
Abstract
Introduction
As cancer care increasingly shifts to outpatient settings, patients with incurable cancer and their caregivers face growing challenges in addressing supportive oncology needs across five domains: informational, physical, emotional, social, and spiritual. Integration of supportive care in routine oncology practice—or primary palliative care—remains limited. Oncology encounters prioritize clinical agendas, leaving little time for supportive care and setting the stage for adverse outcomes. This study pilot tested a primary palliative care communication intervention, PRECURSOR (NCT05995860), using a nonrandomized (10 usual care control, 10 intervention) approach in a gynecology oncology clinic.
Methods
PRECURSOR combines a brief Freelisting activity—used to elicit communication intentions about supportive oncology needs among patients, caregivers, and providers—with an educational handout on the five domains of supportive oncology needs. Primary outcomes were feasibility (≥25% enrollment rate; ≥4 enrollments/month) and acceptability (overall and by component). Exploratory outcomes were communication behaviors (qualitatively coded from audio-recorded encounters) and post-encounter outcomes (via surveys).
Results
Of 1356 screened, 78 were eligible, and 20 enrolled (26%) in 38 weeks (2 enrollments/month). Most (70-78%) patients, caregivers, and providers rated PRECURSOR as acceptable overall. Patients and caregivers found both components acceptable, but providers favored the educational handout. Among exploratory outcomes, a greater proportion of the supportive oncology needs discussed during encounters were initiated by patients in the intervention group (46%), compared to control (37%). Average distress and anxiety scores were lower in the intervention group. No other patterns were observed among the exploratory outcomes. Qualitative findings indicated PRECURSOR was valuable, but refinements were suggested to increase impact.
Conclusions
PRECURSOR was a feasible and acceptable primary palliative care communication intervention in the outpatient oncology setting. PRECURSOR holds potential to foster more patient-centered communication about supportive oncology needs and improve the psychological well-being of patients and caregivers facing incurable cancer, though refinements are needed.
Introduction
Advances in treatment have made it possible for patients with incurable cancer to live long periods of time before their illness enters the terminal phase.1,2 Among the six most common cancers alone (bladder, breast, colorectal, lung, melanoma, prostate), it is estimated that nearly 700 000 people are living with incurable cancer as a chronic condition in the United States, and these numbers are expected to increase. 3 This growing cohort of cancer survivors and their caregivers experience needs that extend beyond the routine clinical aspects of care to include complex supportive oncology needs, yet research efforts to address these needs in this population are limited.3-7
Supportive oncology needs fall into five domains: informational, physical, emotional, social, and spiritual.4,8 The prevalence of these needs is high among patients with incurable cancer and their caregivers, where informational (eg, treatment risk/benefit) and physical (eg, fatigue, pain) needs approach 100%, emotional (eg, anxiety) needs approach 75%, and social (eg, social support) and spiritual (eg, spiritual pain) needs approach 50%.9,10 As cancer care increasingly shifts to the outpatient setting,11,12 patients with incurable cancer and their caregivers are experiencing greater demands navigating these supportive oncology needs. Consequently, comprehensively addressing supportive oncology needs is of critical importance to delivering high-quality cancer care when patients and caregivers interact with providers in the outpatient setting.
Unfortunately, supportive care is not routinely integrated into outpatient oncology care.4,13-16 Nearly all patients with incurable cancer and their caregivers report unaddressed supportive oncology needs due to inadequate communication during outpatient oncology encounters.5,13,17-22 Supportive care delivered by oncology providers alongside routine oncology care (ie, hereafter, primary palliative care [PPC] 23 ) requires expert communication to address supportive oncology needs. However, oncology providers disproportionately focus communication during outpatient encounters on clinical agendas (routinized assessment, test results review) and tend to dominate the conversational space (53-70% of spoken content is provider-driven).21,24-30 As a result, patients and caregivers have few opportunities to fully communicate their supportive oncology needs.21,29 Even when these needs are discussed, the conversation is typically limited to needs under the physical domain. 5 Furthermore, caregivers are frequently overlooked during these encounters, despite their central roles in supporting patients and having their own supportive oncology needs.17,26-28,31 Poor outcomes ensue from this inadequate communication, including negative patient and caregiver perceptions of the quality of care and communication received as well as increased distress, anxiety, and depression.17,32-35 When accumulated across the incurable illness trajectory, unaddressed needs also result in poor outcomes downstream, including missed opportunities for supportive care referrals and increased healthcare utilization (eg, hospitalization) that may be unwanted or burdensome.14,36,37
The impact of PPC communication interventions to address these pitfalls among the oncology population has been limited or mixed to date.38-42 Provider-directed interventions dominate, where only 18% of interventions have patient- and caregiver-directed components.36,43 This ignores the often triadic (patient-caregiver-provider) nature of encounters and generates approaches that are not patient- and caregiver-centered. Moreover, PPC interventions remain infrequent in the outpatient setting and are less likely to involve patients with incurable cancer and their caregivers, despite their elevated supportive oncology needs and growing representation within the cancer survivor population.44,45 Thus, there is an urgent need for PPC communication interventions that expand the focus of outpatient oncology encounters to address a broader set of patient- and caregiver-centered supportive oncology needs in the context of incurable illness. 14
The purpose of this study was to pilot test a theory-informed intervention called PRECursOr (PRior Elicitation of Communication Intentions for Oncology Encounters, hereafter PRECURSOR, NCT05995860) that was designed to elicit communication intentions about supportive oncology needs among the patient-caregiver-provider triad prior to an outpatient oncology encounter. The goal of the intervention was to reshape communication behaviors in the direction of supportive oncology needs during encounters, while also enhancing communication outcomes following encounters. We chose to conduct this pilot study first among patients with incurable gynecologic cancer and their caregivers, based on evidence that these individuals experience a greater number of unmet supportive oncology needs, especially in the physical and emotional domains, compared to patients with other cancers.7,46,47 This suggests they may particularly benefit from an intervention designed to target communication about supportive oncology needs. Consistent with Stage 1 of the NIH Stage Model of Behavioral Intervention Development, the primary aim was to evaluate the feasibility and acceptability of PRECURSOR. The secondary aim was to explore group differences in communication behaviors during encounters and communication outcomes following encounters.
Methods
Design
This was a nonrandomized pilot study with the usual care control group (n = 10) recruited first, followed by the PRECURSOR intervention group (n = 10). This report follows TREND guidelines for reporting of nonrandomized study designs, 48 and was approved by the Indiana University Institutional Review Board (Approval Date: 04/26/2023; IRB#18860) as well as the Indiana University Melvin and Bren Simon Comprehensive Cancer Center’s Scientific Review Committee (Approval Date: 03/10/2023; Protocol# CTO-IUSCCC-0827).
Participants
Setting
This pilot study took place at Indiana University Melvin and Bren Simon Comprehensive Cancer Center, and Indiana University Health Joe and Shelly Schwarz Cancer Center, a satellite cancer center that is a part of Indiana University Health healthcare system.
Sample and Eligibility Criteria
Patients were: (1) adult women with an incurable gynecologic cancer (evidence of refractory/progressive disease after first-line treatment or recurrent disease), (2) not receiving specialty palliative care or hospice, (3) English-speaking, (4) able to participate in the discussion during the outpatient oncology encounter (ie, no cognitive impairment), and (5) able to provide informed consent. Caregivers were: (1) identified as the individual who was primarily involved in the patient’s care, (2) able to attend the outpatient oncology encounter, (3) English-speaking, (4) able to participate in the discussion during the outpatient oncology encounter (ie, no cognitive impairment), and (5) able to provide informed consent. Providers were: (1) physicians or advanced practice providers (eg, nurse practitioner, physician assistant), (2) who specialized in gynecologic oncology, and (3) provided outpatient oncology care at one of the study sites.
Recruitment
All participants provided informed consent prior to study enrollment. Clinic appointment schedules of consented providers were screened for eligible patients. Eligible patients were identified and recruited first, followed by their primary caregivers. Eligible patients were sent a study packet (ie, standardized informational letter, copies of the patient and caregiver informed consent forms) approximately three weeks in advance of their appointment. A follow-up recruitment call was made using a standardized script within one week of the date the study packet was mailed. If interested and eligibility confirmed, verbal consent was obtained by phone and documented in the secure Research Electronic Data Capture (REDCap) study database. Caregivers were recruited either during the patient call (if cohabiting) or via a separate phone call (if living separately), with verbal consent obtained accordingly. All participants were informed of their rights and the voluntary nature of the study. Additionally, if potentially eligible patients and their caregivers were identified in real time during the clinic day, in person written informed consent was conducted on-site. Following the non-randomized approach, participants were sequentially enrolled in the study were assigned to the control group first until the control group recruitment goal was reached, followed by assignment to the intervention group until the intervention group recruitment goal was reached.
Study Conditions
PRECURSOR Intervention
PRECURSOR is a PPC communication intervention delivered immediately prior to the outpatient oncology encounter. PRECURSOR is rooted in an adapted version of the Integrative Model of Behavior Prediction and Behavior Change Theories,
49
which posits that the performance of a behavior, such as communication, is the direct result of one’s intentions to perform it (Figure 1). PRECURSOR is also informed by the Basic Science of Communication Conceptual Framework,
36
which links communication behaviors (ie, verbal and non-verbal) to immediate (ie, how communication was perceived), proximal (ie, how communication was experienced, markers of effective information exchange), and distal (ie, long-term impacts on healthcare utilization) communication outcomes. Theoretical Underpinnings of PRECURSOR
PRECURSOR integrates Freelisting to elicit communication intentions about supportive oncology needs among the patient-caregiver-provider triad. This involves participants independently generating a list of words/phrases (ie, a Freelist) in response to an open-ended prompt, “List all the words that come to mind when you think about the supportive oncology concerns/needs you hope/plan to discuss during the clinic visit today.” To ensure the utility of the Freelisting responses, participants were provided a visually concise educational handout with a standardized explanation of the five domains of supportive oncology needs and example needs under each domain (Figure 2). Freelisting was time-limited (<5 min.) and participants were encouraged to limit each item in the Freelist to a few words.
50
This approach offers a personalized alternative to preset inventories, like question prompt lists, which may lack specificity to individual clinical situations and can limit meaningful communication by constraining patients to generic concerns.
51
Participants were not instructed to discuss their Freelisting responses during the encounter, leaving the decision to discuss elicited communication intentions up to individuals as the conversation naturally occurred. PRECURSOR was delivered by the principal investigator (KL) or a trained research assistant. Educational Handout for PRECURSOR
Control Group
Participants in the control group received usual care.
Data Collection
The principal investigator or a trained research assistant collected data in a private clinic room. All study data were securely stored and captured in the REDCap study database. Data collection included: pre-encounter: collecting Freelists from the patient, caregiver, and provider independently using an electronic tablet (intervention arm only); during encounter: audio-recording the encounter; post-encounter: administering survey-based outcome measures and conducting an audio-recorded qualitative interview with patients and caregivers; and post-study: conducting a qualitative interview with providers. Participants each received a $50 gift card.
Outcome Measures
Primary Outcomes
Feasibility
This was determined through overall accrual (at least 25% of those eligible will enroll 52 ), accrual rate (4 enrollments/month), and encounter duration.
Acceptability
Perceived benefits of the intervention overall were measured using an adapted version of an 11-item, 5-point Likert scale measure. 53 The Acceptability of Intervention Measure (AIM), 54 was administered twice to determine the perceived benefits of the two intervention components (educational handout, Freelisting). This is a 4-item, 5-point Likert scale measure.
Exploratory Outcomes
Communication Intentions Before Encounters
Communication intentions about supportive oncology needs were measured via the Freelisting responses generated by patients, caregivers, and providers in the intervention arm.
Communication Behaviors During Encounters
Communication behaviors were measured by qualitatively coding the transcribed encounter recordings for conversation content consistent with the five domains (informational, physical, emotional, social, and spiritual) of supportive oncology needs.
Communication Outcomes Following Encounters
Immediate
The Heard and Understood55,56 (α = 0.84) measure, a 4-item, 5-point Likert scale instrument, and the General Subscale of the Quality of Communication 1.0 (QOC 1.0) 57 (α = 0.94) measure, a 7-item, 11-point Likert scale instrument, were used to assess how the communication was perceived by patients and caregivers immediately following encounters.
Proximal
Some proximal outcomes focused on the individual level. The Perceived Efficacy in Patient-Physician Interactions (PEPPI) Questionnaire 58 (⍺ = 0.91) measures self-efficacy to obtain medical information and get one’s most important health concerns discussed in a clinic visit and is a 5-item, 5-point Likert scale instrument. The Patient Activation Measure® (PAM®) 59 (⍺ = 0.81) assesses an individual’s perceived ability to be an effective and informed manager of their health and is a 13-item, 4 point Likert scale instrument (https://www.insigniahealth.com/). The Distress Thermometer 60 is a visual analog rating of distress, where responses range from 0 (no distress) to 10 (extreme distress). The Hospital Anxiety and Depression Scale-Anxiety Subscale (HADS-A)61,62 (⍺ = 0.85) measures generalized symptoms of anxiety. It is a 7-item, 4-point Likert scale instrument.
Other proximal communication outcomes were relational in nature. The Human Connection Scale (⍺ = 0.90) measures an individual’s perceived sense of mutual understanding, caring, and trust with a provider. It is a 16-item, 4-point Likert scale instrument. The Perceived Goals of Treatment63,64 measures whether there is a shared understanding of the treatment goals among the patient-caregiver-provider triad following the encounter. Responses are cure, live longer, or improved quality of life. Finally, Supportive Care Referrals (eg, home health, pain management, physical therapy, specialty palliative care) made immediately following encounters were tracked.
Qualitative Interview
A post-encounter qualitative interview was conducted with patients and caregivers to add explanatory insights into the feasibility and acceptability of PRECURSOR as well as opportunities for intervention refinement. The interview guide contained open-ended questions with probes to encourage in-depth responses (eg, What did you like best about the intervention? Could you tell me if there are ways you could see the intervention being improved?). Providers completed the same qualitative interview after study recruitment was complete.
Analysis
Primary Outcomes
Descriptive statistics (eg, frequency counts to tabulate proportions/averages) were used to assess the feasibility and acceptability benchmarks, except for average encounter duration, where a t-test (P < .05) was used.
Exploratory Outcomes
Communication Intentions Before Encounters
Freelisting responses were standardized by the principal investigator (KL) by grouping similar responses (eg, fatigue and tiredness; “Will chemo work?” and treatment response) and morphological derivatives (eg, anxious and anxiety). Descriptive statistics were used to assess the average length (ie, number of support oncology needs in each Freelists at the participant-level). Freelisting responses were synthesized at the domain level (proportion of patient, caregiver, and provider Freelisting responses matching to the five domains of supportive oncology needs). Individual Freelisting responses were examined for triadic concordance (proportion of encounters where patients, caregivers, and providers had at least one supportive oncology need they intended to discuss in common).
Communication Behaviors During Encounters
Communication behaviors were identified by qualitatively coding the transcriptions of the audio-recorded encounters for conversation content that was consistent with the five domains of supportive oncology needs. To do so, directed content analysis 65 was utilized, which involves a structured approach to qualitative coding wherein a priori codes are used to highlight portions of the data that represent specific codes. Accordingly, a codebook was used to guide this directed content analysis, which contained a list of codes and their operational definitions derived from supportive oncology literature.4,5,8 Each code contained three parts: (1) domain, (2) supportive oncology need, (3) participant initiating the discussion. Thus, if a patient initiated a discussion about their pain management during the encounter, that conversation content would be coded as “Physical-Pain-Patient.” These codes were synthesized by totaling the number of supportive oncology needs expressed by patients, caregivers, and providers in the intervention group vs the control. Then group differences in the distribution of those needs across the supportive oncology domains were explored.
Communication Outcomes Following Encounters
Given the pilot nature of this study, group differences in the average scores on the immediate and proximal outcome measures were explored descriptively only.
Immediate
For the Heard & Understood measure, counts of participants who answered “completely true” to all four items were tabulated. For the QOC 1.0, item ratings were averaged (range: 0-10), where higher average scores indicated higher quality of communication.
Proximal
For the PEPPI, item ratings were totaled (range: 5-25), where higher total scores indicated higher self-efficacy. For the PAM, item ratings were totaled (range: 13-52) and then converted to generate a score of 0-100, where higher scores indicated greater activation. Distress Thermometer ratings were averaged, and scores 3 or higher were considered clinically significant for this population. 66 For the HADS-A, item ratings were totaled to generate a summary score (range: 0-21), where scores 8 or higher were considered clinically significant for this population. 67 For the HCS, item ratings are totaled (16-64), where higher total scores indicated greater therapeutic alliance. Perceived Goals of Treatment responses were examined for triadic concordance among the patient-caregiver-provider triad. Counts of initiated Supportive Care Referrals were tabulated.
Results
Participant Flow
Of 1356 screened, 78 were eligible (6% eligibility), 62 approached, and 20 enrolled (Figure 3). Control group participants were recruited between June and November 2023 and intervention participants between May and November 2024. The lag between control and intervention recruitment was planned a priori and reflected a sequential enrollment approach to accommodate and separate the timing of other ongoing clinic-based research activities. Recruitment Diagram
Sample Characteristics
Sample Characteristics

*missingness.
Outcomes
Primary Outcomes
Feasibility
Among those approached, 32% enrolled (26% of those who were eligible). There were no withdrawals. This indicates PRECUSOR was feasible based on the a priori overall accrual benchmark. Yet, the accrual rate was slower than anticipated—an average of 2 enrollments/month. There were no significant group differences in encounter duration (t = 0.72, P = 0.48), where control encounters averaged 26 min (range: 10-58 min) and intervention encounters 21 min (range: 8-55 min).
Acceptability
With respect to the overall acceptability of PRECURSOR (intervention group only), 70% of patients and 78% of caregivers responded “agree” or “completely agree” to at least 80% of the overall acceptability items. With respect to the Freelisting component, 70% of patients and 89% of caregivers responded “agree” or “completely agree” to at least 80% of the AIM items. With respect to the educational handout, 70% of patients and 78% of caregivers responded “agree” or “completely agree” to at least 80% of the AIM items. This indicates patients and caregivers largely rated PRECURSOR and its components as acceptable. Additionally, 75% of the providers responded “agree” or “completely agree” to at least 80% of the overall acceptability items. However, the providers rated the educational handout component as more acceptable than the Freelisting component, where 100% of providers responded “agree” or “completely agree” to at least 80% of the AIM items for the educational handout, but only 25% responded this way to the AIM items for the Freelisting component.
Exploratory Outcomes
Communication Intentions Before Encounters
Among participants in the intervention group, patients (M = 5.1, SD = 1.9) listed a greater average number of Freelisting responses before encounters than caregivers (M = 3.8, SD = 1.0) and providers (M = 3.6, SD = 1.9). Synthesized at the domain level, most providers’ Freelists included at least one response that corresponded to intentions to communicate about supportive oncology needs under the informational (70% of provider Freelists), physical (60%), and/or social (50%) domains (Figure 4). Most caregivers’ Freelists had responses that corresponded to the same domains as providers, just in higher proportion—informational (100% of caregiver Freelists), physical (70%), and/or social (70%). Most patients’ Freelists included responses that corresponded to intentions to communicate about supportive oncology needs under all domains except the spiritual domain—informational (90% of patient Freelists), physical (70%), emotional (80%), and/or social (70%). Communication Intentions Before Encounters and Communication Behaviors During Encounters. Note. Communication Intentions About Supportive Oncology Needs are Those Elicited by the Freelisting Activity Prior to Outpatient Encounters; Communication Behaviors Represent the Supportive Oncology Needs That Were Discussed During Encounters; for Each Supportive Oncology Domain, Proportions Indicate the Total Number of Encounters Where at Least One Supportive Oncology Need That Was Freelisted (Intentions) or Discussed (Behaviors) Matched to that Supportive Oncology Domain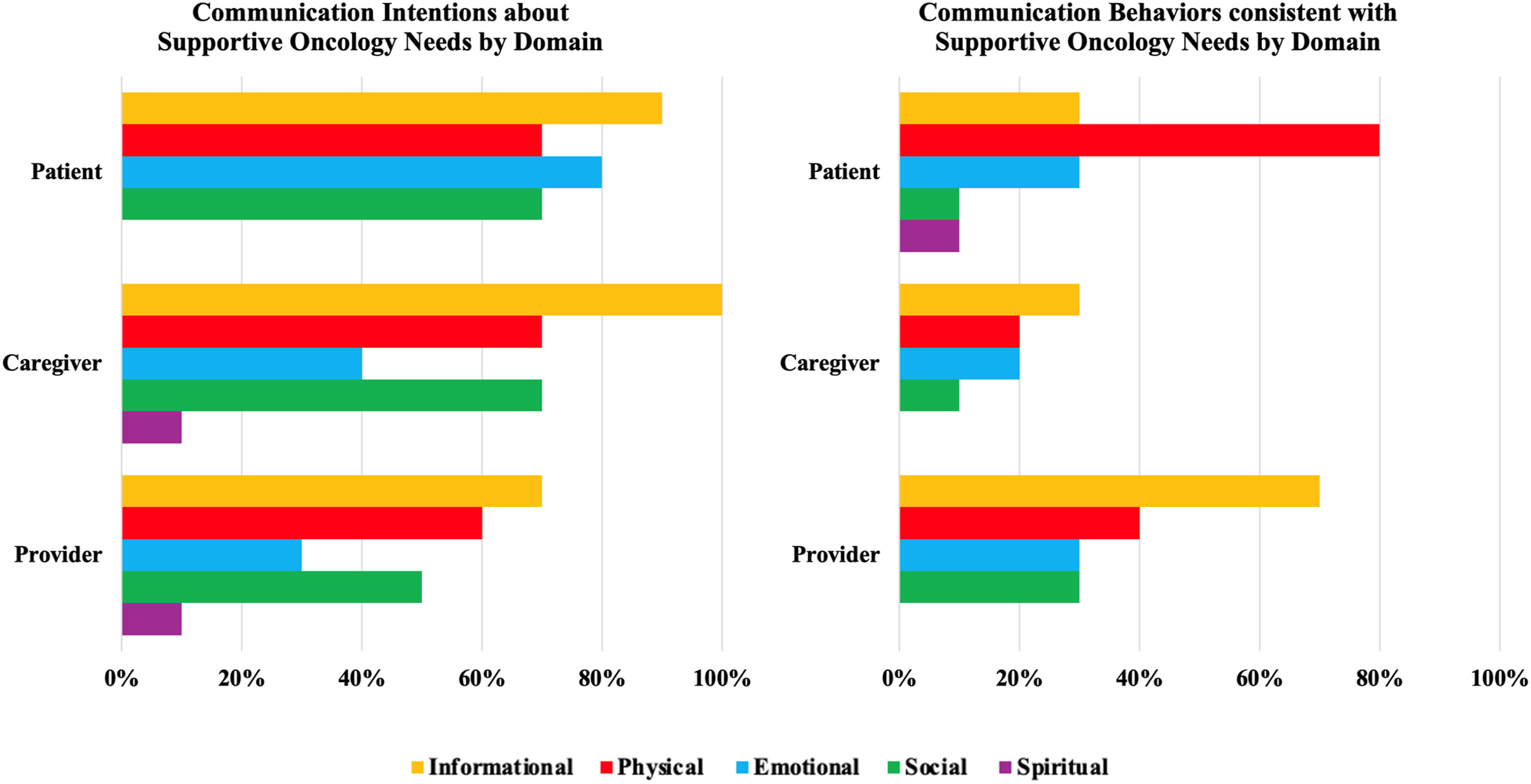
At the level of the individual Freelisting responses, patients, caregivers, and providers entered encounters with intentions to communicate about diverse and differing supportive oncology needs (Supplemental Table A). Supportive oncology needs were highly individualized, where only two (20%) of the intervention encounters demonstrated concordance among the patient-caregiver-provider triad on any one intention to discuss a supportive oncology need (eg, treatment side effects, pain control).
Communication Behaviors During Encounters
Participants in the control group initiated discussion about a greater number of supportive oncology needs (110 total, patient = 41, caregiver = 24, provider = 45) than participants in the intervention group (69 total, patient = 32, caregiver = 11, provider = 26) (Figure 5). This suggests that PRECURSOR may have led to more targeted communication during outpatient oncology encounters, making more efficient use of the conversational space. A greater proportion of the individual supportive oncology needs discussed during encounters were initiated by patients in the intervention group (46%), compared to the control (37%). This also suggests that PRECURSOR holds potential to make communication about supportive oncology needs more patient-centered during encounters. However, this pattern did not hold for caregivers, where 16% of the supportive oncology needs that surfaced during conversations were initiated by caregivers in the intervention group, compared to 22% in the control. The distribution of these discussed supportive oncology needs across the supportive care domains did not vary greatly between the intervention and control groups (Figure 5). For example, 69% of the supportive oncology needs discussed by patients in the intervention group, and 68% in the control group, fell under the informational and physical domains (Figure 5). Similar, patterns were true for caregivers and providers, indicating that when communication about supportive oncology needs occurred it typically was limited to the informational and physical domains, regardless of study condition. Supportive Oncology Need Communication Behaviors During Encounters by Domain
Freelisting responses (ie, communication intentions) were compared to the communication behaviors during encounters (Figure 4). While the providers’ communication behaviors during encounters largely mirrored their communication intentions before encounters, patients’ and caregivers’ intentions did not consistently surface during encounters. For example, 90% of patients and 100% of caregivers Freelisted intentions to communicate about supportive oncology needs under the informational domain, but only 30% of both patients’ and caregivers’ communication behaviors reflected this domain. This pattern may reflect a reluctance by patients and caregivers to bring up these supportive oncology needs or that the provider may have addressed those needs first, negating the need to bring them up.
Communication Outcomes Following Encounters
Immediate
Communication Outcomes Following Encounters

Proximal
Patients’ and caregivers’ average distress ratings approached or slightly exceeded clinically significant levels in both study conditions, but were lower in the intervention group, compared to the control (Table 2). While average anxiety scores were not clinically significant, they were lower in the intervention group, compared to the control. Patients’ and caregivers’ average ratings of their self-efficacy to communicate with providers and activation in care approached maximum ratings, regardless of study condition. Both patients and caregivers indicated high levels of therapeutic alliance with their providers, regardless of condition. Triadic concordance on the goals of treatment was infrequent—only present following 20% of the intervention encounters and 40% of control encounters. Finally, there were slightly more supportive care referrals following encounters in the intervention group (n = 3), compared to the control (n = 2).
Qualitative Interviews
Patients’ and caregivers’ qualitative interview responses largely reflected enthusiasm for PRECURSOR. One patient stated, “It allowed me to be more concise in what I really wanted, the questions I wanted addressed.” Patients and caregivers both indicated that PRECURSOR expanded their expectations of what they could discuss during their visits: “Because we come in here and we don’t really talk emotion […] we usually come in here and stick to […] the facts […] And so that did help me kind of open up a little bit to those options too.” Several caregivers also noted the value of being included: “I never got asked that before. Ever. Nobody ever really, you know, they just act like you were just there […], so it [PRECURSOR] just kind of gets your wheels turning…” and “usually when I come to these, I don't tend to ask a lot of questions. I asked a couple more questions today.” However, not all patients and caregivers found PRECURSOR personally useful, but still saw its value for others, such as patients who come to clinic appointments “solo” or for patients “new to the cancer world.” Several opportunities for intervention refinement surfaced, including the desire to have an expanded list of needs in the educational handout (e.g., “I think maybe add a little bit more options to the chart”) and to see the Freelisting responses of other members of the triad (e.g., “I would like to know. Um, I’m sure she’d [the doctor] like to know what I put in [the Freelist].”).
Providers had similar observations as patients and caregivers, valuing PRECURSOR’s impact on the range of topics they planned to discuss with patients and caregivers, “It gives you a second to think about what else the patient might be concerned about in the appointment aside from my strictly medical agenda.” Similarly, another provider noted, “it forced me to be more intentional […] making sure that I covered some things that I might not had otherwise done.” Several providers also expressed the desire to see the Freelisting responses of other members of the triad, noting that this would not only impact the thoroughness of the conversation but also give them an idea of patients’ and caregivers’ readiness to discuss more difficult topics—“…just like I walk in with my scan and I say, …here’s what your scan showed and here’s your [Freelist] results and let’s look at this together …It would be really helpful to get that like, real time information from them and just structure the visits,” and “…conversations are hard for us on the physician or provider side to bring [up] difficult prognosis […] it’s always hard to know whether the person is ready to talk …but if they’re indicating that it becomes much easier.” Providers universally noted that PRECURSOR did not interrupt clinical workflow.
Discussion
The primary outcome data collectively demonstrate the acceptability and mixed feasibility of implementing a PPC communication intervention, PRECURSOR, prior to outpatient oncology encounters for patients and caregivers facing incurable gynecologic cancer.
Primary Outcomes
Acceptability was high, with 70% or more of patients and caregivers indicating that PRECURSOR and its components were acceptable. This mirrors the high acceptability documented in other communication-based interventions in the oncology population.68-70 Caregivers rated the Freelisting component particularly favorably with qualitative data suggesting that this stemmed from the validation caregivers felt in being asked about their supportive oncology needs. Providers favored the educational handout component of, where qualitative evidence indicated that providers felt the educational handout reminded them to think beyond their clinical agendas to consider what supportive oncology needs patients and caregivers may need to discuss.
Most feasibility benchmarks were met, including overall accrual being attained, a lack of withdrawals, and the limited impact of PRECURSOR on encounter duration. However, recruitment was slow and likely stemmed from a lower than anticipated number of eligible patients at the study sites—only 6% of those screened were eligible. While PRECURSOR was received well by patients with incurable gynecologic cancer and their caregivers, this suggest the need to test PRECURSOR where it has potential to make a larger impact—among outpatient oncology clinics who are seeing larger numbers of cancer survivors living with incurable cancer, such as breast, colorectal, lung, and prostate cancers. Among the eligible participants, refusals were partially due to a lack of interest in the present study, which may have stemmed from participants’ already strong relationships with their providers and high perception of their communication, as indicated by the high therapeutic alliance and quality of communication scores prior to intervention roll-out (ie, in the control arm). PRECURSOR did not significantly impact encounter duration, thus aligning with evidence that effective communication interventions do not necessarily add significantly more time to clinical encounters.71,72
Exploratory Outcomes
Patterns in the exploratory outcomes point to preliminary evidence of the positive impact of PRECURSOR on patients with incurable cancer and their caregivers. With respect to communication behaviors during encounters, a greater proportion of the supportive oncology needs that were discussed during the encounters were initiated by patients in the intervention group compared to the control—suggesting PRECURSOR holds the potential to drive more patient-centered communication about supportive oncology needs in the outpatient setting, facilitating efforts to move away from solely provider-driven communication agendas. This finding holds significance given calls in the field to design palliative care interventions that are responsive to the individualized needs and experiences of patients with cancer and caregivers. 73 Activating patients and their caregivers in this way has been suggested as an underutilized means of improving patients’ communication with their providers. 74 Individualized patient-facing materials (ie, not structured or standardized materials) that allow time for self-reflection as a means for structuring the conversational space have been advocated in the literature, and the Freelisting component of PRECURSOR is emblematic of these recommendations.16,75
With respect to communication outcomes following encounters, patterns suggest PRECURSOR holds the potential to enhance the psychological well-being of patients and caregivers through more targeted communication about supportive oncology needs, given the lower distress and anxiety scores in the intervention group. Even though the scores were lower, it should be noted that the distress ratings were of borderline clinical significance and the anxiety scores were non-clinically significant across groups. No other discernable patterns were noted among these outcomes, particularly the more immediate communication-centric outcomes. This sample of participants reported high quality communication and feeling completely heard and understood regardless of study condition, which may be because of the patients well-established relationships with their providers. Collectively, these findings may indicate a need to identify patients and caregivers with worse quality of communication ratings or higher distress or anxiety in future studies to demonstrate greater impact.
Among participants in the intervention group, patients’ and caregivers’ communication behaviors during encounters did not always reflect their communication intentions (ie, Freelisting responses) prior to encounters, while providers’ communication behaviors were more consistent with their communication intentions prior to encounters. While Freelisting helped individuals to identify potential supportive oncology needs to discuss during the encounter, this finding suggests that more focused efforts to prioritize and negotiate discussion about these supportive oncology needs among the patient-caregiver-provider triad are necessary to structure the conversational space during outpatient oncology encounters. 76 Thus, teaching skills like agenda setting in PRECURSOR may lead to more patient- and caregiver-centered discussions in future iterations of this PPC communication intervention. Such efforts may make the best use of the limited time during outpatient oncology encounters, and prior research documents the desire for this type of visit efficiency. 77 Alternatively, it may indicate that there is not enough time to meet all supportive oncology needs during outpatient oncology encounters, suggesting an alternate solution to follow-up on these needs is warranted in future research.
Opportunities for Intervention Refinement
PRECURSOR was initially designed with scalability in mind, intending to test whether a low-touch solution (ie, triadic Freelisting about supportive oncology needs with an educational handout) was enough to create reshape PPC communication behaviors during outpatient oncology encounters and communication outcomes following encounters. The qualitative findings suggest that while PRECURSOR was acceptable and potentially beneficial, it could be improved with several refinements in future studies to augment its impact: (1) enhancing the educational handout with expanded examples of supportive oncology needs, (2) visualizing the triadic Freelisting responses, and (3) leveraging agenda setting prior to the outpatient encounter. Patients, caregivers, and providers all expressed the desire to visualize the Freelisting responses. Providers noted that knowing this information would be critical in understanding the patient’s and caregiver’s readiness to discuss difficult topics such as prognosis. Formal feedback channels after assessments of need have been endorsed as critical step toward aligning individualized priorities and enhancing communication in the oncology setting.75,77,78 Thus, refining the intervention to include the visualization of the Freelists offers a structured formal feedback mechanism for agenda setting that enables the triad to identify shared and divergent communication priorities, thereby fostering a more democratized approach toward addressing supportive oncology needs. 76
Limitations
Eligibility criteria required patients to have incurable gynecologic cancer, which could mean that patients were actively receiving treatment for their incurable disease or were on surveillance alone. This criterion along with the non-randomized approach could indicate that groups were unbalanced with respect to patients’ treatment context. If so, this may have had an underlying influence on the patterns observed among the exploratory outcomes. Given the pilot nature of this study and its small sample size, it was not statistically powered, so patterns described among the exploratory outcomes are not meant to suggest efficacy, nor generalizability. The demographic homogeneity of the sample indicates the need for more intentional recruitment strategies in future studies. Additionally, the study was limited to patients with incurable gynecologic cancer who had established relationships with their oncology providers, highlighting the importance of testing PRECURSOR among more heterogenous samples of patients with incurable cancer—including those earlier in the illness trajectory and with less established provider relationships—to better assess its generalizability in future studies.
Conclusions
PRECURSOR was a largely feasible and acceptable PPC communication intervention when delivered in the outpatient oncology setting. Exploratory outcomes underscored that PRECURSOR may have fostered a shift away from the providers agenda to more patient-centered communication about supportive oncology needs during outpatient encounters. Exploratory outcomes also suggest PRECURSOR holds potential to improve the psychological well-being of patients and caregivers when facing incurable cancer through enhanced PPC communication about supportive oncology needs. However, findings suggest that refinements to PRECURSOR’s components that augment their agenda setting potential may enhance PRECURSOR’s impact in enhancing PPC communication and outcomes in future studies. Such efforts will help actualize triadic communication intentions about supportive oncology needs during outpatient encounters, serving to address existing gaps in PPC for patients with incurable cancer and their caregivers.
Supplemental Material
Supplemental Material - A Pilot Study of a Primary Palliative Care Communication Intervention (PRECURSOR) to Address Supportive Oncology Needs for Patients With Incurable Cancer and Their Caregivers in the Outpatient Oncology Setting
Supplemental Material for A Pilot Study of a Primary Palliative Care Communication Intervention (PRECURSOR) to Address Supportive Oncology Needs for Patients With Incurable Cancer and Their Caregivers in the Outpatient Oncology Setting by Kristin Levoy, Alexia M. Torke, Krista Longtin, Marianne S. Matthias and Susan Hickman in Cancer Control
Footnotes
Acknowledgements
With deep gratitude to the patients, caregivers, and providers who participated in this research. With great appreciation to Ashley Sheets, Cheri West, and Lynne McCranor for their steadfast commitment to participant recruitment and data collection throughout the conduct of this trial. With great appreciation to Lizzie Mauro for her diligent efforts serving as a dual coder for the directed content analysis of the transcribed encounter recordings.
Ethical Considerations
This study was approved by the Indiana University Institutional Review Board (Approval Date: 04/26/2023; IRB#18860) as well as the Indiana University Melvin and Bren Simon Comprehensive Cancer Center’s Scientific Review Committee (Approval Date: 03/10/2023; Protocol# CTO-IUSCCC-0827). All participants provided informed consent prior to study enrollment. If phone-based recruitment occurred, then verbal informed consent was obtained. If in-person recruitment occurred, then written informed consent was obtained.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an American Cancer Society Institutional Research Grant from Indiana University Melvin and Bren Simon Comprehensive Cancer Center [grant number 19-144-37] as well as Richard and Kaye Woltman Endowed Graduate Fellowship in Health Communication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request with appropriate approval. Access to the data may be subject to restriction due to privacy, ethical, or legal considerations.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.