
Abstract
Objective
To describe the survival outcomes of metastatic non-small cell lung cancer patients with limited access to immunotherapy and targeted therapy in a cancer reference center in Colombia.
Methods
A retrospective analysis of metastatic non-small cell lung cancer patients treated between 2013 and 2018 was performed, majority diagnosed with adenocarcinoma. It was carried out in a public cancer reference center that provides care to patients of low and middle socioeconomic status. Overall survival and progression-free survival were evaluated by Kaplan–Meier analysis and log-rank test. A Cox regression model was performed for univariate and multivariate analysis.
Results
209 patients were included with majority of adenocarcinoma (79.5%). First-line treatment was cytotoxic chemotherapy (50.2%), EGFR-targeted therapy (14.8%), chemoimmunotherapy (1.9%), and ALK-targeted therapy (1.4%). 31.6% received best supportive care. Median time of follow-up was 13 months, median overall survival was 11.2 months (95% CI, 7.9–14.4), 13 months for adenocarcinoma (95% CI, 8.1–17.9), and 2.5 months for squamous cell carcinoma (95% CI, 0.6–4.4) (P < .001). Median progression-free survival was 9.3 months (95% CI, 7.9–10.7) without differences according to the type of first-line therapy. Median time-to-treatment was 55 days and only 54% of patients with a tested actionable mutation in EGFR received an EGFR-targeted therapy as the first-line treatment. Multivariate analysis showed that squamous cell carcinoma histology and receiving best supportive care were independent factors for worse overall survival ((HR:1.8, 95% CI, 1.076–3.082, P=.026) and (HR:14.6, 95% CI, 8.921–24.049, P < .001), respectively). Meanwhile, squamous cell carcinoma histology was an independent factor for worse progression-free survival (HR:3.4, 95% CI, 1.540-7.464, P=.002).
Conclusions
Despite advances in precision medicine, during the study period, cytotoxic chemotherapy was the most used treatment in our patients. Furthermore, about a third of them received best supportive care. The use of targeted therapies has been restricted by access to molecular diagnosis and remained low until 2018. Access to immunotherapy should be prioritized.
Keywords
Introduction
Lung cancer is the leading cause of cancer mortality in the world with 1,796,144 deaths reported in 2020. 1 Approximately 350 persons per day died from lung cancer in the United States in 2022 2 and is the leading cause of disability-adjusted life years (DALYs) with 18.3% of total cancer related DALYs. 3 Advances in translational oncology have made non-small cell lung cancer (NSCLC) a disease whose adverse outcomes have been favorably modified by incorporating molecular diagnostic methods and personalized treatment, especially in the advanced and metastatic setting. This was recently demonstrated in the United States, where a reduction in mortality related to NSCLC has been documented since 2013, when targeted therapies were approved for actionable mutations such as epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK). 4
Low- and middle-income countries (LMICs) have limited access to diagnostic tests, biomarkers, and treatments like immunotherapy and targeted therapy. This makes the implementation of personalized therapy a big challenge.5,6 We have scarce data about the impact of the development of personalized therapies on the survival of our patients in a real-world setting.7,8 This study aims to analyze the survival outcomes of a cohort of metastatic NSCLC patients with limited access to immunotherapy and target therapy treated between 2013 and 2018 in a cancer reference center in Bogota, Colombia.
Materials and Methods
Retrospective cohort study of patients with a biopsy-proven diagnosis of stage IV NSCLC at the National Cancer Institute (INC) in Bogota, Colombia, between 2013 and 2018. Patients under 18 years of age, without histological confirmation of NSCLC, previous systemic treatment for another cancer, lack of follow-up (defined as a patient who was only evaluated on a single opportunity for thoracic surgery or clinical oncology), or with other synchronous tumors except for non-melanoma skin cancer managed with local therapies were excluded from the study. Patients who had a metastatic recurrence after treatment for early stage lung cancer were not included.
Study Setting
INC is a public institution located in Bogota, which is the capital city of Colombia. This institution is one of the main national reference centers for cancer management in Colombia and has affiliations with 34 universities across the country. In 2021, 5562 new cases of cancer were treated at the INC, of which 107 (1.9%) were lung cancer, and of these, 35.5% came from areas of the country other than Bogotá. 9 Colombian General Social Security Health System includes two regimens: contributory regime covers salaried and independent workers that contribute with a percentage of their salary and subsidized regime covers unemployed and population that do not contribute. Additionally, a regime of exceptions that includes, among other populations, indigenous people also exists. 10
Statistical Analysis
Study data were collected from clinical records and managed using RedCap 7.1.2. Continuous variables were summarized using central tendency measures (mean or median) accompanied by their corresponding measures of dispersion: standard deviation (SD) or interquartile ranges (IQR), depending on the characteristics of the distribution of these variables; the distribution was tested using Kolmogorov–Smirnov test. Categorical variables were presented in absolute values and percentages. Data were analyzed using Statistical Package for the Social Sciences (SPSS) (IBM Corp. Released 2010. IBM SPSS Statistics for Windows, Version 19.0. Armonk, NY: IBM Corp.) with the support of the INC statistical team. Overall survival (OS) was defined as the time between the date of the biopsy report of NSCLC and the date of death recorded in the clinical records or censored on the last day of follow-up. Progression-free survival (PFS) was calculated as the time between the date of initiation of first-line systemic therapy with palliative intention until the date of progression, death, or last follow-up if disease progression was not documented. Additionally, time-to-treatment was defined as the time between the date of the biopsy report confirming metastatic NSCLC and the date of the initiation of first-line systemic therapy. OS and PFS were evaluated by Kaplan–Meier analysis and log-rank test to assess differences between survival curves. A Cox regression model was performed for univariate and multivariate analysis to identify independent survival factors. Stepwise forward based on clinical criteria was the methodology for selecting variables for multivariate models. P-values <.05 were considered statistically significant. The reporting of this study conforms to STROBE guidelines. 11
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Research and Ethics Committee of the National Cancer Institute No CEI-00554-19, October 10, 2019. Data collection was supervised by an institutional clinical monitoring group.
Results
Demographics and clinical characteristics of all included patients and according to histology.

IQR: interquartilic range, ADC: adenocarcinoma SCC: squamous cell carcinoma, ECOG: Eastern Cooperative Oncology Group.
aIncluding: 6 patients with NSCLC Not otherwise specified (NOS), 5 with large cell and one with adenosquamous carcinoma.
In this series, 71.8% (n=150) of the patients were tested for targetable mutations (EGFR or ALK). The majority of patients (70.8% n=148) were tested for EFGR mutations, 38.5% were positive. Of these, 25 (43.8%) samples carried Exon 19 deletion. At the time our patients were treated, determination of EGFR status was done in a reference molecular laboratory mostly using RT-PCR COBAS Z480. Additionally, of the patients tested for EGFR, 63.5% were women, 92.6% had adenocarcinoma, and 57.4% were non-smokers. ALK status was tested in our pathology lab in 52 (24.9%) patients with genomic rearrangements found in 25% of those tested using Ventana ALK (D5F3). 91.2% of the EGFR-positive patients, were not tested for ALK rearrangements, due to the sequential testing used during 2013 and 2018; meanwhile, almost 50% of the EGFR-negative patients were tested for ALK rearrangements. Programmed death-ligand1 (PD-L1) was performed in 11% of the cases using Ventana PDL1 (SP263). The most used first-line treatment was cytotoxic chemotherapy (50.2%), followed by EGFR-targeted therapy (14.8%), chemoimmunotherapy (1.9%), and ALK-targeted therapy (1.4%). 66 patients (31.6%) did not receive any cancer-directed therapy and were managed with best supportive care (BSC). Of these, 57% were men, median age was 70 years (IQR=61–74), 62.1% had ECOG ≥2 and 75.8% were classified as M1b or M1c clinical stage. Finally, 54.8% of the patients with SCC histology received BSC, Table 1.
The median time of follow-up was 13 months. The median overall survival for the total population was 11.2 months (95% CI, 7.9–14.4). 34% of patients were alive at two years of follow-up, Figure 1A. For the ADC group, the median OS was 13 months (95% CI, 8.1–17.9) and 38% of patients were alive at two years. For the SCC group, the median OS was 2.5 months (95% CI, .6–4.4) (P < .001, univariate comparison between ADC and SCC) and only 23% of patients were alive at one year, Figure 1B. Women had a median OS of 14.7 (95% CI, 10.1–19.3) months; meanwhile, men had a median OS of 5.7 months (95% CI, .8–10.6) (P = .014, univariate comparison between women and men), Figure 1C. Kaplan–Meier curves (A) overall survival (OS) of all included patients. (B) OS of patients with adenocarcinoma (ADC) and squamous cell carcinoma (SCC). (C) OS by gender. Comparisons with Log-rank test.
The median OS for the subgroup of patients that received any type of treatment was 26.9 months (95% CI, 14.9–38.8) vs 1.4 months for BSC (95% CI, 1.1–1.8) (P < .001).
Among the 143 patients who received any kind of treatment, the median time-to-treatment was 55 days (IQR 30 to 105). Although median OS of patients with chemotherapy and EGFR-targeted therapy was 20.8 (95% CI, 8.5–33.0) and 27.2 (95% CI, 14.5–39.9) months respectively, this difference was not statistically significant (P = .270), Figure 1D. The median OS of patients with targetable mutations and without targetable mutations was 16.9 (95% CI: 3.276–30.524) and 16.8 moths (95% CI: 7.238–26.428), respectively.
The median PFS for the total population was 9.3 months (95% CI 7.9– 10.7), Figure 2A. Median PFS was 8.7 months (95% CI 6.7–10.7) in the chemotherapy subgroup and 9.3 months (95% CI 5.4–13.2) in the EGFR-targeted therapy subgroup, this difference was not statistically significant (P = .545), Figure 2(b). Kaplan–Meier curves, progression-free survival (PFS) of all included patients.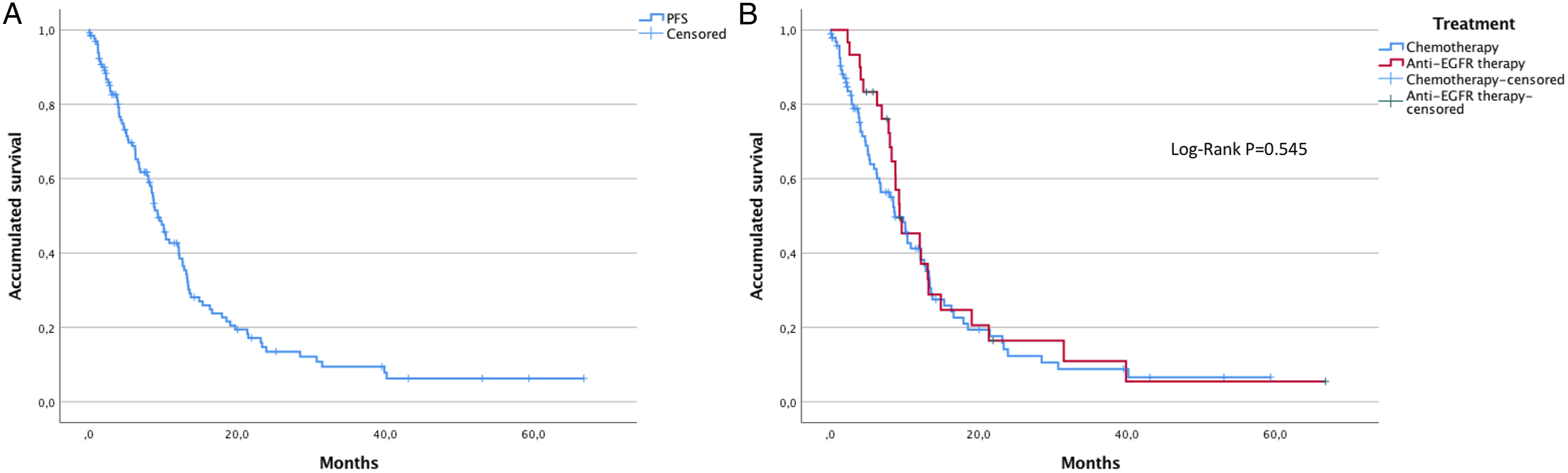
A first-generation tyrosine kinase inhibitor (TKI) was used in 80% of patients who received first-line EGFR-targeted therapy (erlotinib 45%, gefitinib 35%), followed by the second-generation TKI afatinib in 20%. No patient received osimertinib as first-line treatment. The use of EGFR-targeted therapy in the second-line treatment was 33% (n = 19), including four patients treated with osimertinib. Only 54% of patients with a tested actionable mutation in EGFR received an EGFR-targeted therapy as the first-line treatment.
Univariate and multivariate analysis for overall survival (OS).

HR: hazard ratio, ECOG: Eastern Cooperative Oncology Group, ADC: adenocarcinoma, SCC: squamous cell carcinoma, BSC: best supportive care.
Univariate and multivariate analysis for progression-free survival (PFS).

HR: hazard ratio, ECOG: Eastern Cooperative Oncology Group, ADC: adenocarcinoma, SCC: squamous cell carcinoma.
Discussion
Almost 80% of the patients included in this series were covered in the subsidized regime of the Colombian General Social Security Health System. Even though, all regimens have access to the same procedures and treatments, social determinants still make differences between them, underlying the special social vulnerability of our patients.
The treatment approach for patients with metastatic NSCLC is changing year by year with the development of personalized therapies according to the presence of driver mutations.12,13 The frequent use of molecular diagnostic techniques has taught us that the term NSCLC brings together many entities with different clinical and biological behavior. These advances are experienced in a different way in LMICs, where other ethnic, socioeconomic, environmental, and geographic factors make real-life studies a valuable tool for evaluating the impact that these new approaches have on the real care of our patients.14,15 We found that between 2013 and 2018 cytotoxic chemotherapy (50.2%) was the most used treatment in our patients and a striking third of our patients did not receive any systemic treatment and were treated with BSC. This was slightly higher than the percentage described in a series of 9656 patients with metastatic NSCLC from the Flatiron Health database, where 26.7% of patients received no treatment
16
and similar to that described in a cohort of Latin American patients with Metastatic NSCLC
17
; however, with our data we want to highlight the importance of prioritizing interventions that resolve access barriers and address the disparities that explain the differences between our results and other cohorts from developed countries. Additionally, King et al described in a UK series that patients that received BSC were older (average age 79 years), frail (70% clinical frailty score ≥6), functionally limited (80% World Health Organization Performance Status: 3–4), and 68% had stage IV lung cancer.
18
In our series, that included only stage IV NSCLC patients, the median age of the patients that received BSC was 70 years (IQR=61-74) and 62.1% had ECOG ≥2. However, the interpretation of these data needs careful attention to histology, since BSC was the only treatment received by 54.8% of patients with SCC compared to 27.7% of patients with ADC. Differences according to histology were also found in overall survival, with a statistically significant difference in median OS of 13 months in ADC vs 2.5 months in SCC (P < .001). In Taiwan, Wang et al reported that stage IV ADC patients had a significantly better 5-year OS rate than SCC (6% vs 2%) (P < .0001).
19
Although, the functional status of the patients with SCC included in our study was similar than that found in patients with ADC (see Table 1), some factors of SCC patients could explain this gap: they were mainly men (74.2%) and had history of smoking (80.6%). Furthermore, the fact that actionable mutations are not an important therapeutic target in SCC makes the incorporation of immunotherapy into treatment the most impactful strategy, even if it is used after progression to first-line therapy.20,21 PD-1 inhibitors were introduced as second-line treatment for lung cancer in 2016 and determination of PDL-1 expression was not mandatory. Government approval of immune checkpoint inhibitors (ICI) as first-line monotherapy in patients with PD-L1 expression greater than 50% occurred in June 2017. Also, its use in combination with chemotherapy regardless of the determination of PDL-1 expression in non-SCC patients occurred in August 2018 and SCC patients in March 2019 Figure 3. Evaluating these dates, it makes sense that none of the patients with SCC in our cohort received immunotherapy in the first line of treatment and that only one of them underwent determination of PD-L1 expression in tumor tissue. This was probably not the reason for the poor outcomes of SCC patients, but it highlights the importance of facilitating access to immunotherapy for newly diagnosed metastatic SCC patients. Waterhouse et al
22
described, in a series that included 4271 patients that received immunotherapy plus chemotherapy for stage III-IV NSCLC, a median OS of 10.6 months (95% CI: 9.3–11.8) in patients with SCC and 12.0 months (95% CI: 11.3–12.8) in those with non-squamous NSCLC. Approval timeline of EGFR-targeted therapy and immunotherapy for metastatic NSCLC in Colombia. [Source: Instituto Nacional de vigilancia de medicamentos y alimentos (INVIMA)].
In our series, the median overall survival for the total population was 11.2 months; meanwhile, patients that received some type of first-line treatment had a striking median OS of 26.9 months. Cramer‐van der Welle et al, in their series that included 1950 patients with stage IV NSCLC diagnosed between 2015 and 2018, showed that 47% of patients did not receive active treatment and the median OS of those patients who did receive chemotherapy, immunotherapy, or TKI was 7.5 months, 15.6 months, or 15.5 months, respectively. 23 Additionally, in Switzerland, in a study that included 118 patients with stage IV NSCLC treated in the same period and including those who received BSC, the median OS was 8.6 (95% CI, 6.6 to 10.5) months. 24 Therefore, including or not including BSC may explain the difference of our results with other real-life studies and should be interpreted with caution. Moreover, a retrospective study in Brazil, between 2006 and 2014, showed an OS of 8.1 months (95% CI: 7.455–8.841) and also described that women have a 16% lower risk of mortality from lung cancer compared to men, which was explained by a wide variety of factors such as younger age at diagnosis, higher probability of ADC, lower frequency of smoking, higher actionable genomic alterations, and better response to different treatment modalities. 25 Although the survival we found was higher, the gender differences were similar. Additionally, Gender differences in lung cancer treatment and outcomes were also found in other settings, such as academic community practice institutions in the US, where female gender was associated with higher rates of surgical management and lower risk of death. 26
We found similar OS for patients with and without targetable mutations, and there was not a statistically significant difference between the patients with chemotherapy and EGFR-targeted therapy. These findings are not consistent with the information described in the world literature, but they could be influenced to the fact that only 71.8% of the patients were tested for targetable mutations and because only 54% of patients with a tested actionable mutation in EGFR received an EGFR-targeted therapy as the first-line treatment.
Another important factor is time-to-treatment; the hypothesis that prolonged time-to-treatment negatively affects survival in patients with NSCLC has been consistently described in early stages, specifically for surgical patients; however, it doesn’t apply for metastatic settings.27,28 This phenomenon called the “waiting time paradox” could be explained by the fact that early treated patients tend to have more severe symptoms.29,30 Despite this, a median time to treatment of 55 days is beyond the expected time in a referral cancer center and indirectly shows us the limitations that exist in LMICs for timely treatment once a diagnosis has been made. Malalasekera et al, 31 in a 2018 scoping review, described time to treatment (treatment interval) ranging from 6 to 80 days in 52 studies, with a median of 27 days, missing most guideline timelines, such as Australian guidelines that recommend 14 days 32 but below the Danish guidelines recommendation of 42 days. 33 Some of the barriers that can lead to a prolonged time-to-treatment are delays in therapy authorizations by insurers, long access times to oncology consultations, delays in the results of molecular tests, and lack of infrastructure of health service providers. Additionally, the concept of fragmentation of care recently described in Colombian patients with breast cancer, in which diagnosis is made in one institution and treatment in another, associated with long reference times, is another issue that explains the delay in starting treatment. 34
On the other hand, in ADC patients a median PFS of 9.3 months reached with EGFR-targeted therapy (mainly first-generation TKI) is close to the PFS published in EURTAC and iTARGET studies.35,36 The lack of statistical difference in OS or PFS between EGFR-targeted therapy and cytotoxic chemotherapy could be related to the same factors described above (lack of universally EGFR testing and use of chemotherapy as first-line treatment without performing an actionable molecular analysis). Limitations for access to an adequate molecular diagnosis is well known in Latin America (LATAM); a recent survey conducted by International Association for the Study of Lung Cancer (IASLC) shows that 74% of oncologists in LATAM answered that less than 50% of patients with NSCLC are molecular tested in their countries. 37 In a recent publication of a cohort of patients with EGFR mutations in LATAM, the frequency of molecular testing varied widely by country and insurance coverage: reported testing rates were 78.8%, 64.6%, 75% and 27.6% in Argentina, Colombia, Chile and Uruguay, respectively. Furthermore, Colombia was the country with the longest turnaround time for testing with 20.4 days compared to a reported turnaround time of 9.9, 10.0, and 13.5 days in Argentina, Chile, and Uruguay, respectively. 17 We need to face different challenges to improve molecular diagnosis. 38 First, very few laboratories have the technology and knowledge required to perform these tests. Second, the incorporation of these molecular tests in health insurance has been low and progressive, and finally, the unavailability of many targeted therapies to other driver mutations or to overcome resistant mutations makes the routine use of genomic profiling a big issue, as was exposed according to Colombian context previously.39,40
We also observed a large difference in the frequency of testing of the different biomarkers. Although this could be explained by the approval time of targeted therapies (Figure 3); other factors associated were the availability of material for molecular studies, the number of laboratories within the country, and the Health System’s coverage of these tests.
Prior to 2021, EGFR and ALK testing was primarily industry-sponsored, and initially patients had to meet certain conditions, such as being female, having adenocarcinoma, and no tobacco exposure to be tested. In addition, patients were tested sequentially, so EGFR-positive patients were generally not tested for ALK rearrangements.
Our region also needs to strengthen networks for clinical research in lung cancer to deal with the increase of recent cancer burden patterns and trends as well as our unmet medical needs. 41 Cooperative groups have shown important advances for molecular characterization of our own population and paved the way for addressing special regional issues such as ancestries and its implications in the prevalence of certain targetable mutations.42,43
Our daily practice has been changing in recent years. At present, we are running in our institution four test in all metastatic NSCLC patients according to government therapy approvals: EGFR (PCR Cobas), ALK (Ventana D5F3), ROS-1 (FISH), and PDL1 (SP263). Also, we perform pan-TRK immunohistochemistry in patients EGFR, ALK, and ROS-1 negative results because we recently have Larotrectinib approved as an agnostic therapy.
The approval of first-line immunotherapy for the population without mutations allowed a better characterization of the molecular profile in lung cancer. This began to happen in 2017, with new laboratories in the country, greater access to these resources for the population and a progressive implementation of strategies to reduce the barriers of insurers in the delivery of medicines that we believe have changed the landscape of treatment in our population.
Nowadays, we do not perform next generation sequencing (NGS) to all metastatic NSCLC patients at diagnosis, but we really think NGS implementation probably would lead to a faster improvement of patient’s oncologic outcomes. Resources needed to overcome the barriers for implementing NGS in a timely fashion are strengthening and developing new molecular diagnosis labs, enhancing human and technologic resources, updating national clinical guidelines, investing in data generation and implementing molecular tumor boards. 10
We are aware of the small number of patients included and that 2018 (end year of period reviewed) is far from the current year (2023), so the findings reported in this study may be outdated; but, to date, it is the largest cohort of patients with stage IV NSCLC in the country with the largest median follow-up.
Limitations of our study include its retrospective design and single center experience. This may not reflect the practice of LATAM particularly due to the high degree of heterogeneity that exists between and within our countries. Despite this, unlike other real-life studies, we not only show the molecular diagnosis and treatment in a cohort of patients but related them with clinical outcomes which is the main goal of treatment. There was not description of the guideline-concordant treatment used in the study population and there is a lack of information about the type of mutations and techniques used for molecular tests and the appearance of resistance mutations. Although the INC is a cancer reference center, many molecular tests were initially performed in other reference laboratories and were not registered in the institutional medical record. Other limitations are that a power/sample size analysis was not performed and that the definition of OS and PFS used different starting points, making their interpretation confusing.
Conclusions
In our series, cytotoxic chemotherapy continues to be the most widely used treatment for the management of metastatic NSCLC. The histology of squamous cell carcinoma has been associated with a poor prognosis and it is imperative to add immunotherapy to treatment in these patients. In addition, some barriers were found in this series: a large proportion of patients that received better supportive care, prolonged time-to-treatment, limited access to molecular testing and use of targeted therapies; issues that have been reported in several LMICs and that we have been trying to overcome.
Footnotes
Author Contributions
Conceptualization, Diego-Felipe Ballén and Carlos Carvajal.; Methodology, Diego-Felipe Ballén, Carlos Carvajal-Fierro and Ricardo Brugés-Maya; Software, Carlos Carvajal-Fierro; Validation, Diego-Felipe Ballén, Martha-Liliana Alarcón and Camilo Vallejo.; Formal Analysis, Carlos Carvajal-Fierro; Investigation, Diego-Felipe Ballén, Carlos Carvajal-Fierro Ricardo Brugés-Maya, Martha-Liliana Alarcón and Camilo Vallejo; Resources, Diego-Felipe Ballén, Carlos Carvajal-Fierro and Ricardo Brugés-Maya; Data Curation, Diego-Felipe Ballén; Writing – Original Draft Preparation, Diego-Felipe Ballén and Carlos Carvajal-Fierro; Writing – Review & Editing, Rafael Beltrán, Ricardo Brugés-Maya; Visualization, Diego-Felipe Ballén; Supervision, Ricardo Brugés-Maya; Project Administration, Diego-Felipe Ballén.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Research and Ethics Committee of the National Cancer Institute in Bogota, Colombia. No CEI-00554-19, October 10, 2019.
Informed Consent
Patient consent was waived in accordance with the national legislation and the institutional requirements.