
Abstract
Introduction
Prostate cancer death rates in the U.S. and in South Carolina (SC) are twice as high among Black men as they are among White men. In response, the Medical University of SC Hollings Cancer Center developed the SC Prostate Cancer Education and Navigation to Screening Program for African American Men (SC AMEN Program).
Methods
The SC AMEN Program included a one-hour, evidence-based prostate cancer educational session. To recruit participants, the investigators employed a convenience sample strategy, in which community champions volunteered to host the SC AMEN sessions in trusted community venues and recruited the participants for each session. A pre-test survey assessed prostate cancer knowledge using the validated PROCASE Knowledge Index. A post-test survey was administered following the educational session, after which participants were navigated by telephone over the next three months to schedule an appointment to discuss prostate cancer screening with a clinician.
Results
The 568 participants included Black (97.0%), American Indian/Alaska Native (0.9%), Asian (0.2%), Native Hawaiian or Other Pacific Islander (0.2%), and White (0.2%) men, with 3.0% reporting Hispanic/Latino ethnicity. Age ranged from 40-69 years; 7.6% had less than a high school education, 35.7% completed high school, 18.1% completed some college, and 36.3% were college graduates. In the multivariable model, controlling for age, insurance status, and educational level, no statistically significant difference in the change in prostate cancer knowledge scores from pre-test to post-test was observed. Among the 568 SC AMEN Program participants, 475 participants (83.6%) either completed a prostate cancer screening (n = 266; 46.8%) or have scheduled a screening appointment (n = 209; 36.8%). The remaining 24 participants (4.2%) continue to be navigated to a screening appointment, and 69 (12.2%) have refused navigation.
Conclusion
The SC AMEN Program fostered the study participants’ appointments with a clinician to discuss their prostate cancer risk and need for screening.
Plain Language Summary
Black men are twice as likely to die of prostate cancer than White men. This is true both in the U.S. and in South Carolina (SC). To address this issue, the Medical University of South Carolina Hollings Cancer Center developed the SC Prostate Cancer Education and Navigation to Screening Program for African American Men (SC AMEN Program). The program is a community-engaged, statewide initiative. In the SC AMEN Program, community leaders recruited other Black men to the program. This recruitment method led to greater trust in the SC AMEN Program team. The one-hour educational sessions took place in trusted community venues, such as churches and community centers. At the start of each session, the SC AMEN Program team thanked the men for participating and for everything they do to support their families and communities. Then, a baseline survey was administered to assess each participant’s level of prostate cancer knowledge. At the end of each session, participants completed a post-test and received a $50 gift card. A patient navigator was assigned to each participant and called him for the next three months to help guide him to a clinical appointment where he could discuss prostate cancer screening with a clinician. After the three-month assessment, each participant received another $50 gift card. The results show that among the 568 SC AMEN Program participants, there were no significant increases in prostate cancer knowledge from pre-test to post-test. However, 475 participants (83.6%) either completed a prostate cancer screening (n = 266; 46.8%) or scheduled a screening appointment (n = 209; 36.8%). The remaining 24 participants (4.2%) continue to be navigated to a screening appointment, and 69 (12.2%) have refused navigation. The SC AMEN Program seemed to be effective in helping Black men to talk with a clinician about their prostate cancer risk and the need for screening.
Introduction
Prostate cancer is the most common cancer diagnosis among men and is the second highest cause of cancer death among men in the United States (U.S.). 1 It is estimated that in 2025, there will be 313 780 new diagnoses of prostate cancer in the U.S., with an estimated 35 770 prostate cancer deaths. 1
The U.S. has stark racial disparities in prostate cancer incidence and mortality. The prostate cancer incidence rate was 70% higher for Black men than for White men in South Carolina from 2017-2021.
2
Black men are 2.1 times more likely to die from prostate cancer compared to White men. Black men typically are diagnosed at more advanced stages and with higher prostate-specific antigen (PSA) levels at presentation compared to any other racial group.
3
These racial disparities in prostate cancer incidence and mortality are also seen in South Carolina, as displayed in Figures 1 and 2.
2
Prostate Cancer Incidence Rates by Race, South Carolina, 2017-2021 Prostate Cancer Mortality Rates by Race, South Carolina, 2017-2021

Low Prostate Cancer Screening Rates in South Carolina
Despite Black men experiencing higher prostate cancer incidence and mortality rates, PSA screening prevalence is lower when compared to White men in South Carolina from 2019-2020, as shown in Figure 3.
4
Prostate cancer screening rates in South Carolina are low and decreased from 46% in 2014 to 32.8% in 2020.
5
If this downward trajectory continues to occur, the prostate cancer death rates in South Carolina will continue to rise. Prevalence of PSA Test Within Last Two Years for Men Aged 40+ Years by Race, South Carolina, 2019-2020
To address the disparities in prostate cancer mortality and improve screening rates, the South Carolina Prostate Cancer Education and Navigation to Screening Program for African American Men (SC AMEN Program) was developed in 2021 by the Medical University of South Carolina Hollings Cancer Center. The goal of the SC AMEN Program was to increase the number of Black men in South Carolina, ages 40-69 years, who received prostate cancer screening in accordance with current evidence-based prostate cancer screening guidelines. The American Cancer Society guidelines 6 state that men who are at high risk of prostate cancer, such as Black men, should be screened annually or every 2 years starting at the age of 45 years, depending on the results.
The SC AMEN Program included a one-hour prostate cancer educational session followed by coordination with a navigator to address barriers to receiving prostate cancer screening for the three-month period following the educational session. The SC AMEN Program is funded by the TD Charitable Foundation.
Catchment Area
The catchment area of the SC AMEN Program was the entire state of South Carolina. In 2024, the population of South Carolina was 5.48 million people. 7 Twenty-six percent of the population is Black, 69.0% is White, and 2.7% are other racial groups (ie, Asian American, American Indian/Alaska Native, or Native Hawaiian/Other Pacific Islander). 7 The percentage of the South Carolina population living in poverty in 2024 was 13.9%. 7
Among men of all ages, the prostate cancer incidence rate from 2017-2021 was 113.2 and 111.7 (per 100 000 population) in the U.S and South Carolina, respectively. 8 From 2018-2022, the prostate cancer mortality rate (per 100 000 population) among men of all ages was 19.0 in the U.S. and 20.8 in South Carolina. 8
Among men ages 50 years and older, the prostate cancer incidence rate from 2017-2021 was 400.3 and 393.2 (per 1000 000 population) in the U.S. and South Carolina, respectively. 8 From 2018-2022, the prostate cancer mortality rate (per 1000 000 population) among men ages 50 years and older was 68.6 in the U.S. and 75.0 in South Carolina. 8 As shown above, South Carolina had a significantly higher prostate cancer mortality rate among men ages 50+ years as compared with the national rate for this group.
Institutional Review Board Review
The Medical University of South Carolina (MUSC) Institutional Review Board reviewed the protocol for the SC AMEN Program. The program was determined to be a quality improvement study rather than a Human Subjects Research study.
Methods
Overview
The SC AMEN Program had three specific aims. The first aim was to deliver prostate cancer educational sessions at several community locations in South Carolina with a focus on increasing knowledge about prostate cancer risk factors among Black men. The second aim was to provide navigation assistance for the participants following each prostate cancer educational session to address barriers related to scheduling an appointment to discuss prostate cancer screening. The third aim was to administer a three-month follow-up survey to each program participant to assess prostate cancer screening behavior (Figure 4). The study design of the SC AMEN Program was a pre-test/post-test design with no control group. To recruit participants, the investigators employed a convenience sample strategy, in which community champions volunteered to host the SC AMEN sessions in trusted community venues and recruited the participants for each session. The SC AMEN Program Aims
The educational sessions in the SC AMEN Program included information related to the biological factors, including the genetic aspects of prostate cancer, as well as content linking the social determinants of health to prostate cancer. Figure 5 displays the roles of several different social determinants of health and biological factors (modifiable and non-modifiable) and their contributions to health disparities. These factors were discussed during each SC AMEN educational session. Social Determinants of Health and Biological Factors’ Influence on Rural Prostate Cancer Disparities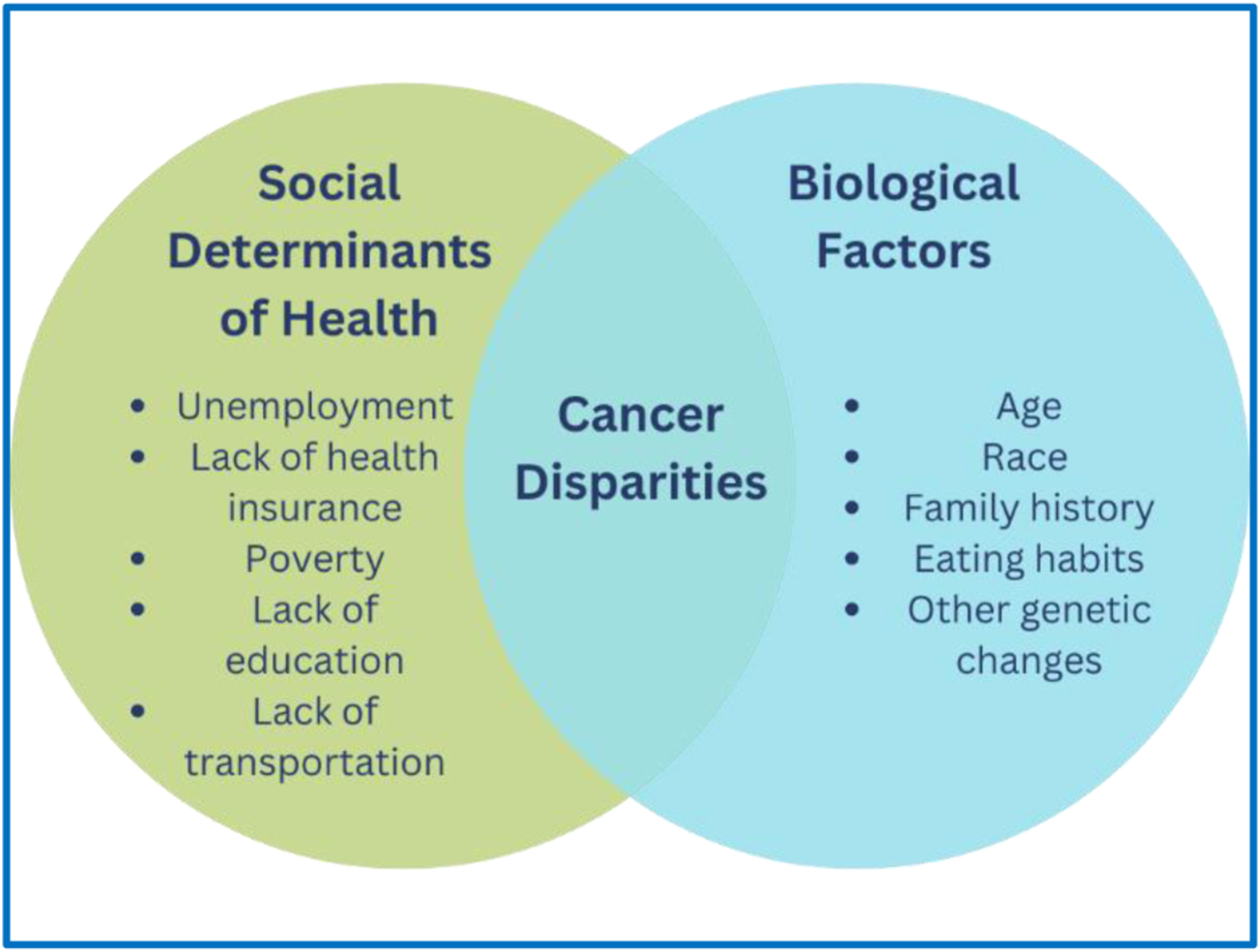
Strategy
The strategy used for Specific Aim 1 included a one-hour prostate cancer educational session delivered by MUSC Hollings Cancer Center community health educators (CHEs). The CHEs worked with underrepresented communities of South Carolina to provide a tailored prostate cancer educational training program.
The CHEs also worked with the MUSC Hollings Cancer Center’s data visualization teams to identify areas of the state with the highest prostate cancer mortality rates from 2018-2022 (Figure 6) and the lowest prostate cancer screening rates from 2017-2021 (Figure 7).
8
These areas then became the high-priority focus areas of the SC AMEN Program. Prostate Cancer Mortality Rates by County in South Carolina, 2018-2022 Prostate Cancer Screening Rates by County in South Carolina, 2017-2021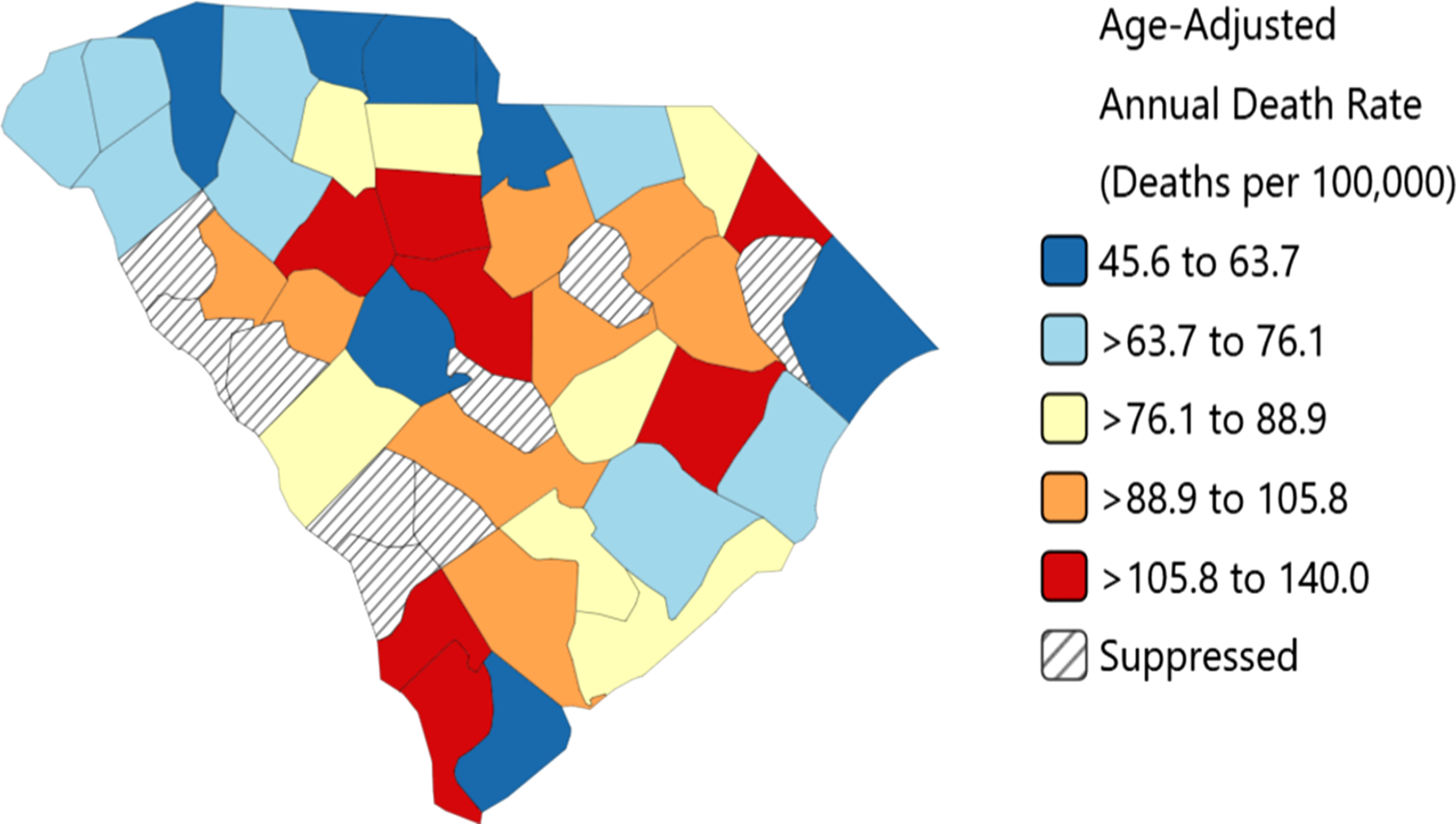

The CHEs worked with community partners who recruited Black men for each prostate cancer education session. Partners included the South Carolina Cancer Alliance, ZERO Prostate Cancer, Trident Urban League, and South Carolina State University.
The SC AMEN Program also partnered with the Seventh Episcopal District of the African Methodist Episcopal Church in South Carolina, which has included the MUSC Hollings Cancer Center in their official Health Ministry Plan. The SC AMEN Program staff collaborated with health ministry leaders of the African Methodist Episcopal Church to draft and plan prostate cancer education sessions at several African Methodist Episcopal churches in South Carolina. The SC AMEN Program also worked with other religion-based groups, such as churches in the South Carolina Baptist Association, to reach men of other religious denominations.
Each educational session included a pre-test and a post-test survey. The surveys included the 10-item Prostate Cancer Screening Education (PROCASE) Knowledge Index, which was developed in a sample of male patients aged 50+ years receiving primary care at four participating Veterans Affairs Medical Centers in the Midwest. 9 The goal of the pre-test and post-test survey was to assess knowledge on prostate cancer, symptoms, and diagnostic testing. Each participant received a $50 gift card as an incentive after completing the session. The key outcome for Specific Aim 1 was to increase prostate cancer knowledge of the SC AMEN Program participants.
The strategy for Specific Aim 2 was to address the social factors contributing to individual, organizational, economic, and sociocultural barriers of Black men in receiving prostate cancer screening. This aim included patient navigators, who assisted the participants in identifying community, health system, and personal resources to overcome these barriers to care.
Patient navigation is an evidence-based approach implemented to reduce cancer health disparities by identifying resources to address barriers to care related to the social determinants of health. Dr Harold P. Freeman created one of the first patient navigation programs in 1990 to help women navigate the process of breast cancer screening and follow-up care.10,11 Patient navigation is based on adult learning, social cognitive, and social support theory/competency evolution and is a barrier-focused intervention designed to ensure timely/efficient access to needed health services. 12 Navigators focus on case identification, addressing individual (eg., fear and anxiety), organizational (e.g., limited/lack of knowledge of screening locations/hours), economic (e.g., transportation and insurance), and sociocultural (eg, mistrust of the health care system) barriers to care, and implementing a care plan.11,13-15 Patient navigation interventions have been effective in navigating patients to cancer screening, through the diagnostic workup and resolution process, and through cancer treatment.16-18 Since lack of access to specialty care is a healthcare disparity that disproportionately affects Black and rural populations, patient navigation interventions can potentially reduce multifaceted barriers to care and improve receipt of optimal screening and follow-up care.19-21
In the SC AMEN Program, the National Cancer Institute’s Patient Navigation Barrier Checklist Form was utilized to help recognize each barrier and create a personalized plan of action using resources in the community and social support services. For example, the SC AMEN patient navigators often linked under- or uninsured participants with a Federally Qualified Health Center (FQHC) close to their homes to provide a medical home for the participants. The navigators also addressed participants’ transportation issues, mistrust of the healthcare system, mistrust of providers, and fear of positive test results.
The strategy for Specific Aim 3 involved surveying the program participants 3 months after the post-educational session to assess each participant’s prostate cancer screening status. The participants received another $50 gift card (in addition to the $50 gift card they received for participating in Aim 1) when they completed the three-month follow-up survey as an incentive. The key outcome of Specific Aim 3 was the receipt of prostate cancer screening.
Statistical Analysis
Characteristics at pre-test are presented as proportions or means (SD). Mean PROCASE Knowledge Index scores at pre-test and post-test were compared across sites and overall using paired t-tests. Multiple linear regression assessed variables associated with the change in pre-test vs post-test PROCASE Knowledge Index scores with adjustment for age, educational level, and insurance status. Participants with missing data were excluded from the analysis.
Results
Demographic Characteristics of Participants in the SC AMEN Program

Note: Age ranges from 40-69 years.
aInformation is missing on race for nine participants, ethnicity for nine participants, education for 13 participants, insurance status for 28 participants, prostate-specific antigen (PSA) test for 126 participants, digital rectal exam (DRE) for 62 participants, both PSA and DRE for 126 participants, and primary care for 23 participants.
Pre-Test and Post-Test Results of the PROCASE Knowledge Index by Site

a2-sided P-value. b(P-value <.050).
Impact of the SC AMEN Program on Prostate Cancer Screening Behavior
Since the program’s inception in September 2021, among the 568 SC AMEN Program participants, 475 (83.6%) either completed a prostate cancer screening (n = 266; 46.8%) or scheduled a screening appointment (n = 209; 36.8%). The remaining 24 participants (4.2%) continue to be navigated to a screening appointment, and 69 (12.2%) have refused navigation.
Multivariable Linear Regression Results of the Change in Pre-Test vs Post-Test PROCASE Knowledge Index Scores After Adjustment for Age, Education, and Insurance Status (n = 555)

Discussion
The South Carolina Prostate Cancer Education and Navigation to Screening Program for African American Men (SC AMEN Program) was launched in September of 2021 by the Medical University of South Carolina Hollings Cancer Center to address the disproportionately high prostate cancer mortality rates among Black men in South Carolina, which are nearly 2.5 times higher than those among White men in the state. 2 The program comprises three core components: a one-hour prostate cancer education session, evaluation of pre- and post- session prostate cancer knowledge, and three months of patient navigation to facilitate prostate cancer screening.
The SC AMEN Program was designed to address multiple factors contributing the elevated prostate cancer mortality rate among Black men, including poor diet—characterized by high consumption of processed foods and red meat and low intake of fruits and vegetables—and sedentary lifestyles, particularly prevalent in rural areas.22-29 These behaviors may increase prostate cancer risk, and molecular differences in tumor biology linked to these factors have been shown to contribute to cancer disparities. For instance, Lowder et al demonstrated that variations in gene expression and tumor microenvironment characteristics contribute to differential prostate cancer outcomes among different racial and ethnic groups. 30
The SC AMEN Program yielded promising results in encouraging screening discussions among Black men. These findings align with national data showing that targeted educational interventions can significantly enhance awareness and screening behaviors in high-risk populations. 31 Bratt et al 31 emphasize that while PSA-based screening can reduce prostate cancer mortality, its effectiveness depends on informed decision-making and selective application—both of which are supported by education and navigation programs such as the SC AMEN Program. 31
Community-based research further validates the SC AMEN Program’s design. For example, Malika et al 32 found that Black men often have significant knowledge gaps and low screening rates despite moderate awareness. Barriers such as lack of provider recommendation, mistrust in the healthcare system, and limited access to culturally relevant information were common. The SC AMEN Program’s culturally tailored education and patient navigation components directly address these challenges and promote informed, proactive health behaviors.
Other investigators have reported that community-based interventions significantly improved prostate cancer knowledge and screening rates among Black men, particularly when delivered through trusted community channels. 33 This supports the SC AMEN Program’s potential for scalability through partnerships with barbershops and other community hubs, as previously demonstrated by Luque et al 34
The SC AMEN Program’s focus on men aged 40 to 69 years represents a younger age group than the U.S. Preventive Services Task Force (USPSTF) recommendation of 55 to 69 years for the general population. However, the SC AMEN Program’s age rage is aligned with USPSTF and American Cancer Society guidelines for screening high-risk populations for prostate cancer, and may promote earlier engagement in screening and improved outcomes in disproportionately affected populations. 35
The SC AMEN Program could be expanded in several ways. First, new partners who engage with large numbers of Black men, such as barbers, could be integrated. Luque et al 34 evaluated a prostate cancer education intervention delivered in rural barbershops and found significant increases in knowledge scores among participating barbers (P < .03), supporting the feasibility of this approach. 34 Although the study was small, it serves as a proof-of-concept for future efforts. 34 Second, the program could be extended to include men of all racial and ethnic backgrounds, particularly those in rural and medically underserved areas. Men in rural regions have been shown to experience higher prostate cancer mortality rates compared to their urban counterparts.36-38 Medically underserved men, regardless of race or ethnicity, also face poorer survival outcomes. 39
The SC AMEN Program aligns with clinical prostate cancer screening recommendations for high-risk populations and with community-based prostate cancer screening evidence. It addresses critical gaps in knowledge and access and offers a replicable model for reducing prostate cancer disparities in underserved populations. Future iterations could consider expanding to include other high-risk groups and incorporate mechanisms for tracking long-term screening outcomes.
While the SC AMEN Program showed promising short-term results, several limitations should be noted. The absence of a control group limited causal inference, and the modest knowledge gains observed in univariable analysis were not statistically significant in multivariable models. Missing data and the lack of access to clinical screening results further constrained outcome evaluation. Additionally, the three-month follow-up may not reflect long-term screening adherence. Despite these limitations, the SC AMEN Program demonstrated strong community engagement and offers a replicable model for addressing prostate cancer disparities in high-risk populations.
Conclusion
The SC AMEN Program was successful in leading to improvements in receipt of prostate cancer screening. However, the work in the high-impact SC AMEN Program goes far beyond prostate cancer screening. It also guides the development and implementation of cancer prevention, control, and treatment strategies focused specifically on Black men, which will ultimately create a framework for increasing health equity among other medically underserved, rural, and racially/ethnically diverse populations. The SC AMEN Program and others like it will be beneficial in decreasing the disparities in prostate cancer.
Footnotes
Acknowledgements
The authors would like to acknowledge the community partners who participated in the SC AMEN Program.
Ethical Consideration
The Medical University of South Carolina (MUSC) Institutional Review Board reviewed the protocol for the SC AMEN Program. The program was determined to be a quality improvement study rather than a Human Subjects Research study.
Author contributions
All those designated as authors should meet all four criteria for authorship, and all who meet the four criteria should be identified as authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported, in part, by the following funding sources: TD Charitable Foundation (GR089448, GR10002422, PR000236), Healthy Me/Healthy SC; Medical University of South Carolina Cancer Center Support Grant (P30CA138313); South Carolina Cancer Disparities Research Center (SC CADRE) (U54CA210962 and U54CA210963); South Carolina Clinical and Translational Research Institute (SCTR) (UL1TR001450). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Subject to appropriate ethical and legal considerations, the authors are willing to: (1) Share their research data in a relevant public repository. (2) Cite these in their research.