
Abstract
Introduction
Colorectal cancer (CRC) ranks as the third most diagnosed malignancy and the second leading cause of cancer death in the US. 1 It is expected that there will be approximately 152 810 new cases and 53 010 deaths due to CRC in 2024. 1 Due to increased screening and a decrease in risk factors exposure, the overall incidences of CRC have been declining by 3-4% annually during the 2000s and by 1% from 2011-2019.2,3 Conversely, the incidences of early-onset CRC increased in the US since the 1990s.4,5 Consequently, early-onset CRC has emerged as a leading cause of mortality among individuals younger than 50. 2
In May 2018, the American Cancer Society (ACS) recommended that CRC screening begin at age 45 for individuals at average risk. 6 In 2020, the US Preventive Services Task Force (USPSTF) also proposed that CRC screening should include individuals aged 45-49. 7 However, there are concerns regarding this recommendation, including the significant expansion of the target population compared to the relatively small rise in cases of early-onset CRC, as well as the high costs associated with colonoscopy screening.8-10 Moreover, the recommended colonoscopy screening specifically targets individuals aged 45-49 years and primarily focuses on adenocarcinoma, the main histological type of early-onset CRC. However, the recent trends in early-onset CRC adenocarcinoma incidence in this specific age group have not been well characterized.11-15
This study aims to determine the temporal changes in incidences and case numbers of early-onset CRC, particularly adenocarcinoma, by sex, race, and anatomic sites in individuals aged 45-49, using a national database capturing the entire population of the US. The findings will help identify high-risk individuals and provide better insights into the rationale behind the new screening recommendation.
Patients and Methods
Early-onset CRC cancer patients were obtained from the National Program of Cancer Registries and Surveillance, Epidemiology and End Results Program (NPCR-SEER) Database (2001-2019), 16 which covers 100% of the population for all 50 states and the District of Columbia in the US. Sex, age, race, tumor anatomic site, and histological types of early-onset CRC patients were extracted from the database. Race was grouped into Non-Hispanic White (NHW), Non-Hispanic Black (NHB), Non-Hispanic American Indian and Alaska Natives (AIAN), Non-Hispanic Asians/Pacific Islanders (API), Hispanics, and unknown. The tumor anatomic site was grouped into the proximal colon (C18.0 cecum, C18.2 ascending colon, C18.3 Hepatic flexure, and C18.4 transverse colon), distal colon (C18.5 splenic flexure, C18.6 descending colon, and C18.7 Sigmoid colon), and rectum (C19.9 rectosigmoid junction and C20.9 rectum) based on International Classification of Diseases for Oncology (ICD-O-3) codes. In contrast, cancer in the appendix (C18.1) was excluded. The ICD-O-3 morphology codes for adenocarcinoma were 8140/3, 8141/3, 8143/3, 8144/3, 8210/3, 8211/3, 8213/3, 8220/3, 8221/3, 8255/3, 8260-8265/3, 8310/3, 8323/3, 8440/3, 8460/3, 8470/3, 8472/3, 8480-8482/3, 8570/3, 8574/3 and 8576/3; and for carcinoids included 8013/3, 8240/3, 8241/3, 8243/3, 8244/3, 8245/3, 8246/3, and 8249/3. 12 Since all data were de-identified, human investigation approval was unnecessary for this project.
Statistical Analysis
Categorical data was analyzed using the Chi-square test. We used SEER*Stat version 8.4.1 (National Cancer Institute) to calculate the age-adjusted incidence rates (AAIR) per 100 000 population by sex, age, race, anatomic site, and histological types. The AAIR was age-adjusted to the 2000 US standard population. Tiwari et al’s 2006 modifications were applied to calculate the confidence interval (CI). 17 The Joinpoint Regression Program (The National Cancer Institute) was used to generate incidence graphs and calculate the annual percent change (APC) using the least square method. The change in the case number of early-onset CRC from 2001 to 2019 was analyzed using the linear regression analysis (SAS 9.4, Raleigh, NC). For all analyses, two-sided P < .05 was deemed as statistically significant.
Results
Characteristics of Early-Onset Colorectal Cancer Diagnosed During 2001-2019
Characteristics of Early-Onset Colorectal Cancer Patients Aged 45-49 by Anatomical Site Diagnosed During 2001-2019.

Abbreviations: AIAN, Non-Hispanic American Indian and Alaska Native (AIAN); API, Non-Hispanic Asian or Pacific Islander; NHB, Non-Hispanic black; NHW, Non-Hispanic white.
Trends in Age-Adjusted Incidence Rates and Case Numbers for Proximal, Distal Colon, and Rectal Adenocarcinoma in Individuals Aged 45-49 During 2001-2019
The incidence of proximal colon adenocarcinoma displayed no significant change with an APC of (−0.3, P = .352) from 2001-2010 and then a slow increase with an APC of 0.7 (P = .032) only during 2010-2019 (Figure 1A and Supplementary Table S2). Conversely, the incidence of distal colon adenocarcinoma increased with an APC of 1.3 (P < .001) from 2001 to 2019. Additionally, rectal adenocarcinoma incidence increased at APCs of 1.2 (P = .005) from 2001 to 2011 and then 2.1 (P = .001) from 2011 to 2019 (Figure 1A and Supplemental Table S2). Over the same period, the AAIRs increased from 7.2 per 100 000 to 7.5 for proximal colon adenocarcinoma, 8.4 to 10.1 for distal colon adenocarcinoma, and 9.1 to 12.1 for rectal adenocarcinoma. Notably, the US population of individuals aged 45-49 years was constantly over twenty million from 2001 to 2019 (Supplemental Figure S1). Temporal Changes in Age-Adjusted Incidence Rates (A) and Case Numbers (B) of Early-Onset Proximal, Distal Colon, and Rectal Adenocarcinoma in Individuals Aged 45-49 Years During 2001-2019. APC, Annual Percent Change. * Indicates the Significant Change.
The number of cases did not significantly change for proximal colon adenocarcinoma(P = .237) but there was a significant increase of 17 cases per year for distal colon adenocarcinoma (P < .001) and 27 cases annually for rectal adenocarcinoma (P < .001) throughout the period from 2001 to 2019 (Figure 1B).
Changes in the Age-Adjusted Incidence Rates and Case Numbers for Proximal, Distal Colon, and Rectal Adenocarcinoma by Gender in Individuals Aged 45-49 Years During 2001-2019
The incidence rates of early-onset proximal colon adenocarcinoma in males showed a non-significant decrease (APC = −0.2, P = .735) from 2001 to 2008, followed by a significant increase from 2008 to 2019 at an APC of 0.9 (P = .006). In females, there was a non-significant decrease (APC = −0.4, P = .073) from 2001 to 2010 and then a non-significant increase (APC = 0.4, P = .447) from 2010 to 2019 (Figure 2A and B and Supplementary Table S2). For distant colon adenocarcinoma, the incidence rates significantly increased in males at APCs of 0.9 (P = .021) during 2001-2011 and 2.6 (P < .001) during 2011-2019. In females, the rates stabilized from 2001-2011, followed by a significant increase at an APC of 2.2 (P < .001) from 2011 to 2019. The incidence rates of rectal adenocarcinoma rose continuously throughout the entire study period in males, while for females, the increase occurred only from 2010 to 2019 (Figure 2A and B and Supplementary Table S2). Temporal Trends of Age-Adjusted Incidence Rate and Case Number of Early-Onset Proximal, Distal Colon, and Rectal Adenocarcinoma in Individuals Aged 45-49 Years by Gender During 2001-2019. Colorectal Cancer Incidences in Males (A) and Females (B) Colorectal Cancer Case Numbers in Males (C) and Females (D). APC, Annual Percent Change. * Indicates the Significant Change.
In terms of case numbers, the cases of early-onset proximal colon adenocarcinoma in males did not significantly increase in males (P = .167) but showed a significant decrease by 4 cases annually in females (P = .001) (Figure 2C and D). The case numbers of distal colon adenocarcinoma significantly increased from 840 in 2001 to 1050 in 2019 in males (an average increase of 13 cases per year, P < .001), and from 892 in 2001 to 1002 in 2019 in females (an average increase of 4 cases annually, P = .028). Additionally, the case numbers for rectal adenocarcinoma increased significantly by an average rise of 18 cases per year in males (P < .001) and 9 cases per year in females (P < .001).
Changes in the Age-Adjusted Incidence Rates and Case Number for Proximal Colon Adenocarcinoma by Sex and Race in Individuals Aged 45-49 Years During 2001-2019
There was a slow yet significant increase in the incidences of proximal colon adenocarcinoma in NHW males (APC = 0.9, P < .001). On the contrary, the incidences significantly decreased in NHB females (APC = −1.0, P = .008). No significant changes were observed in NHW females, NHB males, API males and females, and Hispanic males and females (Figure 3A and B and Supplementary Table S3). NHB individuals still had the highest incidences of proximal colon adenocarcinoma, followed by NHW, in both males and females. Temporal Trends of Age-Adjusted Incidence Rate and Case Number of Early Onset Proximal Colon Adenocarcinoma in Individuals Aged 45-49 Years by Gender and Race During 2001-2019. Proximal Colon Adenocarcinoma Incidences in Males (A) and Females (B) Proximal Colon Adenocarcinoma Case Numbers in Males (C) and Females (D) APC, Annual Percent Change; API, Non-Hispanic Asian or Pacific Islander; NHB, Non-Hispanic Black; NHW, Non-Hispanic White. * Indicates the Significant Change.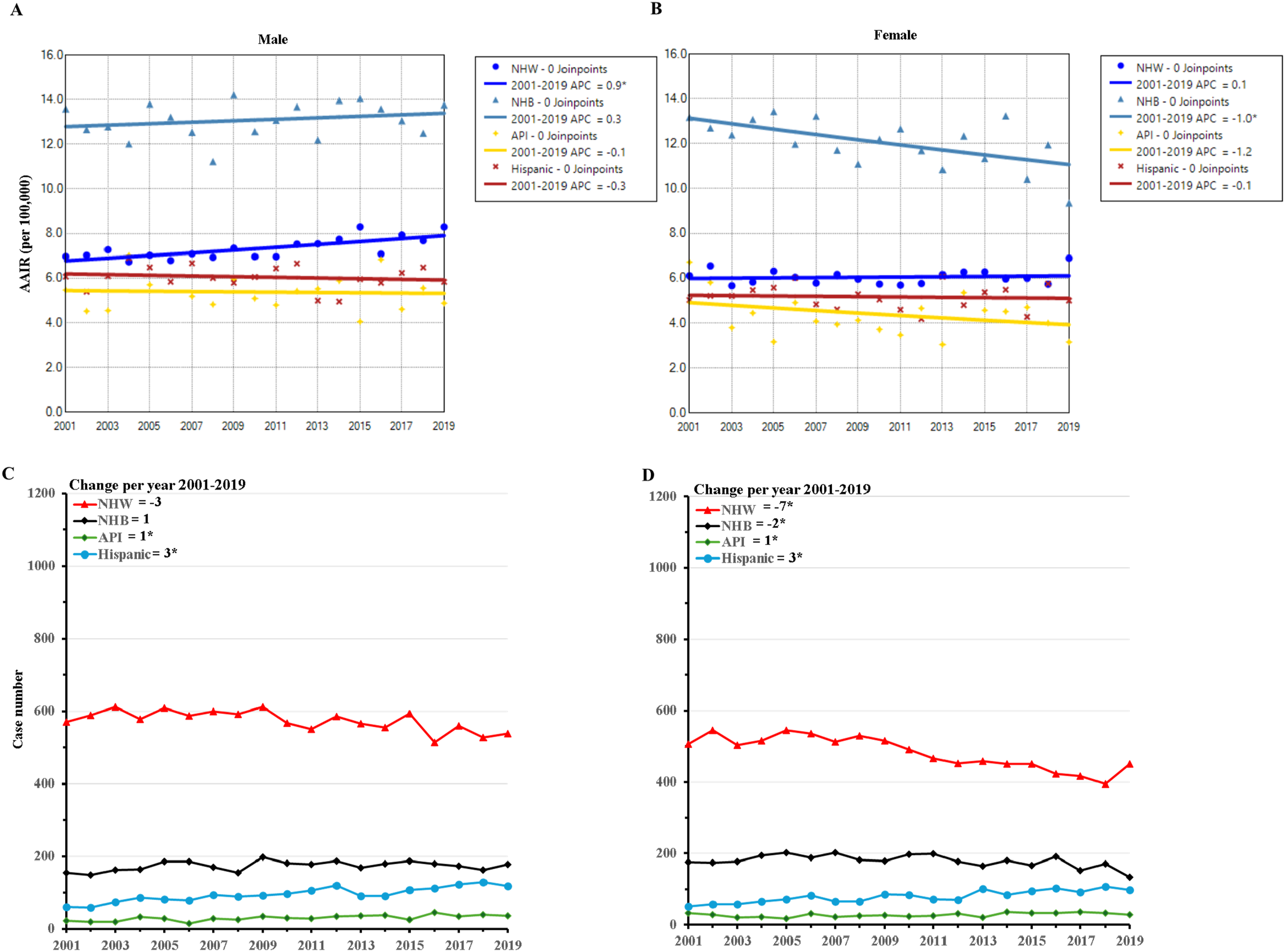
The case numbers of proximal colon adenocarcinoma significantly decreased in NHW males (averaging 3 fewer cases annually, P = .002) and females (averaging seven fewer cases annually, P < .001), and NHB females (averaging two fewer cases annually, P = .026). However, there was no significant change in the case numbers for NHB males. The case numbers were much lower but significantly increased in API and Hispanic males and females (Figure 3C and D). Due to the small number of cases in AIAN individuals, incidences of CRC within this age group for many individual years were not shown in the database and, therefore, were not presented in this study.
Changes in Age-Adjusted Incidence Rates and Cancer Numbers for Distal Colon Adenocarcinoma by Sex and Race in Individuals Aged 45-49 Years During 2001-2019
There was a significant increase in the incidence of distal colon adenocarcinoma in NHW males during the study period (APC = 2.4, P < .001). In NHW females, the incidence remained stable from 2001 to 2008 but significantly increased thereafter (APC = 2.2, P < .001). Conversely, the incidence significantly decreased in NHB females from 2001 to 2019 (APC = −1.3, P = .012). NHB males, API males and females, and Hispanic males and females had no significant change in the incidences of distal colon adenocarcinoma during the study period (Figure 4A and B and Supplementary Table S4). NHB still had the highest incidence of distal colon adenocarcinoma in males and females in earlier years, but NHW males and females exceeded NHB counterparts in recent years. Temporal Trends of Age-Adjusted Incidence Rate and Case Number of Early Onset Distal Colon Adenocarcinoma by Gender and Race in Individuals Aged 45-49 Years During 2001-2019. Distal Colon Adenocarcinoma Incidences in Males (A) and Females (B) Distal Colon Adenocarcinoma Case Numbers in Males (C) and Females (D) APC, Annual Percent Change; API, Non-Hispanic Asian or Pacific Islander; NHB, Non-Hispanic black; NHW, Non-Hispanic White. * Indicates the Significant Change.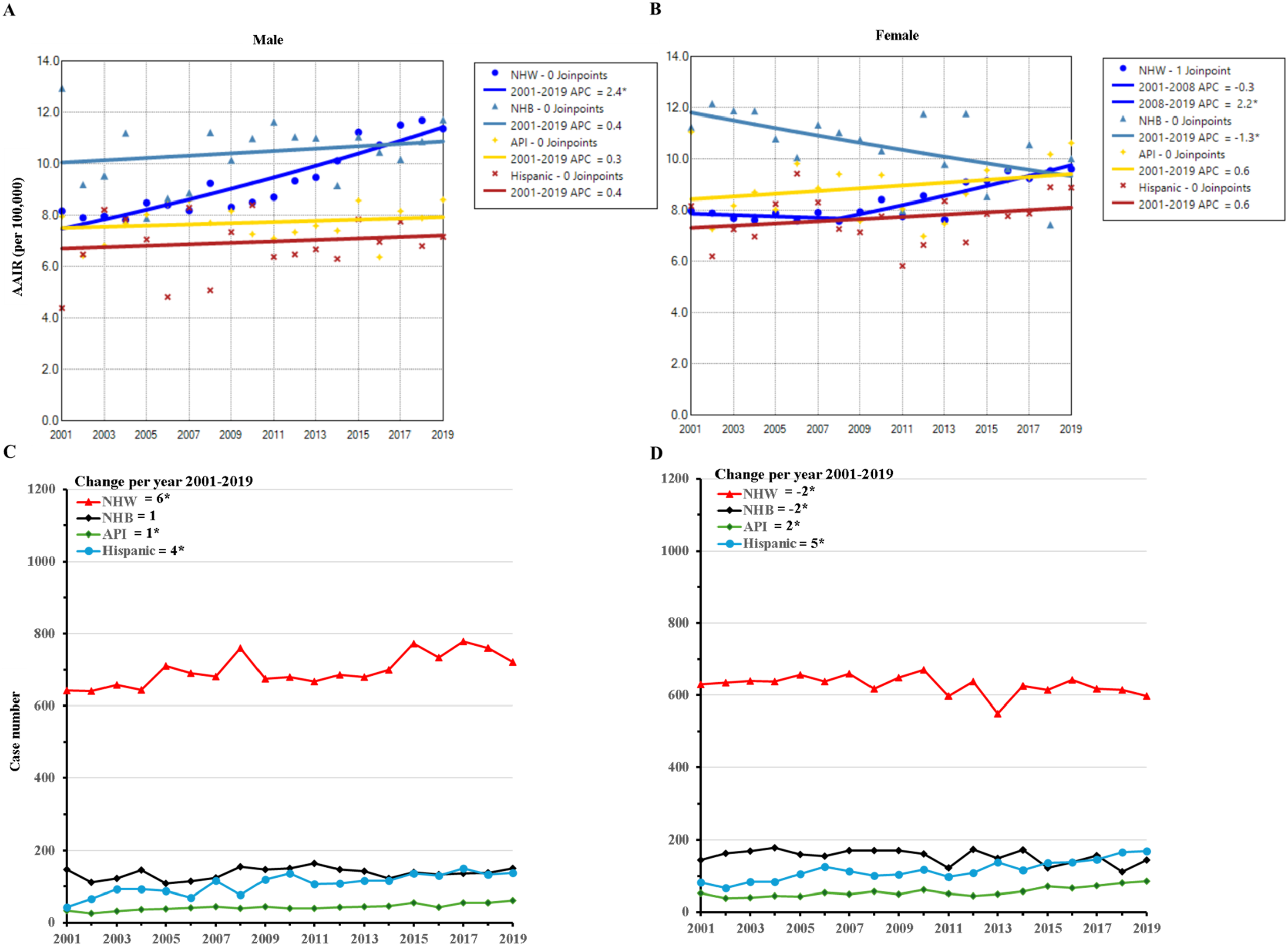
The case numbers significantly increased in NHW males, API males and females, and Hispanic males and females, while the case numbers decreased for NHB females. There were no significant changes in case numbers for NHW females and NHB males (Figure 4C and D).
Changes in the Age-Adjusted Incidence Rates and Case Numbers for Rectal Adenocarcinoma by Sex and Race in Individuals Aged 45-49 Years During 2001-2019
The incidences of rectal adenocarcinoma significantly increased in NHW males with an APC = 1.9 (P = .001) during 2001-2012 and then an APC of 3.2 (P = .001) during 2012-2019. NHW females also had a significant increase in incidences, with an APC = 2.0 (P < .001) during 2001-2019. Additionally, we observed increased incidences with an APC of 1.4 (P = .007) in API males and an APC of 1.3 (P = .001) in Hispanic males during 2001-2019. NHB males displayed no significant change in rectal adenocarcinoma incidences during 2001-2008 but then a significant decrease (APC = −1.8, P = .024) between 2008 and 2019. The incidences did not significantly change in NHB, API females, and Hispanic females (Figure 5A and B and Supplementary Table S5). NHW males and females had the highest incidences in recent years. Conversely, male and female NHB had the lowest incidences of rectal carcinoma in recent years. Temporal Trends of Age-Adjusted Incidence Rate and Case Number of Early-Onset Rectal Adenocarcinoma by Gender and Race in Individuals Aged 45-49 Years During 2001-2019. Rectal Adenocarcinoma Incidences in Males (A) and Females (B) Rectal Adenocarcinoma Case Numbers in Males (C) and Females (D) APC, Annual Percent Change; API, Non-Hispanic Asian or Pacific Islander; NHB, Non-Hispanic Black; NHW, Non-Hispanic White. * Indicates the Significant Change.
The number of rectal adenocarcinoma cases significantly increased in NHW males, API males and females, and Hispanic males and females. However, there was no significant changes in the case numbers for NHW females, NHB males, and NHB females (Figure 5C and D).
Changes in the Age-Adjusted Incidence Rates and Case Numbers for Carcinoids and Other Histological Types of Colon Cancer in Individuals Aged 45-49 Years During 2001-2019
Due to their low incidences, we obtained the incidences of carcinoids and other histological types of combined proximal and distal colon cancer. Our results indicated that the incidences of colon carcinoids (P = .485) were not significantly changed, whereas other histological types of colon cancer significantly decreased (APC = −1.2, P < .001) from 2001 to 2019 (Figure 6A and Supplementary Table S6). Temporal Trends of Age-Adjusted Incidence Rate and Case Number of Early-Onset Colon Carcinoids and Cancer of Other Histological Types in Individuals Aged 45-49 Years During 2001-2019. Incidences of Early-Onset Colon Carcinoids and Cancer of Other Histological Types (A) and Case Numbers of Early-Onset Colon Carcinoids and Cancer of Other Histological Types (B) APC, Annual Percent Change. * Indicates the Significant Change.
The case numbers of colon carcinoids remained around 100 or less (P = .912) from 2001 to 2019. In contrast, the number of cases for other histological types of colon cancer significantly decreased by an average of 3 fewer cases annually (P < .001) throughout the study period (Figure 6B).
Changes in the Age-Adjusted Incidence Rates and Case Numbers for Rectal Carcinoids and Cancer of Other Histological Types in Individuals Aged 45-49 Years During 2001-2019
The incidences of rectal carcinoids exhibited a more rapid increase, with an APC of 5.8 (P = .004) from 2001 to 2006, followed by an APC of 2.2 (P < .001) from 2006 to 2019. The incidences rose from 0.9 per 100 000 in 2001 to 1.5 in 2019, or by an average APC of 3.2 (P < .001). In contrast, there were no significant changes in the incidences of other histological types of rectal cancer (Figure 7A and Supplementary Table S6). Temporal Trends of Age-Adjusted Incidence Rate and Case Number of Early-Onset Rectal Carcinoids and Cancer of Other Histological Types in Individuals Aged 45-49 Years During 2001-2019. Incidences of Early-Onset Rectal Carcinoids and Cancer of Other Histological Types (A) and Case Numbers of Early-Onset Rectal Carcinoids and Cancer of Other Histological Types (B) APC, Annual Percent Change; API. * Indicates the Significant Change in APC.
Additionally, the case numbers of rectal carcinoids significantly increased, with an average of 6 more cases annually (P < .001). The case number increased from 177 in 2001 to 295 in 2019. However, there was no significant changes in case numbers for other histological types of rectal cancer (Figure 7B).
Discussion
This study utilized the database covering the entire population to determine the incidences and case numbers of CRC, particularly its adenocarcinoma, among individuals aged 45-49 years in the US from 2001 to 2019. Our data revealed that the case numbers of proximal colon adenocarcinoma did not significantly change during the study period, while the incidences significantly increased from 2010 to 2019. Additionally, the incidences and case numbers mildly but significantly increased for distal colon adenocarcinoma and more rapidly increased for rectal adenocarcinoma throughout the study period. The increased incidences predominately occurred in NHW. Moreover, incidences and case numbers of carcinoids increased in the rectum but not in the colon.
Our study showed different trends in incidences and case numbers of proximal and distal colon cancer in individuals aged 45-49 years during 2001-2019. There was a slowly increased incidence of proximal colon adenocarcinoma only during 2010-2019, without significant case numbers during the entire study period. On the other hand, the incidences (average APC of 1.3) and case numbers (by an average of 17 more per year) significantly increased for distant colon adenocarcinoma. It is noted that adenocarcinoma accounted for as high as 93.9% of early-onset proximal colon cancer and 96.5% of early-onset distal colon cancer. Accordingly, the incidences and case numbers of colon carcinoids and other histological types were low without a significant increase. Similar to this finding, a previous study observed no change in the case number of proximal colon adenocarcinoma in those aged 20-49 years from 2001-2002 to 2017-2018. 13 This set of data reveals that the increases in the incidences and case numbers were minimal for proximal colon adenocarcinoma and mild for distal colon adenocarcinoma in individuals aged 45-49 years from 2001 to 2019.
In contrast, the incidences and case numbers of rectal adenocarcinoma increased more rapidly. The average APC was 1.6 for the increased incidences, and the average 27 annual increase in case numbers during the entire study period. In this age group, adenocarcinoma and carcinoids accounted for 84.6% and 9.7% of early-onset rectal cancer, respectively. Rectal carcinoids displayed significantly increased incidences at AAPC of 3.2 and case number by six annually. Without histological classification, one earlier study reported no significant change in the incidences of proximal cancer and significant increases in incidences of distal colon (AAPC of 0.87) and rectal cancer (AAPC of 1.5) in this age group during 2001-2016. 15
Given the population of over twenty million, it is arguable that the costive colonoscopy should be adopted non-selectively for early-onset CRC screening for all individuals aged 45-49 years. Notably, nearly half of early-onset CRC cases occur in this age group. Adenocarcinoma is the main histological type of early-onset CRC and the primary histological type targeted by colonoscopy screening. With the continuous rise in incidences of proximal, distal colon, and rectal adenocarcinoma, and in cases of distal colon and rectal adenocarcinoma, it makes sense to screen those at average risk in this age group.6,18
This study revealed that the increased incidences of early-onset colorectal adenocarcinoma mainly occurred in NHW among individuals aged 45-49. NHW males had an increased incidence of proximal colon adenocarcinoma, and both NHW males and females had increased distal and rectal adenocarcinoma. Hispanic and API males only had increased incidences of rectal carcinoma. In contrast, NHB females had decreased incidences of proximal and distal colon adenocarcinoma. NHB males even displayed a reduced incidence of rectal adenocarcinoma from 2008 to 2019. A very recent study also reported NHW males had increased incidences of early-onset proximal colon adenocarcinoma, and NHW males and females had increased incidences of early onset distal colon and rectal adenocarcinoma among those aged 20-49 years from 2001-2002 to 2017-2018. 13 Though many other studies consistently reported increased incidences of early-onset CRC among NHW, the findings for NHB and other races were inconsistent.2,11,15,19 This inconsistency arises from different classifications by age group, gender, histological type, and anatomic site. These varying results suggest that early-onset CRC incidences differ across racial and age groups, emphasizing the need to identify high-risk individuals within their respective age brackets.
The incidence rates of early-onset CRC varied by anatomic site and race within this specific age group during the study period. NHB males and females had the highest incidence rates of proximal colon adenocarcinoma, followed by NHW males and females. However, the incidences of early-onset distal colon adenocarcinoma in NHW exceeded that of NHB patients in recent years. The incidences of rectal adenocarcinoma were the highest in NHW males and females compared to other races. This pattern of early-onset CRC incidences among different anatomical sites and races has been noted in previous studies.12-15 Interestingly, both male and female NHB have shown the lowest incidences of rectal adenocarcinoma in recent years within this age group. These results indicated that NHB males and females remained at the highest risk for proximal colon adenocarcinoma, while NHW have started to experience the highest risk for distal colon and rectal adenocarcinoma among those aged 45-49 years.
The rising incidences of early-onset CRC since the 1990s have been linked to the birth cohort effect.4,20 In addition to this, numerous other risk factors have been implicated in the development of early-onset CRC.11,13 These factors include obesity, 21 higher body mass index (BMI), 22 cigarette smoking and alcohol consumption,23-26 poor-quality diets,27-29 sedentary lifestyle, 30 high stress, 31 and a dysbiosis of the gut microbiome.32,33 Early-onset CRC often has genetic determinants or a family history.34-39 Socioeconomic inequities also contribute to disparities in exposure to risk factors, health behavior, and healthcare access, all of which are related to the risks of CRC.3,31 However, more research is needed to understand the causes of the distinct patterns of CRC incidences and case numbers among different genders, histological types, anatomical sites, and racial groups in individuals aged 45-49 years.
The study has several limitations. It is unknown whether these patients were diagnosed due to screening by colonoscopy or other ways. There is a lack of information on individual-level risk factors such as diet, obesity, physical activity, and lifestyle. Information about family history or genetic background for these patients was not available. The database does not include socioeconomic information, which is essential for studying the causes of differences in early-onset CRC incidences and case numbers observed in this study. The strengths of our study include the use of a high-quality database that encompasses the entire U.S. population and is updated through the year 2019.
In conclusion, this study reveals increasing incidences of CRC adenocarcinoma and rising case numbers of distal colon and rectal adenocarcinoma among individuals aged 45-49, with notable differences among genders and races at varied anatomical sites. Moreover, incidences and case numbers of carcinoids increased in the rectum but not in colon. Further research is necessary to understand the underlying causes of the differences and to find ways to reduce the incidence of early-onset CRC.
Supplemental Material
Supplemental Material - Temporal Trends in Colorectal Cancer Incidence and Case Numbers Among Individuals Aged 45-49 in the US During 2001-2019
Supplemental material for Temporal Trends in Colorectal Cancer Incidence and Case Numbers Among Individuals Aged 45-49 in the US During 2001-2019 by Chunmei Li, Tianle Chen, Huimin Chen, Bo Zhang, Bing Sun, Pengyang Zhou, Qiken Li, and Weiping Chen in Cancer Control
Footnotes
Statements and Declarations
Author Contributions
Weiping Chen and Chunmei Chen developed the concept and design. Chunmei Li and Tianle Chen acquire data and perform data analysis. Tianle Chen, Chunmei Li, and Weiping Chen drafted the manuscript. All authors had read and revised the manuscript for the final submission. Weiping Chen obtained funding and supervised the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Key Research and Development Project of Zhejiang Province (2023C04018, to Chen Weiping), Chinese Medical Science and Technology Project of Zhejiang Province (2021ZB030, to Chen Weiping) and Medical Science and Technology Project of Zhejiang Province (2021KY575, to Chen Weiping).
Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.