
Abstract
With the introduction of early-onset colorectal cancer (EO-CRC), defined as diagnosis before the age of 50, research has increasingly focused on distinguishing it from late-onset colorectal cancer (LO-CRC). However, the majority of these studies have delved deeply into specific aspects of the condition, and there is still a limited number of articles that comprehensively review the overall differences between EO-CRC and LO-CRC. In this review, we conducted literature searches on PubMed, Embase, and ScienceDirect databases using keywords such as “early-onset colorectal cancer”, and “late-onset colorectal cancer”. The retrieved articles were further screened to select those related to clinical manifestations, pathological features, molecular mechanisms, and prognosis for detailed analysis. Our findings indicate that the potential pathogenesis of EO-CRC is closely associated with lifestyle and environmental changes of the younger population. Compared to LO-CRC, EO-CRC tends to present with more severe initial symptoms, is more often diagnosed at an advanced stage, and primarily affects the left half of the colon. Postoperative pathology shows greater malignancy and invasiveness. At the biomolecular level, PIK3CA mutation and TP53 deletion exhibits a higher mutation rate in EO-CRC compared to LO-CRC, while other common gene mutations such as APC, KRAS, and SMAD4 are relatively less frequent. Additionally, MSI-H is more prevalent in patients with EO-CRC. Differences in transcriptomics and metabolomics profiles have also been observed between EO-CRC and LO-CRC, which may account for their distinct biological characteristics. The prognosis of EO-CRC is a subject of controversy, with varying trends observed across different age groups at onset, as well as between genders and ethnicities. In this study, we aimed to uncover the potential mechanisms behind the continuous rise in EO-CRC incidence and to provide a basis for optimizing standardized screening and treatment strategies for EO-CRC through a comprehensive analysis of the differences between EO-CRC and LO-CRC.
Introduction
Colorectal cancer (CRC) is 1 of the three most common cancers worldwide, with its incidence and mortality continuing to rise. 1 Due to the large-scale progress of the early screening program for CRC, the majority of patients receive timely clinical intervention at the stage of intestinal polyps or precancerous lesions. As a result, CRC incidence has stabilized among individuals aged ≥50 years. However, the incidence rate among individuals aged 20 to 49 is increasing globally. 2 With the age of the first diagnosis gradually decreasing, the concepts of early-onset colorectal cancer (EO-CRC),—defined as CRC occurring in individuals under the age of 50, has gained increasing attention. 3 Although some organizations, such as the American Cancer Society (ACS), revised the recommended age for CRC screening from 50 to 45 in 2018, and the U.S. Preventive Services Task Force (USPSTF) proposed a similar screening recommendation in 2021, current CRC screening guidelines in most countries still recommend regular screening for individuals aged 50-75.4-6 Moreover, most previous studies have consistently used age 50 as the cutoff for distinguishing between early-onset and late-onset colorectal cancer, and a substantial body of research and clinical practice has established this standard, which has, to some extent, created a certain degree of inertia.7,8 Therefore, this review continues to adopt the definition of EO-CRC as occurring in individuals under the age of 50, while further dividing the age into subgroups for a more detailed discussion. Current research has shown that EO-CRC differs from late-onset colorectal cancer (LO-CRC) in terms of disease development, progression, and prognosis. EO-CRC is now increasingly recognized as a distinct disease entity rather than merely a specific subtype of CRC. 9
In this review, we conducted a comprehensive literature search using PubMed, Embase and ScienceDirect databases. Search terms included: “early-onset colorectal cancer” AND “late-onset colorectal cancer” AND “differences”, “early-onset colorectal cancer” AND “epidemiology”, “early-onset colorectal cancer” AND “pathogenesis”, “early-onset colorectal cancer” AND “metabolomics”, “early-onset colorectal cancer” AND “clinical manifestations”, “early-onset colorectal cancer” AND “genes” AND “pathways”, “early-onset colorectal cancer” AND “prognosis” AND “risk factors”. Subsequently, duplicate literature across different databases were removed, and the remaining literature was preliminarily screened by reviewing the titles and abstracts to select those that met the objectives of this review. Full texts of the selected literature were obtained through database websites or library resources and were thoroughly examined. Inclusion criteria: Studies published between 2015 and 2025 were included in this review if they focused on research involving the EO-CRC group, LO-CRC group, and a healthy population control group. Exclusion criteria: Studies were excluded if the full text was not available electronically, or if they were conference abstracts, letters, or case reports. The entire literature screening process is detailed in the PRISMA flowchart (Figure 1). In this study, we aimed to provide a comprehensive review of the differences between EO-CRC and LO-CRC in terms of epidemiology, potential pathogenesis, biomolecular characteristics, and clinical manifestations to enhance understanding of EO-CRC and inform future screening and treatment strategies. Flowchart of the Literature Study Process and Selection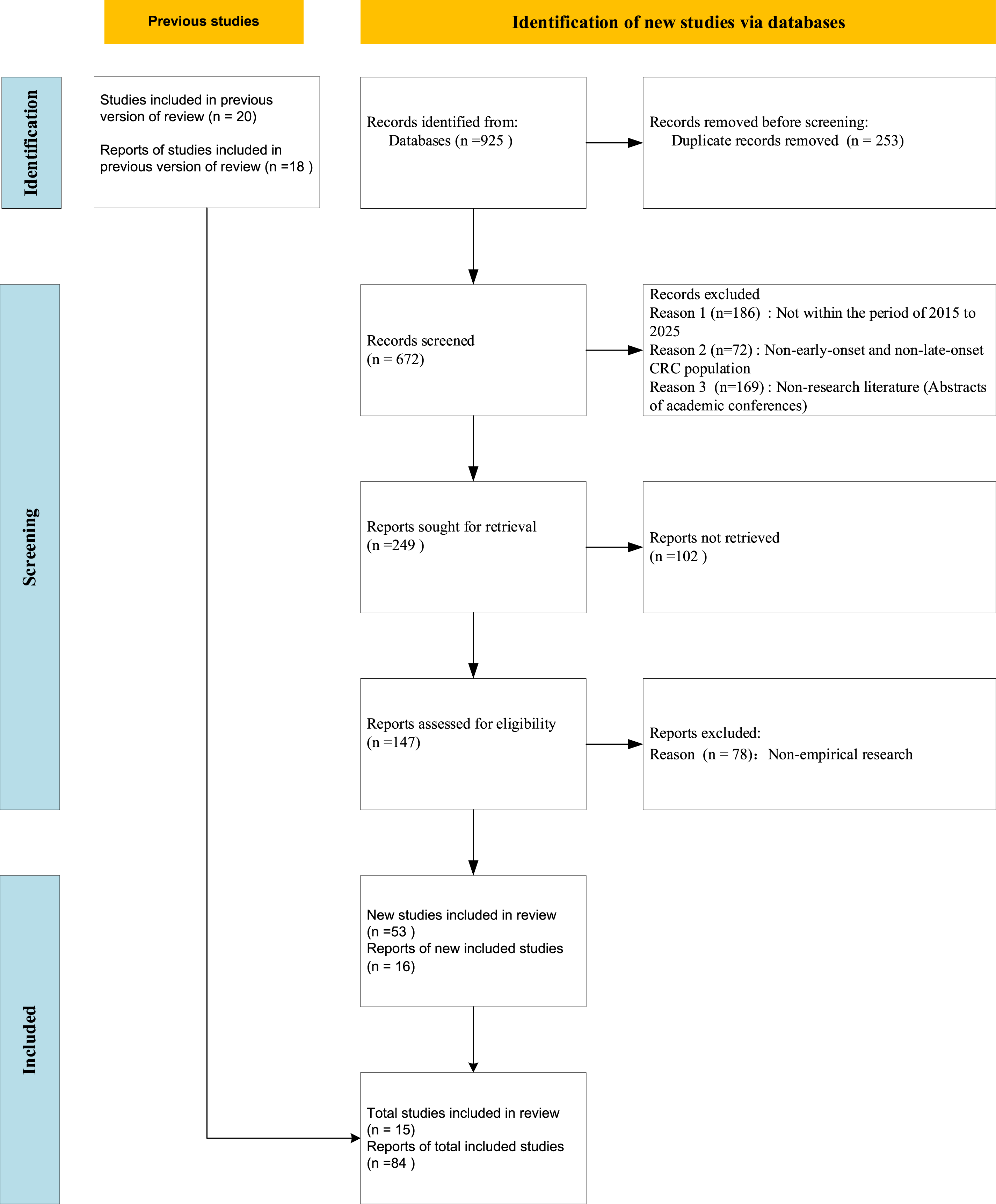
Epidemiologic Trends
Age
Over the past few decades, the incidence of CRC has increased year by year, while the age of onset has been gradually decreased. 10 Similarly, a retrospective study conducted in 2022 observed a significant upward trend in CRC among adults under 50 years of age after 2001, while a downward trend was noted in patients with CRC over 50 years during the same period. 11 Jian L et al. analyzed the changing trends of EO-CRC in China from 1990 to 2019. Their findings revealed that, compared to 1990, the number of new EO-CRC cases in 2019 had increased by 264.53%, and the number of deaths increased by 76.92%. 12 In another study by Fanny EV et al., further analysis stratified by age was conducted on patients under the age of 50, the incidence of CRC increased annually by an average of 7.9% in the 20-29 age group, 4.9% in the 30-39 age group, and 1.6% in the 40-49 age group. 13 Looking ahead, it is estimated that 10% of colon cancers and 25% of rectal cancers will be detected in individuals under 50 years of age. In the 20-34 age group, the incidence of colon and rectal cancers is projected to increase by 90% and 124%, respectively. in the 35-49 age group, the incidence is expected to rise by 27% and 46%, respectively. 14 These changes in the incidence of CRC, the trend toward younger onset age, and the differences in growth rates across different age groups underscore the severity and urgency of paying attention to EO-CRC.
Region
Although the incidence of EO-CRC is on the rise, it continues to exhibit a certain degree of geographical pattern. Over the past decade, CRC incidence rates have been steadily increasing in young adults in nine high-income countries (Germany, USA, Australia, Canada, New Zealand, UK, Denmark, Slovenia, and Sweden) across North America, Europe, and Oceania where rates in older adults are stable or declining. Notably, in countries such as the Netherlands and Norway, the incidence of CRC among young individuals has doubled compared to that in the elderly. Moreover, a 2021 analysis of cancer data from 42 countries revealed that CRC incidence rates among individuals aged 20-49 years were lowest in India and highest in Korea. Looking ahead, some projections estimate that by 2030, individuals under 50 years could account for up to 32% of all CRC cases in the United States, given the current trajectory of EO-CRC incidence.15-17 The overall decline in CRC incidence among individuals aged ≥50 years is largely attributed to widespread CRC screening, which has led to increased detection and removal of intestinal polyps and precancerous lesions, thereby preventing cancer progression. Conversely, significant shifts in environmental factors, lifestyle behaviors, and dietary habits among younger populations since the 20th century are believed to contribute to the rising incidence of EO-CRC. However, further investigation is needed to fully elucidate the underlying causes and risk factors driving this trend.
Etiology and Pathogenesis
Obesity and Overweight
Obesity is a known risk factor for CRC and various malignancies. Adipose tissue contributes to systemic inflammation and metabolic alterations, including insulin resistance, hyperglycemia, oxidative stress, and dysregulated adipokines such as lipocalin and leptin, all of which have been implicated in CRC development. 18 Globally, obesity rates continue to rise. From 1990 to 2022, the age-standardized prevalence of obesity globally increased from 6.6% to 15.8%, and the number of obese individuals rose from approximately 195 million to 890 million. 19 A 2024 meta-analysis on the global prevalence of overweight and obesity among adolescents indicated that the overall prevalence of obesity in children and adolescents was 8.5% (95% CI,8.2-8.8); compared to the period from 2000 to 2011, the prevalence from 2012 to 2023 increased by 1.5 times. 20 In a large cohort study, Song et al. followed 3,340,635 health check-ups over 7 years, during which 7492 participants were diagnosed with EO-CRC. Persistent general and abdominal obesity were associated with a higher risk of EO-CRC compared to normal-weight individuals. 21 Similarly, Jin EH et al. investigated the relationship between metabolic syndrome and EO-CRC in the Korean population and found that metabolic syndrome was associated with an increased risk of EO-CRC (adjusted hazard ratio: 1.20; 95% CI: 1.14-1.27). Furthermore, they discovered that a higher body mass index (BMI) was significantly associated with an increased risk of EO-CRC (P < .0001). 22 In another study, Li et al. reported that individuals with a BMI ≥30 kg/m2 at the ages of 20, 30, and within 10 years before diagnosis had a 2.56-fold (95% CI: 1.20-5.44), 2.06-fold (95% CI: 1.25-3.40), and 1.88-fold (95% CI: 1.30-2.73) higher risk of early-onset CRC, respectively, compared to those with a BMI <25 kg/m2. 23 Taken together, these findings suggest that the rising obesity rate among the younger population is a potential factor contributing to the increased incidence of EO-CRC. BMI, as a crucial indicator for quantifying individual obesity levels, has consistently been associated with an increasing risk of EO-CRC as BMI rises. Therefore, BMI is expected to play a pivotal role in future EO-CRC risk assessment and early screening.
Dietary Patterns
Strong evidence supports the link between dietary habits and CRC progression. Wang et al. examined 18 dietary patterns and found that the Western diet was among those most strongly associated with CRC. 24 Over the past half-century, dietary habits have shifted, with higher intake of protein, sodium, and processed foods and lower consumption of fruits and vegetables. This Western dietary pattern—characterized by high consumption of red and processed meat, elevated protein intake, and low dietary fiber—is increasingly prevalent among young adults. 25 A study examining dietary factors and EO-CRC incidence among U.S. adults aged 25-49 found that alcohol consumption has risen significantly, with intake positively associated with EO-CRC risk. 26 High-protein, low-fiber diets may disrupt the gut microbiota, leading to chronic inflammation, while alcohol may increase cancer risk through multiple mechanisms. Therefore, future research should explore how dietary modifications and lifestyle changes can reduce EO-CRC risk.
Antibiotic Misuse
Comparison of Anti-anaerobic Antibiotics and the Risk of Different Types of Colorectal Cancer

Gut Microbiota
Gut microbiota is involved in various physiological processes, including metabolism, immune regulation, and inflammatory responses, and are closely related to human health. Imbalance in gut microbiota can increase the risk of CRC by promoting inflammation and genetic instability.42,43 A study from China revealed that the alpha diversity of gut microbiota in patients with EO-CRC was significantly lower than that in patients with LO-CRC and healthy young volunteers. The most abundant bacteria in the EO-CRC group were Fusobacteria, while in the LO-CRC group, Bacteroidetes predominanted. 44 In a study conducted by Xu Z et al., microbial analysis was performed on tumor tissues of patients. In addition to the consistent finding that the intestinal microbiota richness in patients with EO-CRC was lower than that in patients with LO-CRC, the study also observed that patients with EO-CRC exhibited a higher prevalence rate of Actinomycetales compared to those with LO-CRC. Furthermore, Actinomycetales demonstrated good performance in identifying EO-CRC, with an area under the curve (AUC) of 0.747. 45 In addition to the composition of the gut microbiota, there are also differences in the metabolites produced by gut microbiota between the two groups. Studies have found that EO-CRC is characterized by higher levels of choline and bile acid metabolites. 46 These studies suggest that gut microbiota may play a certain role in the prediction and treatment of EO-CRC. Additionally, previously discussed factors such as obesity, dietary habits, and excessive use of antibiotics can also influence the composition of the gut microbiota, thereby contributing to the development and progression of CRC.47-49 Given its relevance, the gut microbiota is of significant importance in understanding the pathogenesis of EO-CRC. However, current research on the characteristics of gut microbiota in relation to EO-CRC remains relatively limited. Future studies need to delve deeper into the differences in gut microbiota in fecal samples and tumor tissues from patients across different regions and age groups, and integrate these findings with the interactions between the development and progression of EO-CRC, associated risk factors, and prognosis.
Advances in Multi-Omics Research
Comparative Analysis of Multi-Omics Studies on Different Types of Colorectal Cancer

Genomics
Lieu CH et al. conducted genetic testing on tumor specimens from patients with EO-CRC and found that mutations in APC, TP53, KRAS, PIK3CA, and SMAD4 were the most common, similar to those observed in traditional colorectal cancer. Some researchers have analyzed the genetic mutation profiles of patients with EO-CRC and LO-CRC and discovered that the prevalence of APC, KRAS, and BRAF mutations is significantly lower in patients with EO-CRC compared to patients with LO-CRC. In studies on TP53 deletion, it was found that the incidence of TP53 deletion is relatively high among European patients with EO-CRC. However, data from a study in Asia showed no difference in TP53 mutation rates between the two groups, while PIK3CA mutation (20% vs 12.1%) was more prevalent in patients with EO-CRC. These findings suggest that genomic alterations in patients with EO-CRC may have certain regional correlations.50-53 In the study of pathway alterations, Ferrell et al. used genomic data from cBioPortal and divided published genomic data into two age groups (≤50 years and >50 years) for a comprehensive bioinformatics analysis of mutations associated with the WNT and TGF-β signaling pathways. Their findings indicated a higher prevalence of TGF-β–related mutations in LO-CRC, while no significant differences were observed in WNT pathway alterations between EO-CRC and LO-CRC. 54
Epigenomics
The occurrence and progression of EO-CRC are closely associated with epigenetic changes. Previous studies have also found that BRAFV600 E mutations increased with age, while BRAF mutations were less common in EO-CRC. In contrast, cases with CpG Island Methylator Phenotype (CIMP)–positive mutations were highly prevalent, suggesting that CIMP frequently coexists with BRAFV600 E mutations. Although CIMP-positive cases represent a significant proportion of EO-CRC, the frequent co-concurrence with BRAFV600 E mutations suggest that CIMP may influence EO-CRC through distinct mechanisms.50,55 Additionally, genes involved in DNA damage repair and replication stress were significantly less active in EO-CRC, suggesting that reduced DNA damage repair efficiency may contribute to EO-CRC development. 56
Transcriptomics
Transcriptomics primarily examines gene transcription and transcriptional regulation at the RNA level in cells. At the transcriptomic level, CRC is typically classified into four molecular subtypes (Consensus Molecular Subtype, CMS): (1) CMS1, associated with tumors characterized by immune JAK-STAT signaling pathway activation, microsatellite instability, and high DNA mutation; (2) CMS2, mainly exhibiting classical WNT/MYC activation; (3) CMS3, characterized by metabolic alterations; and (4) CMS4, associated with epithelial-mesenchymal transition (EMT) and immune suppression. Compared to LO-CRC, EO-CRC exhibits distinct CMS subtypes, with CMS1 being more prevalent. While the Microsatellite Instability (MSI) phenotype accounts for less than 10% of CRC and LO-CRC cases, Microsatellite Instability-High (MSI-H) occurs in 10%–30% of EO-CRC cases. 57 Understanding the differences between Microsatellite Stable (MSS) and MSI tumor in EO-CRC can improve clinical diagnosis and treatment strategies. Although the genetic prevalence of CRC is estimated at 2%–5%, hereditary tumor susceptibility syndromes occur in 16%–35% of EO-CRC cases. 58 Among them, Lynch syndrome, which is strongly associated with CRC, particularly EO-CRC, increases lifetime CRC risk to as much as 70%, with a 50%–70% risk by the mid-40s. 59 This syndrome is characterized by defects in DNA Mismatch Repair (MMR) gene, which heighten cancer susceptibility and contribute to MSI development. In CRC, CIMP-positive tumors are often associated with MMR gene silencing, leading to a deficient MMR (dMMR) status. As previously mentioned, EO-CRC has a higher prevalence of MSI-H and CIMP positivity than LO-CRC, which may contribute to the increased incidence of Lynch syndrome in EO-CRC. MicroRNAs (miRNAs) have garnered significant attention as non-invasive biomarkers for CRC due to their stable presence in bodily fluids, making them promising biomarkers for cancer detection. Several studies have identified specific miRNAs associated with colorectal cancer. For example, Sabry D et al. found that in traditional colorectal cancer, the expression level of miR-21 is upregulated, demonstrated the highest diagnostic performance with an AUC of 0.973, a sensitivity of 91.4%, and a specificity of 95%. It was also correlated with TNM staging and the clinical stage of colorectal adenocarcinoma (P < 0.001), indicating high diagnostic value. 60 Liu et al. discovered through sequencing that the expression of miR-31-5p was significantly upregulated in EO-CRC tumor tissues compared to adjacent tissues, while this difference was not observed in LO-CRC, suggesting its potential role in the development of EO-CRC. 61 In their analysis of miRNA expression profiles in patients with CRC, Nakamura K et al. found that four miRNAs (miR-513a-5p, miR-628-3p, miR-193c-5p, and miR-210) were upregulated in EO-CRC compared to LO-CRC. These could serve as liquid biopsy markers for EOCRC, with the AUCs of the training and validation sets reaching 0.92 and 0.88, respectively. 62 Other studies have also reported that the upregulation levels of miR-148a-3p and miR-1247-3p in EO-CRC are higher than those in LO-CRC, while the expression level of miR-326 is downregulated. Functional analysis of these miRNAs revealed that alterations in their expression levels may lead to dysregulation of metabolic pathways and disorders in tissue morphogenesis, thereby promoting epithelial-mesenchymal transition. Tumor cells can meet the increased demands of growth and proliferation through extensive metabolic reprogramming and by competing with surrounding cells for essential nutrients in the microenvironment. 63 However, research on miRNAs in EO-CRC remains relatively limited. Given the differential expression of miRNAs in various types of CRC, future studies should intensify research in this area to promote the integration of miRNAs with fecal occult blood tests, which holds promise as a powerful biomarker for cancer detection and monitoring disease progression.
Metabolomics
Previous studies have identified certain differences in the metabolomics profiles of patients with EO-CRC and LO-CRC. One study analyzed plasma samples from both patients with EO-CRC and LO-CRC, revealing through lipidomic profiling that the levels of PC O-38:7, PC 34:2, Hex2Cer, LPC 16:0/0:0, and PC 36:3 in plasma were elevated in EO-CRC patients. Additionally, significant differences were observed in polar metabolomic differences between the EO-CRC and LO-CRC groups. The levels of aminoadipate, L-lysine, L-glutamic acid, choline, 2-aminomuconic acid, and L-tyrosine were increased in the EO-CRC group, while the levels of nicotinamide, acetyl-L-carnitine, L-threonine, 4,6-quinolinediol, 2-aminosuccinamate, uridine, urea, cytosine, and uracil were elevated in the LO-CRC group.64,65 EO-CRC cases exhibited higher levels of amino acids (eg, lysine, glutamate, and tyrosine) may reflect the demands of rapid cancer cell proliferation. For instance, the increase in L-lysine and L-glutamate might support tumor cell growth and protein synthesis. The increase in metabolites such as nicotinamide and uracil in LO-CRC may be associated with the enhanced DNA repair and cellular stress response in LO-CRC, as previously discussed. The increase in acetyl-L-carnitine may be related to the regulation of mitochondrial function and energy metabolism, which could affect the survival and drug resistance of tumor cells. In another analysis of differential metabolite abundance conducted by Farha et al. citrate exhibited a significant difference between the two groups (odds ratio = 21.8, FDR P = 0.04), with higher citrate levels observed in LO-CRC compared to EO-CRC. 66 Citrate plays a crucial role in cellular metabolism and is closely associated with the tricarboxylic acid (TCA) cycle, which influences cellular energy production and metabolic regulation. Therefore, differences in citrate levels between EO-CRC and LO-CRC patients may reflect distinct regulatory mechanisms in the metabolic pathways of these two cancer types. These metabolic differences provide potential targets for early detection and the development of tailored therapeutic strategies for EO-CRC and LO-CRC. For instance, monitoring the levels of specific lipids and metabolites in plasma could aid in early diagnosis and risk assessment. Furthermore, pharmacological interventions that target metabolic pathways may emerge as novel therapeutic approaches for both types of cancer, particularly for patients with specific metabolic profiles.
Although EO-CRC and LO-CRC share many key molecular drivers, some sequence differences remain evident. The molecular characteristics and drivers underlying EO-CRC and LO-CRC are not yet fully understood, making them a focal point for ongoing research.
In Clinical Characteristics
Clinical Symptoms and Disease Staging
EO-CRC and LO-CRC differ in clinical manifestations. First, variations exist in symptoms and disease staging at the time of initial diagnosis. Because individuals aged 20-49 years are not typically included in routine CRC screening, they often seek medical attention due to symptoms such as blood in the stool, changes in bowel habits, and wasting. As a result, EO-CRC is often diagnosed at Stage III or Stage IV. 67 Second, EO-CRC is associated with a higher incidence of abdominal pain, abdominal heaviness, and palpable abdominal masses. Patients with EO-CRC also tend to exhibit elevated serum glycoantigen 19-9 levels, but have lower rates of comorbidities such as hypertension, diabetes mellitus, and cardiovascular disease. Furthermore, EO-CRC is linked to lower serum carcinoembryonic antigen (CEA) levels compared to LO-CRC.
Tumor Location
Studies indicate that EO-CRC tumors primarily develop in the distal colon and rectum. 68 Willauer et al. observed that CRC tumors in the left hemicolon were more prevalent among younger patients than those aged >50 years, suggesting a possible correlation between age and tumor location. 69 Ascending colon cancer is biologically distinct from descending colon and rectal cancer. In older adults, right and left hemi-colon cancers are recognized as distinct diseases, with well-established diagnostic and therapeutic strategies. However, research on early-onset right- and left-sided colon cancer remains limited, highlighting the need for further investigation.
Pathologic Features
Evidence suggests that EO-CRC exhibits more aggressive histopathologic characteristics. Compared with LO-CRC, EO-CRC has a higher proportion of poorly differentiated tumors, Stage III disease, T4 and N2 classifications, and preoperative CEA positivity. Additionally, EO-CRC tumors are more likely to demonstrate neural infiltration. In addition, patients with EO-CRC undergo a higher number of intraoperative lymph node dissections and are more likely to receive chemotherapy and neoadjuvant radiotherapy. 70 Extensive national and international data indicate that younger patients more frequently present with ulcerative tumors, mucinous carcinomas, and signet-ring cell carcinomas. EO-CRC is also characterized by larger tumor size, advanced TNM staging, increased vascular and neural infiltration, higher rates of distant metastases, and a lower proportion of cases without lymph node involvement.17,71
Prognosis
The risk factors and prognostic differences between EO-CRC and LO-CRC remain controversial. As discussed in Section 4, EO-CRC is more commonly associated with perineural infiltration, poor differentiation, mucinous cell carcinoma, and signet-ring cell morphology. Additionally, EO-CRC tumors are more aggressive and present at later TNM stages, indicating poor tumor biology and an unfavorable oncologic prognosis. However, findings across studies are inconsistent. For example, Kanter’s study found no significant difference in disease-free survival and overall survival (OS) between EO-CRC and LO-CRC. while Andrea et al. reported better OS in EO-CRC compared to LO-CRC.72,73 Moreover, we found that the prognosis of EO-CRC varies across different age groups, races/ethnicities, and sex. To better understand these differences, subgroup stratification is necessary for further in-depth analysis.
Different Age Groups: 20-39 vs 40-49 vs >50 Years
A 2020 cohort study based on patients with EO-CRC in England showed that the incidence rates of both proximal and distal tumors were higher in the 20-39 age group than in the 40-49 age group, and were continuing to rise. 74 Compared to EO-CRC patients aged 40-49, those aged 20-39 were more likely to present with gastrointestinal symptoms such as abdominal pain and nausea, while those over 40 or more frequently exhibited systemic symptoms such as anemia and decreased appetite. 75 Due to relatively lower awareness of CRC among young people, early symptoms are often overlooked and attributed to common gastrointestinal disorders or improper diet, prolonging the time from the onset of initial symptoms to diagnosis. In a retrospective study conducted by Chen et al. involving 485 patients with CRC, the median time to diagnosis for patients with EO-CRC was 128 days, whereas for patients with CRC over 50 years old, it was only 79 days. 76 This delay in initial diagnosis among young patients may have allowed the tumor to metastasize or invade surrounding tissues during this period, increasing treatment difficulty and potentially worsening prognosis. However, some studies suggest that patients with EO-CRC receive more aggressive surgical and perioperative treatments compared to patients with LO-CRC,50,73 which may explain why the prognosis between the two groups does not differ significantly.
Different Sex
Notably, Bingyi Ren et al. found that female patients with EO-CRC had better OS than male patients. However, this sex-related prognostic difference was not observed in LO-CRC, leading to the hypothesis that sex hormones may influence EO-CRC outcomes. 77 Females experience a sharp decline in estrogen levels during menopause, typically around the age of 50. The estrogen receptor ERβ is believed to exert anti-tumor effects through multiple mechanisms, suggesting that male sex may be an independent risk factor for EO-CRC. A retrospective study comparing patients with EO-CRC, LO-CRC, and those without cancer indicated that EO-CRC was more prevalent in males, supporting this hypothesis. 78 Therefore, in EO-CRC, sex plays a significant role in prognosis. Future research should further explore the specific mechanisms by which sex hormones affect EO-CRC and how personalized prevention and treatment strategies can be developed based on sex differences. This may help improve the prognosis of patients with EO-CRC, particularly by enhancing treatment outcomes for male patients.
Different Races/Ethnicities
In our epidemiological trend analysis, we observed a certain geographical pattern in the incidence of early-onset colorectal cancer, which prompted us to examine whether racial and ethnic differences affect the prognosis of EO-CRC. One study found that EO-CRC was more common among Black and Asian individuals. 78 Additionally, another study reported that the 5-year relative survival rate for Black patients with EO-CRC was lower than that for White patients, suggesting that race may also be a risk factor for EO-CRC. 79 Furthermore, a cohort study involving Asian Americans (including Chinese, Filipino, Japanese, Korean, South Asian, Southeast Asian, and other Asians), Hispanic, Native Hawaiian or other Pacific Islander, non-Hispanic American Indian or Alaska Native, non-Hispanic Black or non-Hispanic White individuals found that, non-Hispanic Black individuals had a higher likelihood of death compared to other ethnic groups. When the Asian American population was further disaggregated, Southeast Asian individuals were observed to have the highest likelihood of death, reinforcing findings from previous studies. 80 These findings indicate that the incidence and prognosis of EO-CRC vary significantly across different racial and ethnic groups. The incidence rates are higher among Black and Asian populations, with particularly elevated mortality risks observed in non-Hispanic Black and Southeast Asian individuals, suggesting that racial and ethnic backgrounds may play a significant role in the pathogenesis and disease progression of EO-CRC.
Discussion
Through a comprehensive and multidimensional analysis of the differences between EO-CRC and LO-CRC, we found that the increasing incidence of EO-CRC may be associated with unhealthy lifestyles, obesity, antibiotic use, and altered intestinal flora. At the molecular level, EO-CRC is frequently characterized by TP53 mutations, CIMP positivity, and MSI-H, whereas BRAF mutations are less common. Clinically, compared to LO-CRC, EO-CRC presents with more severe symptoms at the initial visit and is often diagnosed at an advanced stage. EO-CRC tumors predominantly occur in the left hemi-colon and rectum, with a higher incidence of poorly differentiated adenocarcinoma, mucinous adenocarcinoma, and signet-ring cell carcinoma, all of which exhibit a high degree of invasiveness. There are notable differences in OS and cancer-specific survival between patients with EO-CRC and LO-CRC, which are associated with factors such as age of onset, race, and sex. However, while EO-CRC exhibits greater aggressiveness, its prognosis is not necessarily worse, potentially due to higher rates of surgery, radiotherapy, and chemotherapy. 50 Future research should further investigate the mechanisms underlying these differences to optimize diagnostic and therapeutic strategies for EO-CRC.
Given the more aggressive nature of EO-CRC, it is essential to optimize CRC screening strategies for young adults. Each country should determine the appropriate starting age for CRC screening based on the onset age of EO-CRC in their local populations, potentially lowering it to 45 or even younger, to detect potential lesions at an earlier stage. In addition, enhancing disease awareness among younger populations is essential. It is important to reverse the misconception that CRC is solely a disease of the elderly, and to encourage active participation in health check-ups and timely medical consultations when clinical symptoms appear to avoid delays in diagnosis and treatment. Early prevention targeting risk factors such as obesity, consumption of red and processed meat, and a family history of CRC is also necessary. The use of aspirin has also been found to be associated with a reduced risk of EO-CRC onset, and it may become an effective protective measure against EO-CRC in the future. 81
Despite significant advancements in the prevention, screening, and treatment of CRC over the past few decades, the current approach is not well-suited to address EO-CRC. 82 Future research should intensify efforts to identify potential microbiome and transcriptomic biomarkers associated with EO-CRC. To improve screening uptake among young individuals, it is essential to promote non-invasive and convenient screening methods, such as CRC liquid biopsy techniques or multi-target stool FIT-DNA tests, which can enhance both acceptance and compliance. Additionally, integrating genomic information, including mutations in genes such as APC, TP53, KRAS, PIK3CA, and SMAD4, metabolomic data, such as changes in plasma amino acid levels (lysine, glutamic acid, and tyrosine), and differences in urea levels, is crucial for developing risk prediction models that combine genomics, metabolomics, and microbiome data. Moreover, given the close relationship between the composition and diversity of the gut microbiota and the development of CRC, as well as the significant potential of gut microbiota in the treatment of colorectal cancer, large-scale microbiome studies should be conducted to identify specific microbial markers for EO-CRC, develop corresponding diagnostic kits, establish an analytical platform that integrates microbial markers with clinical data, and explore the efficacy of Fecal Microbiota Transplantation (FMT) in the treatment of EO-CRC.83,84
Conclusion
This study presents a multidimensional analysis of the characteristics of EO-CRC and LO-CRC, revealing that EO-CRC is associated with factors such as obesity, dietary habits, antibiotic misuse, and alterations in the gut microbiota. It also shows differences from LO-CRC across various omics aspects, including genomics, transcriptomics, and metabolomics. Clinically, EO-CRC presents more severe symptoms and exhibits greater invasiveness. Based on epidemiological trends across different regions, ethnicities, and genders, it is advisable to appropriately lower the screening age for colorectal cancer, enhance disease awareness and early prevention efforts among younger populations, promote non-invasive screening methods, integrate multi-omics data to construct predictive models, and explore the efficacy of FMT in the treatment of EO-CRC. These efforts will contribute to enhancing the early diagnosis rate of EO-CRC, improving prognosis, and optimizing treatment protocols.
Footnotes
Acknowledgements
Ethics Statement
This manuscript is a review article and does not involve a research protocol requiring approval by the relevant institutional review board or ethics committee.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.