
Abstract
Background
Prostate cancer is the most common malignancy in men globally. This study aims at investigating the incidence rates and trends of prostate cancer in Lebanon, and to compare them to those of countries from different regions in the world.
Methods
Data on prostate cancer were obtained from the Lebanese national cancer registry for the years 2005 to 2016. The calculated age-standardized incidence and age-specific rates were expressed as per 100 000 population.
Results
In Lebanon, prostate cancer is ranked as the most common cancer in men. The age-standardized incidence rate of prostate cancer has increased from 29.1 per 100 000 in 2005 to 37.3 per 100 000 in 2016; the highest rate was in 2012, surpassing the global average incidence rate for that year. The age-specific incidence rate of prostate cancer has increased exponentially starting at the age of 50 years to reach its peak in men aged 75 years or more. Two trends were identified in the age-standardized incidence rate of prostate cancer; an average significant increase of 7.28% per year for the period 2005–2009 (P-value < .05), followed by a non-significant decrease of around .99% for the period between 2009 and 2016 (P-value > .05). The age-standardized incidence rate in Lebanon was higher than most countries in the Middle East and North Africa region and Asia, but lower than the rates reported in Australia, America, and different European countries.
Conclusion
Prostate cancer is the leading cancer among men in Lebanon. Screening practices, changes in population age structure, and prevalence of genetic and risky lifestyle factors may explain the increased incidence rates of prostate cancer. Given the controversy of screening recommendations and the slow growing nature of prostate cancer, increasing public awareness on ways of prevention, and implementing the latest screening recommendation of the United States Preventive Services Task Force are the suggested way forward.
Background
Prostate cancer (PCa) is the fourth most common cancer globally, and the second most common malignancy among men. 1 PCa has had an increasing incidence over the years, with a staggering 1,414,259 new cases in 2020, compared to 1,276,000 reported in 2018; 1,112,000 in 2012; and 913,000 cases in 2008.2-4 It is the fifth most common cause of cancer-related mortality in men worldwide, leading to around 375,304 deaths in 2020 (6.8% of all cancer-related deaths in men), 358,989 deaths in 2018, 307,000 deaths in 2012, and 261,000 deaths in 2008.1-4 Its projected age-standardized incidence rate adjusted to the world population (ASRw) per 100,000 person-years was estimated to be 30.7 in 2020, compared to 29.3 in 2018, 31.1 in 2012, and 28.5 in 2008.1-4 Globally, the incidence of PCa shows a substantial geographic disparity that can exceed 25-fold between one region and another.2,3
Countries with high or very high standard human development index (HDI, a measure of the average achievement of a country in 3 key dimensions of human development: long and healthy life, being knowledgeable, and having a decent standard of living), 5 were reported to have the highest estimated incidence of PCa in 2018. These countries are located mainly in Oceania, Northern and Western Europe, and Northern America regions. 2 The estimated incidence of PCa is lower in less developed regions such as the Caribbean, Southern Africa, and South America, and much lower in Asia and Africa (particularly Northern and Eastern Africa).2,3 This geographic variation in PCa incidence may be explained by a higher frequency of screening for PCa in some developed countries, as well as differences in the prevalence of risk factors or protective factors for PCa among different populations.2,3,6-9
The introduction of prostate-specific antigen (PSA) in 1986 as a screening test for the early detection of PCa was associated with a significant upsurge in the incidence of PCa globally for many years to come. 2 Another major shift occurred in the last decade, particularly in the United States of America (USA) and most Nordic countries subsequent to the recommendation of the United States Preventive Services Task Force (USPSTF) against screening for PCa in 2012, following which there was a decline in the global incidence of PCa.2,10 However, USPSTF changed their recommendation again in 2018 and proposed a shared decision for PCa screening 11 ; the impact of this change on the incidence of PCa remains to be seen.
Risk factors of PCa.

Lebanon is a small developing country in the Middle East (population estimated at 6 million in 2016) with health indices close to those of the western world, 18 and it has a high HDI based on the standard HDI formula (.757 in 2017). 5 PCa is one of the most common cancers in men in the country, and it accounted for 16.5% of cancer-related deaths amongst men in 2014. 19 The Lebanese national cancer registry (NCR) was officially restarted in 2002 after years of inactivity due to multiple wars; this registry provides an almost absolute count of all incident cancer cases nationwide. NCR data are being continuously collected from the capture system (data collected passively from physicians’ reports) and recapture system (data collected actively from histopathological and hematological laboratories) 20 ; the recapture system confirms and complements the capture approach. 21 The NCR covers most cancer cases (more than 90%) in Lebanon, 20 but it excludes in situ lesions. The NCR periodically publishes its cancer incidence data electronically on the Ministry of Public Health (MoPH) website; the currently available data cover the period extending from 2005 to 2016. 21
This study aims at analyzing the 12-year incidence rates and temporal trends for PCa in Lebanon. It also compares the incidence rates in Lebanon, the Middle East and North Africa (MENA) region, and other countries and regions worldwide. Recommendations for effective PCa screening and prevention are highlighted, taking into consideration the different risk factors prevalent in the Lebanese context.
Materials and Methods
Twelve-Year Trend Analysis From 2005 Until 2016
In this study, PCa data include diagnosis with the code C61 of the International Classification of Diseases, 10th revision (ICD-10). The age-standardized incidence rate adjusted to the world population (ASRw) and the age-specific incidence rates, expressed per 100,000 men, were retrieved from the Lebanese NCR data published on the MoPH website for twelve consecutive years from 2005 to 2016. 21 The ASRw is a weighted average of the age-specific incidence rates per 100,000 persons, with weights being the proportions of persons in the corresponding age groups of a standard population. Standardization is important when comparing different populations with different age structures. The most used standard population is the world standard population, which is drawn from a pooled population of several countries. In this study, the ASRw was calculated using the modified world standard population by Doll as the reference population. 22 The age-specific incidence rate is the number of new cancer cases occurring during a specific period, in a population of a specific age and sex group, divided by the number of mid-year population of that age and sex group. 23
The annual percent change (APC) and the average annual percent change (AAPC) of PCa incidence rates over the years were calculated using the Joinpoint Regression Program (JRP) 4.7.0.0 with a statistical significance level defined at a P-value < .05. The APC is based on the hypothesis that cancer rates change at a constant percentage of the previous year’s rate. 24
Projections of the ASRw of PCa in Lebanon for the Year 2025
Projections were estimated using the currently available PCa data over the 12-year period (2005–2016). Log-linear regression model was found to be the best fit model in this study (R-squared or R2: .607); therefore, future ASRw for PCa was projected by fitting a log-linear regression model to observed ASRw against observed years (y = 3.375ln(x) + 31.562). Linear and log-linear regression models, which assume a Poisson distribution for the observed number of incident cases, have been reported to be the most practical methods that can be used to estimate future patterns of cancer incidence for periods up to 10 years, while assuming that there is no change in underlying trends. 25

Comparison of Prostate Cancer Incidence Rates in Lebanon to Regional and Worldwide Countries
Prostate cancer ASRw and age-specific rates in Lebanon were subsequently compared with age-standardized and age-specific incidence rates from selected regional and worldwide countries that have cancer data available for a comparable period. These data were extracted from the Cancer Incidence in 5 Continents Time Trends (CI5plus), 26 Cancer Incidence in 5 Continents Volume XI (CI5 XI) 27 , or from the Regional or Country National Cancer Registry.28-32 The rates mentioned in CI5plus and CI5 XI are built on high-quality population-based cancer registries. For comparison, we included countries that surround Lebanon geographically, as well as randomly selected countries from the MENA region and other regions of the world.
Results
Incidence Trends (2005–2016) and Average Annual Percent Change (AAPC)
In Lebanon, PCa is ranked as the most common cancer in men (followed by lung, trachea, and bladder cancer) over the 12-year study period (2005–2016). A total of 9790 incident cases of PCa were reported during this period, with 92.4% of cases affecting men aged 50 years or more, and 70.3% affecting men aged 65 years or more. The average number of new cases of PCa per year was 816. The age-specific incidence rate increased exponentially starting at age of 50 years and reached its peak in men aged 75 years or more (Figure 1). Age-specific incidence rates (per 100,000 population) for prostate cancer, Lebanon 2005–2016.
Trend analysis for prostate cancer age-specific rate (per 100 000) in men by age group per year in Lebanon from 2005 to 2016.
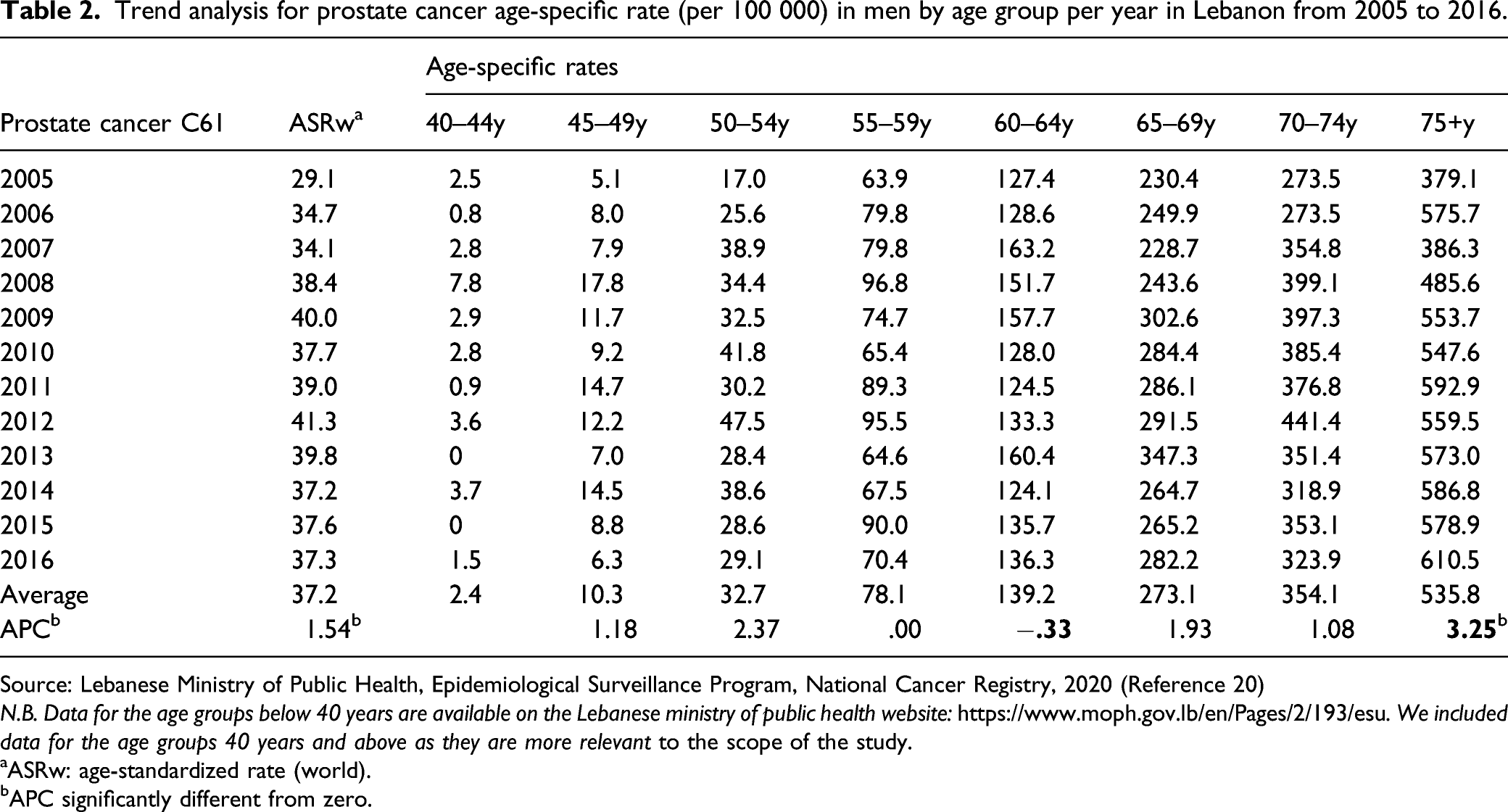
Source: Lebanese Ministry of Public Health, Epidemiological Surveillance Program, National Cancer Registry, 2020 (Reference 20)
N.B. Data for the age groups below 40 years are available on the Lebanese ministry of public health website: https://www.moph.gov.lb/en/Pages/2/193/esu. We included data for the age groups 40 years and above as they are more relevant to the scope of the study.
aASRw: age-standardized rate (world).
bAPC significantly different from zero.

Age-standardized incidence rates (ASRw) for prostate cancer in men, Lebanon 2005–2016 (0 joinpoints model).

Age-standardized incidence rates (ASRw) for prostate cancer in men, Lebanon 2005–2016 (1 joinpoint model).
Projected ASRw of PCa in 2020 and 2025
Using log-linear regression model, the ASRw of PCa per 100 000 men was estimated at 32.8 cases in 2020 (95% confidence interval: 20.8, 51.7) and 30.0 cases in 2025 (95% confidence interval: 11.0, 81.0).
Comparison of Prostate Cancer Incidence Rates in Lebanon to Regional and Worldwide Countries
Prostate cancer age-standardized incidence rates (ASRw) and age-specific rates per 100 000 men in Lebanon compared to MENA and non-MENA countries.

Abbreviations: ASR(w), age-standardized incidence rates (World Population); MENA, Middle East and North Africa; N.B, we included data for the age groups 40 years and above as they are more relevant to the scope of the study.
Projections from the published reports of the International Agency for Research on Cancer/Global Cancer Statistics (IARC/Globocan) revealed that the ASRw of PCa in Western countries was lower in 2020 than in 2012 following the 2012 USPSTF recommendation against the routine use of PSA testing (figure 4).
10
The 2018 USPTF recommendation does not seem to have a measurable effect yet.
11
As per Globocan 2020, Lebanon still has the highest ASRw (28.5) in MENA region after Israeli Jews and non-Jews (figure 5), although the Globocan projection figure for Lebanon is lower than our projection based on the NCR data (ASRw: 33.1, 95% confidence interval: 20.7, 45.4). Projected age-standardized incidence rates (ASRw) for prostate cancer by regions based on GLOBOCAN 2008, 2012, 2018, and 2020. Projected age-standardized incidence rates (ASRw) for prostate cancer in MENA countries-GLOBOCAN 2020 (Reference 1).

The ASRw of PCa in Lebanon increased by 7.5% between 2008 (38.4) and 2012 (41.3), mirroring a global increase in the ASRw by 9.1% between 2008 (28.5) and 2012 (31.1).3,4 The ASRw of PCa in Lebanon decreased by 9.7% between 2012 (41.3) and 2016 (37.3), concomitant with a global decrease by 6.1% between 2012 (31.1) and 2018 (29.3).2,3 Overall, the ASRw of PCa in Lebanon increased by 7.5% over the decade between 2006 (34.7) and 2016 (37.3), while it increased globally by 2.8% for the decade between 2008 (28.5) and 2018 (29.3) (the decades are not identical and are based on currently available NCR data and Globocan, respectively).2,4
Discussion
PCa is the most common cancer among men in Lebanon, like many countries worldwide.2,3 In 2018, PCa was the most common incident cancer among men in more than 50% of the countries worldwide (105 out of 185). 2 The ASRw of PCa in Lebanon was among the second highest in the MENA region after the Israeli Jews (almost equal to Israeli non-Jews), and higher than many countries in Asia, but much lower than the rates recorded in Australia/New Zealand, and countries in Northern and Western Europe and Northern America.2,3
The increase in the incidence of PCa and the variation in ASRw among different countries can be attributed to several factors including genetic factors, differences in population size and age structure, prevalence of risk factors, PCa screening recommendations and access to diagnostic and health care services.2,33,34 Despite the relatively moderate to high incidence rates of PCa in Lebanon, little research has been done to study this disease. Establishing epidemiological studies and statistics on PCa, along with a better understanding of its etiology and causative risk factors, are essential for creating the necessary infrastructure needed for the primary prevention and/or early detection of this disease. This infrastructure will provide strategies to identify at-risk men and to support the development of effective screening and prevention methods. In the following section, we will discuss various factors that may have contributed to the increased incidence of PCa in Lebanon.
However, global PCa incidence declined in the past few years, particularly in the USA and most Nordic countries since the USPSTF (in 2008 and again in 2012), the Canadian Task Force of Preventive Services (in 2014), and United Kingdom (UK) (in 2015) issued recommendations against screening.2,10,40,41 USPSTF updated their recommendations in 2018 and reconfirmed those of the American Urological Association (AUA) calling for screening men in age group 55–69 years based on shared decision, that is, asking patient approval after explaining the benefits and harms of screening.11,42 USPSTF and AUA do not recommend screening men aged 70 years and above or those between 40 and 54 years with average risk for PCa,11,42 namely, because of high overdiagnosis rates (23% to 42%) and common serious side effects associated with treatment. 43 Screening men in the age group 40–54 years with high risk for PCa should be individualized; high risk include men of African American race, and those with a family history of metastatic or lethal adenocarcinomas (e.g., prostate, male and female breast cancer, ovarian, and pancreatic) crossing multiple generations, affecting multiple first-degree relatives, and that developed at younger ages.11,42 More research is being conducted currently on more effective ways to screen for PCa, identify its fatal forms, detect men at higher risk and use of chemoprophylaxis such as aspirin and 5α-reductase inhibitors. 44
In Lebanon, the increased utilization of PSA testing, widely available over the counter, may have also partially accounted for some of the increasing trend in PCA incidence till 2012. National public awareness campaigns promoting screening for PCa were initiated since 1994. 45 These campaigns were either supported by the MoPH or the Lebanese Urological Society or by academic medical centers. However, the 2012 recommendation against the routine use of PSA testing by the USPSTF have probably influenced the practice of primary care physicians, resulting in a decline in the ASRw of PCa in Lebanon after that. In fact, only 29% of family physicians in Lebanon reported to systematically screen men aged above 50 years for PCa. 46 With the recent change in the recommendations by the USPSTF, the rates of screening might rise again leading to higher incidence rates in the future. It is worth noting that 25% of patients in Lebanon present with metastatic prostate disease, 47 which increases the need to enhance awareness among men namely those at increased risk.
In Lebanon, risky lifestyles (unhealthy diet and physical inactivity), obesity, and smoking are becoming more conspicuous.52-54 Physical inactivity is prominent among adults, with 61% of those aged 18-69 years report having low levels of physical activity, 55 and 34.8% of adults (40.9% of men) report spending more than 12 sedentary hours per day. 52 Obesity is also reaching an alarming level, 54 with 27% of adults aged 18-69 being obese, and 37.9% being overweight. 55 Tobacco smoking is also common among male adults, with a prevalence increasing from 43% in 2009 to 48% in 2016.52,55 Adult Lebanese consume high number of cigarette packs, reaching 12.4 packs per person per month. 56 Moreover, unsafe smoking-related indoor air pollution levels in several public places, 57 puts people at risk of passive smoking.
The association of alcohol with PCa is not conclusive. 8 Based on a recent meta-analysis, this association may vary with the type of alcohol; for example, the risk of non-aggressive PCa was associated with liquor (linearly) and beer (non-linearly), but not with wine or total alcohol intake. Moreover, the risk of aggressive PCa was higher with low liquor or heavy wine intake. 58 Alcohol consumption in Lebanon is the highest in the Arab region, 59 with 51.9% of adult men reporting drinking alcohol. 52
Our study is based on the cancer data published by the MoPH on its official website. Despite the improvements done in data collection for the NCR, information on collected cases is still incomplete lacking in-situ conditions, risk factors, as well as mortality and survival rates. Since our results are based on PCa rates for the years 2005 through 2016, caution is to be exerted when interpreting these results beyond the study period.
Conclusion
PCa is a significant health problem in Lebanon, affecting mainly older men. Changes in population age structure, screening and early detection practices, and prevalence of genetic and risky lifestyle factors could have increased the incidence rate of this disease. Despite that PCa is a slowly growing tumor, early detection and treatment can still improve the quality of life in men. To date, there is no evidence whether the introduction of a population screening program would reduce mortality without significant numbers of men being overtreated. Recommendations in this regard are still controversial. Countries are implementing different screening programs for addressing PCa burden. For example, United Kingdom implemented an informed choice program for PSA testing in asymptomatic men, using a tool that promotes patient-centered care and involves patients and physicians in weighing the benefits and harms of PSA testing.60,61
Given the high incidence rate of PCa in Lebanon, it is important to increase the awareness among men on primary prevention through adopting healthier lifestyle, and to strengthen healthy lifestyle education programs at the primary care level. Moreover, it is advised to follow the USPSTF latest recommendations regarding PSA testing, that is, shared decision testing in asymptomatic men aged 55–69 years and individualized testing in high-risk men aged 40–54 years.
Footnotes
Abbreviations
APC Annual Percent Change
AAPC Average Annual Percent Change
ASRw age-standardized incidence adjusted to the world population
AUA American Urological Association
C15 Plus Cancer Incidence in 5 Continents Time Trends
C15 XI Cancer Incidence in 5 Continents Volume XI
HDI Human Development Index
IARC International Agency for Research on Cancer
ICD10 International Classification of Diseases, 10th revision
IGF-I Insulin-like growth factor-I
JRP Joinpoint Regression Program
MENA Middle East and North Africa
MoPH Ministry of Public Health
NCR National Cancer Registry
PCa prostate cancer
PSA prostate-specific antigen
SNP single nucleotide polymorphism
UK United Kingdom
USA United States of America
USPSTF United States Preventive Services Taskforce
WHO World Health Organization
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.