
Abstract
Background
Despite Zambia implementing the World Health Organisation's (WHO) tri-pillar cervical cancer prevention goals 90-70-90 Prevent, Screen, and Treat, cervical cancer claims 2000 lives annually and reigns as the most common cancer among women, especially those living with HIV (WLHIV). Our study describes the national uptake of screening and treatment from the ZAMPHIA 2021 survey.
Methods
Utilising a two-stage cluster sampling approach, the study included participants aged 15 years and older across Zambia’s ten provinces. Data were collected on demographic traits, reproductive history, sexual behaviour, and cervical cancer prevention using a structured questionnaire, and HIV was diagnosed from biological samples. Women aged 15-49 were eligible for inclusion in the analysis. The primary outcome of interest was whether a woman self-reported being screened for cervical cancer. Sociodemographic characteristics were calculated for categorical variables using the SAS proc surveyfreq procedure, producing both raw and weighted estimates. The weighted estimates and their variance were generated using jackknife replicate weights for each record.
Results
Of the 8801 surveyed women, 22.2% reported undergoing cervical cancer screening, the majority being aged between 35-49 years. Cervical cancer screening uptake was more likely among compared to HIV negative counterparts (aOR = 3.92, 95% CI: 3.10, 4.95), those aged 25-34 years (aOR = 1.76, 95% CI: 1.42, 2.21) or 35-49 years (aOR = 2.65, 95% CI: 2.11, 3.33) than younger and those with 1-4 (aOR = 2.16, 95% CI: 1.54, 3.02) or more than 5 live births (aOR = 1.98, 95% CI: 1.37, 2.87) than none. Marital status, WLHIV, education, and parity were other factors significantly associated with screening.
Conclusion
We report low cervical cancer screening uptake compared to the 70% target of WHO. The WHO’s call for bolstered strategies and efforts to increase cervical cancer screening and treatment is timely and urgent. Therefore, ongoing messaging and health education among all women is key.
Introduction
Globally, about 350,000 women died from cervical cancer in 2022, with an estimated 660,000 incident cases. 1 Cervical cancer, caused by oncogenic human papillomavirus (HPV), is the most common female cancer in sub-Saharan Africa (SSA), with high morbidity and mortality. 2 Zambia shares a high burden of cervical cancer with an age-standardized incidence rate of 71.5/100000 women years and a mortality rate of 49.4/100000 women years. 1
The World Health Organisation (WHO) has developed a three-pillar strategy; Prevent, Screen, and Treat, to help reduce the incidence of cervical cancer. The aim of this strategy is to have 90% of girls fully vaccinated with the HPV vaccine by age 15 years, 70% of women screened with a high performance screening test by age 35 and again by age 45, and 90% of women with precancers treated and those with invasive cancer managed appropriately. 3 This paper focuses on the achievement of the second pillar within the sample population of women of reproductive age in Zambia.
Cervical cancer is preventable, yet the incidence continues to soar. Many factors contribute to these statistics, such as HIV infection, socioeconomic status, unsafe sex practices and early age of sexual debut. 4 Co-infection with HIV and HPV has shown an increased risk of developing cervical cancer. Women in Zambia carry a disproportionately higher prevalence of HIV than men. For example, the 2021 Zambia Population-based HIV Impact Assessment (ZAMPHIA) survey reports an HIV prevalence of 14% among women of reproductive age compared to 8% among male counterparts of similar ages, 5 similar to the 2016 ZAMPHIA report. 6
Consequently, Zambia has one of the highest age-standardised incidences of cervical cancer attributable to HIV at over 20 per 100000 women, 7 further compounded by the late presentation and delayed diagnosis. 8 Hence, primary prevention methods such as abstinence and vaccination and secondary prevention methods such as screening and treatment of precancers are important. WHO recommends cervical cancer screening for women aged 30-49 years but may start earlier at 25 years in women living with HIV (WLHIV). 9
Despite these efforts, cervical cancer screening uptake remains low in Zambia owing to low levels of knowledge, sociocultural issues, myths and misconceptions 10 that parallel many of the same factors associated with HPV vaccination hesitancy. 11
Understanding the social demographic characteristics of women screening for cervical cancer is important in determining gaps within the country in the dissemination of information concerning cervical cancer prevention. Women of low socioeconomic status are at increased risk of developing cervical cancer worsened by poor health-seeking behaviour. 12
Age is another significant factor that affects the frequency of cervical cancer screening in Africa. Older women are more likely than younger women to engage in screening, partly explained by their increased interaction with health facilities and heightened risk perception.12,13 Additionally, education attainment has been associated with high cervical cancer screening uptake. It contributes to health literacy and enables women to make informed decisions about their health and seek preventive care. 14
Zambia runs a robust cervical cancer screening program offered free of charge in public health facilities across the country’s ten provinces. 4 Cervical cancer screening using visual inspection with acetic acid began in 2006 and is one of the largest programs in SSA. In the formative years of the screening program, it was opportunistic and only based in the capital city, Lusaka, primarily focusing on WLHIV. 4 However, the service has been rolled out nationally to all eligible women regardless of HIV status.
In 2019, cervical cancer screening incorporated HPV DNA testing, primarily targeting WLHIV. By 2021 HPV DNA testing was scaled up to all the country’s ten provinces.15,16 Additionally, in the same year, Zambia rolled out a free national HPV vaccination program targeting 14-year-old adolescent girls 11 and, in 2023, introduced a multiage cohort of 9-14 years. 17
Despite all the measures taken to prevent cervical cancer, the population coverage remains low at 26%. 16 There is a paucity of data on factors associated with cervical cancer screening uptake among Zambian women. Therefore, this study aimed to describe self-reported cervical cancer screening uptake among women of reproductive age participating in a nationally representative sample of the ZAMPHIA 2021 survey.
Methods
Study Design
This was a secondary analysis of data from the ZAMPHIA 2021 population-based survey, whose detailed methods have been previously described elsewhere. 18 Briefly, a two-stage cluster sampling approach was utilised to include individuals aged 15 years and older from the ten provinces of Zambia between April 2021 and December 2021.
Data Collection
Eligible participants were interviewed individually within the confines of their own homes by trained research assistants, utilising Census and Survey Processing System (CSPro) software (US Census Bureau, Washington DC). The questionnaire aimed to gather information pertaining to demographic characteristics, reproduction history, sexual activity, and cervical cancer screening. Participants aged 18 years or older and emancipated minors who provided informed consent were enrolled in the study. Blood samples were collected from all participants for HIV testing using the national algorithm. For minors aged 15-17, parental informed consent followed by the minor’s permission was required for enrolment. Each participant was assigned a unique participant identification number (PTID).
Data Management and Analysis
Women aged 15-49 years were eligible for inclusion in the analysis. The primary outcome of interest was whether a woman self-reported being screened for cervical cancer. If the individual being interviewed in the household was female, they were asked, “Have you ever been tested for cervical cancer?” If they answered yes, they were asked additional questions about the date of the last test, result, treatment and HPV vaccination. All data was deidentified before analysis. Sociodemographic characteristics were calculated for categorical variables using the SAS proc survey-free procedure, producing both raw and weighted estimates. The weighted estimates and their variance were generated using jackknife replicate weights for each record. 5 Categorical variables are presented using counts and proportions.
A multivariable logistic regression analysis using SAS proc surveylogistic was conducted to assess for associations with covariates of interest. HIV status and variables with a Rao-Scott chi-square P-value of ≤0.2 from the bivariate analysis were included in the model. Following the analysis of all women aged 15-49 years, this sample was a subset of those women who tested positive for HIV in the ZAMPHIA 2021 survey to examine associations among women living with HIV. Lastly, among women who had reported being screened for cervical cancer, associations between covariates and reporting abnormal test results were examined using multivariable logistic regression. All data analysis was conducted using SAS v9.4.
Detailed methods, including validation of the questionnaire, are available in the ZAMPHIA Technical Report, which can be found online https://nada.zamstats.gov.zm/index.php/catalog/1/related-materials. 5 This study is reported according to the STROBE checklist for observational studies. 19
Ethics Approval Statement
All methods were carried out in accordance with relevant guidelines and regulations. The study protocol was approved by the University of Zambia Biomedical Research and Ethics Committee in Lusaka, Zambia (UNZABREC Ref. 523-2019) and registered with the Zambia National Health Research Authority (NHRA 0002/30/10/2023). Further approval was sought from the Institutional Review Boards of the University of Maryland, Baltimore (UMB HCR-HP-00089211) and the Centre for Disease Control (CDC #7265, Under Common Rule, Initial approval September 21, 2020).
Results
Socio-Demographic Characteristics of Participants (Women Aged 15-49 Years), N = 8801.
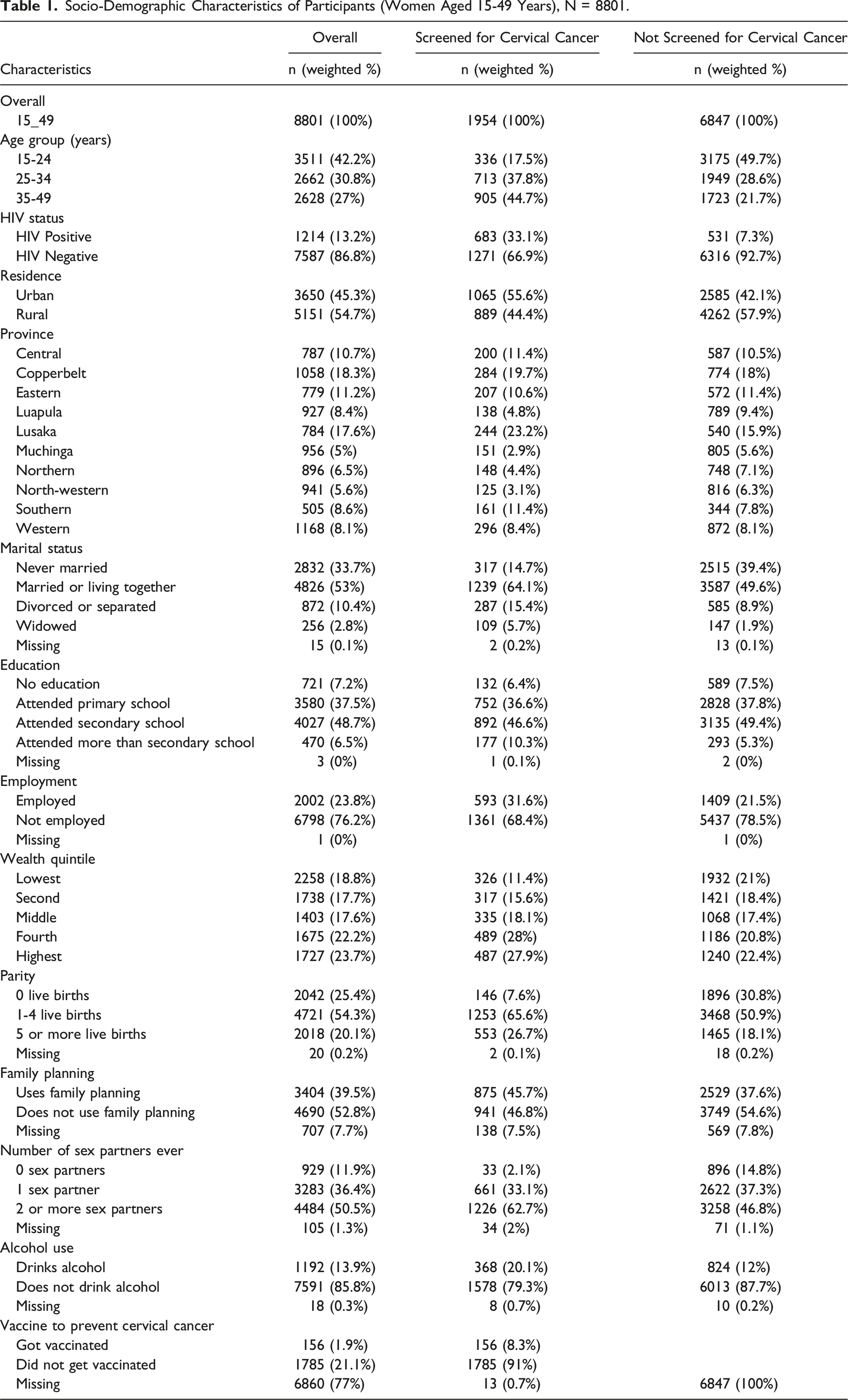
Furthermore, among women who had been screened for cervical cancer, the greatest proportion reported 1.4 live births (1253: 65.6%), reported not using family planning (941: 46.8%), and did not drink alcohol (1578: 79.3%).
Factors Associated with Cervical Cancer Screening Among Women Aged 15-49 Years
Unadjusted and Adjusted Association Between Client Characteristics and Cervical Cancer Screening, N = 8696.

AOR = Adjusted odds ratio, Ref = Reference group, CI = Confidence Interval.
Women aged 25-34 years (aOR = 1.76, 95% CI: 1.42, 2.21) or 35-49 years (aOR = 2.65, 95% CI: 2.11, 3.33) compared to those aged 15-24 years, those married or cohabiting (aOR = 1.6, 95% CI: 1.23,2.09) vs those never married, those who attended secondary school (aOR = 1.50, 95% CI: 1.06, 2.13), attained more than secondary school (aOR = 1.93, 95 CI: 1.17, 3.18) vs those with no education, and those with 1-4 live births (aOR = 2.16, 95% CI: 1.54, 3.02) or more than 5 live births (aOR = 1.98, 95% CI: 1.37, 2.87) vs those with none were significantly more likely to undergo cervical cancer screening. Women living with HIV (aOR = 3.92, 95% CI: 3.10, 4.95) were more likely to screen compared to HIV-negative women.
Conversely, women from the Luapula (aOR = 0.5, 95% CI: 0.31, 0.79) or North-western provinces (aOR = 0.54, 95% CI: 0.31, 0.94) compared to the Central province were significantly less likely to report having been screened for cervical cancer.
Cervical Cancer Screening Among Women Living with HIV Infection
HIV Positive Women 15-49, Unadjusted and Adjusted Associations Between Predictors and Cervical Cancer Screening Uptake N = 1214.

AOR = Adjusted odds ratio, Ref = Reference group, CI = Confidence Interval.
In terms of age, WLHIV aged 25-34 years (aOR = 2.29, 95% CI: 1.29, 4.04) and 35-49 years (aOR = 3.84, 95% CI: 2.10, 7.03) were more likely to screen for cervical cancer than those aged 15-24 years. Similarly, women who were married or cohabitating (aOR = 1.69, 95% CI: 1.05, 2.73) compared to those never married, and those who reported 1 sexual partner (aOR = 26.7, 95% CI: 4.84, 147) or 2 or more sexual partners (aOR = 23.8, 95% CI: 4.58, 124) as compared to none, were more likely to screen for cervical cancer.
In contrast, women residing in rural areas (aOR = 0.58, 95% CI: 0.36, 0.91) compared to urban areas, and those living in Luapula (aOR = 0.29, 95% CI: 0.17, 0.50) or Muchinga (aOR = 0.41, 95% CI: 0.21, 0.80) provinces in comparison to the Central province were less likely to participate in cervical cancer screening.
Discussion
This study sought to describe the uptake of cervical cancer screening among women in their reproductive years and other independent risk factors, using a national representative survey, ZAMPHIA 2021. Among the respondents, 22.2% indicated having undertaken cervical cancer screening, slightly exceeding the 20.7% reported by Nyambe et al, in 2019, whose data was limited to Lusaka province of Zambia, 20 but still falling short of the WHO’s strategy target of 70%. 3
The key determinants associated with the uptake of cervical cancer screening included older age, living with HIV, province of residence, being married or cohabiting, higher level of education and those reporting more live births. When stratified by HIV status, these findings were similar to WLHIV. Those who reported cervical cancer screening were predominantly older, residing in urban areas, married, and had multiple sexual partners.
We found low reported cervical cancer screening uptake, which is comparable to other regional data, such as a recent systematic review and meta-analysis; with a pooled uptake of 12.87%. 21 However, most high income countries such as Finland, 22 the United Kingdom 23 and Australia 24 have much higher cervical cancer screening uptake rates. The low screening uptake found in our analysis could be explained partly by demographics, some cultural norms, and structural barriers.21,25 For example, the use of a speculum for cervical screening is misunderstood to cause more harm than good and its use may be considered a cultural taboo for married women. 10
Additionally, mistrust in some reproductive health-related interventions such as cervical cancer screening may have a negative effect on uptake. Those who trust the health related services are likely to take preventive interventions. For example, a recent study on HPV Vaccination uptake in Zambia, revealed that parents who had screened for cervical cancer were more likely to consent to their daughters’ HPV vaccination. 11 Therefore, ongoing community messaging on the importance of early detection and treatment of cervical cancer, as well as debunking myths, are key strategies for increasing uptake. 26
We found that women older than 35 years were more likely to be screened for cervical cancer compared to younger women. Previous research has also found that older women were more likely to be screened for cervical cancer compared to younger women. 27 This might be due to increased awareness and perception of risk as women age. 28
However, this finding must be further investigated as to why young women shun cervical cancer screening when studies have shown that in Zambia, women less than 35 years old and are HIV positive are likely to have screen-positive results.4,29 One of the plausible reasons could be that cervical cancer is more common and overt in older women 30 hence, their risk perception may be higher.
Targeted interventions and strategies are needed in Zambia to increase the uptake of cervical cancer prevention programs among various age groups.31-33 The implementation of mobile screening programs to reach distant areas, raising awareness through community education campaigns, guaranteeing accessibility, and addressing prevailing cultural attitudes are some of the strategies which can be contextualised.33,34
Women who were married or cohabiting had a higher likelihood of screening for cervical cancer. Male partner support in sexual and reproductive health activities has been associated with good compliance. Similar to a study done in Uganda, women who were supported by their male partners were less likely to be lost to follow-up. 35 This could be due to many patriarchal systems in Africa including Zambia needing male figure approval.
We found that women who were more educated and in the higher wealth quintiles (richer) were more likely to take up cervical cancer screening; this is similar to the findings in the Malawi PHIA survey. 36 The findings seem to be consistent even with research done in developed countries as reported by Murfin et al in their systematic review. 37
In this study, WLHIV were more likely to screen for cervical cancer, which is consistent with earlier studies. A study done in Lusaka earlier found good knowledge levels as well as good practices towards cervical cancer screening among WLHIV. 32 However, a systematic review and meta-analysis on pre-cancerous lesions among WLHIV living in SSA found a high pooled prevalence of 25.6% with other associations such as a history of sexually transmitted infections and multiple sexual partners. 38
The findings could be partly explained by the fact that, WLHIV are more likely to encounter health care facilities for ART resupply, and immunological follow-ups in a set-up where medical doctors have shown good knowledge and attitudes towards cervical cancer prevention measures. 39 Further, all WLHIV are offered a free cervical cancer screening test during these routine hospital visits unless they opt-out.
Limitations
This study is not without limitations. First, this data is self-reported hence subject to recall bias and social desirability. Second, the questions asked in the survey were limited hence unable to collect information on a number of other interpersonal reasons for not screening such as costs of transportation, fear, community beliefs, stigma, presence of symptoms and healthcare-associated factors. Additionally, only women who reported cervical cancer screening were asked about their HPV vaccination status.
However, the data has a strength because it is nationally representative and can be generalised countrywide.
Conclusion
Cervical cancer screening uptake in Zambia remains low generally but higher among older women, more educated, and WLHIV. To address the disparities in cervical cancer screening rates, it is important to implement targeted interventions that address the specific barriers faced by different groups. These may include community awareness campaigns, health education programs, and efforts to improve access to screening services, particularly among younger women, unmarried individuals, HIV negative and those with lower levels of education.
Additionally, engaging with local leaders and influential community members can help challenge cultural norms and promote the importance of screening at all ages. Policy makers are encouraged to formulate policies to support screening services to prevent cervical cancer.
Supplemental Material
Supplemental Material - Self-Reported Cervical Cancer Screening Uptake Among Women of Reproductive Age in Zambia: Evidence from the 2021 Zambia Population-Based HIV Impact Assessment (Zamphia) Survey
Supplemental Material for Self-Reported Cervical Cancer Screening Uptake Among Women of Reproductive Age in Zambia: Evidence from the 2021 Zambia Population-Based HIV Impact Assessment (Zamphia) Survey by Mwansa Ketty Lubeya, Angela Sinyani-Kabunda, Moses Mukosha, Brianna Lindsay, Enock Mulowa Mumbula, Chinedu Agbakwuru, Bwalya Daka, Rebecca G. Nowak, Akipu Ehoche, and Gina Mulundu in Cancer Control.
Supplemental Material
Supplemental Material - Self-Reported Cervical Cancer Screening Uptake Among Women of Reproductive Age in Zambia: Evidence from the 2021 Zambia Population-Based HIV Impact Assessment (Zamphia) Survey
Supplemental Material for Self-Reported Cervical Cancer Screening Uptake Among Women of Reproductive Age in Zambia: Evidence from the 2021 Zambia Population-Based HIV Impact Assessment (Zamphia) Survey by Mwansa Ketty Lubeya, Angela Sinyani-Kabunda, Moses Mukosha, Brianna Lindsay, Enock Mulowa Mumbula, Chinedu Agbakwuru, Bwalya Daka, Rebecca G. Nowak, Akipu Ehoche, and Gina Mulundu in Cancer Control.
Footnotes
Acknowledgments
We would like to acknowledge the Ministry of Health for the opportunity to use this data and all the study participants.
Author Contributions
MKL: Conceptualisation, data curation, Initial draft manuscript writing, supervision ASK: Conceptualisation, draft manuscript writing, MM: Conceptualisation, draft manuscript writing, BL: data analysis, draft manuscript writing, EM & BD: draft manuscript writing, CA: draft manuscript writing RN: draft manuscript writing, AE: data analysis, draft manuscript writing, GM: Conceptualisation, data curation, draft manuscript writing, Supervision. All authors read the final manuscript and approved it for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is supported by the President’s Emergency Plan for AIDS Relief (PEPFAR) through the Centers for Disease Control and Prevention (CDC) through a cooperative agreement (#U2GGH002172) with the University of Maryland, Baltimore.
Authorship Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the funding agency.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.