
Abstract
Introduction
Health and psychosocial outcomes are often interdependent for people with cancer and their informal caregivers. However, few studies have examined interdependence among U.S. Black patients and their caregivers. In this prospective study, we analyzed whether Black women with breast cancer and their caregivers demonstrated interdependence in depressive symptoms and other outcomes over time.
Methods
Patient and caregiver data were collected via telephone surveys at three timepoints (baseline, two months, four months). Actor-Partner Interdependence Models (random-intercept cross-panel models in Mplus) were used to analyze depressive symptoms (Center for Epidemiology Studies Depression scale; CES-D), physical and mental health quality of life, perceived social support, and health behaviors. We hypothesized patients and caregivers would demonstrate interdependence for these outcomes both cross-sectionally and over time.
Results
We enrolled 210 participants. All patients and 93% of caregivers identified as Black/African American; 70% of caregivers identified as female. Two-thirds (66%) of dyads did not live together. Mean baseline CES-D score was 15.0 (SD = 10.9) for patients and 11.9 (SD = 9.0) for caregivers. We did not find prospective interdependence for any outcomes. Dyad members were moderately correlated in overall levels (intercepts) of physical health quality of life (r = .25), mental health quality of life (r = .28), social support (r = .37), and health behavior scores (r = .33).
Conclusion
This study is one of the first longitudinal, dyadic examinations of outcomes for Black breast cancer patients and their informal caregivers. Although our hypothesis of prospective interdependence was not supported, we observed moderate correlations of overall levels of several measures. These results suggest that patients with lower social support, poor health behaviors, and worse quality of life may also have caregivers who could benefit from intervention.
Plain Language Summary
Keywords
Introduction
Clinicians and researchers have conceptualized cancer as a “family affair” affecting both patients and the people close to them.1-3 Intimate partners, family members, and friends often serve as informal caregivers for people with cancer and provide unpaid support along a variety of dimensions (tangible, emotional, and/or social).2,4,5 Dyadic research that analyzes both patients and informal caregivers or other partners has suggested that, in the context of cancer and other chronic diseases, health and psychosocial outcomes in patients and caregivers are often interdependent.6-11 A systematic review 12 found that, in heterosexual spousal dyads in which the female partner had breast cancer, depression in one member of the dyad is a risk factor for depression in the other; the authors note, however, that research in more diverse samples is needed. The observation that caregiver mental health is associated with patient mental health is consistent with theories of emotional contagion 13 and has led to the suggestion that screening and treating spouses of cancer patients for depression may improve patients’ mental health.9,14
Although dyadic effects in the context of cancer and other chronic diseases are common, Litzelman et al 15 point out that these effects are by no means uniform, with some studies showing influence from patients to caregivers, some showing influence from caregivers to patients, some showing reciprocal influence, and some showing a lack of dyadic influence. The authors suggest that variability in dyadic effects may be due to differences in context and population. 15 Although much of the early work in dyadic cancer research involved spousal dyads,16,17 more recent studies have found dyadic effects in heterogeneous samples of spousal and non-spousal caregivers.9,11,18 One dyadic study of caregivers and patients with cancer, dementia, diabetes, and stroke suggested the possibility of differences in interdependence by the dyad’s relationship type; the authors describe the differences as substantive but not statistically significant. 15 Another study that tested moderation of interdependence by relationship type in cancer patients and caregivers did not find significant differences. 19 Patient-caregiver coresidence, which is often strongly associated with type of relationship (spousal vs non-spousal), 20 is another important factor to consider.21,22
One major shortcoming of much dyadic cancer research to date has been a lack of racial and ethnic diversity.23,24 In particular, there has been little work examining outcomes for Black cancer patients and their informal caregivers together, especially over time. A cross-sectional study of Black Americans with lung, breast, colorectal, or prostate cancer (74% of whom had metastatic disease) and their Black family caregivers 25 found that mental distress was prevalent (reported by 50% of patients and 53% of caregivers), and that greater caregiver mental distress was associated with lower quality of life for both patients and caregivers. The authors note that their study did not investigate patterns over time and may not generalize to patients with early-stage disease. 25 The Detroit Research on Cancer Survivors (ROCS) Study26-28 has provided insights into the experiences of caregivers for African American patients. The authors found that most caregivers for African American patients (over 75%) were female, and the vast majority (97%) were African American themselves. 26 Caregivers provided more than 35 hours a week of care on average, and they often reported making changes to work due to caregiving as well as bearing caregiving-related costs.26-28 Although important, the ROCS findings take caregivers as the unit of analysis rather than examining how patients and caregivers affect each other’s outcomes.
This lack of dyadic research focused on Black patients is particularly problematic in light of the well-documented disparities Black women with breast cancer face due to structural racism.29-33 Among Black women in the United States, breast cancer is the most commonly diagnosed non-skin cancer 29 and the leading cause of cancer death. 31 Compared to White women, Black women with breast cancer are 41% more likely to die from the disease. 29 They may experience lower quality of life,34,35 deal with interpersonal discrimination during treatment, 36 and face disparities in receipt of guideline-based treatment and follow-up care.30,37,38 Researchers have pointed out that the health system’s reliance on informal caregiving has the potential to exacerbate health disparities (if, for example, both patients and the people in their support networks have lower socioeconomic status or lack access to opportunities and resources). 39 Analyzing data from a dyadic perspective is one way to examine these patterns of mutual influence.
Recruiting samples from a range of racial and ethnic backgrounds is especially important because past work has indicated that patterns of caregiving and social support may differ by race.5,39 Black women with breast cancer who are in partnered relationships often receive support from their spouses/intimate partners,40,41 but the majority of older Black women in the U.S. are not married. 42 Prior work has shown that Black women with breast cancer are often supported by a network of friends and family, especially female family members.43-45 As a result, it is unclear whether past dyadic work with primarily spousal couples generalizes to Black cancer patients and their caregivers. In addition, there are relatively few supportive resources designed specifically for Black breast cancer patients,45-47 their caregivers, 48 or patient-caregiver dyads that include Black patients. 23 In order to develop effective supports for such dyads, clinicians need to know more patterns of mutual influence among dyads of Black patients and caregivers.
Actor-Partner Interdependence Models (APIMs) can be used to analyze dyadic data and test whether one person’s predictors are associated with not only their own outcomes but also those of a dyad member. 49 Kenny, Kashy, and Cook 49 describe four potential sources of interdependence within dyads: compositional effects (in which a dyad shares similar characteristics), partner effects (in which one person’s characteristics or behavior affect the other person’s outcomes), mutual influence (in which both people’s outcomes affect each other through a feedback process), and common fate (in which a shared causal factor affects both members of a dyad). Longitudinal dyadic models allow for testing these effects over time while also accounting for people’s own autocorrelated measurements across time points.49,50 In random-intercept cross-panel models, as used in this study, specific model components map cleanly onto two of these sources of interdependence. Compositional effects are represented by correlated intercepts (baseline tendencies) and momentary correlations at early time points, and partner effects are represented by prospective effects in the model.
The current dyadic analyses draw on the Dyadic Cancer Outcomes Framework (DCOF), 21 a general model of the effects of cancer on both spousal and non-spousal dyads. The DCOF, designed to be used in conjunction with modeling approaches such as the APIM, describes how individual- and dyad-level factors may affect patient, caregiver, and dyad-level mental health, physical health, and relationship outcomes over time. The DCOF highlights the importance of the broader social context in which relationships and dyadic processes unfold. Elements of the framework helped frame the research questions, guide our inclusion criteria, and select the outcomes of interest.
This longitudinal dyadic study is, to our knowledge, one of the first to analyze longitudinal interdependence between Black patients and their caregivers. We examined interdependence between Black breast cancer patients and their caregivers over four months shortly after the patient’s diagnosis. We chose measures based on the literature and the DCOF. 21 Our primary outcome was depressive symptoms, which are often prevalent in cancer patients and caregivers.12,24,25 Secondary outcomes, chosen because they are commonly used to assess wellbeing in patients and caregivers, included physical and mental health quality of life,21,25,51 perceived social support,52,53 and health behaviors.10,11,21 We hypothesized that patients and caregivers would demonstrate compositional effects (i.e., concurrent correlations) and prospective interdependence, on these measures—that is, that one person’s measures at one time point would predict the other person’s measures at the next time point.
Methods
In this prospective study, we used longitudinal Actor-Partner Interdependence Models (APIMs) to examine interdependence over time in Black women with breast cancer and their informal caregivers. The team followed Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines 54 in reporting results.
Sample and Procedures
Patients were eligible if they self-identified as a Black/African American woman, were 18 years of age or older, had a new first diagnosis of breast cancer (i.e., were within 8 weeks of their new patient visit), were able to answer questions in English, and had an informal caregiver whom they reported would participate in the study. Patients who reported being multiracial were eligible if they considered themselves Black/African American as part of their identity. Patients were excluded if metastatic breast cancer was diagnosed or strongly suspected at initial clinical presentation; however, those who later developed metastatic breast cancer were not excluded from continuing in the study. Caregivers were eligible if they were able to answer questions in English, were 18 years of age or older, and had been identified as a support person by a patient who was eligible for the study.
Potentially eligible patients were identified by screening patient records of collaborating surgeons at a NCI-designated Comprehensive Cancer Center in the Midwest. Patients were identified consecutively and mailed study information for themselves and a caregiver (described to patients as “your most important support person in dealing with breast cancer”). Study staff followed up with a phone call to assess interest, screen for eligibility, and obtain caregiver contact information. All participants provided verbal informed consent for data collection prior to the first survey; patients also consented to extraction of cancer-related information from their medical records. Surveys were administered by trained study staff over the telephone at baseline, two months, and four months; an additional 18-month exploratory timepoint is not included in the current analyses. Participants were considered enrolled in the study if they completed at least half of the baseline survey, and participants who enrolled were contacted by phone at every follow-up timepoint unless they notified the study team that they wished to withdraw from the study. The Qualtrics platform was used for computer-assisted data capture during survey administration. Participants received a check or gift card as a thank-you for completing each survey ($30 at baseline, $35 at 2 months, $40 at 4 months). At the end of every survey, participants were offered referrals to counseling/social work if desired. Data for the first three timepoints were collected January 2021 – July 2023. This study was approved by Institutional Review Boards at Washington University in St. Louis, where data collection took place (IRB #202010222, initial approval 12/3/2020), and the University of North Carolina at Chapel Hill, where data analysis was conducted (IRB #23-1627, initial approval 10/9/2023).
Measures
To conduct APIM analyses, the same measures must be administered to both members of a dyad. The team therefore chose measures appropriate for people with and without chronic disease. Our choice of outcome measures was guided by the Dyadic Cancer Outcomes Framework, 21 which was developed based on the literature about patient-caregiver dyads in the context of cancer.
Depressive symptoms (primary outcome)
Depressive symptoms, which are often prevalent in cancer patients and caregivers,12,24,25 were assessed with the Center for Epidemiologic Studies Depression scale (CES-D), a 20-item measure that has been used in populations with and without chronic disease and that has been shown to be reliable and valid in African American cancer survivors.55-57 Scores range from 0 to 60, with greater scores indicating higher levels of depressive symptoms; a score of ≥16 is often used as a cutoff to indicate the need for further evaluation. In this sample, the CES-D demonstrated excellent reliability (baseline Cronbach’s alpha = .891 for patients, .869 for caregivers).
Physical and mental health quality of life (secondary outcomes)
General physical and mental health quality of life measures are often used to assess overall wellbeing in cancer patients and caregivers.21,25,51 Participants completed the PROMIS Global-10 v.1.2, a 10-item patient-reported outcome measure that has shown good reliability and validity in the general U.S. population.58-60 Four items are summed to create a raw physical health quality of life subscale score, and four items are summed to create a raw mental health quality of life subscale score; two items not included in either subscale score are not used in these analyses. Raw scores are transformed into scaled scores with a U.S. population mean of 50 and a standard deviation of 10, with higher scores indicating better health. 59
Perceived social support (secondary outcome)
Perceived social support, which has been associated with physical and mental health outcomes in cancer patients 52 and caregivers, 53 was measured with the 19-item Medical Outcomes Study Social Support Survey (MOS-SSS). This measure has been shown to be reliable and valid in community-dwelling adults with chronic disease 61 and has been successfully used in studies of Black women with breast cancer 52 and in control study participants without cancer. 62 Transformed MOS-SSS scores are on a scale of 0-100, where higher scores indicate greater social support. 63
Health behaviors (secondary outcome)
Health behaviors may also be interdependent in patient-caregiver pairs.10,11,21 Participants were asked about three health behaviors that have been associated with mortality in prior research.64-67 A composite health behavior variable was created from three items adapted from prior health surveys: smoking cigarettes (every day/some days/not at all), days of exercise per week (0-7) 68 and number of servings of fruits and vegetables per day (0, 1, 2, 3, 4, 5+). 69 Whereas some previous work has combined multiple health behaviors by dichotomizing separate indicators into healthy/unhealthy and then summing them,64,65,67 we chose to retain as much information from the original items as possible. Because the items used different response scales, responses were transformed by dividing each by the maximum then combining, with percent of the maximum of exercise and fruits and vegetables added and percent of maximum smoking subtracted. This approach was used for combining items rather than z-scores (which would have the effect of removing any trends over time). The resulting index was conceptualized as a general measure of health behaviors.
Demographic data
Patients and caregivers were asked to provide information about age (in years), insurance status (dichotomized into some private insurance vs not), marital status (dichotomized into married/partnered vs not), work status (dichotomized into working at least part-time vs not), highest level of education (some high school or less; high school diploma/GED; some college/technical school; bachelor’s degree; graduate/professional degree), income (under $20,000; $20,000 to <$40,000; $40,000 to <$75,000; $75,000 or more), the number of children under 18 in the home, and the number of other adults in the home. Patients and caregivers reported their relationship to one another, dichotomized into spousal/romantic partner vs not; romantic partner dyads included dyads in which patients chose “another relationship” to describe the dyad and elaborated that the caregiver was their boyfriend or fiancé. Participants reported the length of their relationship in years and whether they lived together all, some, or none of the time (dichotomized into living together some/all of the time vs not). Type of dyad, dyad coresidence, and length of relationship in years were based on patient self-report, supplemented by caregiver self-report if no patient data were available.
Identifying as a Black/African American woman was an inclusion criterion for patients; no additional race or gender information was collected from them in surveys. Caregivers were asked to choose all that applied to describe their racial identities (Asian; American Indian or Alaska Native; Black or African American; Native Hawaiian or Other Pacific Islander, White, or prefer to self-describe; dichotomized as Black/African American vs not). Patients and caregivers were asked if they considered themselves Hispanic/Latino. Caregivers were asked whether they considered themselves male, female, or preferred to self-describe (dichotomized into male or female, since no caregivers self-described).
Analyses comparing patients who did and did not enroll in the study used two variables obtained from the medical record at the time of record screening: age in years at the time of the patient’s new cancer visit and marital status, which was coded as married vs another relationship status.
Cancer staging
Cancer stage was taken from the medical record at the time of the 4-month survey and was categorized as early (Stage 0, 1, or 2A), locally advanced (Stage 2B or 3), metastatic (Stage 4), or unknown. Although patients were ineligible for the study if they presented with metastatic disease at the time of their new cancer visit, the few patients who later developed metastatic disease were not excluded from continuing to participate.
Analysis Plan
Descriptive and bivariate statistics were conducted in IBM SPSS Statistics Version 29.0.1.0 70 to characterize the patients and caregivers in the sample. We also used bivariate tests to examine differences between patients who did and did not enroll in the study. Actor-Partner Interdependence Models assessed interdependence of patient and caregiver measures over time. 49 The random-intercept cross-panel model was the primary analytic method, but when there were indications of linear trends, latent growth models were also examined. Analyses were conducted in Mplus version 8 using the MLR (maximum likelihood estimator robust to violations of normality) or Bayes estimator with uninformative priors. 71
Analytic Changes to the Preregistration and Rationales for Those Changes

Power
The a priori power analysis and sample size estimate were based on the cross-lagged panel models originally planned (see Figure 1 and Table 1). We used a Monte Carlo simulation study with 1000 replications in Mplus 8 based on the following assumptions: a population correlation between patient and caregiver of 0.2 for CES-D score
72
; a standardized regression coefficient for partner effect of 0.18;
8
and a moderate amount of missing data (for patients: 2% at baseline, 10% at T2, and 20% at T3; for caregivers, 5% at baseline, 15% at T2, and 25% at T3).
52
The simulation yielded a power of at least .90 for the planned tests to detect a partner effect with a sample of 100 dyads; a sample of 110 dyads was planned in case attrition was higher than anticipated. Illustration of a Random-Intercept Cross-Lagged Panel Model (RI-CLPM). Whereas a more conventional cross-lagged panel model estimates only the solid paths, a random intercept model also conceptualizes each timepoint as also being affected by a person’s overall tendency toward that construct (the dotted paths). For simplicity, patient-caregiver correlations and correlated errors for each timepoint are not shown here, but they are included in all models.
Subsequent to this power analysis, as described below and in Table 1, we changed our primary modeling strategy to a more conservative test that might in some cases reduce power. We address this issue further in the Discussion.
Missing data
These analyses include all participants who provided meaningful data at baseline (i.e., finished at least half of the first survey). The MLR and Bayes estimators generally handle missing data appropriately without listwise deletion, whereas listwise deletion would result in biased parameters. 73 For this reason, we included data from patients and caregivers in the rare instances when the other member of the dyad did not enroll. One exception is when covariates are missing; in this case we minimized the number of listwise deleted participants by predicting the most missing covariate (patient income, n = 5) with whether the patient had private insurance; as a result, adjusted analyses are missing two participants.
Preregistration and modifications to preplanned analyses
The original analysis plan was preregistered on OSF prior to data collection (https://osf.io/xf4ac). Table 1 provides information about changes made to the preregistered study design and data analysis plans and a rationale for all changes.
Of note, the original analysis plan stated that cross-lagged panel APIMs would be used to test for interdependence. Due to new evidence that failure to account for correlated intercepts produces inflated cross-construct relationships, 50 we used Random Intercept Cross-Lagged Panel Models (RI-CLPMs) to conduct APIM analyses. RI-CLPMs, as implied by the name, add a random intercept to the cross-panel model (see Figure 1). This allows the model to better account for individual tendencies toward higher or lower scores that affect all observations. That is, some people have a higher level of depressive symptoms generally, in such a way that all of their scores tend to be higher than other people’s. In the case of the current models, it is likely this general tendency towards higher or lower scores pre-dates the first measurement. When this influence is accounted for, correlations at each time point represent momentary correlations between patient and caregiver that are specific to that timepoint and do not merely reflect pre-existing tendencies. Notably, both correlated intercepts and momentary correlations fall under the concept of compositional effects. Correlated intercepts suggest pre-existing compositional effects, whereas momentary correlations suggest newly formed compositional effects.
Failing to take correlated intercepts into account can produce spurious relationships between variables that are better attributed to correlated random intercepts: Dyads might appear to influence each other when the more parsimonious explanation is that both dyad members are prone to having similar scores. Alternatively, dyads might appear to have a correlation at Time 1 and not later timepoints, which is misleading if their tendency to correlate is not restricted to Time 1 and is more appropriately understood as a correlated underlying tendency. Using the RI-CLPM avoids these issues, and at the same time allows us to examine two aspects of compositional effects. Thus, using RI-CLPM is consistent with our pre-registered intentions, although we originally intended to use standard cross-panel models. We also provide the pre-registered model results for comparison.
When interpretation or convergence was problematic, we used the Bayes estimator instead of MLR provided the variables analyzed appeared approximately normal (judged via skewness and kurtosis). The Bayes estimator has various helpful properties including (a) it does not estimate negative variances and (b) its estimates and standardized estimates have consistent significance estimates, whereas in MLR these can conflict. When the Bayes estimator is used, we report whether effects are statistically significant at P < .05 based on the 95% credible interval not containing zero.
Multiple group models tested whether results differed by whether patients and caregivers lived together. The Bayes estimator does not have a multiple group models implementation in Mplus, so the MLR estimator was used when possible, or separate Bayesian models were run in each group. Tests of whether covariates modified results were conducted by regressing all the outcome variables (at all time points) on the covariates directly. Tests of interdependence were then conducted on the residuals of the outcomes once the covariates and the random intercepts had been accounted for.
Results
Figure 2 provides a flow diagram of recruitment, enrollment, and survey completion. A total of 258 patients were mailed materials inviting them to participate. In all, 107 patients and 103 caregivers enrolled and provided baseline data, for a total of 210 participants (108 complete and partial dyads). Although every effort was made to enroll both members of a dyad, there were five patients who met eligibility criteria (including reporting that a caregiver was willing to participate) whose caregivers were ultimately unable to be reached for study enrollment. One patient expressed interest in study participation and her caregiver was then contacted and enrolled; the patient was subsequently unable to be reached. There were no significant differences in age or marital status between patients who did and did not enroll in the study. In the 108 dyads, survey completion was 97% at baseline (one patient and five caregivers missing), 94% at two months (four patients and nine caregivers missing), and 90% at four months (eight patients and 13 caregivers missing). Flow Diagram of Study Participants (N = 210)
Descriptive Statistics for Baseline Measures From Patients and Caregivers (N = 210 Participants: 102 Complete Dyads, 5 Patients Without Caregivers, and 1 Caregiver Without a Patient)
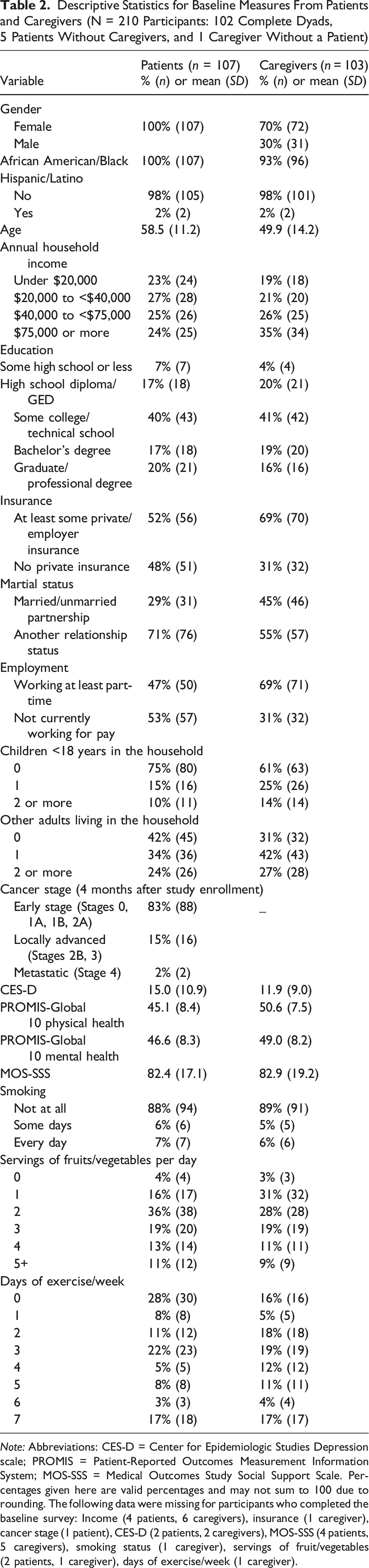
Note: Abbreviations: CES-D = Center for Epidemiologic Studies Depression scale; PROMIS = Patient-Reported Outcomes Measurement Information System; MOS-SSS = Medical Outcomes Study Social Support Scale. Percentages given here are valid percentages and may not sum to 100 due to rounding. The following data were missing for participants who completed the baseline survey: Income (4 patients, 6 caregivers), insurance (1 caregiver), cancer stage (1 patient), CES-D (2 patients, 2 caregivers), MOS-SSS (4 patients, 5 caregivers), smoking status (1 caregiver), servings of fruit/vegetables (2 patients, 1 caregiver), days of exercise/week (1 caregiver).
Mean baseline CES-D score was 15.0 (SD = 10.9) for patients and 11.9 (SD = 9.0) for caregivers. Forty-two percent of patients and 28% of caregivers had baseline CES-D scores ≥16. In 56% of complete dyads providing baseline CES-D data, one or both dyad members were at or above that threshold.
Depressive Symptoms
Complete Standardized Coefficients for the Unadjusted Model of Patient and Caregiver Depressive Symptoms, as Measured by the CES-D

SE = standard error; CES-D = Center for Epidemiologic Studies Depression scale.
Post hoc analyses for depressive symptoms
Simple examination of means, which declined for both groups over time, revealed that it was possible that many patients and caregivers demonstrated changes in depressive symptoms over time. The presence of linear trends would confound the models above. We examined this possibility with a latent growth curve model in which both patients and caregivers had an intercept and slope, both of which were permitted to vary randomly across participants. This model revealed that whereas neither patients nor caregivers had a systematic linear tendency, caregivers did have significantly varying slopes (Variance = 9.63, P = .025), which suggests that some caregivers had systematically decreased depression over time whereas others had systematically increased depression. Prospective effects could only be modeled if effects of the same type were constrained to be equal (e.g., patient autoregressive parameter was the same from Time 1 to Time 2 as from Time 2 to Time 3), and then only using the Bayes estimator. No signs of interdependence were detected in this model. When participants were restricted to those who lived together, the correlation between residual variances reported above was present (r = −.79, P < .05).
Physical Health Quality of Life
Evidence of partner effects was found only in exploratory tests, but evidence of compositional effects was found in the primary model. The planned RI-CLPM showed inconsistency between standardized and unstandardized parameters in the MLR-estimated model for the correlation of the random intercepts, and thus a Bayesian model was used. In the Bayesian model, the random intercepts correlated significantly (r = .25, P < .05); patients and caregivers tended to have similar physical health quality of life. Adding covariates to the RI-CLPM did not change the significance of this finding (r = .27, P < .05). In contrast, the standard cross-lagged panel model instead showed a correlation between patient and caregiver at Time 1 only (r = .24, P = .009). The multiple-group model for dyads indicated that this correlation did not differ markedly across groups, in that in both groups the correlation was in the .2 range but not statistically significant, plausibly due to the smaller sample size for those analyses. In addition, dyads that lived together vs lived apart showed divergent prospective patterns of interdependence. For patients who lived apart from their caregivers, caregiver physical health quality of life at Time 2 predicted improved patient health at Time 3 (standardized coefficient = .42, P = .015), whereas this relationship was negative when dyads lived together (standardized coefficient = −1.04, P = .001). In addition, correlations were observed at different timepoints for those who lived apart vs together (apart: Time 3, r = .47, P = .005; together: Time 1, r = .73, P = .002).
Post hoc analyses for physical health quality of life
The finding of significant slope variance in depressive symptoms for caregivers above suggested the necessity of checking for a linear trend for other secondary outcomes as well. In an initial model including slope and intercept for both patient and caregiver, caregivers did not have a significant mean or variance for their slope (ps > .10) and thus their slope was omitted. Patients showed a slight tendency to have deceasing physical health, with little variance as estimated by a nonsignificant negative estimate (M = −0.68, P = .042, variance P > .30). When the small negative variance was constrained to be zero, the intercept for patient and caregiver correlated as reported above (r = .28, P = .006). Similarly, when prospective effects were added in a Bayesian version of the same model, none were statistically significant but the correlation between intercepts remained.
Mental Health Quality of Life
No evidence of partner effects was found for mental health quality of life, but evidence of compositional effects was clear. The planned RI-CLPM displayed correlated random intercepts (r = .28, P = .002); patients and caregivers tended to have similar mental health quality of life. The multiple-group model would not converge, but separate models for dyads who lived together vs apart using the Bayesian estimator did converge and revealed no additional evidence for interdependence. Significant findings were unchanged when covariates were added; only the random intercept correlation (r = .23, P = .006) suggested interdependence. In contrast, the standard cross-lagged panel model showed a correlation between patient and caregiver at Time 1 (r = .29, P = .004).
Post hoc analyses for mental health quality of life
The finding of significant slope variance in depressive symptoms for caregivers above suggested the necessity of checking for a linear trend for other secondary outcomes as well. In an initial model including slope and intercept for both patient and caregiver, caregivers did not have a significant mean or variance for their slope (ps > .10) and thus their slope was omitted. Patients showed a slight tendency to have deceasing physical health, with little variance as estimated by a nonsignificant negative estimate (M = −0.68, P = .042, variance P > .30). When the small negative variance was constrained to be zero, the intercept for patient and caregiver correlated as reported above (r = .28, P = .006). Similarly, when prospective effects were added in a Bayesian version of the same model, none were statistically significant but the correlation between intercepts remained.
Perceived Social Support
No evidence of partner effects was found in the preferred model for perceived social support, but evidence of compositional effects was clear. The planned RI-CLPM displayed correlated random intercepts (r = .37, P = .002); patients and caregivers tended to have correlations in overall levels of social support. An additional correlation at Time 1 was inconsistent across estimates but not statistically significant in a Bayesian version of the model. The multiple-group model would not converge, but separate models for dyads who lived together vs apart using the Bayesian estimator did converge and revealed no additional evidence for interdependence. Adding covariates did not change substantive results. In contrast, the standard cross-lagged panel model showed a marginal correlation between patient and caregiver at Time 1 (r = .16, P = .051) as well as a prospective effect such that patient social support at Time 3 was predicted by caregiver social support at Time 2 (standardized coefficient = .16, P = .040).
Post hoc analyses for social support
Similar to the linear trend effects seen in depressive symptoms, caregivers had significant variance but no significant mean for their social support (variance = 15.36, P = .012); patient variance was marginal (variance = 38.54, P = .060). As with the models above, a Bayesian model in which constrained prospective effects were estimated alongside random slopes and intercepts indicated no additional signs of interdependence and the correlated intercepts were no longer statistically significant.
Health Behaviors
No evidence of partner effects was found in the preferred model for health behaviors, but evidence of compositional effects was clear. The planned RI-CLPM displayed correlated random intercepts (r = .33, P = .026); patients and caregivers tended to have similar health behaviors. In the multiple group model, dyads living apart had correlated intercepts (r = .40, P = .008), whereas those living together showed a correlation at Time 3 (r = −.53, P = .026). With covariates added, the correlation between intercepts was reduced to a trend (r = .35, P = .052). In contrast, the standard cross-lagged panel model showed a correlation between patient and caregiver at Time 1 (r = .30, P < .001). Unlike the other outcome variables, health behaviors showed no sign of linear trends, with means and variances of slopes all non-significant (ps > .550), and therefore no follow-up models were conducted.
Discussion
This is one of the first longitudinal analyses of data from Black women with cancer and their informal caregivers. The Dyadic Cancer Outcomes Framework 21 guided our selection of mental and physical health outcomes, as well as our decision to allow patients to nominate a range of caregivers (despite the analytic heterogeneity introduced by this choice). The DCOF also led us to be mindful of the broader social context in which caregiving takes place in the U.S. Consistent with Ellis et al, 25 we found depressive symptoms were prevalent among Black patients and their caregivers; in over half of the dyads in the current study, at least one member met or exceeded the cutoff for depressive symptoms that would indicate the need for further screening. The large majority (78%) of patients nominated a non-spousal caregiver as their most important support person in dealing with cancer. This is perhaps unsurprising given that only 29% of the patients reported being married or partnered at baseline. At the same time, even among patients who reported being married or partnered, 39% did not nominate their spouse. These findings, consistent with previous work showing the importance of female caregivers,43-45 underline the importance of asking patients who is providing them with support rather than assuming that spouses are the primary source of support for most patients.
Our hypothesis that dyads would demonstrate prospective interdependence in depressive symptoms, mental and physical health quality of life, social support, and health behaviors was not supported. In other words, we did not observe what some have called partner effects 49 and what others have called spillover effects 15 or emotional contagion 13 during the 4-month study period. Findings are consistent with the assertion of Litzelman et al 15 that, although dyadic effects are common, there may be heterogeneity in dyadic effects across different populations; it is important to assess dyadic interdependence in a range of populations instead of assuming prior work will generalize to people from other backgrounds. It is also possible that these null findings were due to the time interval at which we assessed patients and caregivers. Although our study design was similar to others who have measured psychosocial outcomes at 2-month intervals, 9 it is possible that we missed dyadic processes unfolding over longer or shorter timeframes. For example, alternative methods, such as laboratory observations, ecological momentary assessment, or daily diary studies, would be able to detect shorter-term shifts in mood.74,75
We did observe small-to-moderate compositional dyadic effects for several outcomes, meaning that patients and caregivers were similar to one another in their overall levels of physical and mental health quality of life, perceived social support, and health behaviors. The average relationship length among these dyads (35.5 years), as well as the fact that many caregivers were patients’ family members, suggests dyadic processes may have unfolded for years or decades prior to study enrollment and were therefore relatively stable by the time of the study period. In the cases of spouses or romantic partners, there may have also been assortative selection into partnerships (i.e., people choosing partners due to similar characteristics). The combination of lack of prospective dyadic effects with fairly consistent compositional effects underscores the importance of collecting and analyzing longitudinal dyadic data (as suggested by the Dyadic Cancer Outcomes Framework 21 ). Correlations that might have been observed at Time 1 alone did not translate to prospective effects.
Although our study was not designed to detect the sources of these compositional effects, the observed similarity in psychosocial characteristics and health behaviors has implications for screening and intervention. Findings are consistent with the idea that patients who face challenges may also be supported by network members facing similar challenges. 39 Systematic patient and caregiver screening for a range of health and psychosocial outcomes could help identify dyads that might benefit from intervention.23,76 For example, our findings are consistent with prior research10,11 showing suboptimal health behaviors in patient-caregiver dyads; more than half of our patients and caregivers reported exercising three days a week or fewer, and more than half ate two or fewer servings of fruits and vegetables on a typical day. Such dyads may particularly benefit from interventions centered on health behaviors.76,77 Even though dyads in the current observational study did not demonstrate prospective interdependence, dyadic interventions often incorporate support or counseling designed to strengthen a pair’s relationship and communication skills.23,78,79 Thus, it is possible that participating in a dyadic intervention together may nurture new processes of mutual influence within a pair. Existing dyadic interventions could be adapted specifically for Black women with breast cancer and their informal caregivers in a range of ways (e.g., by using thoughtful targeted outreach/recruitment strategies, incorporating racially diverse staff, and acknowledging historic racial discrimination in healthcare).76,80 Our team is currently analyzing qualitative interviews conducted with a subsample of dyads from this study to learn more about participants’ preferences for intervention.
In these analyses, we used RI-CLPMs because recent work has argued (convincingly, in our view) that they are superior to standard cross-lagged panel models for measuring outcomes in dyads over time. 50 On a philosophical level, standard cross-lagged panel models assume that any relationship between the outcome variables is due either to time-specific correlations or prospective effects. In contrast, the RI-CLPM acknowledges the fact that people differ in their overall tendencies in certain measurements. Standard cross-lagged panel models using data like ours might lead researchers to conclude that patients and caregivers have similar health behaviors, physical health, social support, and mental health at an initial timepoint but that this relationship disappears over time. In contrast, the RI-CLPM suggests a more plausible interpretation: People in dyads are more similar to each other than to people in other dyads, and these compositional effects likely arose prior to data collection rather than at the time of the baseline measurements. More technically, failing to account for these correlated errors can lead to findings of apparently prospective effects that are better accounted for by a combination of correlated intercepts and measurement error, as might be the case for the social support finding that the standard model suggested but that the RI-CLPM did not corroborate. It should also be noted that state-of-the-art techniques for intervention trials include mixed-effects models or similar strategies which, like the RI-CLPM, include random intercepts and thus account for participants’ stable tendencies when measuring intervention effects.81,82 Researchers conducting future dyadic studies should carefully consider the best analytic tools for analyzing the dyadic processes they expect to observe.
Strengths and Limitations
This work has several strengths. We recruited a sample of 210 Black patients and caregivers and followed participants over three waves of data collection. Our retention rate was very high, with over 90% of patients and caregivers who enrolled completing their follow-up surveys at the third (4-month) timepoint. We tested preregistered hypotheses and included a range of outcome measures commonly used in dyadic studies that have been shown to be reliable and valid in populations with and without chronic disease. Analyses include both preplanned models and post hoc models to explore our findings more fully.
This work has several limitations. Although most of these outcome measures have been shown to be reliable and valid, our composite health behavior variable was created for this study. Our power analysis was based on using cross-lagged panel models; the RI-CLPMs that we ultimately employed are more conservative. In addition, power calculations were based on a test of our primary outcome (depressive symptoms); secondary outcomes and post hoc tests should be considered exploratory. However, results are generally consistent across modeling frameworks and variables here, such that power alone cannot explain our results. Instead, the RI-CLPMs simply offered greater conceptual clarity.
Several characteristics of the sample should also be noted. We recruited participants with nonmetastatic disease from one NCI-designated Comprehensive Cancer Center in the Midwestern United States. Results may not generalize to patients from other U.S. regions or other countries, those with an initial diagnosis of metastatic disease, or those treated in community hospitals. Although our 41% enrollment rate for patients is consistent with previous dyadic studies and is higher than the average seen across behavioral trials of patients and caregivers, 83 the majority of patients approached for participation did not enroll. We found that patients who chose to enroll in the study were not significantly different from those who enrolled in regard to age and marital status, but there may have been other, unmeasured differences between participants and non-participants.
Conclusions
This study is one of the first longitudinal, dyadic examinations of outcomes for Black breast cancer patients and their informal caregivers. As suggested by the Dyadic Cancer Outcomes Framework, 21 we analyzed patient, caregiver, and relationship variables and examined interdependence longitudinally. We found correlations within dyads in overall levels of mental and physical health quality of life, perceived social support, and health behaviors. Although there was no dyadic interdependence demonstrated for CES-D scores, the high prevalence of elevated depressive symptoms in patients and caregivers indicates that many may benefit from additional support. Given the limited time and resources clinicians have for providing caregiver services, 80 it may make sense to administer brief screenings to caregivers or dyads and then offer interventions to those most in need. Researchers and clinicians should continue to build an evidence base for how best to support patients, caregivers, and patient-caregiver dyads from a range of racial and ethnic backgrounds in order to improve outcomes for all patients and their loved ones.
Footnotes
Acknowledgements
We would like to thank the study participants for their time and participation. We would also like to thank Charlene Caburnay, Christi M. Lero, Amy McQueen, and Jennifer Wolff for their assistance with this project.
Ethical considerations
This research was approved by Institutional Review Boards at Washington University in St. Louis, where data collection took place (IRB #202010222, initial approval 12/3/2020), and the University of North Carolina at Chapel Hill, where data analysis was conducted (IRB #23-1627, initial approval 10/9/2023). Verbal informed consent was obtained from all individual participants included in the study.
Author Contributions
Tess Thompson: conceptualization, funding acquisition, methodology, project administration, investigation, data curation, formal analysis, visualization, supervision, writing-original draft, writing-review and editing; Thomas Rodebaugh: methodology, formal analysis, visualization, writing-original draft, writing-review and editing; Polly Haun: project administration, investigation, writing-review and editing; Karin Han: project administration, investigation, writing-review and editing; Naitra Ramchander: project administration, investigation, writing-review and editing; Krutika Chauhan: investigation, writing-review and editing; Jada Meads: investigation, writing-review and editing; Julie Margenthaler: supervision; resources; writing-review and editing; Katherine Glover-Collins: resources; writing-review and editing; Graham A. Colditz: Conceptualization; funding acquisition; supervision; writing-review and editing
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the American Cancer Society (MRSG-19-086-01-CPPB, PI: Thompson). The sponsor did not play a role in study design; in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the article for publication. Use of REDCap for data management was supported by the Clinical and Translational Science Award Grant (UL1 TR002345) and the Siteman Comprehensive Cancer Center and NCI Cancer Center Support Grant P30 CA091842). The Siteman Health Behavior, Communication and Outreach Core provided assistance with survey programming.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.