
Abstract
Introduction
Cervical cancer remains a significant cause of morbidity and mortality among women globally, despite the availability of effective prevention tools. The use of self-sampling devices for human papillomavirus (HPV) testing is a promising strategy to increase screening participation, particularly in settings dominated by opportunistic models. Understanding women’s preferences regarding invitation methods and device design is essential to ensure effective and equitable programme implementation. This study explored the expectations, preferences, and perceived barriers of women aged 35 to 65 in the Valencian Community (VC), Spain, in anticipation of launching a population-based cervical screening program.
Methods
A qualitative study was conducted using four face-to-face focus groups involving 29 women, selected from the target population of the screening programme (healthy women aged 35-65 residing in the VC). The session combined an individual assessment (questionnaire and electronic response system of five self-sampling devices) with a structured group discussion. Preferences regarding invitation channels, test communication, and device usability were analyzed through descriptive statistics and thematic content analysis.
Results
Self-sampling was highly accepted, with 96.4% of women stating they would perform it at home. Preferred channels for both invitations and results were SMS and local health centers. Simplicity and ease of use were the key features of the device accepted by the largest number of women—FLOQSwab. Evalyn Brush was also positively valued for its attractive design and was the preferred option for some women. Participants expressed concerns about reliability and proper use, particularly among older women or those with limited body awareness. Familiarity with colorectal screening supported acceptance. Importantly, device selection emerged as a key factor in facilitating participation. The integration of digital technologies (SMS, health apps) was positively valued as a means of increasing accessibility, improving communication, and supporting equity in outreach efforts.
Conclusion
Self-sampling is a feasible and widely accepted strategy for cervical cancer screening. Effective implementation requires validated devices, culturally adapted information campaigns, and digital engagement tools to maximize participation and reduce inequalities.
Plain Language Summary
Cervical cancer can often be prevented with regular screening tests. However, in many places, only women who go to the doctor on their own get tested. This limits how many women are protected.
This study looked at a new way to improve participation in cervical cancer screening. It explored what women think about using self-sampling devices (tools that allow women to collect their own samples for HPV testing at home). Researchers wanted to understand which devices women prefer and how they feel about getting invited to screening using digital tools like text messages or health apps.
The study included 29 women aged 35 to 65 in the Valencian Community, Spain. They saw five different self-sampling devices and shared their opinions in group discussions. Most women (96%) said they would use self-sampling at home. They preferred simple devices that were easy to use. They also liked being contacted by SMS and having the option to return the sample to a health center.
Some women had concerns about doing the test correctly and missing a chance to talk to a doctor. Others felt confident and said it reminded them of the home test for colon cancer.
This study shows that self-sampling is well accepted and can help reach more women. Choosing the right device and using modern communication tools may increase screening and reduce health inequalities.
Introduction
Cervical cancer ranks as the fourth most common cancer among women worldwide in both incidence and mortality. According to estimates from the International Agency for Research on Cancer (IARC), the global mortality rate in 2020 was 8.8 per 100,000 women per year. 1 In most cases, cervical cancer is caused by persistent infection with high-risk human papillomavirus (HPV) types. Cervical carcinogenesis is a slow, progressive process involving multiple genetic and morphological changes in the epithelial cells of the cervix, which allows for the early detection and treatment of precancerous lesions, thereby preventing invasive cancer.
In 2018, the World Health Organization (WHO) issued a global call to action for the elimination of cervical cancer, setting the goal that by 2030, 70% of women over the age of 35 should have access to screening tests. 2 In line with this strategy, the European Commission has emphasized that cervical cancer screening should be conducted within the framework of structured, population-based programs.3-5 Such programs involve an organized and integrated health system approach in which all activities are planned, coordinated, monitored, and evaluated within a framework of continuous quality improvement. To ensure effectiveness and equity, it is essential to actively invite the entire target population and to implement outreach strategies specifically designed for socioeconomically disadvantaged groups.
Despite these recommendations, opportunistic screening models still predominate in many countries, where women are not actively invited and must seek testing on their own initiative.6-9 This approach limits population coverage and reduces the overall impact of screening efforts. At the same time, a major technological shift has occurred in recent years, with HPV detection becoming the preferred primary screening method. 10 This shift has been accompanied by the development of self-sampling devices, which allow women to collect their own samples for HPV testing at home. The effectiveness of self-sampling has been well documented,11-15 and the WHO now recommends it as a valid option for cervical cancer screening.2,16
Self-sampling has the potential to increase participation in screening programmes, particularly among women who face access barriers or have limited engagement with healthcare services. Several studies have reported high levels of acceptance.17-21 While the use of self-sampling for HPV detection is widely studied and generally well accepted, preferences among the different types of devices (eg, swab, brush, lavage-based) vary across populations and contexts. Several studies have compared usability and acceptability of different devices, highlighting that comfort, ease of use, and familiarity influence women’s preferences.21-24 However, further research is still needed to guide device selection in specific implementation contexts. Device format, appearance, and mode of use can significantly influence participation, making it essential to investigate women’s preferences and perceptions.
Countries today face the dual challenge of transitioning from opportunistic models to population-based screening programs and, simultaneously, incorporating HPV testing as the primary method. Implementation varies widely: some countries have already adopted organized screening programs, many using HPV as the primary test, and several have incorporated self-sampling through various strategies.6,8,25,26 In this context, self-sampling is viewed as a key tool for achieving WHO targets and ensuring effective screening coverage worldwide.
In parallel, the use of new digital technologies—such as mobile applications and social media—offers a promising opportunity to enhance outreach and engagement with the target population. These tools are increasingly being used for invitation, information, and follow-up purposes and have shown potential to improve participation in population-based screening programs.27,28
In Spain, the Ministry of Health established the implementation of cervical cancer screening in 2006 and later revised the criteria through various regulations. Program organization is delegated to the autonomous communities, where most programs have followed an opportunistic model based on cytology as the primary test. In 2019, following European recommendations, the Ministry mandated the implementation of population-based screening programs nationwide, designating HPV testing as the primary strategy for women aged 35 to 65. 29 However, the level of implementation varies among regions. In the Valencian Community (VC), where opportunistic screening has been in place since 1995, current regulations have promoted the inclusion of HPV testing for women aged 30 to 65, performed by healthcare professionals, and complemented with reflex cytology and colposcopy if needed. A transition toward a fully organized program is currently underway, including consideration of self-sampling devices, as in other regions.30,31
To ensure the success of these programs, achieving high coverage and participation rates is essential. Strategies must be tailored to the cultural, social, and organizational characteristics of each region. 32 Population-specific factors, as well as program-level elements—such as the type of test, invitation methods, and communication channels—have a direct influence on outcomes. 33 Understanding in depth the preferences, expectations, barriers, and concerns of the target population regarding different screening approaches is a critical step in ensuring effective and equitable implementation. 34
Objective
Given the imminent implementation of a population-based cervical cancer screening program in the Valencian Community, this study aimed to explore women’s expectations, preferences, and perceived challenges regarding different invitation methods, outreach strategies, and self-sampling devices for HPV detection through a qualitative approach. The ultimate goal was to identify key elements that may inform the design of interventions to maximize participation in the forthcoming population-based prevention program.
Materials and Methods
Design
A qualitative study based on expected utility theory techniques was conducted based on the focus group technique. It was conducted in two consecutive steps within a single 120-min face-to-face session, with four groups participating simultaneously.
Sessions were moderated by JM and MG (PhD and MPH), both with over 20 years of experience in qualitative research. Before the sessions, participants received informed consent documents and authorization for audio recording, ensuring anonymity and confidentiality at all times. The study was conducted in meeting rooms at a healthcare education center, and some authors attending as observers. There was no prior relationship between the researchers and the study participants. Recruitment continued until the target sample size was reached.
The researchers carried out the study following a predefined and approved discussion guide, which included all relevant topics and had been previously reviewed by the research team. All methods of the study were performed in accordance with the Declaration of Helsinki, and the study was approved by the Committee of Ethics and Research Integrity of Miguel Hernández University of Elche (reference no. AUT.DPS.JMS.01.21, date 30/09/2021). The reporting of this study conforms to the COREQ guidelines. 35
Participants
The number of women participating in the study was determined based on the minimum required for the formation of the qualitative technique used, set between 8 and 9 participants per group, with a total of 29 women. For the composition of each group, efforts were made to ensure representativeness in terms of age, education level, and employment status, creating mirror groups to maintain comparability.
Participants were recruited by phone through women’s associations using snowball sampling. Women were selected from the target population of the screening programme, specifically healthy women aged 35-65 years residing in the VC, and the sampling aimed to ensure ethnic diversity. Recruitment continued until the target sample size was reached. Of 61 women contacted, 29 agreed to participate. The most common reason for non-participation was lack of time.
Description of Interventions and Content
First step
The first part of the session included a presentation of the proposed cervical cancer screening program using a draft version of the official informational leaflet. This document contained details about the screening process and proposed a model based on self-sampling devices as a screening method for women aged 35 to 65 years. The proposed protocol outlined in the information leaflet involved mailing self-sampling kits to women’s homes, sample drop-off at health centers, and result communication via postal mail. Afterward, participants completed a written questionnaire that included questions about their previous participation in cervical cancer screening and their knowledge of other screening programs. The questionnaire included multiple-choice questions on communication preferences, result delivery methods, and preferred sample drop-off locations. Finally, they were asked about their willingness to participate in the program if self-sampling were offered as a testing option.
Later in the first step, five models of self-sampling devices were distributed to the participants. The tests evaluated in this study were (Figure 1): (Device A) FLOQSwabs® 552C.80 (Copan Diagnostica Inc), (Device B) Evalyn® Brush (Rovers Medical, (Device C) Aptima Multitest Swab® (Hologic), (Device D) IUNETEST® (Self Test Technologies, S.L.), (Device E) Qvintip® (Aprovix). The selection of the tests evaluated in this study considered their previous use in screening programs and their ease of use. Upon distribution, researchers provided instructions based on the manufacturer’s guidelines. Participants then responded in their workbooks to two specific questions: whether they considered the device easy to use and whether they would use it at home, along with an open-ended question to explain their assessment. Self Sampling Devices AssessedNote (Device A) FLOQSwabs is a plastic swab with a rounded tip made of nylon fibers, which must be removed from the tube containing it by rotation, inserted into the vagina up to the indicative line and reintroduced into the tube; (Device B) EvalynBrush is a plastic device, with a brush at one end and a plunger at the other end, with a cap. It must be inserted up to the side wings, rotate the plunger 5 times and put the lid on; (Device C) Aptima Multitest Swab consists of a cardboard swab with a rounded cotton tip and a tube with a liquid medium. After inserting the swab into the vagina up to the indicative line, it must be inserted into the liquid medium and broken to leave the tip inside; (Device D) IUNETEST is a plastic tube with a cap at one end and a rotary plunger at the other. To use it, it must be inserted, the plunger pushed and rotated, and finally the lid is placed; (Device E) Qvintip contains a test tube and a wand with a hooked tip at one end. For use, after inserting and rotating the wand in the vagina, the plastic tip must be inserted into the tube, resting on its walls to unhook it of the wand and leave it inside.
After completing the questionnaire, a comparative ranking was conducted using the audience response system. Participants selected the device they found easiest to use, most trustworthy, and most comfortable. They also identified the best and worst devices overall and ranked their top three preferences.
This initial evaluation provided key insights, which were further explored during the group interview phase.
Second step
The second step used a structured group discussion to confirm observed trends and identify any emerging themes not addressed during the individual assessment. Participants discussed the screening program design, content of the leaflet, and impressions of the self-sampling devices.
During the structured discussion, participants debated the new screening program, the content of the informational leaflet, and the self-sampling devices. Data triangulation was applied to identify patterns across groups, analyzing both convergence and divergence of opinions. Discussions concluded when thematic saturation was reached.
Analysis
A descriptive analysis was performed on the multiple-choice and closed-ended questionnaire responses and voting data, calculating frequencies and percentages using Microsoft Excel.
For the open-ended question on device evaluation, responses were categorized into positive and negative assessments for each device to facilitate comparison.
Qualitative data from the group discussions were transcribed and analyzed by identifying and categorizing distinct ideas into mutually exclusive categories. Two researchers independently coded the responses; discrepancies were resolved by a third researcher to reach consensus. The number of participants who independently raised each idea was also documented to estimate relevance and recurrence.
No feedback sessions were conducted to share the results with participants.
Results
A total of 29 women participated in the study, with a mean age of 50.3 years. In terms of educational level, 44.8% had a university degree, 27.6% had vocational training, and the remainder had completed compulsory secondary education. A large majority (96.6%, n = 28) had previously undergone a Pap smear, and 86.2% (n = 25) reported doing so every 3 years or less. In addition, 79.3% (n = 23) were aware of other cancer prevention programs, such as breast or colorectal screening.
First Step: Questionnaire and Audience Response System
Regarding the proposed cervical cancer screening program, 86.2% of participants indicated that health centers were their preferred source of information. When asked about their preferred method for receiving the screening invitation, SMS (58.6%) and postal letters (48.3%) were the most selected. Similarly, SMS was preferred for receiving test results (65.5%), followed by postal mail (37.9%). Health centers were also the preferred location for returning the self-sampling kits (86.2%). If the self-sampling method were offered as part of the screening program, 96.4% of participants stated they would be willing to use it (Figure 2). Preferences Relating to Different General Aspects of the Screening Program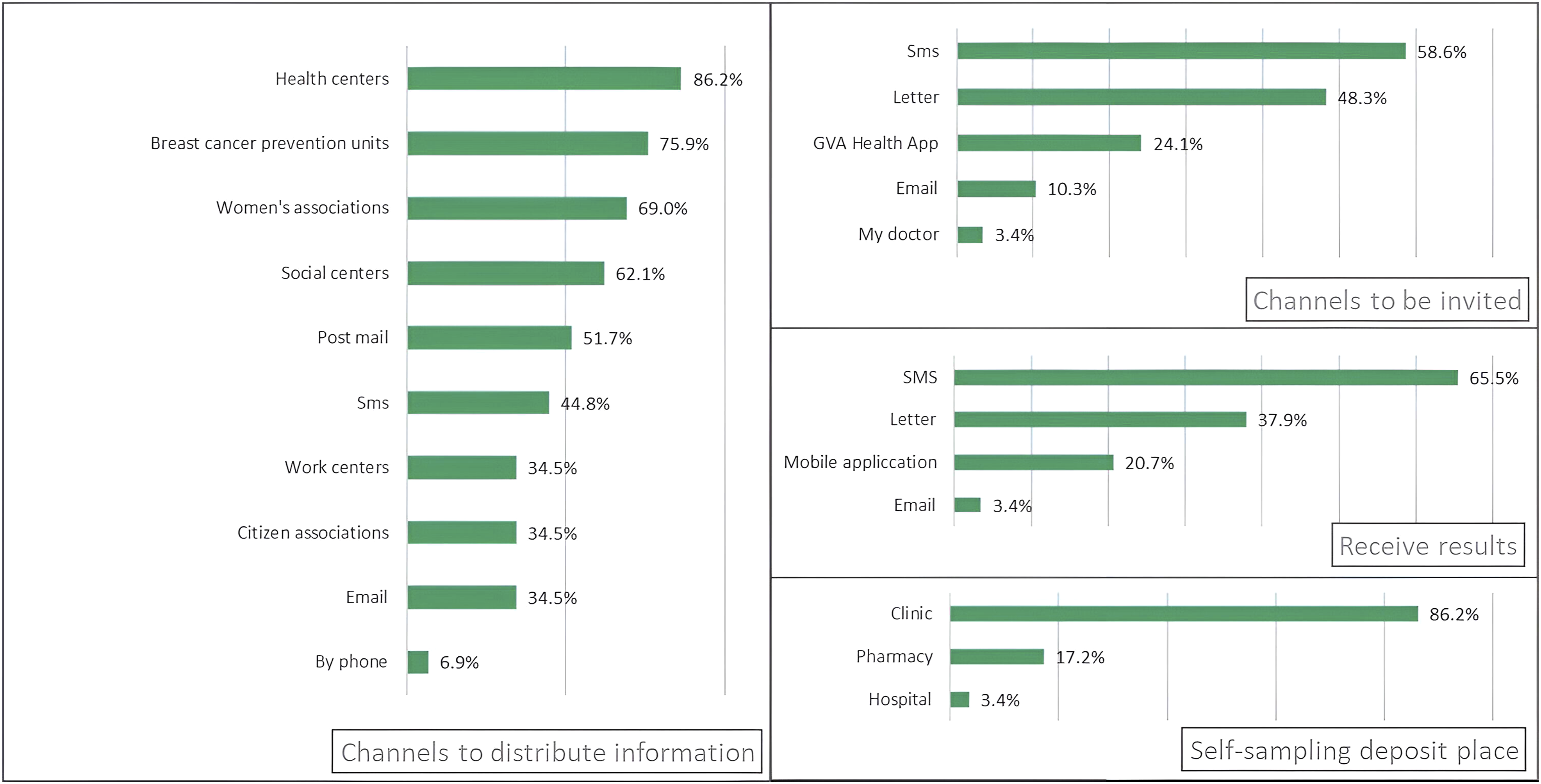
In the closed-ended questions assessing the devices, Device A was considered the easiest to use by the majority of participants (93.1%). Devices A and D were the most accepted for home use, both with an acceptance rate of 75.9% (Figure 3). Results of the Individualized Assessment of Devices according to Ease of use and their Acceptance for use at Home
Positive and Negative Evaluations of the Self-Sampling Devices Collected from the Open-Ended Question

Among the negative aspects, Device C was the most criticized, mainly for being difficult to use or manipulate (9 mentions). Discomfort was reported for Devices D and E (5 mentions each). In Device E, 7 women perceived a high risk of sample contamination due to the handling method. Additionally, Device A was considered fragile by 5 participants. Device C accumulated the highest number of negative remarks (24 in total).
In the comparative evaluation using the audience response system, Device A was rated highest for ease of use (52.38%), while Device B received the highest ratings for perceived trustworthiness (51.72%) and comfort (35.71%). Device B was the most liked overall (31.03%), whereas Device C was rated the lowest (28.57%) (Figure 4). Regarding the top three preferred devices for performing self-sampling at home, Devices A, B, and D received the most votes (22, 20, and 18, respectively). Devices C and E were selected by 13 and 11 women, respectively (data not shown in figures). Results of the Selection of a Device for its Greater Ease, Reliability, Comfort and More and less Appreciated
Second Step: Structured Group Discussion
Finally, ideas that came up in the group session revealed many positive attitudes towards a new screening program based on self-sampling devices (n = 9). The existence of another screening programme based on a self-sampling device (fecal occult blood screening devices used in the colorectal cancer prevention program) is seen as an opportunity (n = 3). Some verbatim examples are as follows: If you can take the self-sample test for the colon cancer prevention programme, you can do this one, too. I think it's great that everyone takes their own sample. We’re already familiar with the colon cancer program...or know someone that has taken part... I think it will be much easier to implement the cervical cancer prevention programme
The convenience of performing the test at home was highlighted, especially regarding speed and ease (n = 1), as well as its potential to reach vulnerable populations (n = 2): People of different ethnicities or races will have a better chance of being screened. It can reach more people and free up in-person appointments. You don't have to wait, because sometimes you can’t be bothered to go to the gynecologist to get it done.
They believed that this program will be accepted, on the one hand, due to women’s increased awareness of screening (n = 2) and, on the other hand, because they consider that people will eventually adapt to the new measures (n = 1).
Ideas were provided for improving the content of the message in information leaflets or possible campaigns, showing the need for a stronger message (n = 6): Include information on mortality, Be more forceful messaging.
Concerns were raised regarding the reliability of the self-sampling process (n = 4), including doubts about proper technique and accuracy: Maybe we won't do the test correctly and the results aren’t right. Questions about precision: how many centimeters it should be, counting the turns, etc. Uncertainty of not going to a clinic/hospital and not noticing any other illnesses or mistakes with self-sampling.
The feeling of a lack of protection for certain age groups or groups that might not be able to use the self-sampling device due to a lack of knowledge about their own bodies also generated uncertainty. Here are some verbatim statements: Feeling of lack of protection and information for older people”, “due to their age, they prefer traditional screening. Many women do not have sufficient knowledge of their own bodies to do this themselves.
Verbatim Statements Provided in the Group Session to Assess the Cervical Cancer Screening Programme and Self-Sampling, Grouped by Category

*The figures in brackets represent the number of times the message was mentioned by women.
Discussion
The findings of this study provide key insights for the design and implementation of a population-based cervical cancer screening programme in the VC. The high level of acceptance observed regarding the proposed contact channels—particularly SMS, postal letters, and the regional health app—is consistent with previous studies highlighting the effectiveness of digital technologies in improving health communication, especially following the COVID-19 pandemic.36,37 The use of such channels can significantly contribute to increasing participation and reducing traditional logistical barriers.
Self-sampling was widely accepted among participants, with 96.4% of women willing to perform the test at home if this option were available. This strong acceptance aligns with other studies that emphasize usability, convenience, and device design as key factors for adoption.21,23,24,38
The present study revealed notable differences in acceptance between the various self-sampling devices, attributable to both functional and aesthetic factors. Devices perceived as more complex or difficult to handle, such as Qvintip or Aptima Multitest Swab, were more frequently rejected due to perceived difficulties in use and discomfort during insertion. In contrast, devices offering a simple and ergonomic design—such as the swab-type FLOQSwab—were most highly rated, consistent with previous studies that identify simplicity as a key determinant of acceptability. 24
Evalyn Brush, in turn, was positively evaluated for its visually appealing design, which some women interpreted as a product specifically developed for self-collection. Its color, shape, and overall presentation inspired greater confidence. These findings reinforce the idea that not only functionality but also aesthetics and subjective perceptions influence women’s preferences.
While some studies, such as that by Di Gennaro et al, 39 found no significant differences in acceptance by device type, these discrepancies may be explained by cultural, educational, or sociodemographic factors that shape user experience. For this reason, pilot studies prior to large-scale implementation, as recommended by Arbyn et al 40 are essential to identify the most suitable device for each population context.
Nevertheless, some women expressed concerns regarding the reliability of the procedure and their ability to perform it correctly, particularly those with limited body awareness or older age. This perceived lack of confidence has also been documented in the literature and should be addressed through clear and accessible educational campaigns that build trust in the method and provide simple, comprehensible instructions for self-sampling.17,22,41,42
In addition to these technical concerns, some participants reported feeling unprotected due to the absence of a face-to-face clinical consultation, as is traditionally associated with opportunistic screening. This perception should be considered when designing communication strategies and could be addressed through messaging that reinforces the reliability and preventive benefits of the procedure, while emphasizing the importance of professional support when needed.
It is also worth noting that some women drew positive parallels with the colorectal cancer screening program, suggesting that familiarity with similar self-sampling models may facilitate the acceptance of this approach. Such comparisons could prove useful in awareness campaigns, helping to normalize the process.
Finally, and with a view to implementation, this self-sampling-based screening model must ensure adherence to the fundamental principles of population screening programmes: the use of validated tests, continuous outcome monitoring, and a robust follow-up system for women testing positive for high-risk HPV.43,44 In addition to the well-established need for HPV test validation, 45 it will also be necessary to validate the devices used, along with technical aspects such as transport media, dilution, sample stability and preservation time, and compatibility with molecular amplification platforms. Several technical sources have noted that these parameters may directly affect the sensitivity and specificity of the method and must be carefully adjusted and validated prior to large-scale implementation.43,46,47
Unlike most studies that have explored self-sampling as a strategy targeting only non-attending women, this study examines its acceptability within the entire target population. This provides novel evidence to support its integration as a primary screening modality within population-based programs. This approach has already been adopted in countries such as the Netherlands and Australia, where self-sampling is offered as a first-line option within the national cervical screening program.48,49 This perspective allows for a broader strategic approach to screening, promoting more accessible, equitable, and sustainable models aimed at maximizing participation across all social groups.
Limitations
This study presents certain limitations that should be considered when interpreting the findings. Firstly, the use of convenience sampling may have introduced selection bias, with an overrepresentation of women with higher educational attainment. This sample composition limits the generalizability of the results to the entire target population, particularly to subgroups with lower educational levels or greater social vulnerability.
Secondly, although participants handled the self-sampling devices and received detailed instructions regarding their use, they did not perform the self-sampling in real-life conditions. This limitation may have influenced their assessment of aspects such as perceived usability, confidence in the procedure, and overall comfort.
Thirdly, the study design was purely qualitative and did not include a quantitative component or statistical comparisons between devices. Incorporating such analyses in future research, with larger and more representative samples, could allow for methodologically rigorous comparisons and strengthen the generalizability of the findings.
Despite these limitations, the qualitative design employed allowed for an in-depth exploration of women’s perceptions, attitudes, and barriers related to self-sampling in cervical cancer screening. This approach provided a rich and nuanced understanding of the phenomenon, highlighting contextual and subjective factors essential for developing culturally sensitive and population-adapted strategies. Identifying the key determinants of acceptance and understanding contributes valuable insights to the preparatory phases of program implementation and supports more effective and equitable planning.
Conclusions
This study provides relevant evidence on women’s preferences, perceptions, and barriers regarding different self-sampling devices and invitation strategies for cervical cancer screening. The high level of acceptance of the method, along with the clear preference for simple and comfortable devices, reinforces its viability as a strategy to increase participation in population-based programs.
However, the diversity of opinions expressed and the persistence of certain concerns underscore the need to accompany the implementation of these programs with clear, culturally and linguistically adapted informational and educational campaigns that foster trust and minimize health inequalities.
Moreover, the study highlights significant variation in the perceived acceptability of the different self-sampling formats, underscoring the importance of considering both functional and perceptual aspects in device selection. This choice should be guided by criteria such as acceptability, ease of use, and perceived safety by the target population.
Familiarity with other screening programs involving self-sampling, as well as the acceptance of digital communication channels, further strengthens the feasibility of implementing this model. The broad acceptance observed across the general target population—beyond non-responders—offers novel evidence supporting the consideration of self-sampling as a primary screening modality, consistent with experiences already adopted in countries such as Australia and the Netherlands.
Its integration, however, will require the technical validation of the devices, appropriate adjustment of sample transport and storage conditions, and the training of healthcare professionals to ensure proper implementation. In addition to usability and acceptance, cost considerations may also influence device selection, as some options may be less expensive and therefore more attractive to the health system.
Ultimately, this study contributes to the design of more inclusive and sustainable strategies, providing insights to reduce health inequalities and advance towards more accessible, efficient, and user-centered models of population-based cervical cancer screening.
Footnotes
Acknowledgements
The authors would like to thank all the women that participated in the study for their time and contributions.
Ethical Consideration
All methods of the study were performed in accordance with the Declaration of Helsinki and the study was approved by the Committee of Ethics and Research Integrity of Miguel Hernández University of Elche (reference no. AUT.DPS.JMS.01.21, date 30/09/2021).
Informed Consent
Participants were informed and subsequently signed a consent form to participate in the study and agreed to the sessions being audio recorded.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.