
Abstract
Decreased prostate-specific antigen screening since 2008 has generated much concern, including report of recent increase in metastatic prostate cancer incidence among older men. Although increased metastatic disease was temporally proceeded by decreased screening and decreased localized prostate cancer at diagnosis, it is unclear whether the 2 trends are geographically connected. We therefore used the National Cancer Institute Surveillance, Epidemiology, and End Results (SEER) database to assess geographic-specific associations between changes in localized (2008-2011) and later changes in metastatic prostate cancer incidence (2012-2015). We examined trends from 200 health-care service areas (HSAs) within SEER 18 registries. While on average for each HSA, localized incidence decreased by 27.4 and metastatic incidence increased by 2.3 per 100 000 men per year, individual HSA-level changes in localized incidence did not correlate with later changes in metastatic disease. Decreased detection of localized disease may not fully explain the recent increase in metastatic disease at diagnosis.
Introduction
There is conflicting evidence and ongoing controversy regarding the effectiveness of prostate-specific antigen (PSA) screening for prostate cancer. 1,2 Analyses of national health survey and claims data suggest PSA screening utilization has decreased since 2008. 3,4 Nationally, this decrease in screening has been temporally associated with a decrease in detection of localized prostate cancer, and more recently, an increase in incidence of metastatic prostate cancer among older men. 5 However, PSA screening patterns vary by geographic region, and while decreased detection of localized disease is hypothesized to increase likelihood of metastatic disease at diagnosis, it remains unknown if the 2 trends are correlated geographically. 6 In other words, one might expect that geographic regions with larger decreases in detection of localized prostate cancer would also have a relatively greater increase in metastatic prostate cancer incidence. Therefore, we used recent population-level registry data to examine geographic-level associations between changes in localized and changes in metastatic prostate cancer at diagnosis.
Materials and Methods
We chose a priori to examine most recent years 2012 to 2015 for changes in metastatic disease, and the preceding years, 2008 to 2011, for changes in localized disease. We assumed a 4-year difference in time interval (“lead time”) between the development of metastatic disease and potential detection via screening due to previous analysis of randomized trial data suggesting clinically occult disease can progress to advanced disease in as little as 4 years. 7 We used the Surveillance, Epidemiology, and End Results (SEER) database to obtain prostate cancer incidence among United States men aged 70 years or older. We chose to examine this age-group due to recent epidemiologic evidence suggesting metastatic prostate cancer incidence is increasing among older men, and the most recent United States Preventive Services Task Force (USPSTF) guidelines recommend against screening among men aged 70 years or older. 8 We used SEER Summary Stage to classify localized (local) and metastatic (distant) prostate cancers. 9
We calculated incidence rates by National Cancer Institute (NCI) modified health service areas (HSAs), which each represents a relatively self-contained region of hospital care. The original HSAs were formulated by the National Center for Health Statistics and comprised of geographic areas containing one or more counties such that most residents of those areas received care from the same hopsitals. 10 The HSAs were subsequently modified by NCI such that individual HSAs did not extend across state boundaries or SEER registries. This resulted in approximately 950 NCI-modified HSAs containing approximately 3200 counties, with considerable variation in geography and population between HSAs. 11 We used population-weighted linear regression with heteroscedasticity-consistent (Huber-White) standard errors to determine correlation between changes in the incidence of localized versus metastatic disease during the study period.
Results
A total of over 66 600 cases of localized and 6400 cases of metastatic prostate cancer among men aged 70 or older from 200 HSAs were included for analysis. From 2008 to 2011, localized incidence decreased from 613.6 to 534.2 per 100 000 men aged 70 or older overall, with an average annual decrease for each HSA of 27.4 per 100 000 men (Figure 1 A). From 2012 to 2015, metastatic incidence increased from 54.7 to 62.1 per 100 000 men aged 70 or older overall, and for each HSA on average increased by 2.3 per 100 000 men for each year (Figure 1 B). There was considerable variation across HSAs, with standard deviations of 37.3 for localized incidence and 9.5 for metastatic incidence, both per 100 000 men per year. Linear regression between HSA-level changes in localized and metastatic disease revealed a correlation coefficient of −0.023 (standard error = 0.017, P = .16, 95% confidence interval: −0.056 to 0.009), representing lack of a statistically significant relation between decreases in localized disease and later increases in metastatic disease within individual health-care service areas (Figure 2). In sensitivity analysis, there is no statistically significant correlation between changes in localized incidence and later changes in metastatic incidence despite increasing the lead time to 5 years or including younger men aged 50 or older.
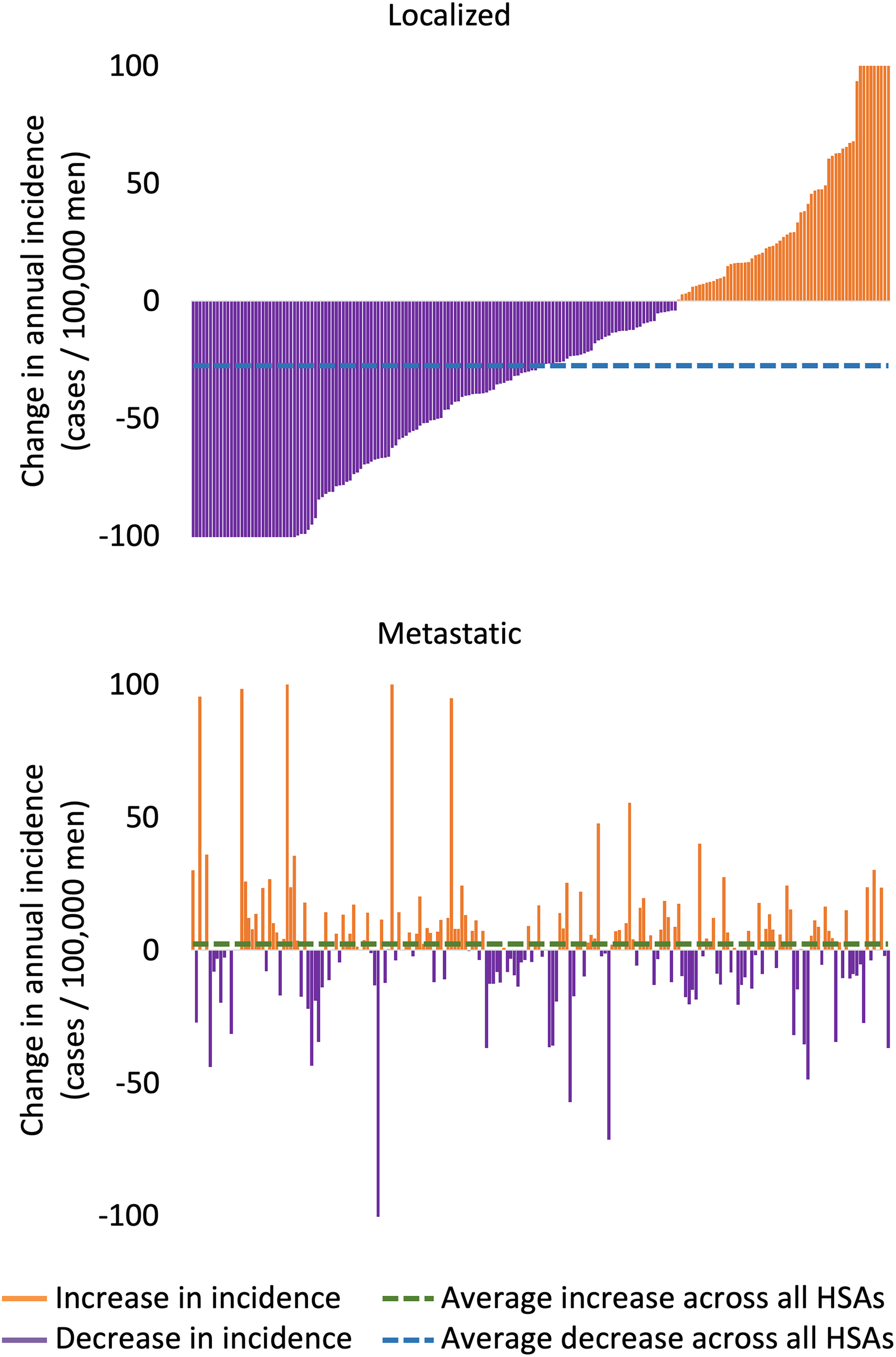
Average change in localized (top) and metastatic (bottom) prostate cancer incidence for each health services area sorted by change in localized incidence.

Population-weighted linear regression between HSA-level changes in localized and metastatic prostate cancer incidence.
Discussion
Our study shows that there was no statistically significant correlation within HSAs between changes in localized prostate cancer incidence and subsequent changes in metastatic prostate cancer incidence during the time periods compared. Although previous studies in context of USPSTF recommendations against prostate cancer screening have suggested decreased PSA screening as the most plausible explanation for the recent increase in metastatic prostate cancer incidence, our results show that when incidence trends are examined at a more granular geographic level, the relationship between decreased detection of localized disease and subsequent increase in metastatic disease is not apparent if the lead time between screening detection and development of metastatic disease is assumed to be 4 years. 5,12 -15 Reasons for increasing rates of metastatic disease besides a lack of screening should be considered, although there are currently no clearly established temporal trends in underlying risk factors, such as race/ethnicity, socioeconomic status, lifestyle factors, family history, and genetic factors to explain the observed changes in metastatic disease incidence. 6,16 -18 Additionally, it is possible that with greater assumed lead time and further follow-up, a geographic relationship between lower rates of localized prostate cancer and higher rates of metastatic disease may ultimately be revealed.
Despite 3 large randomized clinical trials evaluating its efficacy, prostate cancer screening remains the subject of ongoing controversy. 19 -21 Most recent 2018 USPSTF statement on prostate cancer screening now recommends individualized decision-making for men aged 55 to 69 years, and against PSA screening for men aged 70 years and older. 8 This will likely continue to affect PSA utilization patterns. Moreover, practice pattern changes in disease treatment and monitoring will also continue to shift the balance of benefits and harms of early detection. For example, increased adoption of active surveillance as a conservative management option for low-risk prostate cancer has been suggested to mitigate the potential harms of overdiagnosis and overtreatment. 22 -24 Future studies are needed to closely monitor changes in disease incidence and possible underlying causal factors, as well as trends in disease treatment options.
Strengths of our study include large cohort taken from a nationally representative cancer registries database, which provides accurate and contemporary incidence rates. Interpretation of our results is limited by study design and available data. We report an association observed by health service areas, which represent relatively small regions and are more subject to statistical fluctuations. Our study is ecological and therefore cannot prove the presence or absence of any causal relationship. Confounding is a major concern inherent to ecologic study design. We cannot account for individual-level factors such as lifestyle and family history. Population-level covariates such as HSA population density, racial and ethnic composition, median income and education level, among others, can also potentially confound our results. We do not report mortality data, which requires longer follow-up. We also assume a relatively short lead time, which may not be reflective of the natural history of prostate cancer progression, and further longitudinal studies are needed. Given the retrospective design of our study, we chose a priori to examine the described age-group and years. Nevertheless, our findings are robust to sensitivity analysis. Although we observe a temporal relationship at the national level, a geographic HSA level association is not observed despite varying age-group or years of diagnosis.
In summary, our population-level observation suggests that decreased detection of localized disease during an era of decreasing utilization of routine PSA screening may not fully explain the recent increase in metastatic disease incidence among older men in the United States if a lead time of 4 years between screen detected cancer and metastatic disease is assumed. Alternative reasons for increased metastatic disease may be evaluated, along with longer assumed lead time between screening detected cancer and subsequent development of metastatic disease.
Footnotes
Authors’ Note
This study used deidentified cancer registry data and does not involve human or animal subjects.
Acknowledgments
This work was presented at the American Society of Clinical Oncology (ASCO) Annual Meeting; June 2019; Chicago, IL.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Gross received research grants from Johnson & Johnson, and Pfizer, and funding for travel from Flatiron Inc, outside the submitted work. Dr Yu received personal fees from Augmenix Inc, outside the submitted work.