
Abstract
Introduction:
Uptake of cervical cancer screening services in Chinese migrant workers is unknown and may be lower than non-migrant workers in China.
Methods:
We conducted a cross-sectional study among migrant and non-migrant women aged 21-65 at 7 provinces across China and administered a questionnaire investigating knowledge and attitudes regarding cervical cancer, human papillomavirus (HPV), and HPV vaccine. We used multivariable logistic regression to evaluate odds of previous cervical cancer screening in migrant workers.
Results:
737 women participated in the study. Mean age was 41.9 ± 7.2 years. 50.2% of the participants were migrant workers. 27.6% of the migrant workers reported previous cervical cancer screening compared to 33.2% of local participants. 36.6% migrant workers reported awareness of HPV compared to 40.2% of local participants. In adjusted analysis migrant status was not associated with increased odds of previous cervical cancer screening (aOR = 1.11 95%CI: 0.76-1.60). High school or higher education compared to less than high school education and employer-sponsored insurance compared to uninsured were associated with increased odds of previous cervical cancer screening (aOR = 2.15 95%CI: 1.41-3.27 and aOR = 1.67 95% CI: 1.14-2.45, respectively). Having heard of HPV compared to no awareness of HPV was associated with increased odds of cervical cancer screening (aOR = 2.02 95%CI: 1.41-2.91). Awareness of HPV among migrant workers was associated with increased odds of cervical cancer screening compared to migrant and local participants without awareness (aOR = 2.82 95% CI: 1.70-4.69 and 2.97 95%CI: 1.51-5.83, respectively).
Conclusions:
Efforts to increase education opportunities, provide insurance, and promote HPV awareness could increase cervical cancer screening uptake in migrant women in China.
Introduction
The rapid urbanization and development of China has led to massive amounts of internal migration. In 2018 there were an estimated 288 million rural migrant workers in China. 1 These migrant workers are defined by the China Labor Bulletin as workers that hold a rural household registration (Hukou) and are employed by an urban workplace and reside in an urban area. These people serve as important economic pillars, providing a cheap, young, and replaceable workforce in a rapidly developing country. 2 Despite their economic role, migrant workers have unequal access to education, healthcare, and childcare support in their transplanted homes. 3 -5 This is due to the Chinese Hukou system which grants Chinese citizens access to education, healthcare, and other social services when they live in the rural area they or their parents were born in, but not in the transplanted urban centers where migrant workers actually live and work. 6
Cervical cancer continues to be a major issue in developing countries like China. Currently, cervical cancer is the fourth most frequently detected cancer among females worldwide, with an estimated 570,000 new cases and 311,000 deaths in 2018. 7 In 2018, there were an estimated 106,430 new cases of cervical cancer and 47,739 deaths related to cervical cancer in China. 7 China has invested substantial amounts of resources into population-wide cervical cancer screening programs since 2009 so that local townships are able to provide pap tests, Human Papillomavirus (HPV) DNA testing, or visual inspection with acetic acid/Lugo’s iodine (VIA). 8,9 With these efforts, proportion of Chinese women aged 20-64 reporting ever receiving screening ranges from 25.7% of all women, 33.7% in eastern urban centers compared to 24.4% in eastern rural regions, 26.9% in middle urban areas compared to 20.3% in middle rural regions, and 25% in western urban regions compared to 23.6% in western rural regions. 10 Despite these efforts, it is unknown how effective these programs have been for migrant workers. It is thought that due to the lack of national health insurance, lower rates of employer-sponsored insurance, and high out-of-pocket expenses, over half of migrant workers do not have access to a health care provider when they need it. 11 -13 Furthermore, previous studies have found that migrant workers in other countries have impaired access to cancer screening and other preventative services, including cervical cancer screening. 14 -17
Thus, the objective of our study was focused on evaluating uptake of cervical cancer screening services in migrant workers compared to non-migrant workers in major metropolitan areas of China. We hypothesized that migrant workers would have less uptake of cervical cancer screening as compared to non-migrants.
Methods
This study was a multi-center, cross-sectional study conducted in 7 different provinces across China on March 8, 2015, using stratified multi-stage non-randomized cluster sampling. Cities and provinces included: Changzhi, Shanxi; Urumqi, Xinjiang; Dalian, Liaoning; Wuhan, Hubei; Guangzhou, Guangdong; Chengdu, Sichuan; and Jinan, Shandong. These cities were chosen due to high migrant population and to recruit a diverse sample of migrant women. Women were recruited for 2 weeks prior to the study day through convenience sampling via posted flyers in the surrounding neighborhoods around the hospital at each city. Migrant women were defined as women who held a rural household registration (Hukou) and who have worked in an urban destination for at least 3 months and no more than 5 years. Local participants were defined as those who held a Hukou registration at the research site’s location. Further eligibility requirements included: 21 to 65 years of age, able to consent to participate in the study, not currently pregnant, and no history of previous high-grade cervical lesions, treatment for cervical disease, or hysterectomy. Written informed consent was acquired from each participant. If participant was unable to speak or read Mandarin, local study staff read and explained the questionnaire and informed consent form to the participant in the necessary local dialect. The study was approved by the Ethical Review Committee of the Cancer Institute, Chinese Academy of Medical Sciences in Beijing, China.
Questionnaire in Mandarin Chinese was self-administered to evaluate socio-demographic information as well as knowledge and attitudes toward cervical cancer, HPV, and HPV vaccine. The outcome of interest for this study was prior history of cervical cancer screening, as evaluated by the following question: “Have you ever had cervical cancer screening?” (yes/no). Primary independent variable of interest for this study was migrant status. In addition, we assessed interaction between migrant status and education, insurance status, and awareness of HPV. For purposes of multivariate and interaction analysis, education was dichotomized to less than high school education and high school and higher education. Education was considered as a possible interaction variable as migrant workers often receive inferior education, lack access to education, and the high mobility can cause fragmented education. 18 Furthermore, it was hypothesized that education would affect migrant women’s understanding of the importance of cervical cancer screening. Insurance status was dichotomized for purpose of interaction analysis to yes/no (no/do not know). Migrant workers are not offered state-sponsored insurance in their transplanted homes, but some migrant workers possess employer-sponsored insurance. 3 We hypothesized there was an interaction effect with migrant status and insurance status on odds of prior cervical cancer screening. Finally, having heard of HPV was evaluated for interaction as migrant workers often do not seek preventative services but are known to have high health information seeking behaviors. 19,20
Two data input clerks in each research site were recruited to double-enter data from the questionnaire to the computer-based database independently. All finished double-entry databases were sent to Beijing research center for validation by running EpiData (EpiData Association, Odense, Denmark). In case of any inconsistencies found by the Beijing research center between the 2 databases, the 2 local data entry clerks were required for adjudication until all database discrepancies were addressed.
Statistical analysis was performed utilizing STATA 16 (College Station, TX). Frequency and percentages were calculated to describe the characteristics of participants, knowledge of cervical cancer and HPV, as well as previous cervical cancer screening. The Chi-squared test, proportional z-test and Mann-Whitney test was used when comparing quantitative variables between migrant workers and local workers. Univariate logistic regression model among participants with complete information was employed to analyze the associations of potential factors with previous cervical cancer screening and then multivariable logistic regression among participants with complete information to examine the associations of migrant status with the outcome variable. Confounders were isolated using direct acyclic graphs to identify relationships between the predictor variable and outcome variables. 21 Age, marital status, and ethnicity were covariates thought to possibly have a confounding effect and were selected a priori. Age was chosen because older women are less likely to be migrant workers and to have been screened for cervical cancer. 19,22,23 Marital status was controlled for because unmarried Chinese are less likely to be screened for cervical cancer and more likely to be migrant workers. 23,24 Finally, ethnicity was adjusted for as Chinese ethnic minorities are more likely to be migrant workers and are much less likely to be screened for cervical cancer. 23,25 Odds ratios (ORs) with corresponding 95% confidence intervals (CIs) were calculated and reported. In addition, interaction analysis was done with prespecified variables. We tested for multiplicative by including the product term in multivariate logistic regression models. Additive interactions (relative excess risk due to interaction, RERI) were evaluated by ORs derived from multivariate logistic regression models. This study applied a 2-tail test with α = 0.05 and β = 0.20. Statistical power was originally calculated based on the hypothesized absolute difference of 10% in screening between migrant women and non-migrant women. This absolute difference was based on previous differences found between rural and urban screening rates. 23 The number of participants needed in each group was 356 as calculated using a sample size calculator. 26 Considering that China has 7 geographic regions, this study planned to include approximately 100 women (50 migrant and 50 non-migrant women) from each region.
Finally, in an effort to improve assessment of our study’s strengths and weaknesses we followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) cross-sectional reporting guidelines when presenting our study. 27
Results
Participants Characteristics
Of the 739 participants enrolled in the study, 2 were excluded for final analysis as they were over the inclusion criteria for age. For the included participants in initial analysis (n = 737), 50.2% (n = 370) were migrant worker participants and 49.8% (n = 367) were local participants. Average age of participants was 41.9 ± 7.2 years. 93.9% were married, and 94.6% had at least one child. 89.6% of participants identified as Han Chinese, of which 13.0% of migrant workers were non-Han Chinese compared to 7.9% of local participants (P = 0.02). At least 40% of participants had completed high school, of which 27.6% of migrant workers had completed high school compared to 53.4% of local participants (P < 0.001). 47.5% lacked employer-sponsored insurance, of which 55.6% of migrant workers lacked insurance compared to 39.4% of local participants (p < 0.001). Median household income per year was 41,000 with interquartile range of 40,000 (in RMB as of March 2015 1 USD = 6.14 RMB). Finally, 38.4% of the participants had heard of HPV before, with 36.6% of migrant workers stating that have heard of HPV and 40.2% of non-migrant workers (Table 1).
Demographics of Study Participants (n = 737).
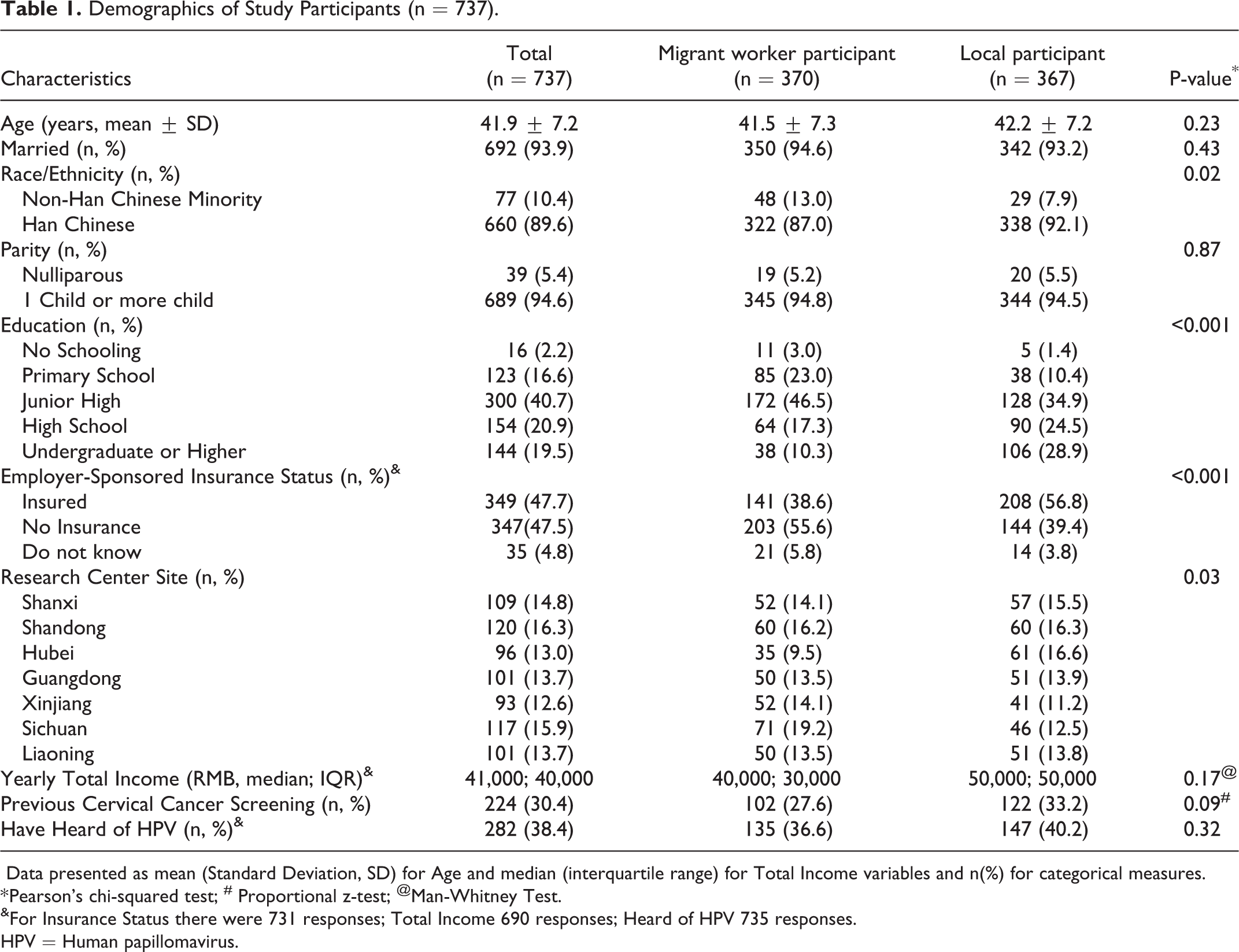
Data presented as mean (Standard Deviation, SD) for Age and median (interquartile range) for Total Income variables and n(%) for categorical measures.
* Pearson’s chi-squared test; # Proportional z-test; @Man-Whitney Test.
&For Insurance Status there were 731 responses; Total Income 690 responses; Heard of HPV 735 responses.
HPV = Human papillomavirus.
Relationship Between Migrant Status and Reporting Previous Cervical Cancer Screening
Overall, 30.4% of the participants reported previous cervical cancer screening. Of those, 27.6% (95%CI: 23.0-32.1) of migrant workers had been previously screened compared to 33.2% of local participants (95%CI: 28.4-38.1), though they were not statistically different (P = 0.09). In bivariate analyses, migrant status as compared to local participants was associated with decreased odds of previous cervical cancer screening (OR = 0.76 95%CI: 0.56-1.05), but not statistically significance. Those with high school or higher education as compared to those with less than high school education and those with employee-sponsored insurance compared to uninsured had increased odds of previous cervical cancer screening (OR = 2.62 95%CI: 1.89-3.61 and OR = 2.31 95%CI: 1.68-3.21, respectively). Having heard of HPV was associated with increased odds of cervical cancer screening (OR = 2.70 95%CI: 1.95-3.72) (Table 2).
Reporting Previous Cervical Cancer Screening (N = 729@).

aOR = adjusted Odds Ratio; CI = Confidence Interval; HPV = Human papillomavirus.
*=adjusted for all variables included in table.
In our adjusted model (n = 729 with complete records for variables of interest) without interaction analysis, odds of previous cervical cancer screening was not significantly different among migrant workers compared to local participants (aOR = 1.11 95%CI: 0.76-1.60). High school or higher education compared to less than high school education and insured versus uninsured retained their association with increased odds of previous cervical cancer screening (aOR = 2.15 95% CI: 1.41-3.27 and aOR = 1.67 95%CI: 1.14-2.45, respectively). Finally, having heard of HPV compared to not was still associated with increased odds of cervical cancer screening (aOR = 2.02 95%CI: 1.41-2.91) (Table 2).
Interaction Between Migrant Status and Awareness of HPV
Interaction analysis (n = 729 with complete records) of migrant status and having heard of HPV provided possible measure of interaction on the multiplicative scale (OR = 1.99 95% CI: 0.99-4.04, P = 0.06) and additive scale (RERI = 1.50 95% CI: −0.16-3.16, P = 0.08). Given this possible multiplicative and additive interaction, further interaction was analyzed. Migrant workers that have heard of HPV as compared to local participants who have not heard of HPV demonstrated strong evidence for increased odds of previous cervical cancer screening (aOR = 2.97 95%CI: 1.51-5.83). Furthermore, local participants that have heard of HPV as compared to local participants that have not heard of HPV also demonstrated increased odds of having previous cervical cancer screening, though was not significant (aOR = 1.41 95%CI: 0.85-2.35). Migrant workers who have heard of HPV as compared to migrant workers who have not heard of HPV also demonstrated strong evidence for increased odds of previously being screened for cervical cancer (aOR = 2.82 95%CI: 1.70-4.69). When comparing interaction between migrant workers that have heard of HPV compared to local participants who have heard of HPV there were estimates of increased odds of previous cervical cancer screening but was not statistically significant (aOR = 2.10 95%CI: 0.98-4.49) (Table 3).
Interaction Between Migrant Status and Having Heard of HPV on Odds of Reporting Being Screened for Cervical Cancer (n = 729†).

Measure of Interaction on Multiplicative Scale: Ratio of ORs (95%CI) = 1.99 (0.99-4.04); P-value = 0.06.
Measure of Interaction on Additive Scale: RERI (95%CI) = 1.50 (-0.16-3.16); P-value = 0.08.
aOR are odds ratios of being screened for cervical cancer of non-migrant worker versus migrant worker participants adjusted for age, marriage status, research center, ethnicity, insurance status, insurance interaction, education, and education interaction.
†=Complete data available for 729 participants.
*= Reference group is the local participant who has not heard of HPV.
@=Reference group is the local participant who has heard of HPV.
#=Reference group is the migrant worker who has not heard of HPV.
aOR = adjusted odds ratios; HPV = Human papillomavirus; with/w/o = with and without; RERI = Relative excess risk due to interaction.
Interaction Between Migrant Status and Education Level/Insurance Status
Interaction between migrant status and education and migrant status and insurance status yielded minimal evidence of multiplicative or additive interaction. For interaction between migrant status and education, there was no evidence of multiplicative interaction (aOR = 0.69 95%CI: 0.21-1.51, P = 0.36) nor additive interaction (RERI = −0.76 95%CI: −2.45-0.92, P = 0.38) (Supplemental Table 1). Interaction between migrant status and insurance was not present on the multiplicative scale (aOR = 0.86 95%CI: 0.41-1.80. P = 0.69) or additive scale (RERI = −0.22 95%CI: −1.40-0.95, P = 0.71) (Supplemental Table 2).
Discussion
China has made major and impressive improvements in their cervical cancer screening coverage despite the challenges of such a massive, mobile, and rural population. Our study found that 30.4% of all our participants reported previous cervical cancer screening, corroborating current estimated screening rates. 10 However, migrant women reported a lower cervical cancer screening rate as compared to local participants in an urban setting, though not statistically significant. Our study also demonstrates that migrant women, which are from rural provinces in China, have a higher rate of screening when compared to women who primarily live in rural areas of China. 10,11 This could be due to the effects of awareness of HPV on migrant workers. Our study found that migrant workers have higher odds of previous screening if they have heard of HPV as compared to non-migrants who have heard of HPV and migrants without awareness of HPV.
Overall, awareness of HPV in our study cohort was low (∼38%) which is in line with other studies investigating HPV awareness in China. 28 -30 Our study also corroborated another study investigating awareness of HPV in migrant workers specifically, which found that about 30-36% of migrant populations had heard of HPV. 31 Though this study did find much higher awareness of HPV in local participants compared to our study (approximately 60%), this could be due to the large number of college graduates in their cohort. The odds of reporting previous screening increased if participants had heard of HPV before, similar to previous a study in China. 32 Our study is novel in that we also found that migrant status has an important interaction with awareness of HPV, as migrants are much more likely to have been screened for cervical cancer if they have heard of HPV as compared to either a migrant worker or local participants who have not heard of HPV. This could be due to migrant women’s increased use of health education materials prompting increased utilization of preventative healthcare in their transplanted homes or when they are in their home province and are able to access state-covered care. 20 Our study also suggests an important benefit of having heard of HPV in local participants for increased likelihood of previous cervical cancer screening, but this did not reach statistical significance.
Our findings are important in context as it adds to the mounting evidence that education campaigns regarding HPV, HPV vaccine, and cervical cancer increase cervical cancer screening uptake in women in China. 33 -36 Our findings suggest that these campaigns may be even more effective at increasing cervical cancer uptake in migrant populations in particular.
In addition to the association with awareness of HPV and cervical cancer screening uptake our study also found that women with higher education levels and employer-sponsored insurance are more likely to report previous cervical cancer screening. This is in line with previous studies that suggest migrant women in China are more likely to be screened if they have had higher education and employer-sponsored insurance, as employer-sponsored insurance will help overcome the cost of screening services. 23 Our study found no interaction with migrant status and education or insurance status. This suggests that increased efforts need to be made to provide these women insurance, education opportunities, and/or no-cost cervical cancer screenings services in their transplanted homes which will likely increase cervical cancer screening and other preventative health behaviors. Furthermore, these findings are in line with research investigating migrant workers in the United States and Europe. In general, low income, less education, and migratory status are all social determinants of health that limit migrant workers abilities to access cancer screening and general preventative services and lead to poor health outcomes globally. 17,37 -41
Strengths and Limitations
Our study has several limitations. First, our sample size is relatively small when considering the massive and diverse population of China. Despite this, our study enrolled participants from 7 distinct regions of the country, mirroring the diverse nature of migrant workers, which could improve generalizability. Next, given the subject matter regarding cervical cancer screening, volunteer bias is possible in this study, especially given its small sample size. Thus, our population volunteering to participate may have more interest in their health as compared to non-volunteers, though our study findings are consistent with other studies in terms of participant demographics such as education and income. Also, our study question specifically mentioned cervical cancer screening, it did not detail the different methods of screening (pap, HPV DNA testing, or VIA) and thus the question may be misinterpreted. Though, we do not believe this to be the case as previous studies have demonstrated high awareness regarding cervical cancer and need to be screened to prevent cancer. 42 In addition, our study only addresses the question of ever being screened for cervical cancer, we do not know how many of these women are actually adhering to screening every 3 years as recommended by the Chinese government. Though, if every eligible women was screened in China just once in their lifetime, cervical cancer cases could be reduced by up to 50%. 43 Future studies should investigate the adherence to the screening schedule in Chinese women, both migrant and non-migrant. Finally, this is a cross-sectional study, so we are unable to establish temporality and causality.
Conclusion
It has been estimated that without widespread HPV vaccination and screening the incidence of cervical cancer in China will triple by 2100. 44 As China continues to invest in its cervical cancer screening program, our results provide a window into current cervical cancer screening uptake in migrant populations and non-migrant workers in urban settings. Cervical cancer uptake is still low and has a lot of room for improvement. Given the interaction of prior awareness of HPV and increased association with cervical cancer screening, future studies could investigate if targeted HPV and cervical cancer related education campaigns could potentially increase cervical cancer screening uptake in both migrant workers living in urban settings as well other urban dwellers.
Supplemental Material
Supplemental Material, sj-pdf-1-ccx-10.1177_1073274820985792 - Inequalities in Cervical Cancer Screening Uptake Between Chinese Migrant Women and Local Women: A Cross-Sectional Study
Supplemental Material, sj-pdf-1-ccx-10.1177_1073274820985792 for Inequalities in Cervical Cancer Screening Uptake Between Chinese Migrant Women and Local Women: A Cross-Sectional Study by Hunter K. Holt, Xi Zhang, Shang-Ying Hu, Fang-Hui Zhao, Jennifer S. Smith and You-Lin Qiao in Cancer Control
Supplemental Material
Supplemental Material, sj-pdf-2-ccx-10.1177_1073274820985792 - Inequalities in Cervical Cancer Screening Uptake Between Chinese Migrant Women and Local Women: A Cross-Sectional Study
Supplemental Material, sj-pdf-2-ccx-10.1177_1073274820985792 for Inequalities in Cervical Cancer Screening Uptake Between Chinese Migrant Women and Local Women: A Cross-Sectional Study by Hunter K. Holt, Xi Zhang, Shang-Ying Hu, Fang-Hui Zhao, Jennifer S. Smith and You-Lin Qiao in Cancer Control
Footnotes
Abbreviations
Authors’ Note
Hunter K. Holt, MD, and Xi Zhang, MD, PhD, contributed equally to this work. This was a nationwide study conducted by YLQ, FHZ, SYH, and JSS. HKH performed the statistical analysis and drafted the manuscript. XZ participated in the data collection and revised the manuscript. All authors read and approved the final manuscript. The dataset supporting the conclusions of this article are available from the corresponding author on reasonable request. The study was approved by the Ethical Review Committee of the Cancer Institute, Chinese Academy of Medical Sciences in Beijing, China (No.14-110/900) prior to implementation. Written informed consent was obtained from each participant prior to the study.
Acknowledgments
We thank the collaborative hospitals involved in this study, including Heping Hospital affiliated to Changzhi Medical College, The Tumor Hospital affiliated to Xinjiang Medical University, Dalian Municipal Women and Children’s Medical Center, Women and Children’s Hospital of Hubei province, Guangzhou Women and Children’s Medical Center, Sichuan Cancer Hospital and Institute and Qilu Hospital of Shandong University. The authors also acknowledge the women who participated in this study from the 7 cities.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Fogarty International Clinical Research Scholars Program (Fogarty International Center, US National Institutes of Health) (5R25TW009340) and CAMS Innovation Fund for Medical Sciences (2017-I2M-1-002, 2017-I2M-3-005).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.