
Abstract
Objective:
To evaluated the oncologic outcomes associated with platinum-based adjuvant chemotherapy following concurrent chemoradiotherapy (CCRT) in the management of patients with locally advanced cervical cancer (LACC).
Methods:
A total of 695 patients with FIGO stage IB2, IIA2, IIB-IVA LACC treated at 6 medical facilities were enrolled and divided into 2 groups: 478 were assigned to CCRT alone (CCRT group) and 217 to adjuvant chemotherapy after CCRT (CCRT-ACT group). The treatment outcomes were retrospectively compared and reported after the propensity score matching (PSM) analysis.
Results:
With a median follow-up of 56.4 months, no statistically significant differences were found in overall survival (OS), disease-free survival (DFS), progression-free survival (PFS) and distance metastasis-free survival (DMFS) between 2 groups. In CCRT-ACT group, patients with lymph nodes involvement or squamous cell carcinoma (SCC) had significantly longer DMFS, but no significant benefit in survival outcomes were observed with more than 2 cycles of adjuvant chemotherapy. Moreover, patients with a high level of CA125 (>20.5U/mL) or SCC-Ag (>22.8μg/L) had a relatively better DFS or PFS, and grade 3-4 acute hematological toxicity, late urinary and lower gastrointestinal complications and diarrhea symptom were more frequent in CCRT-ACT group.
Conclusions:
Adjuvant chemotherapy after CCRT has a potential role in further improving disease control for LACC patients with lymph nodal-metastasis or SCC with a high level of CA125 or SCC-Ag. Due to increased treatment-related complications and diarrhea symptom affecting the quality of life, post-CCRT adjuvant chemotherapy with excessive cycles was not be considered as the most appropriate choice in general.
Keywords
Introduction
Cervical cancer is a major health problem among a global female population. According to the World Health Organization, cervical cancer is the fourth most common cancer and the fourth leading cause of cancer-related mortality in women worldwide. Approximately 570,000 new patients were estimated to be diagnosed in 2018 representing 6.6% of all female cancers, with 311,000 deaths projected; more than 85% of these deaths occurring in low- and middle-income countries. 1 In developing countries like China, patients usually present with locally advanced stages. 2 Currently, concurrent chemoradiotherapy (CCRT) is recommended as the standard treatment strategy for locally advanced cervical cancer (LACC) due to its effectiveness in improving local control and reducing distant metastasis based on the encouraging results from several randomized trials. 3 Although the use of combining chemotherapy with radiation has a therapeutic advantage over radiotherapy alone, about 30%-40% of patients with LACC failed to achieve a complete response to CCRT, and even experienced tumor relapse or distant metastasis after treatment. 4 While several studies pertaining to adjuvant chemotherapy after CCRT in cases of LACC are available, 5 -7 survival benefit from the addition of adjuvant chemotherapy to CCRT in patients with LACC remains unclear. This retrospective clinical study was performed to report outcomes following platinum-based adjuvant chemotherapy after CCRT for LACC at multiple institutions.
Materials and Methods
Patients
We retrospectively analyzed 695 patients with 2009 International Federation of Gynecology and Obstetrics (FIGO) stage IB2, IIA2, IIB-IVA cervical cancer who were treated with definitive radiotherapy between 2007 and 2016 at 1 of 6 hospitals. Patient charts were reviewed for clinicopathological information from existing medical report and follow-up data.
None of the patients underwent prior treatment. Pre-treatment diagnostic evaluation consisted of a gynecological examination and a panel of laboratory and radiological tests (including computed tomographic/magnetic resonance imaging scan of the abdomen and pelvis, or positron emission tomography/computed tomography whenever possible). Eligibility criteria included: age < 75 years, Karnofsky performance status (KPS) scale ≥ 60, normal cardiovascular function, normal blood cell counts, and normal serum levels of blood urea nitrogen, creatinine, and bilirubin. The therapeutic regimen among these patients was CCRT alone (CCRT group), and CCRT plus adjuvant chemotherapy (CCRT-ACT group).
Treatment Schedule
All patients underwent definitive radiotherapy with a combination of pelvic external beam radiotherapy (EBRT) and high-dose-rate (HDR) intracavitary brachytherapy (ICBT). The pelvic EBRT at a total dose of 45 Gy-50.4 Gy was delivered using 3-dimensional conformal radiotherapy (3D CRT) technique or intensity-modulated radiotherapy (IMRT) technique. Four to 6 fractions of HDR ICBT (once a week) with a prescribed dose of 7-5 Gy were given at high-risk clinical target volume (CTVhr). The details of the radiotherapy were previously described. 8
The concurrent chemotherapy was given weekly with intravenous cisplatin 30-40 mg/m2 for 5 weeks during EBRT in all inclusion patients. In addition, a small number of patients having either pelvic/para-aortic lymph nodes involvement or local residual tumor were treated with the additional cycles of adjuvant chemotherapy after CCRT, depending on patient tolerance and response. The platinum-based adjuvant chemotherapy was administered every 3 weeks following CCRT. A combination regimen was paclitaxel (175 mg/m2 on day 1) combined with either cisplatin (50 mg/m2 on day 1) or carboplatin (AUC 5 on day 1).
Follow-Up Study
Before each cycle of treatment, a physical examination and routine hematologic analysis were conducted. After completing the whole protocol treatment, the disease status and the treatment-related toxic effects were evaluated by the routine work-up at the discretion of the attending physician every 3 months in the first year of follow-up, every 4-5 months in the second year, and every 6 months thereafter. In patients in whom regular follow-up information was not available, an effort was made to contact them by telephone or correspondence to obtain this information. Local recurrence and distant metastasis were calculated according to the follow-up examination results by imaging diagnosis and pathological biopsy. Late treatment-related complications were assessed according to the Radiation Therapy Oncology Group (RTOG) criteria. Quality of life (QoL) in patients was surveyed using the European Organization for Research and Treatment of Cancer quality of life questionnaire version 3 (EORTC QLQ-C30 V3.0).
Statistical Analysis
In this retrospective study, the propensity score matching (PSM) was used to remove the effects of confounding due to measured baseline covariates when using observational data to estimate the effects of treatment. The matching covariates included Karnofsky performance status, lymph nodes status, histological subtypes, and FIGO stage were selected based on prior literature reports and known clinically prognostic factors. Categorical variables are presented as frequencies and percentages, and continuous variables are expressed as the median with range. The frequency distributions of clinicopathological parameters were compared between groups using Chi-square or Fisher’s exact tests. The probabilities of overall survival (OS), disease-free survival (DFS), progression-free survival (PFS) and distance metastasis-free survival (DMFS) were estimated by the Kaplan-Meier method and compared using log-rank test. Univariate and multivariate analyses were performed using the Cox proportional hazards regression model. The statistically significant variables in univariate analyses were included in the stepwise regression for multivariate analyses. Probit models were used for testing relationships for prognostic factors and the probability of survival. All statistical analyses were performed using SPSS for Windows version 18.0 (SPSS Inc., Chicago, IL, USA). All reported P-values were 2-sided, and P-values < 0.05 was considered to be statistically significant.
Ethical Statement
This retrospective study was registered with the Chinese Clinical Trial Registry (ChiCTR-PRC-16008822). All procedures performed in studies involving human participants were in accordance with the ethical standards of the independent Ethical Committee/Institutional Review Board of Jilin University (20160621) and conducted in accordance with the Declaration of Helsinki. Informed consent was waived due to the retrospective format of this study.
Results
Patient Characteristics
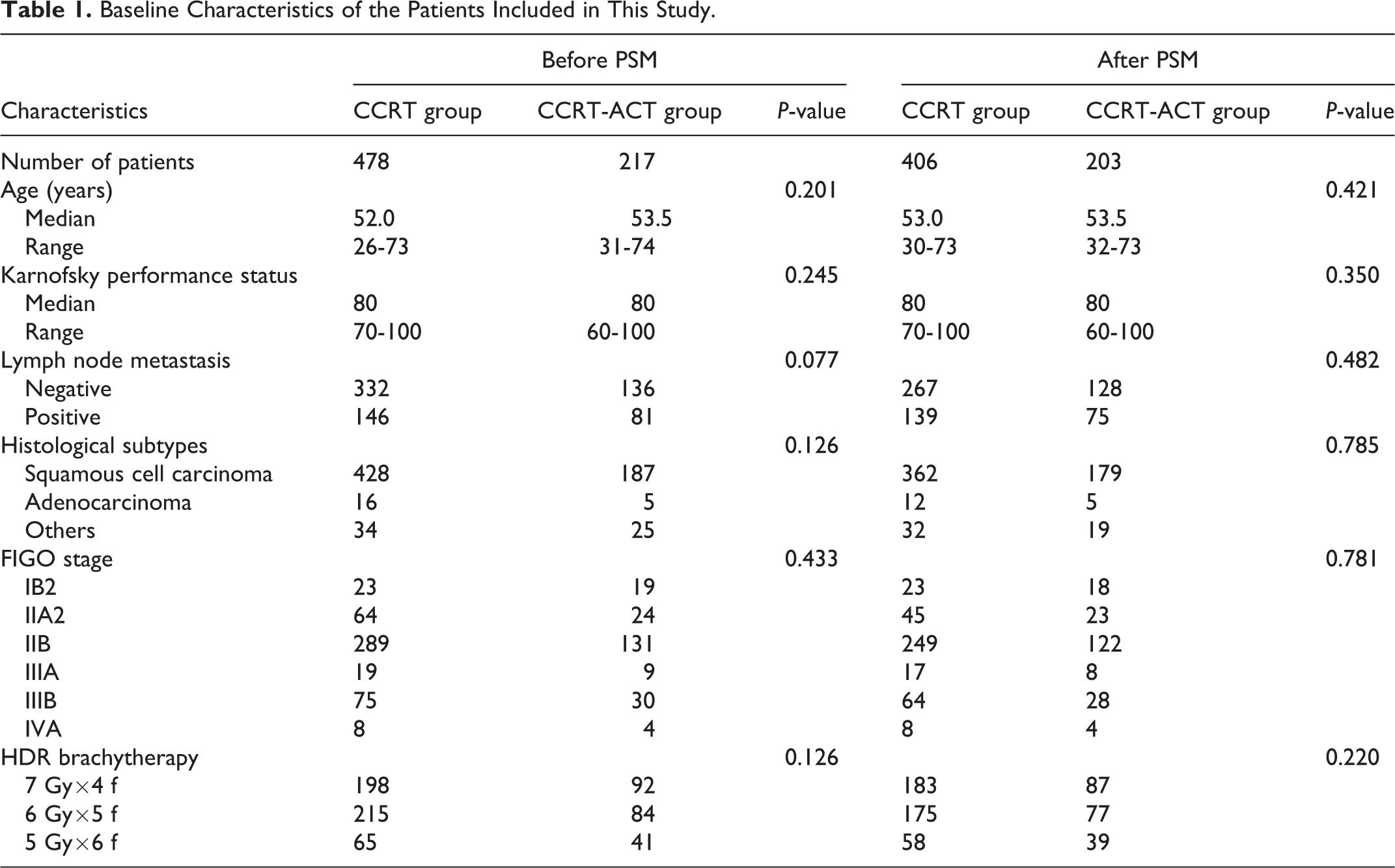
The baseline demographic and clinicopathological characteristics of these patients before and after PSM are shown in Table 1. Of the total patients before matching, the mean age at diagnosis was 52.0 years old (range 26-74), and 615 (88.5%) were histologically diagnosed with squamous cell carcinoma (SCC). Forty-two patients (6.1%) were staged as IB2, 88 patients (12.7%) as IIA2, 420 patients (60.4%) as IIB, 28 patients (4.0%) as IIIA, 105 patients (15.1%) as IIIB, and 12 patients (1.7%) as IVA. After completion of the treatment, CCRT group consisted of 478 patients who were treated with CCRT alone, whereas CCRT-ACT group was composed of 217 patients who received CCRT plus adjuvant chemotherapy. PSM analysis with 2: 1 matching was performed, 406 patients in CCRT group and 203 patients in CCRT-ACT group were included in the final analysis. The baseline characteristics of the 2 groups were well balanced and superimposable in all selected clinical characteristics.
Baseline Characteristics of the Patients Included in This Study.
Treatment Outcome and Survival Analysis
The median follow-up duration was 56.4 months (range 3.6-132.2). In the propensity matched cohort, Kaplan-Meier estimates comparing therapeutic regimens in total patients are illustrated in Figure 1. In patients of CCRT and CCRT-ACT groups, the 1/3/5-year OS rate was 95.8%/84.7%/80.0% and 99.0%/87.2%/80.8%; the 1/3/5-year DFS rate was 88.9%/79.8%/75.4% and 93.1%/80.3%/74.9%; the 1/3/5-year PFS rate was 88.7%/79.6%/74.1% and 92.6%/79.8%/73.4%; and the 1/3/5-year DMFS rate was 91.4%/87.7%/86.9% and 95.1%/88.2%/87.2%. The 2 groups of patients did not significantly differ in OS, DFS, PFS and DMFS (log-rank P = 0.438, 0.499, 0.438 and 0.231, respectively). For those patients with later stages, including tumor extending to the pelvic wall (IIIB) and invading adjacent organs (IVA), no statistically significant difference in outcomes was found between CCRT and CCRT-ACT groups (5-year OS: 73.6% and 87.5%, P = 0.117; DFS: 72.2% and 84.4%, P = 0.173; PFS: 62.5% and 71.9%, P = 0.267; DMFS: 91.7% and 90.6%, P = 0.118, respectively) (Supplementary Figure 1). As demonstrated in Supplementary Figure 2, adjuvant chemotherapy after CCRT played a role in DMFS compared with CCRT alone when evaluating patient outcomes for positive pelvic or para-aortic lymph nodes (5-year DMFS: 93.3% and 82.0%, P = 0.035).
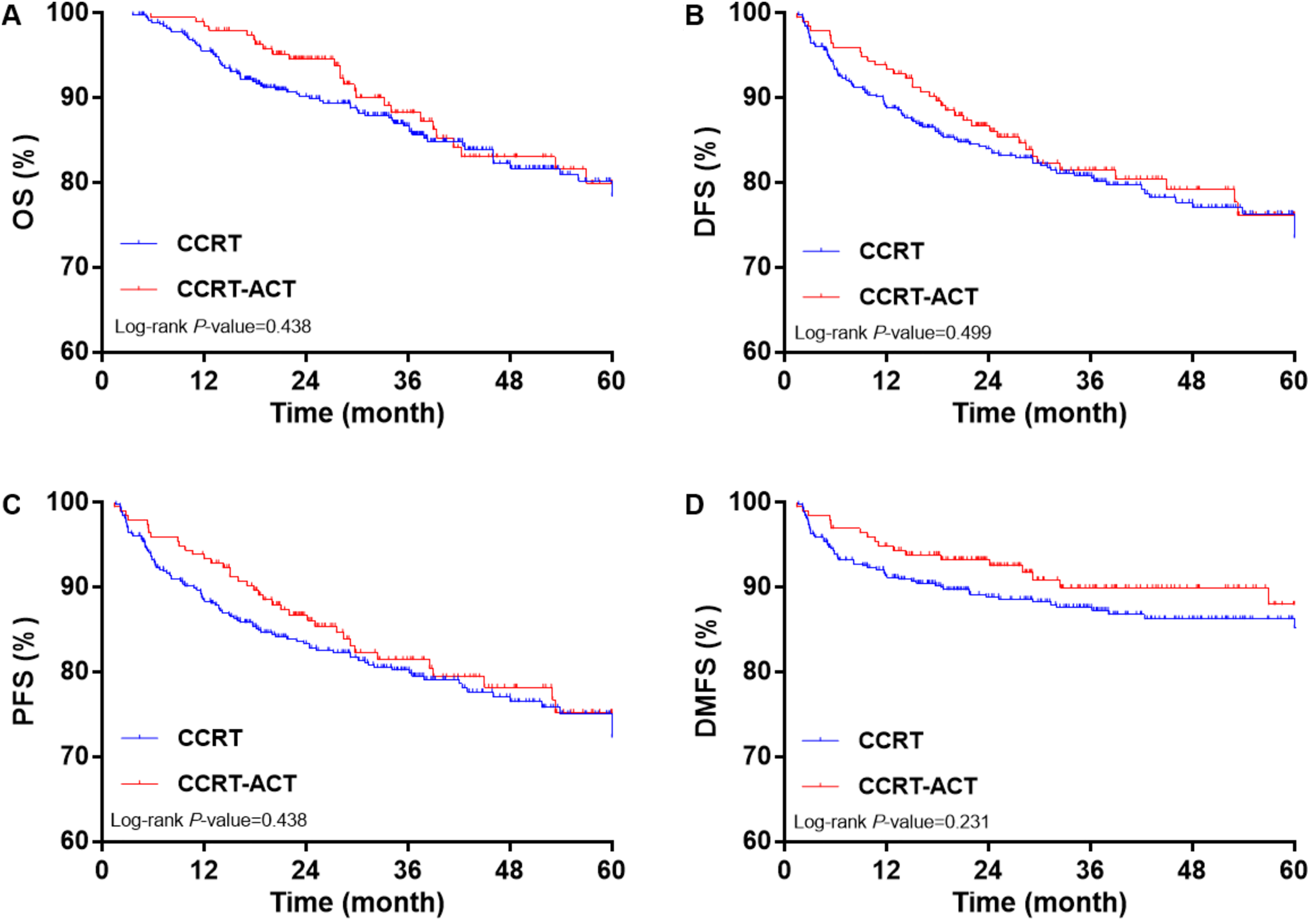
Kaplan-Meier survival estimates of (A) OS, (B) DFS, (C) PFS and (D) DMFS for LACC patients after PSM.
We also carried out a subgroup analysis and investigated the survival in LACC patients only with SCC. The CCRT-ACT group had a similar 1/3/5-year OS rate (98.9%/88.9%/83.2% for CCRT-ACT, and 97.2%/87.6%/82.3% for CCRT, P = 0.443), DFS rate (93.3%/81.6%/76.5% for CCRT-ACT, and 91.7%/82.0%/77.1% for CCRT, P = 0.867) and PFS rate (92.7%/81.0%/75.4% for CCRT-ACT, and 91.7%/82.0%/76.0% for CCRT, P = 0.727) compared to CCRT group. As illustrated in Figure 2, SCC patients treated with adjuvant chemotherapy after CCRT displayed significant improvements in 1/3/5-year DMFS rate (95.0%/92.2%/91.1% for CCRT-ACT, and 90.9%/87.8%/87.0% for CCRT, P = 0.032). Notably, it is the subgroup of patients with non-SCC did not differ significantly in OS, DFS, PFS and DMFS between CCRT and CCRT-ACT groups (log-rank P = 0.134, 0.103, 0.078 and 0.074 for OS, DFS, PFS and DMFS, respectively) (Supplementary Figure 3).

Kaplan-Meier survival estimates of (A) OS, (B) DFS, (C) PFS and (D) DMFS for LACC patients with SCC after PSM.
A total of 179 SCC patients were treated with post-CCRT adjuvant chemotherapy in which less than or equal to 2 cycles adjuvant chemotherapy regimen was used for 95 patients and more than 2 cycles for 84 patients. For the SCC patients receiving adjuvant chemotherapy after CCRT, no significant differences were observed in the respective 5-year OS, DFS, PFS or DMFS rate between patients treated within 2 cycles and more than 2 cycles of adjuvant chemotherapy (OS rate: P = 0.181; DFS rate: P = 0.428; PFS rate: P = 0.604; DMFS rate: P = 0.497). The survival curves for the 2 subgroups are shown in Figure 3.

Kaplan-Meier survival estimates of (A) OS, (B) DFS, (C) PFS and (D) DMFS for SCC patients in CCRT-ACT group with ≤2 vs >2 cycles adjuvant chemotherapy after PSM.
Prognostic Factors Analysis
To identify independent prognostic factors, univariate and multivariate analyses using the Cox proportional hazards regression model were performed. As shown in Table 2, the univariate analysis demonstrated that baseline hemoglobin level, tumor markers (SCC antigen, SCC-Ag; cancer antigen 125, CA125) and histological subtypes were significantly associated with 5-year OS, DFS and PFS (P = 0.025, 0.017, 0.002 and 0.000 for OS; 0.040, 0.011, 0.020 and 0.009 for DFS; 0.007, 0.018, 0.004 and 0.002 for PFS, respectively). Furthermore, univariate analysis of age, histological subtypes, FIGO stage and lymph node metastasis with 5-year DMFS showed a trend toward significance (P = 0.029, 0.002, 0.004 and 0.032, respectively). In the multivariate analysis, it was found that SCC-Ag was an independent predictor of 5-year OS, DFS and PFS (P = 0.020, 1.08 [1.02, 1.14 for OS; P = 0.018, 1.04 [1.01, 1.08] for DFS; P = 0.035, 1.04 [1.00, 1.08] for PFS, respectively), and CA125 was another independent predictor of 5-year OS and PFS (P = 0.003, 1.01 [1.01, 1.02] for OS; P = 0.001, 1.01 [1.00, 1.01] for PFS, respectively). Age and histological subtypes remained as independent prognostic factors for 5-year DMFS (P = 0.011, 1.03 [1.00, 1.04] with age; P = 0.001, 4.05 [1.80, 8.21] with adenocarcinoma; P = 0.000, 6.88 [3.22, 14.26] with other types of carcinoma, respectively) (Table 3).
Univariate Analyses of Factors Affecting 5-Year OS, DFS, PFS and DMFS After PSM.

BMI: body mass index; NEUT: neutrophilic granulocyte; LYM: lymphocyte; HGB: hemoglobin; PLT: blood platelet; ALT: alanine aminotransferase; AST: aspartate aminotransferase; GGT: glutamyltranspeptidase; ALP: alkaline phosphatase; GLU: glucose; BUN: blood urea nitrogen; CRE: creatinine; TP: treponema pallidum; ALB: albumin; SCC-Ag: squamous cell carcinoma antigen; CA125: cancer antigen 125.
Multivariate Analyses for Outcomes According to Prognostic Factors After PSM.

HR: hazards ratio; CI: confidence interval.
Probit Regression Models With a Probability of Survival Related to Tumor Markers
Probit regression was used to model the probability of survival results as a function of the tumor marker level. We found that in both CCRT-ACT and CCRT groups, the probability of survival declined with an increase in the levels of CA125 or SCC-Ag (Table 4). Patients with CA125 above the cut-off value (19.8U/mL for DFS; 20.5U/mL for PFS) receiving adjuvant chemotherapy after CCRT differed significantly in DFS and PFS than CCRT alone. Also, the CCRT-ACT group had significantly higher DFS than the CCRT group with the lowest possible cut-off value of SCC-Ag (22.8μg/L) (Figure 4).
Probit Regression Analysis for Relationship Between Tumor Markers and Survival After PSM.


Probit regression models of data sets with probability of survival (y axis) related to tumor marker levels (x axis). A, Probability of DFS with CA125. B, Probability of PFS with CA125. (C) Probability of DFS with SCC-Ag.
Treatment-Related Complications
The acute and late adverse events for treatment were summarized in Table 5. The most common acute toxicity found in both groups was hematologic toxicity. Twenty-five patients (6.2%) had grade 3-4 acute hematological toxicity in CCRT group, while 27 (13.3%) in CCRT-ACT group (P = 0.003). The other acute toxicities about vagina mucosa, upper/lower gastrointestinal and urinary tract had no significant difference between the 2 groups.
Treatment-Related Toxicities of CCRT and CCRT-ACT Groups After PSM.

# Continuity correction chi-square test.
With regard to late complications of treatment, the most common adverse events were upper/lower gastrointestinal and urinary toxicities. In CCRT group, grade 2 or below, and 3-4 upper gastrointestinal complications occurred in 404 (99.5%) and 2 (0.5%) patients, and 201 (99.0%) and 2 (1.0%) patients in CCRT-ACT group, respectively (P = 0.859). However, grade 3-4 lower gastrointestinal complications were more common in patients from CCRT-ACT group than in those of CCRT group (16 [7.9%] vs 15 [3.7%], P = 0.027). Concerning urinary toxicities, grade 3-4 was observed in 7 patients from CCRT-ACT group, which was more than CCRT group (7 [3.4%] vs 1 [0.2%], P = 0.004).
QoL Status of Patients
EORTC QLQ-C30 V3.0 was used to evaluate the QoL status of patients. The scores range of each subscale or item ranged from 0-100. The higher score indicates better functioning or QoL, as well as a higher rate of symptoms or problems. The comparisons suggested that the majority of QoL aspects were similar in the 2 groups at long-term follow-up. However, the symptom scale in diarrhea was significantly different, and patients who underwent adjuvant chemotherapy after CCRT more frequently suffered from diarrhea than those treated with CCRT only (P = 0.000) (Table 6).
Mean Scores of Subscale/Item of EORTC QLQ-C30 V3.0 in CCRT and CCRT-ACT Groups After PSM.

Discussion
Cervical cancer is one of the most common malignancies and recognized as a major public health problem in China with an increasing incidence and younger age at diagnosis. 9 The incidence of cervical cancer in Chinese married women is highly ranked among female malignant tumors. It is also the common cause of death among women in China presenting in a locally advanced stage. As CCRT is the main aspect of curative treatment of LACC, much of the treatment consists of providing adequate facilities for good-quality EBRT, ICBT, and delivery of adequate concurrent chemotherapy. 10
Adjuvant chemotherapy is the absolute gold standard in the therapy of many tumor types. In contrast, the role of adjuvant chemotherapy for cervical cancer is not fully understood. Furthermore, detailed information on the effects of adjuvant chemotherapy, when added to CCRT, is still not available. 11 In China, adjuvant chemotherapy is generally performed in some patients with cervical cancer at a locally advanced stage, who are at high risk for recurrence and able to tolerate further treatment after CCRT. 12 Yet, the clinical feasibility of treatment with CCRT, followed by adjuvant chemotherapy in a larger group of LACC patients still remains unclear.
In this retrospective multicenter study, data from patients with LACC in stage IB2, IIA2, IIB-IVA, of which mainly IIA2, IIB and IIIB, were collected to make a clinical efficacy comparison between CCRT-ACT and CCRT group. In opposition to the benefits of the additional use of adjuvant chemotherapy after CCRT that has been reported by numerous previous studies, 13 -15 we did not find significant differences related to longer OS, DFS, PFS and DMFS between CCRT-ACT and CCRT group after a median follow-up of 56.4 months. When patients were divided into subgroups based upon whether or not with more advanced stages, OS, DFS, PFS of patients with stage IIIB and IVA in CCRT-ACT group was higher than that of those in CCRT group. However, the difference was not statistically significant. Kim YB et al. 16 assessed the cervical cancer patients with stage IB and IIB who underwent CCRT followed by adjuvant chemotherapy in another retrospective analysis. According to the results of 5-year OS and DFS rates for patients in CCRT and CCRT-ACT groups (85% vs 80%, and 83% vs 78%, respectively), the data failed to show the discernable therapeutic advantage of adjuvant chemotherapy administered after CCRT. This was partly supported by findings from the randomized controlled trial of Tangjitgamol S et al. 17 which found no significant benefit in response rate and survival of adjuvant chemotherapy with paclitaxel plus carboplatin after CCRT for LACC of stage IIB-IVA compared to standard treatment of CCRT alone. Nonetheless, it may be of some therapeutic advantage over CCRT alone in cervical cancer patients with positive pelvic or para-aortic lymph nodes who received post-CCRT adjuvant chemotherapy in the present study. Abe A et al. 18 and Yuan Y et al. 19 also reported encouraging results of adjuvant chemotherapy after completion of CCRT in an attempt to improve outcomes in the management of lymph nodal-metastatic cervical cancer. Future clinical trials are required for confirmation of the clinical efficacy of adjuvant chemotherapy, especially for the patients with poor prognostic factors.
Due to tumor heterogeneity, it is unlikely that the additional use of adjuvant chemotherapy after CCRT could show some improvement in clinical outcomes in patients with cervical cancer with different histological subtypes. 20 Zhang MQ et al. 21 evaluated their experience with chemoradiotherapy for LACC patients only with SCC. They treated patients (stage IIB-IIIB) with CCRT followed by consolidation chemotherapy with paclitaxel and nedaplatin and demonstrated that this treatment regimen was well tolerated and effective. Although the analogical finding in our study was that the addition of adjuvant chemotherapy had no substantial impact on survival in LACC patients receiving CCRT, our protocols employing CCRT followed by adjuvant chemotherapy resulted in longer DMFS in LACC patients with SCC. Adjuvant chemotherapy that follows CCRT can potentially improve distant control of LACC with SCC, as argued by Jelavić TB et al. 22 The improvement in distance metastasis control seems to be caused by a higher response rate to post-CCRT adjuvant chemotherapy in SCC patients. It is worth noting that in our study, only 46.9% of LACC patients with SCC received more than 2 cycles of adjuvant chemotherapy, and 53.1% received within 2 cycles, which was probably due to increased treatment-related morbidity or other causes. Furthermore, our data also showed that adjuvant chemotherapy with more than 2 cycles did not result in significantly improved survival compared to that within 2 cycles of adjuvant chemotherapy. Some clinical studies have confirmed that the addition of adjuvant chemotherapy after CCRT does leads to an increase in the risks of treatment-related adverse effects, requiring coordinated supportive care so as to avoid treatment delays and hospitalizations during the treatment course, as well as relatively poor compliance of patients. 16 These observations related to the untoward effects of more cycles of adjuvant chemotherapy seems to preclude definitive conclusions regarding the true superiority of this modality. Although we failed to observe the potential beneficial effects in the small number of patients with non-SCC receiving adjuvant chemotherapy after CCRT, it is worthwhile to further expand the number of samples to study the treatment effect of patients who are more prone to suffer disease failure. 23
Chemotherapy comprising a platinum agent has been reported to be highly effective in advanced and recurrent cervical cancer. 24,25 Studies have shown that chemotherapy improves survival and decreases local and distant recurrence, yet at the expense of a varying degree of toxicity and morbidity. 26 In the present study, platinum-based chemotherapy after CCRT was administered as adjuvant chemotherapy and comprised paclitaxel combined with either cisplatin or carboplatin. Adjuvant chemotherapy following CCRT increased the severity of the grade 3 or higher acute hematological toxicity and late urinary and lower gastrointestinal complications. In contrast, the frequency of other toxicities did not differ between CCRT-ACT and CCRT group. Some researchers have focused on the radiation toxicity after completing treatment with chemoradiotherapy. 5,16,17 It was reported that hematological adverse event was the more prominent in acute toxicities during the treatment of CCRT followed by adjuvant chemotherapy compared with CCRT alone, however, the incidence of late radiation bladder and gastrointestinal complications did not significantly differ between CCRT-ACT and CCRT groups. The results might be related to differences in sensitivity to chemoradiotherapy in patients from different research groups.
Cervical cancer has long-term effects on health-related QoL of cancer survivors after treatment. 27 Few research studies have focused on the QoL of LACC survivors. 28 In this study, no differences in the global health QoL and functional scale were found between 2 groups; nevertheless, bowel morbidity was prevalent after treatment with definitive chemoradiotherapy in the symptom scale analysis. The LACC patients in CCRT-ACT groups more frequently experienced severe diarrhea symptoms than those who underwent CCRT only. Many patients treated for cervical cancer have long-term complaints regarding bowel function. 29 Digestive system interventions should be valued in improving QoL of cervical cancer chemoradiotherapy patients. 30
The tumor markers, including SCC-Ag and CA125, were identified as significant risk factors for survival (OS, DFS and PFS) in the multivariate analysis. These observations as well as the roles these risk factors have in predicting prognoses in LACC patients, have been reported by several previous studies. 31,32 Likewise, older patients and non-SCC patients were at higher risk for distant metastasis. Atahan IL et al. 33 evaluated possible prognostic factors in patients with LACC (88% with IIB-IIIB), reporting adenocarcinoma as one of the independent predictors for DMFS. In another study by Yokoi E et al. 34 compared the survival outcomes in patients with SCC and adenocarcinoma/adenosquamous carcinoma among patients with LACC. Patients with non-SCC histology experienced significantly worse survival outcomes than those with SCC. Additionally, the reason for the worse outcome in elderly patients may be somewhat aggressive tumor factors. 35
Based on analyses of tumor markers in patients treated with chemoradiotherapy, adjuvant chemotherapy after CCRT might presented a probability of greater DFS and PFS in patients with high level of CA125 (the lowest possible cut-off values were 19.8 and 20.5U/mL, respectively). The level of SCC-Ag was also significantly linked to DFS; more specifically, a greater DFS in CCRT-ACT patients was probably amplified a profit from high SCC-Ag level (above 22.8μg/L) compared with patients receiving CCRT alone. Our study supported the hypothesis that patients who could have been screened for high levels of tumor markers, especially CA125 and SCC-Ag, might have a greater survival benefit from adjuvant chemotherapy after CCRT.
In conclusion, this study was undertaken in a developing country where the majority of the global burden of cervical cancer resides. Our data failed to show the discernable therapeutic advantage of adjuvant chemotherapy given after CCRT in OS, DFS, PFS and DMFS for patients with LACC. However, adjuvant chemotherapy after CCRT had a more favorable distant metastasis control in managing LACC patients, particularly with pelvic/para-aortic lymph nodes involvement or SCC, than those treated with CCRT alone. It is a remarkable fact that the post-CCRT adjuvant chemotherapy with excessive cycle numbers should not be considered as the more appropriate choice, in order to avoid the probability of unnecessary cumulative toxicity, especially severe acute hematological toxicity, late urinary and lower gastrointestinal complications. Diarrhea might be one of the main symptoms affecting the QoL in LACC patients undergoing adjuvant chemotherapy after CCRT. Moreover, compared with standard CCRT treatment, patients with tumor markers above the threshold levels (CA125 > 20.5 U/mL, SCC-Ag > 22.8 μg/L) might have greater DFS and PFS from adjuvant chemotherapy after CCRT. The limitations of the present study is its retrospective nature. Well-designed prospective, randomized clinical trials are required to confirm further the clinical efficacy of CCRT plus adjuvant chemotherapy in patients with LACC.
Supplemental Material
Supplemental Material, sj-jpg-1-ccx-10.1177_1073274821989307 - A Multi-Institutional Retrospective Analysis of Oncologic Outcomes for Patients With Locally Advanced Cervical Cancer Undergoing Platinum-Based Adjuvant Chemotherapy After Concurrent Chemoradiotherapy
Supplemental Material, sj-jpg-1-ccx-10.1177_1073274821989307 for A Multi-Institutional Retrospective Analysis of Oncologic Outcomes for Patients With Locally Advanced Cervical Cancer Undergoing Platinum-Based Adjuvant Chemotherapy After Concurrent Chemoradiotherapy by Ning Wu, Xing Su, Honglin Song, Ying Li, Fei Gu, Xiaoge Sun, Xiaofan Li and Guanghui Cheng in Cancer Control
Supplemental Material
Supplemental Material, sj-jpg-2-ccx-10.1177_1073274821989307 - A Multi-Institutional Retrospective Analysis of Oncologic Outcomes for Patients With Locally Advanced Cervical Cancer Undergoing Platinum-Based Adjuvant Chemotherapy After Concurrent Chemoradiotherapy
Supplemental Material, sj-jpg-2-ccx-10.1177_1073274821989307 for A Multi-Institutional Retrospective Analysis of Oncologic Outcomes for Patients With Locally Advanced Cervical Cancer Undergoing Platinum-Based Adjuvant Chemotherapy After Concurrent Chemoradiotherapy by Ning Wu, Xing Su, Honglin Song, Ying Li, Fei Gu, Xiaoge Sun, Xiaofan Li and Guanghui Cheng in Cancer Control
Supplemental Material
Supplemental Material, sj-jpg-3-ccx-10.1177_1073274821989307 - A Multi-Institutional Retrospective Analysis of Oncologic Outcomes for Patients With Locally Advanced Cervical Cancer Undergoing Platinum-Based Adjuvant Chemotherapy After Concurrent Chemoradiotherapy
Supplemental Material, sj-jpg-3-ccx-10.1177_1073274821989307 for A Multi-Institutional Retrospective Analysis of Oncologic Outcomes for Patients With Locally Advanced Cervical Cancer Undergoing Platinum-Based Adjuvant Chemotherapy After Concurrent Chemoradiotherapy by Ning Wu, Xing Su, Honglin Song, Ying Li, Fei Gu, Xiaoge Sun, Xiaofan Li and Guanghui Cheng in Cancer Control
Footnotes
Authors’ Note
This retrospective study was registered with the Chinese Clinical Trial Registry (ChiCTR-PRC-16008822). All procedures performed in studies involving human participants were in accordance with the ethical standards of the independent Ethical Committee/Institutional Review Board of Jilin University (20160621) and conducted in accordance with the Declaration of Helsinki. Informed consent was exempted due to the retrospective format of this study.
Acknowledgments
The authors thank the patients and their colleagues Drs. Dan Shi, Xin Guo, Mingyuan He, Baocai Liu, Yiping Zhang, and Zhuang Mao for participating in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by grants from the National Natural Science Foundation of China (grant number: 82073331, 81201737); Project of Science and Technology Development Plan of Jilin Province (grant number: 20200201524JC); Jilin University Undergraduate Education Reform Research Project (grant number: 2017XYB080); Medical Education Research Project of Chinese Medical Association Medical Education Branch, China Higher Education Society Medical Education Committee (grant number: 2018B-N15054); Youth Science and Technology Training Program in Health Commission of Jilin Province (grant number: 2018Q014) and Jilin Province Higher Education Research Project of Jilin Association for Higher Education (grant number: JGJX2020D30). The funding source had no role in the design of this study and will not have any role during its execution, analyses, interpretation of the data, writing assistance, or decision to submit results.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.