
Abstract
Purpose
Optimal approaches for tobacco treatment counseling among individuals who currently smoke and are undergoing shared decision-making (SDM) and lung cancer screening (LCS) are unknown. The objective of this cross-sectional study was to determine the rate of reported interest in tobacco treatment counseling and pharmacotherapy among individuals who currently smoke and are receiving integrated nurse navigation for LCS and tobacco treatment in a centralized LCS Program.
Methods
We identified individuals undergoing SDM through our centralized LCS Program between March 2021 and March 2022. The LCS Program tobacco treatment protocol includes counseling both in-person and via telephone during SDM, LCS results review, and an optional 4-week follow-up. Sociodemographic and clinical data for currently smoking individuals participating in LCS were extracted from the LCS Registry.
Results
Among 1034 individuals undergoing LCS through the centralized program, 605 were currently smoking and comprised the study cohort. Nearly half (49.8%) reported interest in tobacco treatment counseling and pharmacotherapy and received a personalized treatment plan. On multivariate analysis, factors significantly associated with expressing interest in treatment included African-American/Black race, higher educational attainment, and returning visit type. Among the 301 individuals expressing interest in tobacco treatment, 35 (11.6%) had documentation of self-reported smoking cessation in the electronic health record. Successful smoking cessation for any length of time was significantly associated with receiving at least one longitudinal tobacco cessation counseling telephone call.
Conclusions
In a centralized LCS Program offering tobacco treatment integrated with screening services, race, education, and visit type were significantly associated with expressing interest in tobacco treatment counseling and pharmacotherapy, while longitudinal tobacco counseling telephone calls were associated with smoking cessation. Randomized controlled trials are needed to test whether this integrated strategy leads to LCS- and tobacco-related outcomes.
Keywords
Introduction
Lung cancer is the leading cause of cancer-related mortality in the United States. 1 With nearly 90% of lung cancers linked directly to cigarette smoking, tobacco cessation and early detection of lung cancer are the most broadly effective interventions for reducing lung cancer incidence and mortality. 2 Specifically, lung cancer screening (LCS) with low-dose computed tomography (LDCT) leads to a relative reduction in mortality risk of 20% or more.3,4 Since publication of updated United States Preventive Services Task Force (USPSTF) eligibility criteria for LCS in 2021, reducing the age (50–80, previously ages 55–80) and smoking intensity threshold (20 pack-years, previously 30 pack-years), an estimated 14.2 million Americans are eligible for LCS.5,6 With a national smoking prevalence of 12%, approximately 30.8 million American adults are estimated to identify as individuals who current smoke. 7 This junction provides a unique opportunity for LCS Programs to leverage screening appointments into a teachable moment for tobacco treatment, particularly in regions of the US where smoking prevalence may be greater than national rates.
Any tobacco use increases lung cancer risk; however, individuals who have stopped smoking have a significant reduction in overall mortality as well as a 39% reduction in lung cancer risk compared to individuals who currently smoke.8,9 Additionally, tobacco dependence is associated with higher rates of screen-detected lung cancer and mortality. 2 Both clinical practice guidelines from specialty societies and the Centers for Medicare and Medicaid Services (CMS) require tobacco treatment as part of high-quality implementation of the LCS process.10-13 Another critical component of LCS as required by CMS is shared decision-making which allows for the confirmation of eligibility, highlights the importance of adherence to annual and short term follow-up for LCS, and educates patients on smoking cessation. SDM provides patients an opportunity to have a discussion regarding potential harms and benefits surrounding LDCT.10-13
Approximately 50% of individuals screened for lung cancer currently smoke, and despite having increased lung cancer risk, these participants are less likely to adhere to annual LDCT than those who formerly smoked.14-17 Previous studies have demonstrated high levels of interest in smoking cessation among currently smoking individuals undergoing LCS.16,18-20 Further, many screening patients report strong interest in smoking cessation counseling in conjunction with nicotine replacement therapy (NRT), and one study found 50% of currently smoking individuals receiving LCS were interested in obtaining a bupropion prescription to assist in cessation.20,21 While undergoing LCS alone may not be associated with smoking cessation, reviewing LDCT results and, in particular, having abnormal LDCT findings has been shown to increase readiness to quit and/or cessation rates in multiple studies.22-26 Retrospective analyses have demonstrated that less than 40% of currently smoking individuals undergoing LCS received any type of cessation resource, and only 5% received both counseling and pharmacotherapy. 27
While there is great promise in offering tobacco treatment as part of LCS, with multiple recent randomized controlled trials testing a variety of interventions, the most effective implementation method is not yet known.28,29 Notably, interventions as part of comprehensive LCS have been shown to be cost-effective regardless of the methodology. 30 Offering multiple points of contact is crucial in encouraging individuals who currently smoke and are undergoing LCS to quit smoking. 21 Moreover, centralized approaches to LCS are associated with significantly higher annual adherence to screening. 31 Additionally, centralized programs improve screening amongst marginalized populations whom have a historically higher rate of tobacco use.32,33 Thus, centralized LCS Programs may be poised to deliver tobacco treatment specifically tailored to individuals at high risk for lung cancer. We aimed to retrospectively characterize tobacco treatment in a centralized LCS Program, which integrates tobacco treatment counseling and pharmacotherapy with LCS nurse navigation.
Methods
Delivery of Tobacco Treatment Counseling and Pharmacotherapy
The Jefferson LCS Program provides centralized, comprehensive LCS at an urban academic medical center. The program is staffed by an advanced practice provider, two master tobacco treatment specialist-certified nurse navigators, and a patient coordinator and is supported by a multidisciplinary team of clinician experts as described in previous publications.17,34-37 The patient coordinator receives referrals from primary care physicians, other clinicians, and self-referrals and works to assess screening eligibility, obtain insurance authorizations, and schedule appointments for SDM with same-day LDCT. The nurse navigators or nurse practitioner confirm LCS eligibility and performs SDM in an in-person or telemedicine appointment, the patient then obtains a scan. During these appointments, the patient will learn about their risk of lung cancer, the importance of screening, and go over the potential harms and benefits of LCS. If applicable, the patient will receive personalized smoking cessation and receive an individualized tobacco treatment protocol. After their appointment, the patient will receive outreach from the nurse navigators or advanced practice provider for results review, management of nodule and non-nodule findings, follow up recommendations, and review of tobacco treatment plan when applicable.
The LCS Program carries out a tobacco treatment protocol accredited by the Public Health Management Corporation’s Smoking Treatment Accreditation and Recognition (STAR) Program with several touchpoints that integrate evidence-based tobacco treatment counseling and/or pharmacotherapy (TTC/P) across the LCS process, leveraging intensive guidance by the nurse navigators. (Figure 1) The integrated touchpoints include obtaining a detailed smoking history upon entry into the program, tailored tobacco dependence counseling during SDM, follow-up counseling at the time of LCS results review, and additional support at an optional 2-week and 4-week appointments and/or ongoing telephone counseling as requested by patients. This integrated process has been part of the standard of care provided by the LCS Program since January 2018. Shared decision-making including tobacco treatment counseling is repeated on an annual basis for all individuals returning for continued screening. Integrated Tobacco Treatment Counseling and Pharmacotherapy with Centralized Lung Cancer Screening. Tobacco treatment services are provided in concert with multiple touchpoints across the lung cancer screening process.
Study Cohort
Individuals undergoing LCS who completed SDM and LDCT between March 30, 2021, and March 30, 2022, were identified retrospectively from the Jefferson LCS Program Registry. Patients who self-reported former smoking status were excluded from this analysis. Sociodemographic and clinical data related to tobacco use and smoking cessation were extracted from the prospectively maintained LCS Registry. Study data were collected and managed using REDCap electronic data capture tools hosted at Thomas Jefferson University.38,39 Patients who were identified as expressing interest in TTC/P underwent additional review in the electronic medical record (EMR) to capture additional outcomes. The Thomas Jefferson University Institutional Review Board granted a waiver of informed consent (#17D.150) for this low-risk, observational, cross-sectional study. The reporting of this study conforms to STROBE guidelines. 40
Outcome Measures: Receipt of Tobacco Cessation Services and Pharmacotherapy
Outcomes related to tobacco use were extracted from the Jefferson LCS Registry and from the EMR. All currently smoking individuals enrolled in the LCS program participants are asked to self-report interest in tobacco treatment during SDM. Individuals who express interest immediately receive individualized tobacco treatment counseling and pharmacotherapy, following clinical practice guidelines from the American Thoracic Society. 41 Patient interest and post-counseling TTC/P plans were recorded prospectively in the Jefferson LCS Registry by the nurse navigators and nurse practitioner. Patients with recorded interest in the Registry were manually chart reviewed in the EMR. Tobacco treatment outcome measures extracted from the EMR included presence of pharmacotherapy prescriptions, frequency and timeframe of follow-up tobacco counseling telephone calls, and documentation of tobacco abstinence of any duration.
Statistical Analysis
Descriptive statistics and frequency tables were used to characterize the study sample. Independent t-tests and chi-square tests were performed. Unadjusted and adjusted logistic regression analyses were conducted utilizing known and previously identified confounders of the receipt of tobacco cessation services and successful smoking cessation.42-44 All analyses performed were 2-sided, using a P < 0.05 significance threshold, and conducted using SPSS statistical software version 29. 45
Results
Baseline Demographics
Among 1034 individuals who underwent LCS during the study period, 605 (58.5%) reported current smoking status and comprised the final cohort for analysis. (Figure 2) The mean age of individuals in this group was 62.9 ± 5.8 years, and 58.3% (n = 353) were female. Slightly more than half of patients were Black (n = 306; 50.6%), 43.5% (n = 263) were White, and 6.0% (n = 36) self-reported races including American Indian/Alaskan Native, Asian, Native Hawaiian/Pacific Islander, and More Than One Race and were classified as Other. Participants reported a mean smoking intensity of 46.6 ± 19.8 pack-years. The most common level of educational attainment was a high school diploma or GED equivalency (n = 276; 45.6%), and Medicare was the most frequent insurance type (n = 201; 33.2%). Study Design. After excluding formerly smoking individuals, 605 currently smoking individuals receiving lung cancer screening between March 30, 2021, and March 30, 2022, comprised the study cohort. This cohort was analyzed to identify the proportion of individuals who expressed interest in tobacco treatment counseling and pharmacotherapy, as well as additional downstream outcomes including smoking cessation prescriptions, follow-up telephone calls for additional counseling, and self-reported smoking cessation.
Primary Outcome: Receipt of a Tobacco Treatment Counseling and Pharmacotherapy Plan
Baseline Demographics of Currently Smoking Individuals Receiving LCS (n = 605).
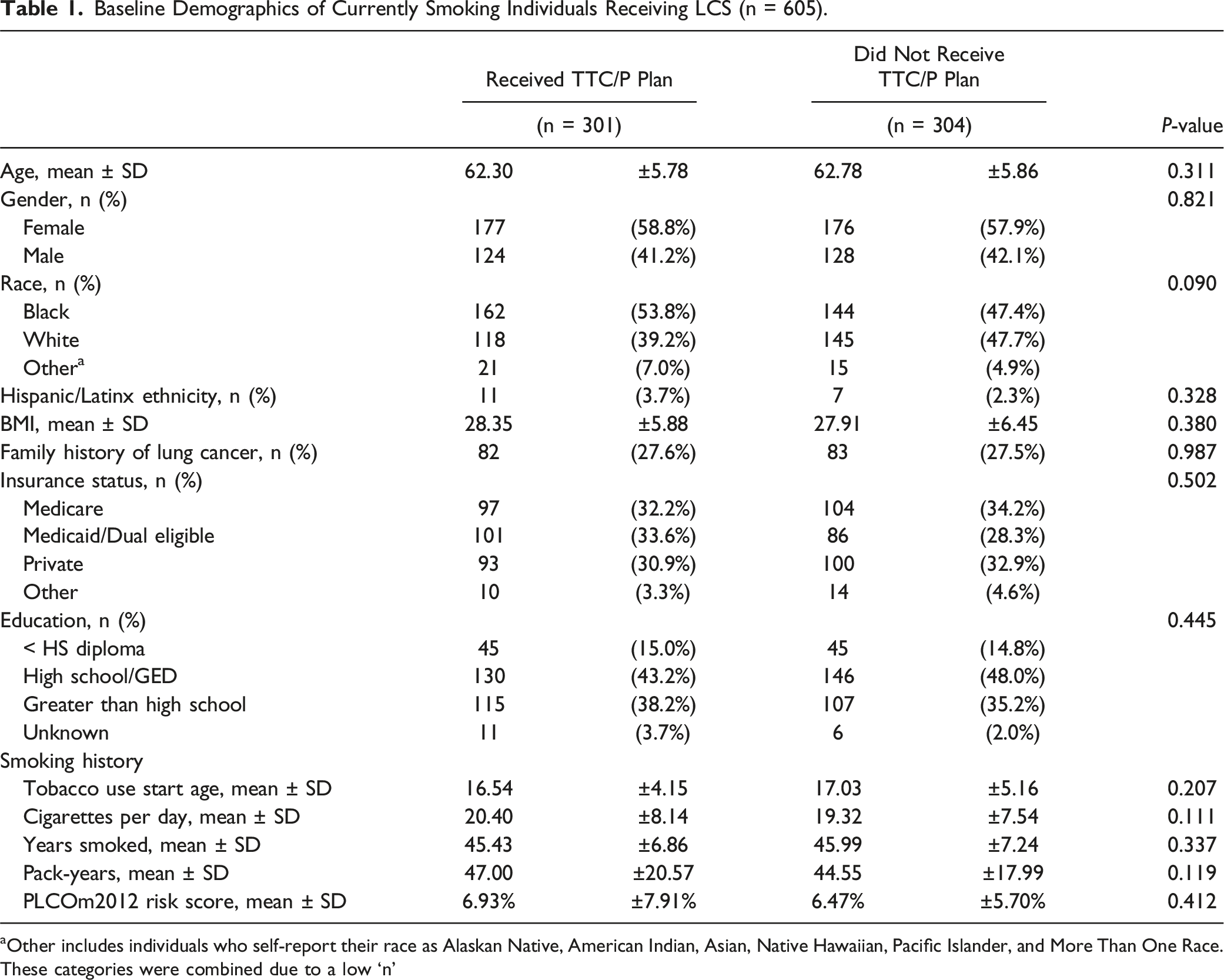
aOther includes individuals who self-report their race as Alaskan Native, American Indian, Asian, Native Hawaiian, Pacific Islander, and More Than One Race. These categories were combined due to a low ‘n’
The planned pharmacotherapy regimen most frequently recorded in the LCS Registry was single nicotine replacement therapy (35.2%), followed by combination nicotine replacement therapy (controlled and reliever, 28.9%). (Supplemental Table 1).
Predictors of Expressing Interest in Tobacco Treatment Counseling And/Or Pharmacotherapy (n = 605).

+P < 0.10, *P ≤ 0.05; **P ≤ 0.01.
aOther includes individuals who self-report their race as Alakasan Native, American Indian, Asian, Native Hawwiian, Pacific Islander, and More Than One Race. These categories were combined due to a low ‘n’.
Tobacco Treatment Counseling and Pharmacotherapy Follow-Up
The group of 301 individuals expressing interest in receiving a TTC/P plan was further characterized for events occurring after SDM, including pharmacotherapy prescription, follow-up telephone calls for additional counseling, and smoking cessation. One-hundred ninety-eight patients (65.8%) received a prescription documented in the EMR from the LCS Program for tobacco treatment, and 103 (34.2%) did not receive a prescription. The most commonly prescribed regimens were nicotine controller plus reliever (n = 73, or 24.3%) and single nicotine replacement therapy (n = 60; 19.9%). Over half (n = 164; 54.5%) of patients receiving TTC/P received a follow-up telephone call for additional counseling, with 20.7% (n = 34) receiving two or more phone calls and most (n = 85, or 51.8%) occurring within 14 days of the SDM appointment. (Supplemental Table 2).
Tobacco Abstinence
Predictors of Smoking Cessation Among Individuals Expressing Interest in TTC/P (n = 301).
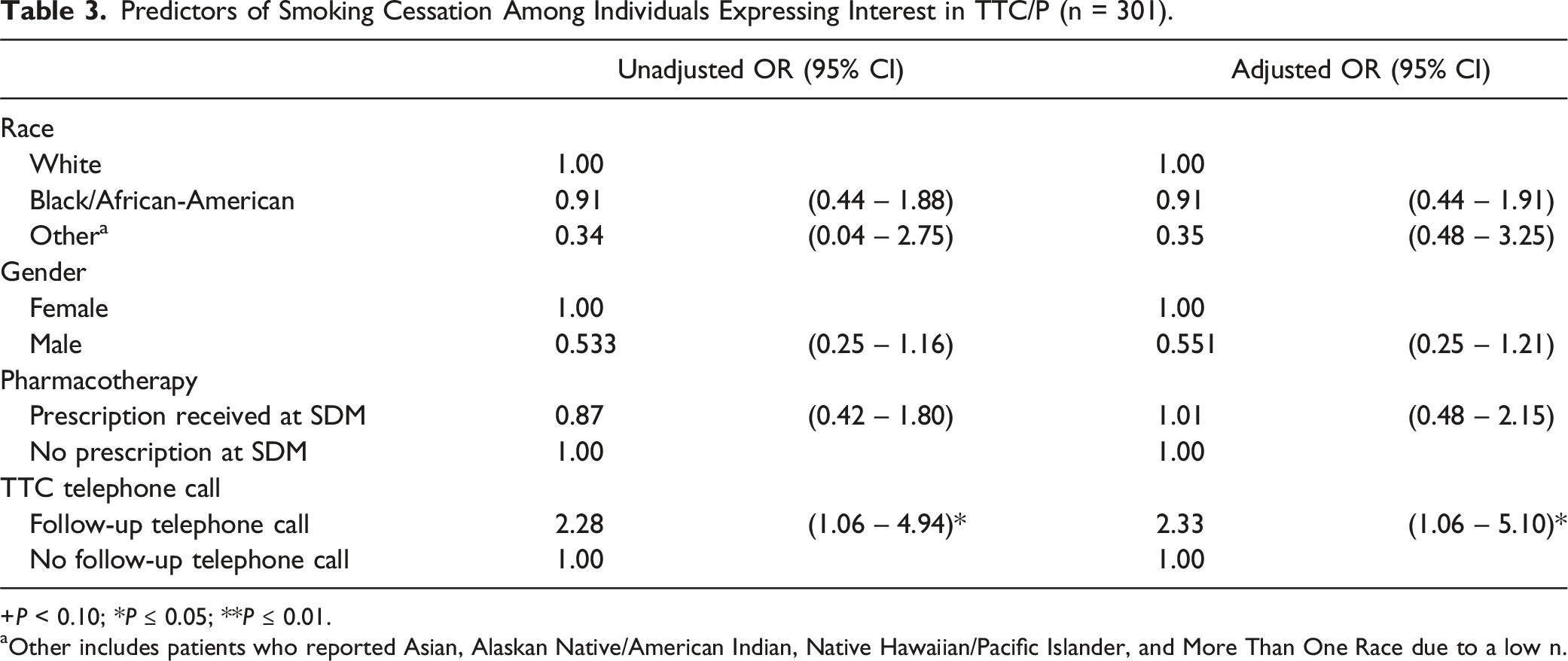
+P < 0.10; *P ≤ 0.05; **P ≤ 0.01.
aOther includes patients who reported Asian, Alaskan Native/American Indian, Native Hawaiian/Pacific Islander, and More Than One Race due to a low n.
Discussion
In the context of LCS, tobacco dependence is associated with higher rates of screen-detected lung cancer, worse lung cancer mortality, and lower annual adherence to screening.8,9 Integrating tobacco treatment counseling and pharmacotherapy with a centralized LCS process is a pragmatic strategy for maximizing “teachable moments” as patients proceed through the LCS continuum. We found that nearly one-half of currently smoking individuals enrolled in our centralized LCS Program received smoking cessation counseling and a pharmacotherapy plan. Black race, educational attainment, and LCS visit type were significant predictors of interest in tobacco treatment and receipt of a TTC/P plan. Smoking cessation among patients who received a TTC/P plan was significantly associated with receiving at least one longitudinal tobacco cessation counseling telephone call.
Among individuals undergoing LCS through a centralized, integrated nurse navigator-driven program, nearly half of current smokers, expressed interest in and received TTC/P plan. This finding is in line with literature describing substantial interest in tobacco treatment services for smokers undergoing LCS.16,18-20 Upon review of the EMR, 65.8% of smokers received a prescribed pharmacotherapeutic, which is significantly higher than the less than 20% rate shown in existing literature.27,46 On multivariate analysis, factors associated with receipt of tobacco cessation services and pharmacotherapy included Black/African-American race, higher educational attainment, and new patient type aligning with data showing that Black/African-Americans are more likely than white patients to participate in smoking cessation programs.47,48
The main strength of this analysis is the large cohort of currently smoking individuals undergoing a standard protocol for integrated smoking cessation by master tobacco treatment specialist-certified nurse navigators. In this unique approach, tobacco services are provided directly by the centralized LCS Program to leverage patient-centered relationships and ensure that tobacco cessation counseling and prescriptions can be provided immediately and within the context of discussing lung cancer early detection and prevention. While the literature describes substantial interest in tobacco treatment services among individuals who currently smoke and are undergoing LCS, implementation of treatment involves multiple barriers.16,18-20 Among veterans receiving LCS, for example, just 1% received both behavioral treatment and pharmacotherapy for tobacco use. 49 Furthermore, in decentralized LCS Programs, only 20% of screened patients were reported to have received a pharmacotherapy prescription.27,46 In our cohort, the proportion of patients expressing interest in – and receiving tobacco treatment – far exceeds that of other studies. Notably, patients returning for annual LCS had significantly lower odds of receiving a TTC/P plan, perhaps paradoxically due to greater familiarity with – and therefore less intensive – SDM process. Interventions tailored to LCS-adherent individuals who continue to smoke should be tested prospectively in multi-center trials.47,48
Despite provision of a TTC/P plan to all patients who expressed interest in tobacco treatment, there was discordance with the frequency of prescriptions in the EMR. This reflects a pitfall of retrospective studies and includes instances where patients had already obtained medications from primary care physicians, over the counter at pharmacies, state quit lines, or other resources. In addition, although tobacco treatment plans were recorded prospectively and EHR prescriptions were reviewed retrospectively, it could not be confirmed whether patients were adherent with either planned or prescribed pharmacotherapy. We may have found that pharmacotherapy prescriptions were not associated with tobacco abstinence because the EHR prescriptions are not a complete record. Specifically, 11.1% of patients that received pharmacotherapy had any length of tobacco abstinence whereas, 12.6% of patients that were not prescribed pharmacotherapy had successful smoking cessation. We observed an overall rate of self-reported smoking cessation of 11.6% in this study, which is similar to that described in LDCT clinical trials and cohort studies. 49 Due to the retrospective nature of this analysis, true point prevalence and continuous abstinence outcomes could not be identified.
Additional limitations of this study include the lack of generalizability as the data came from a single institution. Smoking cessation outcomes were measured via self-report and may not be accurate due to faulty memory and social desirability bias. In addition, greater tobacco abstinence may have been noted among individuals receiving telephone calls due to more opportunities for EMR documentation by providers.
Approximately 55% of patients who expressed interest in smoking cessation received a documented follow-up telephone call. Consistent with previously observed benefit with multiple points of contact throughout the LCS process to encourage cessation, there was a significantly higher quit rate among those who received at least one follow-up call compared to those who did not receive a call. Among individuals with self-reported tobacco abstinence, the proportion of individuals who received two or more telephone calls was greater compared to those who only received one phone call from a nurse navigator. Interestingly, the length of time between SDM and follow-up phone call did not appear to be a factor in successful tobacco abstinence.
Trials from the National Cancer Institute’s Smoking Cessation at Lung Examination (SCALE) collaboration demonstrated similar findings, with one reporting significantly increased short-term quit rates among patients who receive intensive weekly telephone counseling over 8 weeks, and another found patients enrolled in tobacco longitudinal care had clinically meaningful long-term quit rates with more frequent follow-ups, demonstrating the importance of frequent longitudinal cessation counseling as part of a LCS program.28,50-52 Although increased frequency of outreach within a longitudinal tobacco cessation program has a direct correlation to tobacco abstinence, cost and resource intensity may prevent LCS programs from implementing a longitudinal integrated tobacco treatment and cessation program.
However, other SCALE collaborators did not find a difference in tobacco abstinence success with longitudinal follow-up. The OaSis trial found that although patients had an overall significant reduction in tobacco use, there was not a significant difference in abstinence between patients who received less vs more counseling from their assigned radiology facility. 29 Further, there was no meaningful difference in smoking cessation at one year between patients who received calls from cessation counselors and those who did not; however, a greater number of patients who received tobacco counseling calls were given pharmacotherapy. 53 The remaining trials in SCALE have not yet published results.54-56
The findings from these recent clinical trials do not diminish the importance of delivering tobacco treatment and cessation services as part of a LCS program. Centralized programs have the ability to offer integrated cessation services compared to decentralized programs that often have fewer resources. Understanding the principles of frequency, timing, and degree of intervention of tobacco cessation counseling can allow health systems that participate in LCS to adopt cost-effective and customizable cessation services that can be efficacious in long-term smoking abstinence.
Conclusion
Integrating tobacco treatment with LCS navigation through a centralized approach provides an opportunity to provide tobacco treatment in a familiar environment without requiring additional large investment beyond that of the centralized LCS Program. In real-world settings where resources for tobacco treatment services are severely limited and improved LCS adherence (and perhaps additional LCS outcomes) is noted in centralized screening programs, an integrated strategy such as the one described here may be the most pragmatic approach.
Further prospective studies are needed to evaluate specific approaches in implementing tobacco treatment and counseling in the context of LCS. It is imperative to begin discussion of smoking cessation upon first contact with the patient, gauge patient interest in tobacco treatment counseling and pharmacotherapy, and follow-up throughout the LCS process. Future directions should focus on standardizing tobacco treatment and pharmacotherapy in LCS and improving documentation in order to provide measurable outcomes to assess performance.
Supplemental Material
Supplemental Material - Factors Associated With Receipt of Tobacco Treatment Integrated With Nurse Navigation in a Centralized Lung Cancer Screening Program at an Urban Academic Medical Center
Supplemental Material for Factors Associated With Receipt of Tobacco Treatment Integrated With Nurse Navigation in a Centralized Lung Cancer Screening Program at an Urban Academic Medical Center by Christine S. Shusted, Sarah Mukhtar, James Lee, Brooke Ruane, Emily Muse, Lawrence Emeigh-McBride, Eboni Gatson-Anderson, Gregory C. Kane, Kuang-Yi Wen, Hee-Soon Juon, and Julie A. Bar in Cancer Control
Abbreviation
Lung Cancer Screening
Low-Dose Computed Tomography
United States Preventive Services Task Force
Centers for Medicare and Medicaid Services
Nicotine Replacement Therapy
Smoking Treatment Accreditation and Recognition
Tobacco Treatment Counseling and/or Pharmacotherapy
Shared Decision Making
Electronic Medical Record
Smoking Cessation at Lung Examination
Footnotes
Author note
Prevent Cancer Foundation Outstanding Young Investigator Award.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by JAB and CSS. The first draft of the manuscript was written by SM, CSS, and JAB. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported a research grant from the Prevent Cancer Foundation JAB reports research grants from the Genentech Health Equity Innovations Fund, and research grants paid to her institution from Delfi Diagnostics, Inc, outside the submitted work.
Ethics Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.