
Abstract
Introduction
The World Health Organization recommends 4 triage strategies for women with high-risk human papillomavirus infection (hrHPV). These include visual inspection with acetic acid (VIA), colposcopy, reflex cytology, and HPV16/18 partial genotyping. However, in many low-resource settings, access to colposcopy remains limited. This study aimed to compare the diagnostic accuracy of visual inspection vs colposcopy for detecting cervical intraepithelial neoplasia grade 2 or worse (CIN2+).
Methods
Women who tested positive for hrHPV and were referred for colposcopy, with cytology results available as part of routine clinical care, underwent visual inspection with 3% acetic acid immediately before colposcopy. Colposcopic impressions were recorded, and images were scored using a modified Reid colposcopic index and a modified Swede score without iodine staining. We compared diagnostic performance for CIN2+ across visual inspection, colposcopic impression, modified Reid index (score ≥4), and modified Swede score (score ≥5). Statistical analysis used IBM SPSS Statistics and the Cochran Q test, with significance set at P < .05.
Results
Among 450 women, the median age was 38.0 years. A single hrHPV type was detected in 70.4% of cases; types 16, 52, and 18 were most common. Histopathological confirmation of CIN2+ occurred in 97 women (21.6%). Diagnostic accuracy for predicting CIN2+ was 78.2% with VIA and 77.5% with colposcopic impression. Accuracy was 78.4% for the modified Reid index ≥4 and 78.2% for the modified Swede score ≥5. No significant differences were observed among the 4 methods (P = .941).
Conclusions
VIA demonstrates diagnostic accuracy comparable to colposcopy-based assessments in hrHPV-positive women evaluated within a cytology-informed clinical pathway, supporting its potential role in resource-limited settings.
Plain Language Summary
Introduction: The World Health Organization recommends four ways to check women who test positive for high-risk human papillomavirus (HPV): visual inspection with acetic acid (VIA), colposcopy, reflex cytology (Pap smear after HPV test), and testing for HPV types 16 and 18. In many low-resource countries, however, colposcopy is hard to access. Objective: This study compared how well VIA and colposcopy can detect serious cervical changes (CIN2 or worse). Methods: Women who tested positive for high-risk HPV were examined with VIA and then with colposcopy. Colposcopy findings were scored using two standard systems (Reid and Swede scores). We compared the ability of these tests to identify CIN2+. Results: 450 women were included, with a median age of 38 years. Most women (70%) had only one type of HPV, most often types 16, 52, or 18. CIN2+ was confirmed in 97 women (about 22%). Accuracy rates were: 78.2% for VIA 77.5% for colposcopic impression 78.4% for Reid score ≥478.2% for Swede score ≥5. There was no significant difference between the four methods. Conclusions: VIA worked just as well as colposcopy-based methods for finding serious cervical changes in women with high-risk HPV. This suggests VIA could be a practical alternative in places where colposcopy is not widely available.
Introduction
Since the World Health Organization announced its 90-70-90 targets by 2030, stakeholders have aimed to eliminate cervical cancer by the next century. 1 To overcome barriers to provider-based screening, self-collected high-risk human papillomavirus (hrHPV) testing offers a promising solution. This approach exemplifies primary hrHPV screening—which replaces cytology as the first-line test— and incorporates a self-sampling strategy to expand coverage among women who cannot easily access providers while delivering high sensitivity. However, primary hrHPV screening programs must implement effective and affordable triage tests to identify women with cervical intraepithelial neoplasia grade 2 or worse (CIN2+). Those women should then be referred for diagnostic procedures or specialist evaluation.
Many HPV-positive women do not have high-grade lesions, highlighting the need for effective triage. The World Health Organization defines a “screen, triage, and treat” strategy that employs 4 sequential triage tests after hrHPV detection: cytology, HPV 16/18 partial genotyping, visual inspection with acetic acid (VIA), and colposcopy. 1 In contrast, the American Society of Colposcopy and Cervical Pathology 2019, European 2020, and Canadian 2023 guidelines omit VIA and recommend HPV 16/18 partial genotyping with reflex cytology for non-16/18 types. They refer women with HPV 16 or 18 positivity—or non-16/18 positivity plus abnormal cytology—to colposcopy.2-4
In Thailand, primary cytology screening began in 2005, and policymakers adopted primary hrHPV testing alone in 2020. Nevertheless, the cervical cancer incidence in Thailand remains high at 16.4 per 100 000 women. 5 A study reported a 79.7% screening coverage among eligible Thai women in 2014, yet failures in follow-up management likely sustained disease burden. 6 Colposcopy services in Thailand remain concentrated in academic centers and some provincial hospitals, limiting access to follow-up care for many women. This pattern mirrors global trends in developing and low-resource countries, where adherence to colposcopy after a positive screen ranges from 38% to 83%, with higher rates in urban areas.7-9 VIA performed by trained community healthcare workers offers an accessible downstream evaluation option for women who test positive for hrHPV.
Despite the expansion of primary hrHPV screening in Thailand and the availability of multiple post-screening evaluation strategies, evidence comparing VIA’s diagnostic accuracy with standard colposcopy in this setting is scarce. Therefore, this study aimed to compare the diagnostic accuracy of visual inspection vs colposcopy for detecting cervical intraepithelial neoplasia grade 2 or worse (CIN2+) among hrHPV-positive women evaluated within a cytology-informed clinical pathway. We hypothesized that VIA would demonstrate diagnostic performance comparable to colposcopy for detecting CIN2+ in hrHPV-positive women.
Material and Methods
This prospective comparative study received approval from the Siriraj Institutional Review Board (SIRB) (COA No. Si 574/2024) and was registered at the Thai Clinical Trials Registry (20240701003). We conducted the study in accordance with the 2015 Standards for Reporting of Diagnostic Accuracy Studies guidelines. This study was conducted in accordance with the Helsinki Declaration of 1975, as revised in 2024.
Participants and Data Collection
The inclusion criteria were women who tested positive for hrHPV on primary screening using a clinician-collected extended hrHPV genotyping test and were subsequently referred for colposcopy due to one of the following: HPV16/18 positivity, hrHPV positivity with abnormal reflex cytology, or persistent hrHPV positivity with NILM cytology. As part of routine clinical care, many participants had undergone co-testing or reflex cytology prior to referral for colposcopy. Cytology results were therefore available to examiners at the time of VIA and colposcopic assessment. This reflected routine clinical practice. We also required participants to be nonpregnant, have no history of cervical neoplasia or cancer, and provide informed consent. Participants with type 3 transformation zone, HIV positivity, inadequate colposcopic visualization, or missing tissue for pathology were excluded.
We calculated the sample size based on an expected sensitivity and specificity of 80% with a 10% allowable error and a 95% confidence level. This calculation required 62 participants each for histologically confirmed cervical intraepithelial neoplasia grade 1 (CIN1) and CIN2+ lesions. Assuming a CIN2+ prevalence of 14%, the required sample size was 443, and a total of 450 participants was estimated to account for potential data loss. 10
This study was conducted at a single tertiary academic medical center. Experienced gynecologic oncologists performed all colposcopy procedures (SK, IR, WK, PI), blinded to VIA findings. Prior to routine colposcopic examination, they applied 3% acetic acid and conducted visual inspection at 1 min, which was evaluated by MU. VIA findings were classified as negative, positive, or suspected cancer per the International Agency for Research on Cancer (IARC) criteria. 11 The VIA results remained blinded to the colposcopists throughout the procedure. Following a repeat application of acetic acid, the oncologists conducted colposcopic assessment with a 3.4‒21.2× magnification colposcope. They used 3 standardized approaches: colposcopic impression, the modified Reid’s colposcopic index, and the modified Swede score, omitting the iodine-staining component. The oncologists classified colposcopic impression according to the 2011 International Federation for Cervical Pathology and Colposcopy guidelines as normal, positive minor (grade 1), positive major (grade 2), or suspected invasive cancer. 12 They obtained biopsies from all acetowhite lesions and performed random biopsies at the 6 and 12 o’clock positions when no acetowhite areas were visible. A single gynecologic pathologist (SH) evaluated all histopathological specimens. Women with CIN2+ were treated with excisional procedures, invasive cancer cases were referred for oncologic care, and ≤CIN1 lesions were followed according to national guidelines.
Statistics
We collected demographic data, HPV genotyping, concurrent or reflex cytology results, VIA and colposcopic findings, and histopathological outcomes. Statistical analyses were performed using IBM SPSS Statistics version 29 (IBM Corp, Armonk, NY, USA). We reported descriptive data as frequencies and percentages or as medians with interquartile ranges, as appropriate. To evaluate the diagnostic performance of VIA and colposcopy, we used histologically confirmed CIN2+ as the reference standard. This allowed us to assess sensitivity, specificity, positive and negative predictive values, and accuracy. Receiver operating characteristic curves and 95% confidence intervals (CIs) were calculated. Youden’s index was used to determine the best cutoff points of the modified Reid index and the modified Swede score. Diagnostic accuracy was compared using Cochran’s Q test. Regression analysis was used to assess the combined effect of hrHPV genotyping and VIA findings on occult CIN2+ prevalence, reported as odds ratios (OR) with 95% CIs. We defined statistical significance as P < .05.
Results
The flow of participants, inclusion and exclusion criteria, and analysis populations is depicted in Figure 1. Among 450 participants, the median age was 38.0 years (interquartile range [IQR] = 32.0‒44.0), and nulliparous women comprised 52.7% of the cohort (Table 1). Atypical squamous cells of undetermined significance represented the most common index cytology result (40.7%). All screening samples were collected by clinicians. The most frequently detected genotypes were HPV 16, 52, 18, 58, and 39. According to the IARC classification, 144 women had the highest-risk genotype (HPV 16), 45 had other high-risk types (HPV 18 or 45), and 137 had medium-risk types (HPV 31, 33, 35, 52, 58). Another 117 women had lower-risk genotypes (HPV 39, 51, 56, 59, 68). We recorded positive VIA results in 24% of women and colposcopic impressions indicating CIN2+ lesions in 26.8%. Histopathology confirmed CIN2+ in 21.6% of participants. All four cancer cases were microscopic lesions classified per the International Federation of Gynaecology and Obstetrics 2018 staging: three stage IA1 squamous cell carcinoma (associated with isolated HPV 16, 52, or 58 infections) and one stage IB1 adenocarcinoma associated with HPV 16. Table 2 presents diagnostic performance comparisons for 4 evaluative methods in predicting histologically confirmed CIN2+ lesions. VIA demonstrated a diagnostic accuracy of 78.2% for predicting CIN2+. The corresponding accuracies were 77.5% for colposcopic impression, 78.4% for modified Reid index ≥4, and 78.2% for modified Swede score ≥5. No significant differences were observed across the four methods (P = .941). Combining hrHPV genotypes with VIA findings (Table 3) revealed a high prevalence of occult CIN2+, with rates as high as 58-62% in women positive for HPV 16 or 52 and VIA. Flowchart of participant inclusion, exclusions, and analysis populations Characteristics of Study Participants and Findings on Cytology, hrHPV Genotyping, VIA, Colposcopy, and Histopathology (N = 450) Abbreviations: HPV, human papillomavirus; hrHPV, high-risk human papillomavirus; VIA, visual inspection with acetic acid. Data are n (%) unless otherwise indicated. Preceding cytology categories follow the Bethesda nomenclature. Colposcopic impression classified per the 2011 International Federation for Cervical Pathology and Colposcopy criteria. Colposcopy scores are median (interquartile range). Diagnostic Performance of VIA and Colposcopic Methods for Detecting Histologically Confirmed Cervical Intraepithelial Neoplasia Grade 2 or Worse Lesions Abbreviations: CI, confidence interval; NPV, negative predictive value; PPV, positive predictive value; RCI, Reid’s colposcopic index; SS, Swede score; VIA, visual inspection with acetic acid. Reference standard: histologically confirmed cervical intraepithelial neoplasia grade 2 or worse. Diagnostic Performance of VIA Triage Among Women Positive for Each HPV Genotype in Detecting Histologically Confirmed Cervical Intraepithelial Neoplasia Grade 2 or Worse Lesions Abbreviations: CIN2+, histologically confirmed cervical intraepithelial neoplasia grade 2 or worse; HPV, human papillomavirus; VIA, visual inspection with acetic acid.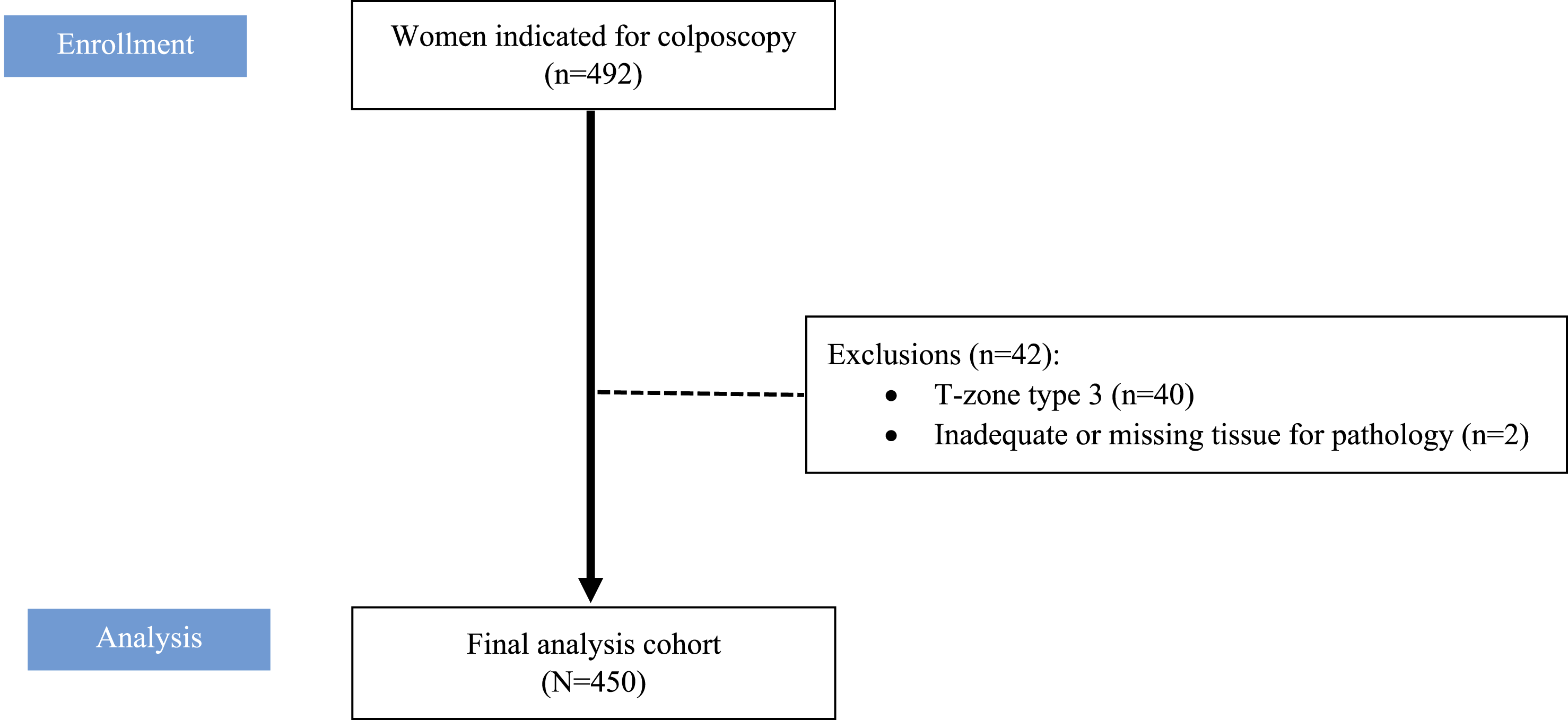



Discussion
The current study found that VIA and colposcopy demonstrated comparable diagnostic accuracy for predicting CIN2+. Barriers to colposcopy access include delayed notification of abnormal results, long travel distances, high travel costs, rural residency, and healthcare personnel shortages.8,13 Given these barriers, VIA may serve as a practical alternative to colposcopy in settings with limited resources.
Studies have evaluated VIA in roles including primary screening—alone or co-testing with hrHPV or cytology—and as a triage test after positive hrHPV from self-collected samples. In women aged 30-59, VIA primary screening alone reduced cervical cancer incidence (hazard ratio = 0.75, 95% CI = 0.55‒0.95) and mortality (hazard ratio = 0.65, 95% CI = 0.47‒0.89). 14 Studies show limited benefit when using VIA adjunctively in co-testing with hrHPV or cytology.15,16 Researchers have investigated VIA as a triage method following hrHPV detection in 2 contexts: provider-collected and self-collected specimens.
In the ESTAMPA study, 14% of women with provider-collected samples tested positive for hrHPV, and 15% of those with hrHPV-positive samples had CIN2+ lesions. Colposcopy as a triage method identified suspected CIN2+ in 13.2% of women, with a sensitivity of 90.4% for CIN2+ and a specificity of 50.1% for less than CIN2. In contrast, VIA detected major abnormalities or suspected cancer in 52.6% of women with sensitivity of 83.9% and specificity of 54.6% for detected CIN2+ lesions. The ESTAMPA study reported high variability in VIA performance, limiting its reliability as a triage tool.17,18 These findings suggest that VIA may overdiagnose disease compared with standard colposcopy, potentially leading to unnecessary treatments.
Three studies in Cameroon, Ethiopia, and Madagascar reported hrHPV positivity rates of 18.6%, 22.2%, and 28% among women using self-sampling. The Cameroonian study applied VIA to triage women for immediate thermal ablation or loop electrosurgical excision. In that study, clinicians also performed cytology, VIA-guided cervical biopsy, and endocervical curettage. Histology confirmed CIN2+ in 12.2% of participants; VIA detected abnormal findings in 58.1%. VIA sensitivity, specificity, positive predictive value, and negative predictive value for CIN2+ were 77.1%, 43.8%, 16.1%, and 93.2%. 19 In the Ethiopian cohort of 197 hrHPV-positive women, VIA sensitivity and specificity for CIN2+ detection were 25.0% and 82.7%. 20 In the Malagasy study of 345 hrHPV-positive women, VIA positivity was 68.9%, and CIN2+ prevalence was 5.8%. 21 Compared with our findings, those studies showed higher CIN2+ prevalence and lower VIA positivity. These results underscore the need for experienced personnel to perform VIA and reduce variability and overdiagnosis. The relatively modest sensitivity of VIA in this study may reflect the use of strict IARC criteria, which prioritize specificity and may under-detect subtle lesions.
Researchers have evaluated the use of VIA as a triage method for colposcopy referral. An Indian study reported 19% hrHPV positivity via self-sampling, with 15.9% diagnosed with CIN2+. VIA triage yielded a 19.5% positivity rate, identifying women for colposcopy referral. 22 Wang et al evaluated a single-visit model that combined VIA and hrHPV testing. In their study, 12.8% of women screened hrHPV positive, 18% had positive VIA, and among hrHPV-positive women, 18.3% had positive VIA. Histopathology confirmed that CIN2+ was identified in 15.5% of women who tested positive on both tests, supporting colposcopy referral and treatment in this subgroup. 23 In comparison to our study, VIA was positive in 24% of hrHPV-positive women, suggesting that VIA could reduce colposcopy referrals to approximately 20%.
Our study found that VIA accuracy for detecting CIN2+ lesions was comparable to that of colposcopy. Adapting the World Health Organization’s “screen-triage-treat” strategy to “screen-triage-biopsy-treat” could enhance diagnostic accuracy. This more reliably identifies CIN2+ and reduces missed microscopic cancers. Additionally, implementing a ‘screen-and-treat' strategy using VIA in cases of HPV 16 or 52 positivity may help reduce overtreatment rates. In our cohort, HPV 52 was frequently associated with CIN2+ lesions alongside HPV 16, reflecting genotype patterns commonly reported in East Asian populations. 24 In contrast, previous studies have shown that, beyond HPV 16 and 18, other high-risk genotypes also contribute meaningfully to CIN2+ risk—particularly HPV 31 and 33 in the United States,25,26 and HPV 35 in African populations. 27 However, consistent VIA performance demands the standardized IARC-recommended training, ongoing quality assurance, and regular monitoring. These measures ensure a skilled workforce. Finally, because VIA is generally unsuitable for women with a type 3 transformation zone, alternative post-screening evaluation methods—such as genotyping, cytology, or direct colposcopy—may be more appropriate for this subgroup.
This study’s strengths include its conduct in a population with a high cervical cancer prevalence, blinding colposcopists to VIA results, and obtaining biopsies for all participants to confirm diagnoses. A gynecologic pathologist evaluated all histopathological specimens to ensure diagnostic accuracy. Because VIA and colposcopy assessments were performed in real time by gynecologic oncologists, we minimized the risk of misinterpretation from poor-quality image capture.
In this study, VIA and colposcopy were performed after primary hrHPV testing with cytology results available as part of routine clinical care. This diagnostic sequence may have contributed to the observed sensitivity and specificity of both methods, as prior cytology information could influence visual interpretation during VIA and colposcopy. Importantly, cytology results were not blinded to examiners, reflecting real-world clinical practice but limiting interpretation of VIA and colposcopy as independent triage tests following HPV alone. Accordingly, our findings should be interpreted as demonstrating comparable performance of VIA and colposcopy within an HPV-plus-cytology evaluation framework.
However, the study has limitations. It lacked long-term follow-up data on subsequent surveillance testing and did not capture cumulative histological outcomes or recurrent CIN cases. Future research should include large-scale community implementation with extended follow-up and randomized controlled designs to compare cumulative CIN2+ incidence detected by VIA vs colposcopy. Adding immunohistochemistry markers (eg, p16/Ki-67) may improve VIA diagnostic performance and reduce reliance on confirmatory histology. A cost-effectiveness analysis is also warranted to assess each method’s practicality in resource-limited settings.
Conclusion
VIA demonstrated diagnostic performance comparable to colposcopy in hrHPV-positive women evaluated within a cytology-informed clinical pathway.
Footnotes
Author Note
Poster Presentation: The ASCCP 2025 Scientific Meeting themed “Moving from Concepts to Caring” in San Diego at the Sheraton San Diego Hotel & Marina from April 24 to April 26, 2025.
Acknowledgements
The authors extend their sincere gratitude to Mr Suthipol Udompunturak for his support with the statistical analyses. Additionally, we thank Miss Sarocha Boonkate, an administrative officer, for her role in data collection.
ORCID iDs
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki and received ethics approval from the Siriraj Institutional Review Board (SIRB) COA no. Si 574/2024, on July 25, 2024.
Consent to Participate
Written informed consent was obtained from all participants prior to enrollment.
Author Contributions
All the authors contributed to the study design and conceptualization. SK, WK, MU, PI, and IR managed the enrollment process, performed VIA and colposcopy, and collected images. SH evaluated and reported the histology results. MU collected the data. SK, WK and IR analyzed and interpreted the data. SK drafted the manuscript, while WK and IR revised it for important intellectual content. WK and IR were essential intellectual contributors. Consent for publication has been obtained from all authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The study data are not publicly available due to privacy concerns, but are available upon request from the corresponding author.