
Abstract
Introduction
Financial hardship during cancer treatment is common in privatised healthcare systems and has been extensively studied in cancer survivorship groups. The experience of financial concerns by people living with advanced, incurable cancer has been less frequently explored. This paper sought to describe the proportion of patients experiencing financial worry longitudinally, in a cohort with advanced colorectal cancer, in a publicly funded healthcare system.
Methods
This secondary analysis of a prospective, observational cohort study ‘Palliative Care Early and Systematic (PaCES)’ project, analysed data from 131 patients with advanced colorectal cancer, from Alberta’s two tertiary cancer centres, treated between January 2018 - December 2020. Rates of self-reported financial concerns were obtained from the Canadian Problem Checklist, completed monthly for 10 months and 3 monthly thereafter.
Results
Fifty-seven patients (43%) affirmed at least once that they had worried about their finances in the preceding month. Of those who reported they had “noˮ financial concerns at enrolment, 41 (35%) subsequently answered “yesˮ. The proportion of patients experiencing financial worry at any given time point fluctuated but the mean proportion was 18%. Multivariable analysis confirmed younger age (<65) was associated with more financial worry (P-value <0.01).
Conclusion
Financial worry is a common and often recurrent concern for patients with advanced colorectal cancer, particularly for younger patients. Serial screening is important to detect persisting or de novo worry.
Keywords
(a) Financial hardship is a common consequence of cancer and its treatment. It is associated with reduced quality of life and poorer outcomes. (b) Financial hardship has been most extensively described in cancer survivorship groups and within privatised healthcare systems.
(a) This secondary analysis demonstrates that financial worry is common and often recurrent in patients with advanced colorectal cancer in a publicly funded healthcare system.
(a) Serial screening for financial worry should be conducted to identify patients in need. (b) Policy change is required to better financially support patients with cancer at all stages of illness.Key Statements
What is Already Known About the Topic?
What this Paper Adds
Implications for Practice, Theory or Policy
Introduction
Financial hardship (FH) is a multi-dimensional consequence of cancer and its treatment encompassing (i) material conditions, (ii) psychological response and (iii) coping behaviours. 1 FH is associated with increased psychological symptom burden, reduced quality of life, potentially increased mortality, and challenges for those transitioning to survivorship.1-3 Financial ‘toxicity’ is sometimes used interchangeably, although is often conceptualised as a treatment side effect akin to medical toxicities. 4
Initial investigations into FH took place in the United States, a majority-privatised system in which coverage may vary with unexpected gaps and out-of-pocket costs (OOPCs), even when medical insurance or Medicare is in place. 5 The existence of universal public healthcare, however, does not mean that serious illness is without personal cost. Growing evidence from Canada, which has publicly funded healthcare, demonstrates that patients also suffer significant FH; this is driven by direct costs outside of universal coverage such as outpatient medications, some home care services, equipment, travel costs, and indirect costs such as lost income.6,7 In 2021, cancer-related costs in Canada were CAD 26.2 billion with 30% of this borne by patients and their families. 8
There is a large body of evidence examining the FH experience of cancer survivors.1,9 The impact of FH on patients receiving palliative-intent treatment or supportive care is less explored. Recent literature suggests that material financial hardship (OOPCs, productivity loss, medical debt, or bankruptcy) affects the majority of patients with metastatic colorectal cancer (CRC) and is associated with reduced health-related quality of life.1,10
Despite the established importance of this FH, many centres have no widely integrated screening tool. 11 This paper explores the longitudinal prevalence of financial worry (FW), an aspect of FH psychological response, as detected by a single-item screening question in a Canadian cohort of patients with advanced CRC.
Methods
This is a secondary analysis drawn from the multi-site, prospective, observational, cohort study ‘Palliative Care Early and Systematic’ (PaCES) Project which developed, implemented and evaluated an early palliative care pathway for patients living with advanced CRC. 12 Ethics approval was obtained from the Health Research Ethics Board of Alberta - Cancer Committee (HREBA-CC), study ID HREBA.CC-17-0429, approval date November 22, 2017. The ”Living With Colorectal Cancer: Patient and Caregiver Experience” study was registered with https://www.clinicaltrials.gov, registration number NCT03572101. All participants provided written informed consent prior to enrolment in the study. All patient data were de-identified.
Participants were receiving either palliative systemic treatment or supportive care. Recruitment took place in outpatient medical oncology clinics in two tertiary cancer centres in Alberta, Canada from January 2018 to December 2020. Eligible patients met at least one of the following criteria: (1) radiologic disease progression on first line chemotherapy, (2) unsuitability for first line chemotherapy, (3) prognosis of less than 1 year as estimated by their treating team or (4) high symptom burden (any score of ≥7/10 on the Edmonton Symptom Assessment System Revised (ESAS-r)).
The Canadian Problem Checklist (CPC) is a 21-item comprehensive screening tool which invites patients to identify ‘concerns in the last month’ and includes a single-item question regarding financial worry. 13 This was collected monthly during the first year of the study and every 3 months thereafter, until study conclusion or patient death. Patients who completed at least one CPC were included in this secondary analysis.
Demographic data included age, gender, ethnicity, marital status, household income, accommodation and education status.
Statistical Analysis
CPC responses were coded as 1 if FW was reported in a given month, and 0 otherwise. Data were structured in long format at the person-month level to accommodate repeated measures.
Explanatory variables were selected based on prior literature and theoretical relevance. All were coded as dummy variables. Age (<65 [ref.] vs ≥65) captured employment and retirement status; ethnicity (White vs Non-White [ref.]) addressed financial disparities; household income was categorized as >$75,000 [ref.], $25,000–$75,000, <$25,000, or “prefer not to disclose”.9,14-17 Marital status (married vs not married [ref.]) served as a proxy for social and financial support. 17 Education (high school or less [ref.], college, university) and gender (female vs male [ref.]) reflected socioeconomic and gender-based vulnerabilities.9,14,15 City of residence was modelled using indicators to capture geographic differences in financial strain. 7
Follow-up time was modelled using monthly dummy variables to flexibly capture non-linear changes in financial worry. This approach was preferred over a linear term, as the trajectory was not expected to be uniform. No interaction terms were included, as the focus was on main effects.
Random-effects logistic regression was used to estimate the odds of financial worry over time, accounting for both within- and between-subject variation. The panel structure was defined using xtset with participant ID and month. Analyses were conducted in Stata version 12. The analytic sample included 1246 person-month observations from 131 participants. Person-months with missing outcome data were excluded. Results are presented as adjusted odds ratios (ORs) with 95% confidence intervals (CIs) and P-values. A likelihood-ratio test supported the use of random effects over a pooled model (χ2(1) = 286.18, P < 0.001).
The reporting of this study conforms to the STROBE guidelines for an observational cohort study. 18
Results
Demographics
Descriptive Statistics for Demographic Variables

Longitudinal Financial Worry
Fifty-seven patients (43%) affirmed at least once that they had worried about their finances in the preceding month. Of those, 46 patients (82%) endorsed this question on at least two encounters and 18 (31%) on more than five. Of those who answered ‘no’ at enrolment (n = 115), 43 (37%) subsequently answered ‘yes’. Of the remaining who answered ‘yes’, 14 of 16 (88%) affirmed further episodes of financial worry.
The proportion of patients experiencing financial worry at any given time point fluctuated (see Graph 1), with mean proportion of 18%. Patient-Reported Financial Worry Longitudinally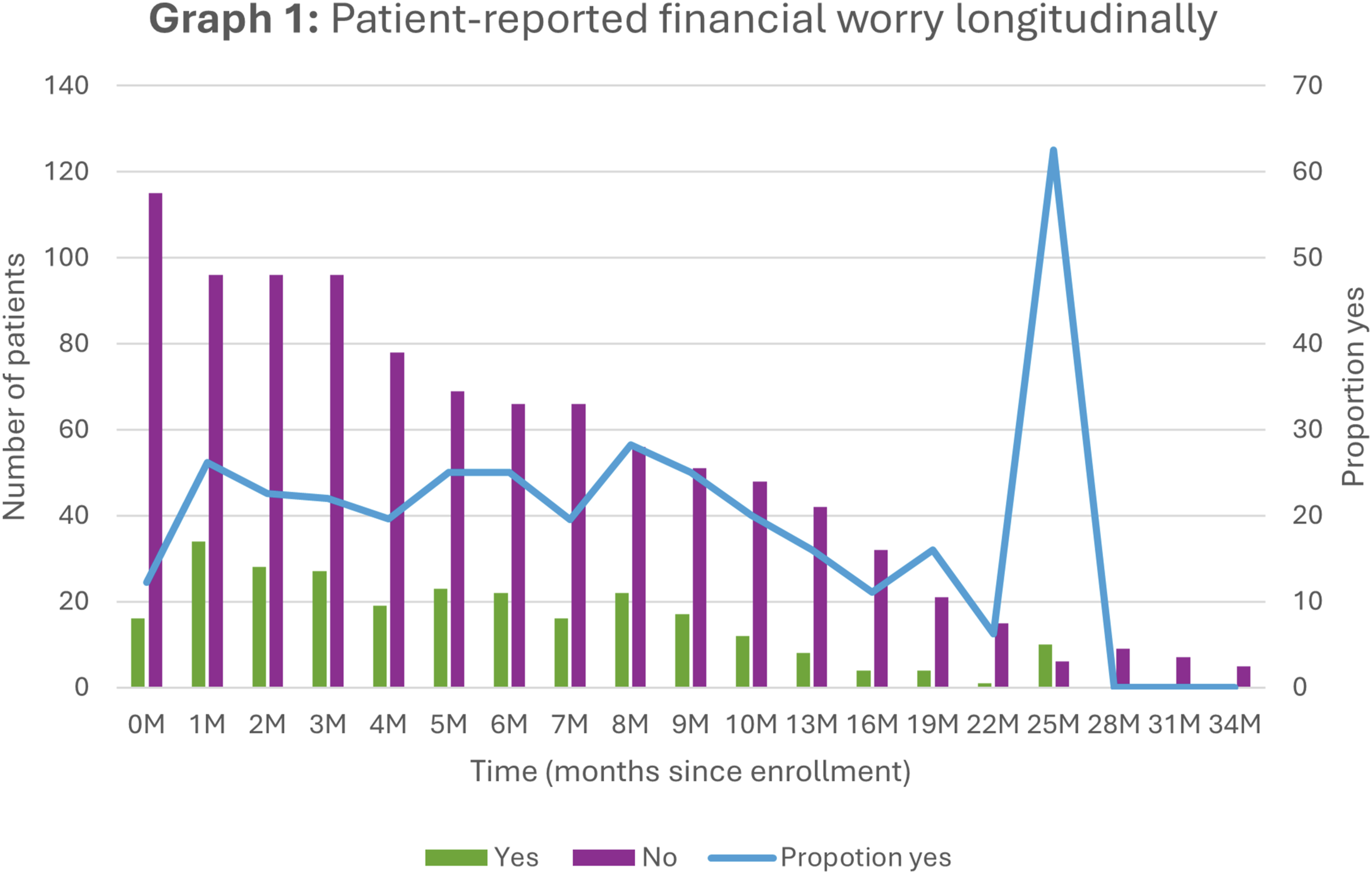
Adjusted Odds Ratios From Multivariable Modelling

aIndicates a statistically significant difference between the explored characteristic value and the reference value (in parentheses) found on multivariable modelling, adjusted for age, ethnicity, income, living status, education, gender, city, and time. The Multivariable analysis included 1246 person-month observations from 131 participants.
Time was modelled using month-specific indicator variables to flexibly capture non-linear changes in financial worry. Compared to baseline (month 0), participants had significantly higher odds of reporting financial worry during several follow-up months. Notable increases were observed at month 1 (aOR = 5.74, 95% CI: 2.39-13.79, P < 0.001), month 2 (aOR = 3.75, 95% CI: 1.54-9.14, P = 0.004), and month 3 (aOR = 3.81, 95% CI: 1.55-9.34, P = 0.004), with additional elevations at months 5, 6, and 8. A pronounced increase was also observed at month 25 (aOR = 19.74, 95% CI: 2.79-139.49, P = 0.003), although this may reflect sparse data.
No formal interaction terms between time and other covariates were included, as the primary focus was on main effects. While some follow-up months showed elevated odds of financial worry, the overall pattern did not suggest a consistent upward or downward trajectory.
Discussion
In this secondary analysis in ambulatory adult patients with advanced colorectal cancer, financial worry was common longitudinally (43%) and often recurrent. Patients who reported financial at enrolment were likely to report further episodes (88%), however, many patients (37%) developed financial worry during follow-up.
What this study adds
Financial worry is common and often persistent even within a publicly funded healthcare system. The presence of persisting or new worry suggests that either recognition of this concern, or the supportive interventions, were not available, not adequate, or that new financial pressures arose for an individual over time. The application of these findings will need to consider the local context of healthcare structures and financial supports available to patients. In Alberta, Canada, the Canadian Problem Checklist was used in routine screening but without a protocolised referral pathway. Social workers are part of the multidisciplinary palliative care team, but referrals are ad hoc based on perceived need. Within Canada, there are province-level differences in screening practices and multi-disciplinary team access.
Compared to other studies in both early and advanced CRC that had similar demographics in age and ethnicity, this cohort reported overall lower proportions of financial worry at a given timepoint (mean 18%).10,19
The findings suggest fluctuations over time rather than a sustained change in financial worry. Therefore, comparisons to studies reporting declining trends in early-stage cancer populations should be interpreted with caution. 20 The apparent peak at 25 months post-enrolment is difficult to interpret given the small patient numbers, however, at an individual level escalating worry as death approaches could worry about costs related to healthcare, after-death expenses like funeral planning, or worry about a diminished financial legacy for loved ones.
The multivariable analysis revealed no association between rates of financial worry and socioeconomic status as measured by overall household income or education. It may be that in advanced CRC, financial worry encompasses concerns for dependents and aspects of identity or personal legacy independent of absolute income. This paper again found that younger age (<65) is associated with financial worry, maybe because of less time in the workforce to accumulate wealth. 15
The high proportion of patients who preferred not to disclose their household income may indicate they regard finances as a private matter and may not recognise their clinicians as a resource for assistance. 21 Sensitive, serial screening initiated by healthcare providers may support disclosure. Social workers may be ideally placed, and preferred by patients, to undertake this. 22 This could prompt further assessment with more detailed, time-consuming, validated tools like COST and P-SAFE, and targeted referral to supportive services.6,16
Strengths/Limitations
The key strength of this study is the long duration of study to assess the longitudinal experience of financial worry.
The primary limitations of this secondary analysis are the small patient numbers and limited racial diversity of the cohort. There was significant attrition in survey completion, especially after 10 months, influenced by a significant proportion of patient who died during the study period (72%).
A second validated survey of financial burden (P-SAFE) was not added to routine survey collection until later in the study. A significantly smaller number of patients completed the P-SAFE survey, and therefore this could not serve as a benchmark for validation. 23
Conclusion
This paper contributes to the compelling evidence that many patients with cancer may have financial concerns, including those in the palliative phase of their illness. We recommend the inclusion of a single-item screening tool at regular intervals for all patients with malignancy. The incorporation of a financial questionnaire into the Edmonton Symptom Assessment System Financial-Spiritual (ESAS-FS) is encouraging progress. 24 In addition to routine screening, policies must be developed that support patients and their families during all phases of cancer treatment. 7
Footnotes
Ethical Consideration
Ethics approval was obtained from the Health Research Ethics Board of Alberta Cancer Committee (HREBA-CC), study ID HREBA.CC-17-0429, on November 22nd, 2017. All participants provided written, informed consent prior to enrolment in the study. All patient data have been de-identified.
Author Contributions
JS and AS were involved in the study design, funding applications, ethics approval and data collection for the original PaCES project. PA conducted the statistical analysis. HDM drafted the manuscript and all authors contributed to data analysis and manuscript revisions.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Canadian Institutes of Health Research Operating Grant: Partnerships for Health System Improvement for Cancer Control (HRC-154127).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data cannot be shared as approval was not sought from the ethics board and the data custodian (Alberta Health Services).