feasibility of complete resection within a multimodality treatment strategy. Invasive restaging after induction therapy was strongly supported in selected scenarios. Across all recommendations, the panel emphasized the importance of multidisciplinary evaluation and individualized decision-making.
Conclusions
This consensus provides practical, context-specific recommendations on the resectability of stage III NSCLC in settings with limited diagnostic and therapeutic resources. By integrating available evidence with expert judgment, these recommendations aim to support multidisciplinary teams in selecting appropriate candidates for surgical management as part of multimodality therapy.
Introduction
Lung cancer is the leading cause of cancer death in the world. For the year 2022, there were approximately 1,817,469 deaths. 1 In Colombia, it ranked fifth in incidence (approximately 7,200 cases in 2022) and second in mortality, with about 6,100 deaths. 2 Non-small cell lung cancer (NSCLC) is the most common histologic type, representing 80% of lung cancer cases, and between 20% and 35% of individuals with NSCLC are diagnosed with stage III disease. 3 Furthermore, stage III patients constitute a heterogeneous group with wide variation in disease extent and lymph node involvement but a uniformly poor prognosis, with 5-year overall survival (OS) ranging from 10% to 40%. 4
The management of stage III NSCLC is also highly diverse and has evolved substantially over the last two decades. Current treatment strategies encompass a broad spectrum, ranging from adjuvant, neoadjuvant, and perioperative targeted and immune strategies in patients with resectable stage III NSCLC with or without oncogenic alterations; as well as novel combinations of chemoradiation and immunotherapy or targeted therapy in unresectable patients. 5 This diversity of therapeutic pathways underscores the complexity of stage III NSCLC, the critical importance of accurate staging and restaging, and the need to individualize treatment decisions based on tumor characteristics, nodal involvement, patient comorbidities, and resource availability.
Operability refers to an individual’s ability to tolerate surgical resection based on cardiopulmonary reserve, comorbidities, and functional status, whereas resectability refers to tumor-related anatomical and oncologic factors, including local extension, nodal involvement, and the feasibility of achieving a complete resection. 6 The role of surgery in the treatment of stage III NSCLC, particularly in patients with ipsilateral mediastinal lymph node involvement (N2), has been debated for decades. This controversy is primarily due to heterogeneous inclusion criteria in clinical trials and a lack of precise definitions for multi-station and bulky N2 disease, among other factors. Bulky lymph node disease has been variably defined by size (short-axis diameter >2.5 or 3 cm), evidence of invasion into surrounding structures (such as the trachea or great vessels), or both.4,7 The heterogeneity of N2 disease and the absence of a universal definition of resectability contribute to uncertainty regarding the optimal treatment approach. 7
General recommendations for managing stage III NSCLC include (a) multidisciplinary team (MDT) discussion with a thoracic surgeon who devotes a significant portion of practice to thoracic oncology, 8 which is not always available in some major cities in low- and middle-income countries (LMICs) 9 ; (b) multimodal strategies incorporating induction chemo-immunotherapy with immune checkpoint inhibitors (ICI),10-12 not yet approved in the neoadjuvant setting in Colombia; and (c) concomitant chemoradiotherapy for unresectable stage III NSCLC, which is often limited by fragmented care and scarce human resources. 13
In Colombia, access to specialized thoracic oncology care is heterogeneous and largely concentrated in major urban centers. The number of thoracic surgeons with dedicated oncologic training is limited, and the availability of advanced mediastinal staging techniques such as endobronchial ultrasound (EBUS) and endoscopic ultrasound (EUS) varies substantially across institutions. 9 While some high-volume referral centers have established multidisciplinary tumor boards, a significant proportion of hospitals managing lung cancer lack formal multidisciplinary committees, contributing to variability in staging and treatment decisions.
Given these constraints, cervical mediastinoscopy was considered the reference invasive mediastinal staging technique for the purposes of this consensus, as it remains widely available, does not require specialized endoscopic equipment, and provides reliable histopathologic confirmation of mediastinal lymph node involvement.
The objectives of this Consensus were to define resectability for people with operable stage III NSCLC who have undergone invasive mediastinal staging and to establish recommendations for restaging after induction therapy in a resource-limited setting.
Materials and Methods
The evidence-based recommendations presented here are intended to guide MDTs in the care of adults with operable stage III NSCLC who have undergone invasive mediastinal staging, as well as healthcare decision-makers and policymakers in LMICs. Critical clinical issues addressed include the resectability of N2 disease, the surgical management of tumor-compromised anatomical structures, and the indications for invasive restaging after induction therapy. Throughout this manuscript, we adhered to the American Society of Clinical Oncology (ASCO) Language of Respect guidelines, using patient-centered, stigma-free terminology that emphasizes the individual rather than the disease.
This expert consensus statement was developed by a multidisciplinary panel of Colombian experts following the European Society for Medical Oncology (ESMO) Standardized Operating Procedures. 14 The panelists were chosen for their academic profile and influence in national health institutions. The panel comprised 18 experts from the main four Colombian cities, representing eight thoracic surgeons (44%), four clinical oncologists (22%), two pulmonologists (11%), one nuclear medicine physician (6%), two radiation oncologists (11%), and one radiologist (6%). Preliminary questions were proposed, and unanimous agreement was reached on seven key clinical questions. A structured literature review covering January 2001 to July 2025 was conducted using predefined search strategies across MEDLINE, OVID, EBSCO, Cochrane, GIN, and L-OVE (Epistemonikos). The search prioritized meta-analyses, systematic reviews (SLRs), and clinical practice guidelines (CPGs). When these were unavailable, review articles, surveys, and large observational studies were considered. References of SLRs and CPGs were also screened. Articles not specific to stage III NSCLC or published in languages other than English or Spanish were excluded. The level of evidence follows the scheme adapted from the Infectious Diseases Society of America/United States Public Health Service Grading System, as used in ESMO Clinical Practice Guidelines. 15 A search strategy was designed using specific MeSH terms per question (supplementary material, Tables s1-s5) and PRISMA-style flow diagrams were constructed for each question to enhance transparency in study identification and selection (supplementary material, Figures s1-s5). This review was conducted to support the consensus process and was not intended as a standalone systematic review. Accordingly, the methodological approach was tailored to inform consensus development.
The consensus process was developed from September 2024 to August 2025. Panelists received summaries of the evidence for each question before the meetings. Two virtual meetings and one in-person meeting were held. The first meeting finalized the clinical questions, the second presented preliminary findings, and the third discussed and voted on recommendations. Voting options included resectable, borderline resectable and unresectable. Consensus was defined as ≥75% agreement for a category. If this was not reached, votes for resectable and borderline resectable were combined, and if ≥75%, the scenario was considered potentially resectable; otherwise, it was classified as no consensus. Voting was conducted using the Microsoft Forms® platform during the meetings. Bulky lymph nodes were defined as those with a diameter equal to or greater than 2.5 cm in short axis based on 2014 ESTS guidelines for preoperative mediastinal lymph node staging for non-small-cell lung cancer. 16 Invasion of lymph nodes was defined as those with extracapsular involvement on histology or infiltrating surrounding structures on imaging, and multi-station N2 disease was defined as the involvement of more than one N2 node station. Lymph node progression was defined according to RECIST version 1.1 criteria, as an increase of ≥20% and an absolute increase of at least 5 mm in the short-axis diameter of a target lymph node, taking as reference the smallest measurement recorded (nadir). Additionally, the appearance of new pathologically enlarged lymph nodes (short-axis ≥10 mm) was also considered progression. 17 All staging classifications used for voting and decision-making during the consensus process were based on the eighth edition of the American Joint Committee on Cancer (AJCC) TNM staging system.
Project chair role: Conception, design, and management of the study; acquisition, review, analysis, and interpretation of data; critical intellectual review and final approval of the version for publication.
Panel group role: Acquired, reviewed, and analyzed both included and excluded articles; interpreted the data; reviewed the intellectual content; drafted the initial manuscript; and approved the final submitted version.
Topics for the working groups: Resectability of stage III-N2 NSCLC; Resectability of anatomical structures compromised in T4 due to invasion with N0-2 disease; Invasive restaging in individuals with stage III-N2 NSCLC after induction therapy.
Statistical Analysis
Data presented in this article was obtained using descriptive statistics (primarily frequency distributions and proportions). Figures and tables were created using this information. No analytical statistical methods were used.
This research did not involve human participants or animal subjects; therefore, ethics approval was not required.
Results
Resectability of Stage III-N2 NSCLC
General results of the structured literature review are presented in supplementary material Figure 1 (Table s6) Table 1. Recommendations on Resectability of Stage III-N2 NSCLC According to the 2nd Spanish Lung Cancer Group (2nd GECP) Consensus,
18
Society of Thoracic Surgeons (STS) Expert Consensus,
19
The Consensual Definition of Stage III NSCLC Resectability Presented at the 2023 World Conference on Lung Cancer by the European Organization for Research and Treatment of Cancer (EORTC)*,23 and a Summary of the Structured Literature Review (This Also Includes the Above Consensuses) *The authors decided to include in this table the recommendations presented by Dingemans at the 2023 EORTC World Conference on Lung Cancer
20
instead of including the survey published by Houda et al.,
12
the results of the systematic review published by Xenophontos et al.
21
or the final consensus definition of stage III non-small-cell lung cancer technical resectability published by Dingemans in 2026.
22
This was, among other reasons, because the latter provided similar recommendations. ** except for T3 Pancoast tumors.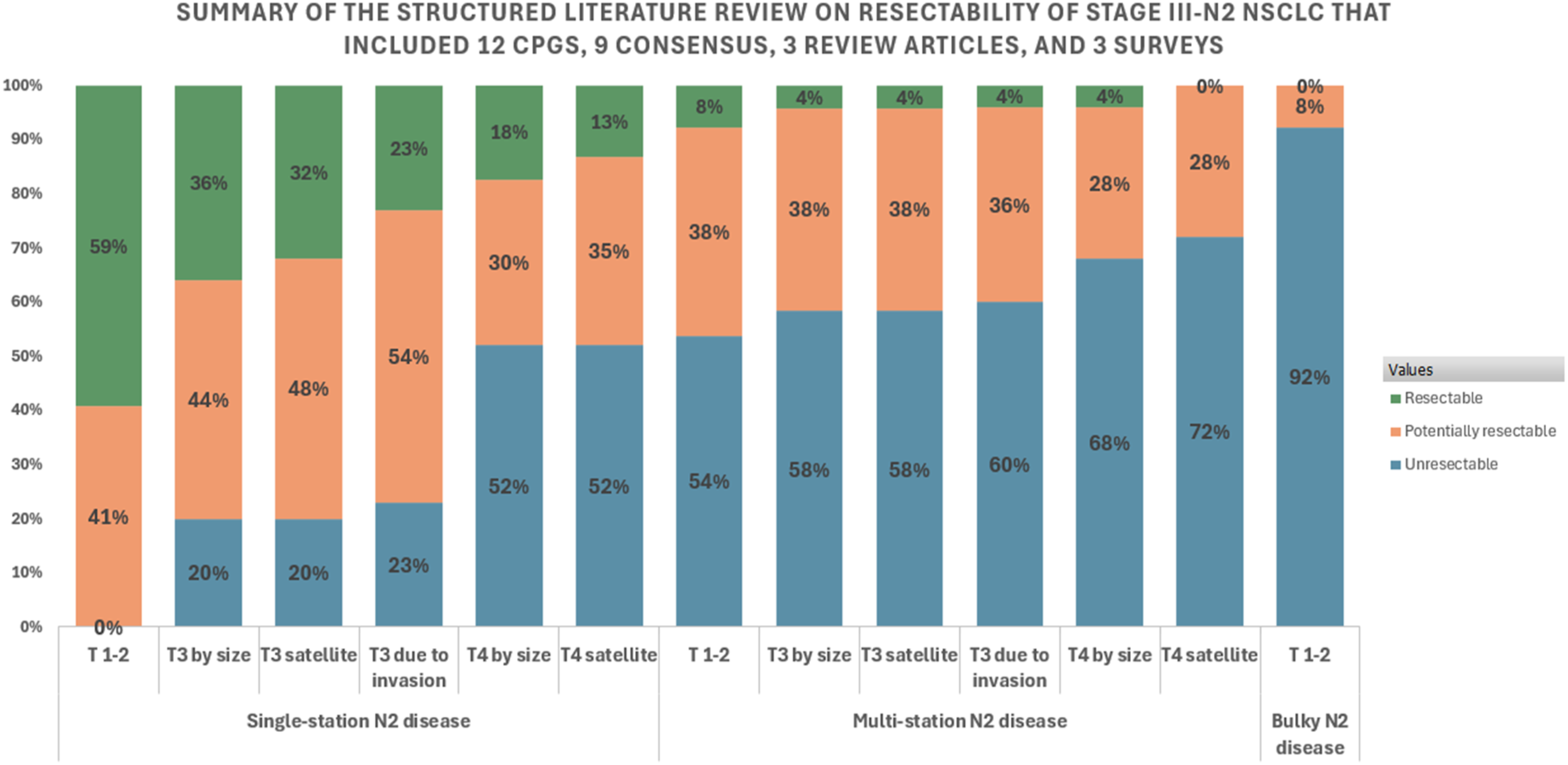


The 2nd GECP, STS, and EORTC Documents Were Selected for Separate Analysis Because They Represent Influential Multidisciplinary Perspectives From Europe and North America and Are Frequently Cited in Discussions on the Surgical Management of Stage III NSCLC. The 2nd GECP and STS Recommendations Were Developed Through Formal Consensus Processes, Whereas the EORTC Document was Based on a Structured Questionnaire Distributed Among Experts Rather Than a Consensus Meeting. Despite These Methodological Differences, the EORTC Document was Included due to its Relevance and Frequent Citation in Clinical Decision–Making.
Summary of Panel Recommendations on the Management of Stage III NSCLC
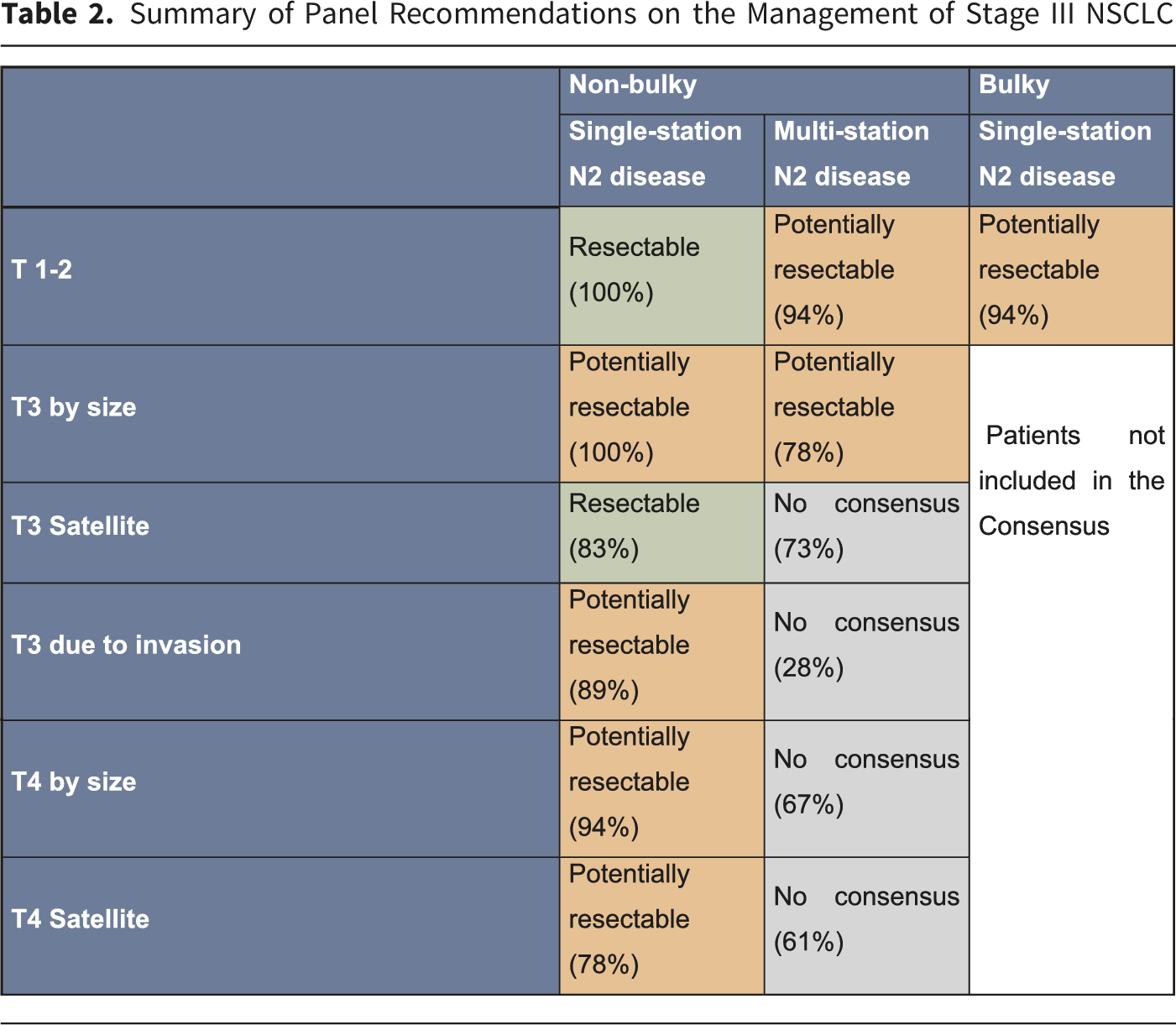

All NCCN member institutions recommend surgery for non-bulky, single-station N2 disease.26-29 Retrospective studies and meta-analyses have also reported favorable outcomes with surgical intervention in these patients.30,31 In contrast, the 2024 Society of Thoracic Surgeons (STS) consensus 19 considered individuals with T1–3 disease and single-station N2 involvement as resectable, except for T3 Pancoast tumors. Similarly, the 2nd Spanish Lung Cancer Group (2nd GECP) consensus, 18 the European Organization for Research and Treatment of Cancer (EORTC) consensus, 20 and the findings of the structured literature review10,12,18-20,23-26,32-49 categorized these cases as resectable or potentially resectable (see Table 1).
Although adjuvant chemotherapy after upfront surgical resection is an acceptable option in selected patients with stage IIIA NSCLC, the panel recommends induction systemic therapy (chemoimmunotherapy) followed by surgical resection as the preferred approach. This preference is based on several clinically relevant advantages: 1) higher antigen load and release from dying cells from tumors with integrity of the immune system and no immunosuppression associated with surgery; 2) neoadjuvant therapy improves mediastinal downstaging and increases the probability of achieving a complete (R0) resection; 3) it allows early treatment of micrometastatic disease; 4) pathologic response can be directly evaluated after induction, providing important prognostic information and potentially guiding decisions regarding adjuvant treatment; and 5) multiple phase III randomized trials have demonstrated superior outcomes with the neoadjuvant strategy. Specifically, the CheckMate 816 trial showed that neoadjuvant nivolumab plus chemotherapy significantly improved event-free survival and pathologic complete response rates compared with chemotherapy alone followed by surgery. 50 Similarly, the KEYNOTE-671 trial confirmed the benefit of perioperative pembrolizumab plus chemotherapy over chemotherapy alone. 51 These results are also reflected in current NCCN and ESMO guidelines,26,52 which endorse neoadjuvant chemoimmunotherapy as the preferred option for patients with resectable stage IIIA disease.
A consensus statement by Indian experts, one of the few studies from LMICs, noted that surgical resection may not be ideal for T4 N2 disease. They suggested that management of N2 disease should consider the extent of lymph node involvement (multi-station or multi-zone) and the volume of the affected lymph nodes. 39 Similarly, Stefani et al. 40 concluded T3–T4 and N2 disease may be considered potentially resectable if pneumonectomy is not required, multi-station N2 disease is absent, and the individual is medically fit for surgery.
The ninth edition of the TNM classification system for lung cancer distinguishes between single-station (N2a) and multi-station (N2b) disease, based on differences in long-term survival outcomes.53,54 Tanner et al. 55 reported on the treatment preferences of medical oncologists in the United States for patients with pN2 disease. They found that most providers (92%) preferred surgery as the primary modality for single-station N2 disease, while a smaller proportion (48%) favored surgery for multi-station N2 disease. Finally, the summary of the structured literature review10,12,18-20,23-26,32-49 did not reach a consensus regarding the management of patients with T1–3 non-bulky, non-invasive, multi-station N2 disease.
Resectability of Anatomical Structures Compromised in T4 Due to Invasion With N0-2 Disease
Summary of the Consensus Panel Agreement on the Evaluation of Resectability of Anatomical Structures Involved in T4 due to N0-2 Invasion
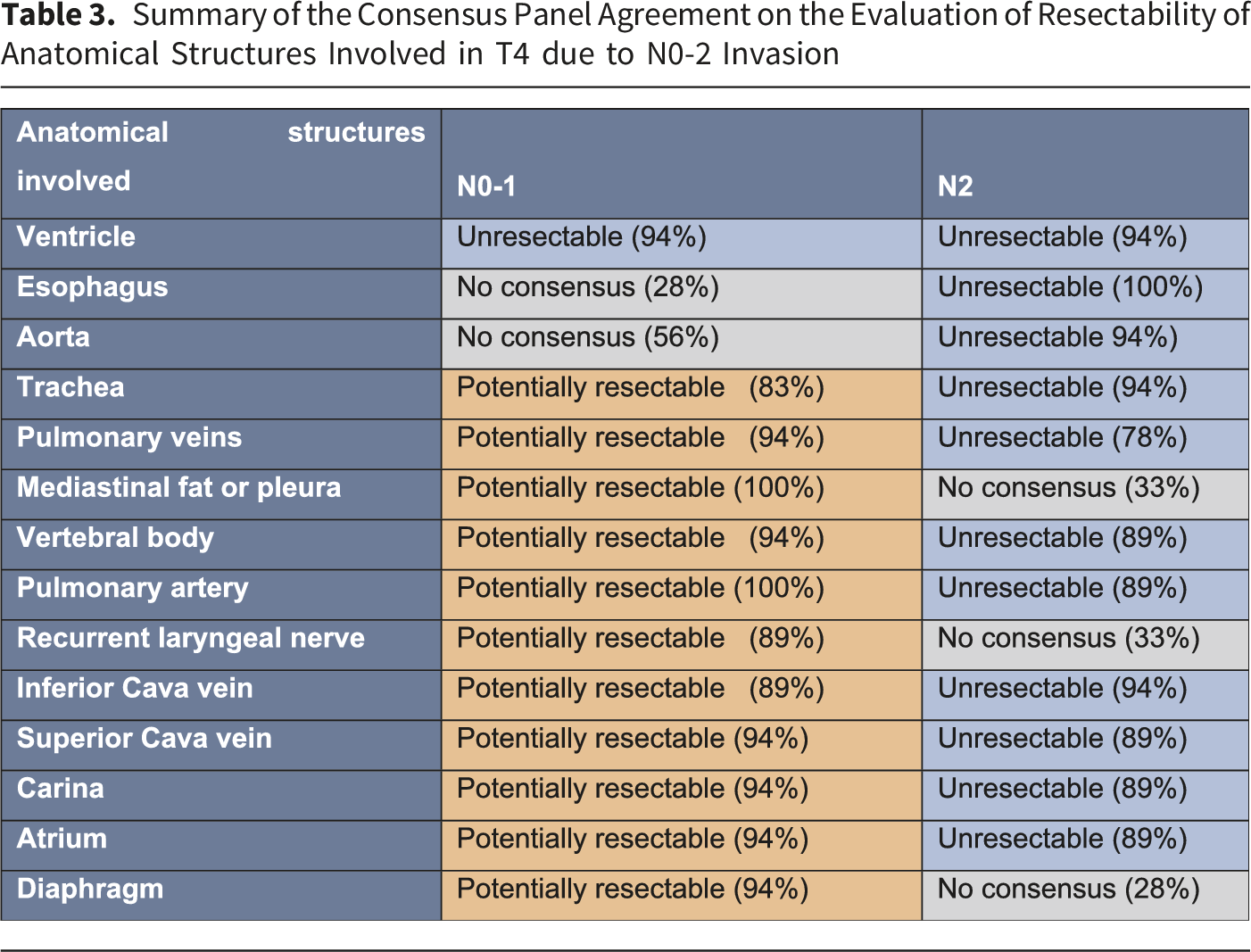

Extended resection for T4 tumors involving the left atrium remains controversial. A systematic review and meta-analysis by Hamouri 59 reported pooled 1-, 3-, and 5-year overall survival rates of 69.1% (95% CI: 61.7–76.0%), 21.5% (95% CI: 12.3–32.3%), and 19.9% (95% CI: 13.9–26.6%), respectively, with a median overall survival of 24 months (95% CI: 17.7–27). Most T4 tumors with central mediastinal invasion are not amenable to surgery. However, in experienced centers, resection of locally advanced tumors invading the spine,60,61 carina,62,63 heart, and great vessels 64 has been shown to be technically feasible with acceptable mid-term outcomes, typically in the absence of N2 or metastatic disease. 32 Surgical resection of the vena cava, vertebral body, diaphragm, mediastinum, atrium, and carina is technically possible and can yield reasonable survival outcomes, making surgery an option when an R0 resection is achievable.63,65 Conversely, resection of tumors invading the aorta or esophagus is associated with high morbidity and poor prognosis and should be approached with extreme caution or avoided.33,66
Advances in diagnostic imaging, surgical techniques, and perioperative care have made surgery possible for carefully selected patients with involvement of the carina, 62 superior vena cava, left atrium, intrapericardial pulmonary artery, aorta, esophagus, and vertebral bodies, achieving 5-year survival rates of up to 50% in some reports.67-69 According to the 2015 ESMO consensus, Eberhardt et al. 37 considered resection of the pulmonary artery, carina, spine, trachea, vena cava, and right atrium potentially feasible but associated with a high risk of incomplete resection. They classified invasion of the esophagus, heart, aorta, and pulmonary veins as unresectable. Tumors invading only the mediastinal fat or mediastinal pleura were considered potentially resectable. 70
Only a few case series have reported resection of T4 tumors involving the diaphragm, with 5-year survival rates ranging from 14% to 33%, depending on the depth of invasion.71-77 Pulmonary artery resection and reconstruction are technically feasible depending on the extent of disease,69,78-81 although specific survival rates for this subgroup have not been well described. Carinal and tracheal resections can also be performed in selected patients, with reported 5-year survival rates between 33% and 44%. 82 Finally, Yildizeli et al. 69 and Pitz et al. 78 described small series of patients who underwent resection of the muscular layer of the esophagus without mucosal invasion.
Invasive Restaging in Patients With Stage III-N2 NSCLC After Induction Therapy
Invasive restaging in patients with stage III-N2 NSCLC after induction therapy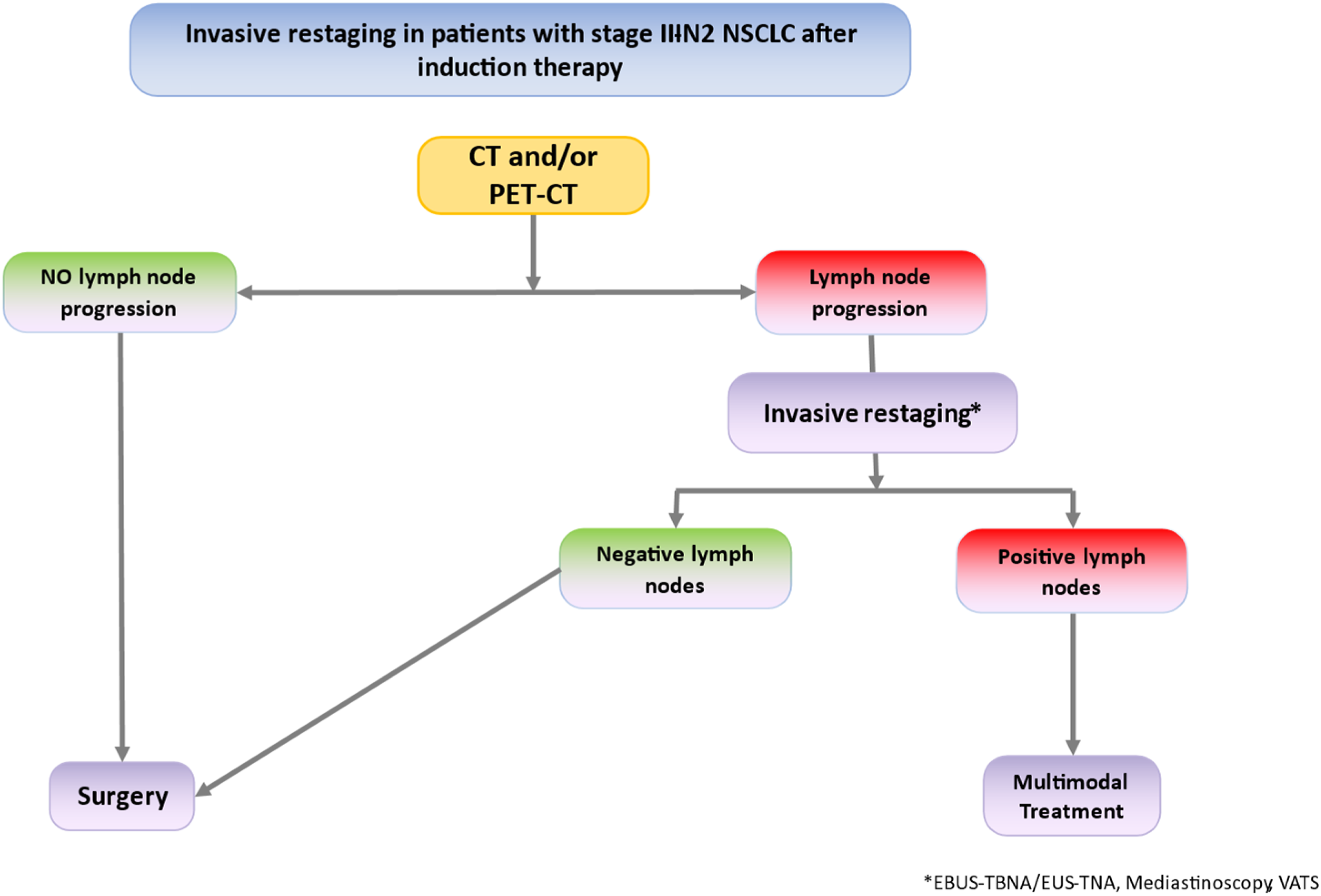
Barriers to the Implementation of Recommendations
Several barriers to the implementation of the recommendations generated by this consensus were identified, particularly in resource-limited settings. 1. Delays or denials in authorizations that restrict access to health services. 2. Shortage of human resources and financial constraints in cancer care. 3. Limited experience of healthcare professionals in managing NSCLC, particularly in low-volume centers. 4. Inefficiencies in the referral and counter-referral processes among related specialties. 5. Absence of multidisciplinary teams for NSCLC management. 6. Limited access to advanced technologies (e.g., ECMO) and to specialized services required for multidisciplinary care, such as cardiovascular and plastic surgery.
Limitations of this study include the size of the expert panel. While 18 specialists from the four main Colombian cities participated, inclusion of a larger panel of experts could have provided broader perspectives and enhanced the robustness of the recommendations. In addition, the proposed recommendations are specific to low- and middle-income countries, which may limit their generalizability to health-care systems with substantially different levels of resources or infrastructure.
Conclusions
Stage III NSCLC is a heterogeneous disease, which makes a multimodal treatment approach and multidisciplinary team discussion essential, particularly in the context of variable access to diagnostic and therapeutic resources. While optimal treatment strategies remain a topic of ongoing debate, the proposed consensus highlights scenarios in which surgical resection may be considered as part of multimodality therapy, following induction treatment, when complete resection is feasible and aligned with local capabilities, for patients with low-volume mediastinal lymph node involvement or with infiltration of structures that are potentially resectable without causing significant morbidity or mortality.
Defining resectability in stage III NSCLC is a complex and critical process that guides treatment decisions. In low- and middle-income countries, the implementation of resectability criteria must explicitly account for limitations in access to invasive mediastinal staging, specialized surgical expertise, and coordinated multidisciplinary care. Numerous barriers that may affect clinical outcomes have been identified and should be considered when applying the recommendations in real-world settings to ensure feasibility and consistency of care. Avoiding fragmentation in cancer care is key, and shared decision-making that incorporates patient preferences remains an essential component of implementation.
The recommendations from this Consensus aim to provide context-specific, practical guidance to support the implementation of surgical decision-making within multidisciplinary teams, improve patient outcomes, and enhance quality of life by promoting informed, resource-adapted clinical decisions in resource-limited settings.
Supplemental Material
Supplemental Material - Stage III Non-small Cell Lung Cancer Resectability in a Country With Limited Diagnostic and Therapeutic Resources: A Colombian Expert Consensus
Supplemental Material for Stage III Non-small Cell Lung Cancer Resectability in a Country With Limited Diagnostic and Therapeutic Resources: A Colombian Expert Consensus by Carlos A. Carvajal, Stella I. Martínez, Diego Pardo, Darwin Padilla, Mauricio Velásquez, Willfredy Castaño, Fernando Alvarado, Ricardo A. Zapata, Jairo A. Zuluaga, Ricardo E. Bruges, Luis L. Rojas, Clarena Zuluaga, Lucia C. Viola, Ana M. Callejas, Alejandro González, Eduardo Guerrero, Fernando Rodríguez, José R. Pieschacón, Wagner-Gutiérrez Nicolle, Natalia Sánchez, and Andrés F. Cardona in Cancer Control.
Footnotes
Acknowledgments
The authors are grateful for the administrative and logistical support provided by Evidentias SAS, ASOCOLTORAX and the unrestricted stipend from AstraZeneca for developing the Consensus.
ORCID iDs
Ethical Considerations
This research did not involve human participants or animal subjects; therefore, ethics approval and informed consent was not required.
Consent to Participate
This research did not involve human participants or animal subjects; therefore, ethics approval and informed consent was not required.
Author Contributions
CAC, JRP, and SM planned and coordinated the study. All authors reviewed included and excluded articles and performed data analysis. CAC, SM, DP, DP, MV, WC, FA, RAZ, JAZ, REB, LLR, CZ, LCV, AMC, AG, EG, FR, JRP, NW, NS and AFC wrote the initial draft of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The development of this Consensus was made possible thanks to the unrestricted support of AstraZeneca Colombia. The funder was not involved in the development of the questions, the elaboration of the recommendations, or the construction of the final document. Editorial control of the manuscript was solely the responsibility of the authors, who bear full responsibility for its analysis and content.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Carlos Carvajal has received speaker honoraria from AstraZeneca. Stella Martinez has received speaker honoraria from Johnson & Johnson (J&J) and Medtronic and has been sponsored by AstraZeneca, J&J, and Medtronic to attend conferences. Diego Pardo has received speaker honoraria from AstraZeneca and J&J and has been sponsored by Roche to attend conferences; he is also a shareholder and manager of Protorax de Colombia SAS, which conducts training activities and structures ECMO programs in various cities across Colombia. Darwin Padilla has received speaker honoraria and has been sponsored by AstraZeneca to attend conferences and by Medinistroas to participate in educational programs. Mauricio Velasquez has received speaker honoraria from MedXpert and has been sponsored by Avance Médico to attend conferences. Fernando Alvarado has received speaker honoraria from AstraZeneca and has been sponsored by AstraZeneca, J&J, and Med Expert to attend conferences. Ricardo Zapata has received honoraria for speaking engagements and has been sponsored to attend conferences by AstraZeneca, J&J, and MSD; also, he has a relative who has received honoraria as a speaker from Pfizer and Bayer. Jairo Zuluaga has been linked to Sinergia Salud and received honoraria as an advisor; he has also received speaker honoraria from Bristol-Myers Squibb(BMS) and has been sponsored to attend conferences hosted by BMS, Tecnofarma and J&J. Ricardo Bruges discloses financial research support from MSD; additionally, has been sponsored by Pfizer and GSK to attend conferences he has also received speaker honoraria from AstraZeneca, MSD and BMS. Leonardo Rojas discloses financial research support from MSD, Roche, AstraZeneca and Pfizer; additionally, he has been linked to and received honorarium as an advisor, participated in the speakers’ bureau, and provided expert testimony to Amarey, AstraZeneca, Amgen, MSD, Janssen, Addium and Ipsen; he has also been sponsored to attend conferences hosted by MSD, Pfizer, Janssen and Amgen. Lucia Viola has received speaker honoraria from AstraZeneca and MSD and has been sponsored by AstraZeneca, GlaxoSmithKline, and MSD to attend conferences. BI has sponsored Ana Callejas to attend conferences. Alejandro Gonzalez has received speaker honoraria from AstraZeneca and has been sponsored by Rocol and Janssen to attend conferences. Eduardo Guerrero has a relative who works with AstraZeneca. Jose Pieschacon has received consulting fees from AstraZeneca and has a relative who has received consulting fees from AstraZeneca. Andrés F. Cardona discloses financial research support from Merck Sharp & Dohme (MSD), Boehringer Ingelheim(BI), Roche, Bristol-Myers Squibb(BMS), and The Foundation for Clinical and Applied Cancer Research (FICMAC); additionally, he has been linked to and received honoraria as an advisor, participated in the speakers’ bureau, and provided expert testimony to MSD, BI, Roche, BMS, Pfizer, Novartis, Celldex Therapeutics, Foundation Medicine, Eli-Lilly, and The Foundation for Clinical and Applied Cancer Research – FICMAC. Willfredy Castaño, Clarena Zuluaga, and Fernando Rodriguez declare that they have no financial or non-financial conflicts of interest that could have influenced the work presented in this article.
Data Availability Statement
“All data generated or analyzed during this study are included in this published article (and its supplementary information files)”.
Artificial Intelligence (AI) Statement
AI tools were used only to improve language, grammar, or text structure.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.