
Abstract
Background
Beliefs and perceptions about cancer risks and accessibility of health information play an important role in influencing cancer screening behaviors and various health outcomes. However, these beliefs and attitudes are not well understood, especially across different racial and socioeconomic groups. The aim of this study was to identify sociodemographic factors associated with cancer risk perceptions and health-information-seeking attitudes among adults.
Methods
This study utilized data from the Understanding Cancer in Oregon (UCanOR) project, which administered a 47-item cross-sectional survey to capture sociodemographic and behavioral information. Participants were recruited through area-based random sampling and public convenience sampling across Oregon. Multivariable generalized linear and logistic regression analyses were used to evaluate attitudes towards cancer risk and accessing health information.
Results
The study included a total of 1357 respondents [mean age of 50.0 (SD = 17.8)], primarily Non-Hispanic White (87.3%), followed by Asians/Pacific Islanders (8.4%), Hispanic White (3.5%), and Black (0.8%). Compared to Non-Hispanic Whites, Asians/Pacific Islanders were 2.5 times more likely to believe cancer is caused by behavior or lifestyle, 2.8 times more likely to agree that there is little one can do to prevent cancer, and 1.6 times more likely to associate cancer with death.
Conclusion
Asians/Pacific Islanders were more likely to agree with statements expressing frustration and distrust towards cancer beliefs and health information searches. Future community outreach efforts should consider tailoring the message to their target audiences. Understanding and addressing the underlying reasons for these negative perceptions is crucial for developing effective education and health promotion strategies.
Introduction
Participating in cancer screening leads to improved cancer early detection, which reduces cancer morbidity and mortality compared to detection at a later stage.1,2 However, screening rates in the U.S. for breast, cervical, colorectal and lung cancers are below targets, with significant sociodemographic disparities. 3 Among all race and ethnicity groups (White, Black, Hispanic, Asian), Asians have the lowest cancer screening rates. 4 For example, the overall breast cancer screening rate among the U.S. population was 75.6% in 2021, below the Healthy People 2030 target of 80.5%, while the rate among Asians/Pacific Islanders was only 66.3%. 5 Similarly, Asian Americans had significantly lower adherence rates to annual lung cancer screening compared to other racial groups [adjusted odds ratio (OR), 0.42; 95% confidence interval (CI), 0.26-0.69]. 6
Social determinants of health (SDOH) play a key role in shaping health behaviors including cancer screening. 7 SDOH, such as socioeconomic status (SES), education, language barriers, and access to healthcare, influence both individuals perceptions of health risks and their ability to access timely and appropriate healthcare services. 7 Lower SES, for example, is often associated with reduced adherence to cancer screenings 8 and lower health literacy. 9
Beliefs and perceptions about cancer risks significantly influence a person’s health behaviors, including participation in various types of cancer screening (eg, mammogram, colonoscopy, Pap smear). 1 Cancer fatalism, the belief that cancer is beyond an individual’s control and inevitably leads to death, is associated with lower perceived benefits about early detection (P < 0.001) and more perceived fear of seeking help for a suspicious symptoms (P < 0.001), 10 and the fatalism may mediate the relationship between socioeconomic status and screening behaviors. Locally tailored interventions, such as community-based educational programs that address cultural beliefs and misconceptions about cancer risks, have effectively increased cancer screening rates.11,12 Therefore, identifying factors, especially among sociodemographic characteristics which are behind these behaviors, is imperative to improve cancer screening participation rates and early detection of aggressive cancers. While some factors like race/ethnicity, age and sex are not modifiable, others such as educational attainment, language barriers, and health literacy are more amenable to public health interventions to improve screening behaviors and outcomes.
Studies conducted in the U.S., U.K., and Denmark have shown that while positive beliefs about cancer are generally prevalent, individuals with lower socioeconomic status (SES) are more likely to hold negative cancer beliefs about cancer.13,14 Health-information-seeking attitudes are closely linked to cancer fatalism, and individuals who experience difficulties accessing health information were more likely to have fatalistic cancer beliefs. 15 Despite this, few studies have been conducted to comprehensively evaluate factors related to negative attitudes toward health-information-seeking behaviors. In this context, “health-information seeking” refers to the process by which individuals search for health-related information, whether online, through social media, or other sources. 16 Understanding these factors is essential for reducing barriers and improving access to reliable health information. Many psychosocial factors, such as the desire to maintain hope, deny risk, or resist repetitive messaging, can lead individuals to avoid health information. 17 This avoidance of cancer risk information has been associated with lower cancer screening rates. 18 Limited research has evaluated race/ethnicity and sociodemographic factors in both negative cancer beliefs and health-information-seeking attitudes simultaneously.
Oregon is a geographically and demographically unique state. Oregon ranks 27th in population size (approximately 4 million) and has a large rural footprint, with 36% of residents living in rural or frontier areas. The Knight Cancer Institute at Oregon Health & Science University (OHSU), based in Portland, serves as the state’s only NCI-designated comprehensive cancer center, covering all 36 counties. While the majority of the state’s population is White (87.4%), the Asian/Pacific Islander population, though relatively small (∼4.5%), is growing and has been historically underrepresented in cancer research.
The objective of this study was to examine sociodemographic factors associated with negative cancer beliefs and health-information-seeking attitudes in Oregon. Using a cross-sectional survey in Oregon, this study aimed to inform targeted outreach for cancer screening and early detection, intervention planning, patient engagement, and cancer-related study participant recruitment. Understanding these factors allows for the strategic implementation and dissemination of evidence-based interventions to communities most in need and will inform whether and how interventions may need to be adapted to fit the unique characteristics of individual communities.
Methods
We conducted a cross-sectional study using de-identified data collected by members of our research team as part of a larger project “Understanding Cancer in Oregon (U-Can Oregon) with data collected among adults across Oregon in 2019. 19 The Oregon Health & Science University (OHSU) Institutional Review Board (Portland, Oregon, USA) approved this cross-sectional study as exempt for the use of secondary data analyses. The approval number is STUDY00027335, and the date of approval is May 31, 2024. Informed consent was waived by the IRB due to the use of de-identified data.
Study Participants
The study participants were recruited through a combination of random sample selection and convenience sampling methods, including meetings, conferences, social media, and word of mouth (Figure 1). This combined recruitment approach is to improve both the study sample size and the representativeness of the Oregon population. For the randomly selected samples, we established a professional service contract with the Marketing Services Group to draw a stratified, address-based sample of 15000 Oregon households (∼10000 urban and ∼5000 rural) based on census block definitions. Recruitment was conducted via email, postcards, and mail.
19
For non-probability sampling recruitment, we used community events, promotion within OHSU staff, OHSU’s internal media site (O2), social media (Facebook, WeChat, etc.), and local events conducted at OHSU. In order to improve the power of the analysis, we pooled the samples together. We excluded 90 participants who had missing data on either all cancer belief items (n = 3), race/ethnicity (n = 15), composite cancer belief and attitude score (n = 70), or employment status (n = 2). The final sample size includes 703 participants from a randomly selected sample and 654 participants from a convenience sample. In the probability (random) sample, 91.18% of participants were Non-Hispanic White. The remaining participants were African American (0.85%), Asian/Pacific Islander (5.41%), and Hispanic White (2.56%). In the public convenience sample, Non-Hispanic White participants still constituted the majority (83.03%), but the proportions of Asian/Pacific Islander (11.62%) and Hispanic White (4.59%) participants were higher than in the probability sample. These differences indicate that the convenience sample was more racially and ethnically diverse than the probability sample. Additionally, the convenience sample had a higher proportion of female participants (86.0%) than the probability sample (71.0%). The age distributions also differed: in the convenience sample, 58.4% of participants were aged 18-44 years, 31.25% were 45-64 years, and 10.24% were ≥65 years. By contrast, in the probability sample, 41.68% were aged ≥65 years, 31.25% were 45-64 years, and 27.17% were 18-44 years. These results indicate that the convenience sample was disproportionately female and younger compared to the probability sample. Analytic Sample Size Flow Chart
Characteristics of Oregon Respondents
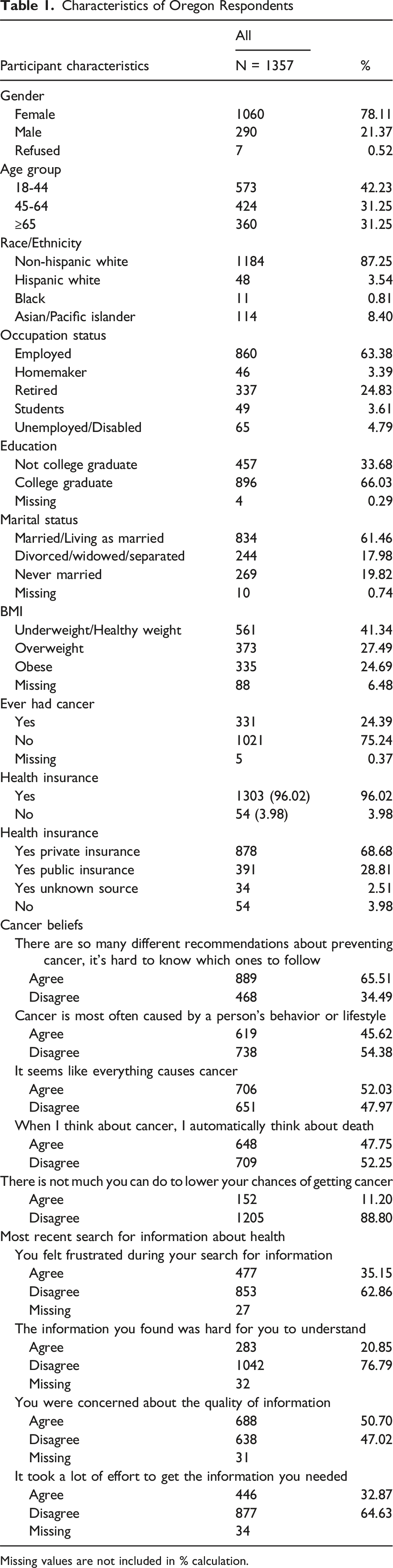
Missing values are not included in % calculation.
This cross-sectional study uses data collected as part of the Understanding Cancer in Oregon (U-Can Oregon) project. 19 The dataset is Oregon-specific and was collected locally by members of our research team. While the data contribute to broader cancer research efforts supported by a National Cancer Institute (NCI) P30 grant, this is not an NCI-administered dataset.
Our primary data collection includes the core demographic and behavioral measures identified by the National Cancer Institute, adding Oregon-specific measures to obtain detailed data regarding attitudes and preferences toward cancer prevention and control, as well as clinical trial participation and information-seeking behaviors. The survey was administered online using Qualtrics. The survey was available in both English and Spanish; translations into additional languages were not provided due to study timeline and resource limitations. We aimed to enhance the breadth of national and state data currently collected with targeted support to better identify health disparities by socioeconomic status, race/ethnicity, and other sociodemographic characteristics such as marital status. In addition, we aimed to gain a deeper sense of the beliefs and perceptions within our diverse catchment area as it relates to cancer and access to health information technology.
Outcome Measures
We used validated measures from the HINTS (Health Information and National Trends Survey), a comprehensive, nationally representative probability-based survey conducted by the National Cancer Institute since 2003 and there have been 16 iterations of HINTS to date, 16 which collects information on the U.S. population’s, attitudes, and behaviors related to cancer and general health information.
Cancer beliefs and perceptions were assessed through 5 survey items: (1) There are so many different recommendations about preventing cancer, it’s hard to know which ones to follow; (2) Cancer is most often caused by a person’s behavior or lifestyle; (3) It seems like everything causes cancer; (4) When I think about cancer, I automatically think about death; (5) There is not much you can do to lower your chances of getting cancer. We assigned a score for the following response categories: 4 = Strongly Agree, 3 = Somewhat agree, 2 = Somewhat disagree, and 1 = Strongly disagree for each of the survey items. A composite score for each of the items on cancer beliefs was calculated based on these questions, with higher total scores representing more negative beliefs. These items, which are intended to measure cancer fatalism, have been used for many years and shown to be effective predictors for preventive health behaviors.21,22
Health-information-seeking attitudes were assessed through 4 statements and 1 question: (1) You felt frustrated during your search for information; (2) The information you found was hard for you to understand; (3) You were concerned about the quality of information; (4) It took a lot of effort to get the information you needed; (5) How confident are you that you could get advice or information about health or medical topics if you needed it? Similar to the cancer beliefs score above, a composite score for health-information-seeking attitudes was also calculated, with higher total scores representing less confident attitudes. These items have previously been used in studies examining health literacy and health-information-seeking attitudes.23,24
In addition to analyzing the composite scores for the cancer beliefs and health-information-seeking attitudes categories, we also conducted item-level analyses for each individual survey question within these categories (Table 3). Each item was treated as a separate binary outcome, reflecting agreement or disagreement with the statement. Before proceeding with the modeling, we recoded the outcome measures to represent agreement (by merging “strongly agree” and “somewhat agree”), and disagreement (by merging “strongly disagree” and “somewhat disagree”). The response categories were merged to improve sample size and study statistical power, and to improve the interpretability of the results.
Main Exposures
The main social demographic factor examined was race/ethnicity (Non-Hispanic White, Hispanic White, African American, Asian/Pacific Islander), employment status (Employed, Homemakers, Retired, Students, Unemployed/Disabled) was analyzed as a secondary factor. In addition to race/ethnicity, employment status was included as it captures an additional dimension of socioeconomic context, including access to resources, social roles, and background knowledge. Also, this selection was informed by prior analyses comparing various socioeconomic factors and the availability of relevant data within our dataset.
Covariates
The covariates assessed were age, sex, marital status (Married/Living as married, Divorced/Separated, Never Married), BMI (Normal/Underweight, Overweight, Obese), health insurance status (Insured, Uninsured), and cancer history (Yes, No).
Statistical Analysis
Chi-squared test for categorical variables (proportions) was used to assess factors in association with cancer related attitude and behaviors (outcomes). To identify factors associated with negative cancer beliefs and health-information-seeking attitudes, we conducted multivariable generalized linear regression and logistic regression analyses. Covariates included age, sex, employment status, marital status, body mass index (BMI), cancer history, and insurance status. We further conducted sensitivity analysis by separating insurance status into private vs public insurance type. These analyses treated cancer beliefs/health-information-seeking attitudes both as a continuous summed variable and as specific categorical variables (Agree vs Disagree).
The PROC Generalized Linear Model (GLM) model was utilized to calculate least squares means (LSMeans) of the perceived total scores of cancer beliefs and perceived total score of the health-information-seeking attitudes (continuous variables). We used LSMeans to calculate means adjusted for multiple covariates. Additionally, PROC LOGISTIC was used to predict agreement with the cancer beliefs and the health-information-seeking attitudes statements (categorical variables: Agree vs Disagree). All data were analyzed using SAS 9.4 (SAS Institute Inc., Cary, NC).
Results
The reporting of this study conforms to STROBE guidelines. 25
Table 1 presents the descriptive demographic characteristics of the survey respondents. The study included 1357 adults with a mean age of 50.0 years (SD = 17.8). The majority of respondents were female (78%), Non-Hispanic White (87%), employed (63%), and married or living as married (61%). About 24% of respondents reported a previous cancer diagnosis. Most participants had health insurance (96%), with 69% covered by private insurance, 29% by public insurance and 2% by insurance from an unknown source.
Multivariate GLM Regression for Negative Cancer Beliefs and Health-Information-Seeking Attitudes Among Oregon Respondents

Proc GLM model LSMEANS predicting agreement with the perceived total score of the following cancer beliefs statements with 4 = Strongly Agree, 3 = Somewhat agree, 2 = Somewhat disagree, and 1 = Strongly disagree: (1) There are so many different recommendations about preventing cancer, it’s hard to know which ones to follow; (2) Cancer is most often caused by a person’s behavior or lifestyle; (3) It seems like everything causes cancer; (4) When I think about cancer, I automatically think about death; (5) There is not much you can do to lower your chances of getting cancer; Proc GLM model LSMEANS predicting agreement with the perceived total score of the following health-information-seeking attitudes statements with 4 = Strongly Agree, 3 = Somewhat agree, 2 = Somewhat disagree and 1 = Strongly disagree: (1) There are so many different recommendations about preventing cancer, it’s hard to know which ones to follow; (2) The information you found was hard for you to understand; (3) You were concerned about the quality of information; (4) It took a lot of effort to get the information you needed.
Significant differences in composite health-information-seeking attitudes scores were also observed based on race/ethnicity (P < 0.0001) with Asian/Pacific Islander having the highest adjusted mean score. Age (P = 0.008), and BMI (P = 0.04) also showed significant differences, with younger age and obese respondents showing more negative health-information-seeking attitudes. Asian/Pacific Islander participants demonstrated the highest adjusted mean score for negative health-information-seeking attitudes [LSMEAN (95% CI) = 5.07 (3.52-6.61)] compared to other groups. No significant differences were found by sex, marital status, insurance status, or personal cancer history.
Multivariate Logistic Regression for Cancer Beliefs and Health-Information-Seeking Attitudes

Hispanic respondents did not differ significantly from Non-Hispanic Whites on most of the cancer belief items. However, they were less likely to report frustration when seeking health information (OR = 0.43; 95% CI: 0.21-0.87), suggesting a potentially more positive information-seeking experience. For Black respondents, while none of the results reached statistical significance due to the small sample size, some point estimates suggest areas for further study.
Regarding employment status, individuals who were unemployed or disabled were 2.8 times as likely as those who were employed to associate cancer with death [OR (95% CI) = 2.75 (1.54-4.89)] and 2.2 times as likely to believe there is not much one can do to lower chances of getting cancer [OR (95% CI) = 2.22 (1.10-4.49)]. Unemployed/disabled respondents were also more likely to report frustration [OR (95% CI) = 1.87 (1.10-3.19)] and difficulty understanding health information [OR (95% CI) = 2.48 (1.42-4.33)], and were less confident in obtaining health information [OR (95% CI) = 0.56 (0.32-0.98)].
Sex, marital status, and health insurance status were generally not significantly associated with cancer beliefs or health-information-seeking attitudes in adjusted analyses.
Discussion
This study found that Asians/Pacific Islanders have significantly more negative cancer beliefs and health-information-seeking attitudes than individuals of other races. For the majority of the cancer belief and health information search attitude statements, Asian/Pacific Islanders, those who are unemployed or disabled were significantly more likely to agree with more negative responses.
Our study found that Asian/Pacific Islanders had the highest composite scores for both negative cancer beliefs and health-information-seeking attitudes. This finding is consistent with prior reports that Asians are underrepresented in cancer screening, despite that the overall cancer incidence and mortality rates are lower among Asians. 26 This discrepancy suggests a potential disconnect between perceptions and actual risk, highlighting the culturally tailored health communication strategies targeting these populations. Cultural beliefs and taboos influence a person’s willingness to seek diagnosis. 27 Other studies suggest that it is possible that Asians have more negative cancer beliefs due to cultural differences surrounding health and seeking healthcare. A 2003 survey of 798 Chinese immigrants living in San Francisco suggests that community stigmas prevent some Chinese immigrants from seeking early diagnosis and highlights the importance of concerted education efforts in dispelling myths about cancer. 28 Language barriers, the role of family decision making, and reliance on traditional health practices may also play a role in the underutilization of cancer screening resources among Asian populations. 29 In our study, Asians/Pacific Islanders were more likely to agree that “cancer is most often caused by a person’s behavior or lifestyle” and that “there is not much you can do to lower your chances of getting cancer,” indicating both belief in the role of one’s behavior in cancer risk and a higher degree of fatalism. In previous studies, agreement with the belief “cancer is most often caused by a person’s behavior or lifestyle” was associated with higher self-efficacy and knowledge regarding cancer risk.30,31 Agreement to these seemingly contradictory statements highlights the need for culturally tailored interventions that address the unique barriers in cancer prevention faced by Asian/Pacific Islander communities. Such interventions could include culturally tailored education initiatives that provide actionable prevention strategies, expanded training and employment of community health workers from Asian/Pacific Islander backgrounds to build trust and deliver targeted health messages, and collaborations with traditional medicine practitioners to integrate modern prevention strategies in ways that respect cultural practices and beliefs.
Based on these findings, several recommendations emerge for improving cancer-related beliefs and information-seeking behaviors in Asian/Pacific Islander communities. First, culturally tailored education campaigns should be developed to address fatalistic beliefs and misinformation while offering clear, actionable prevention strategies. Second, expanded training and employment of community health workers from Asian/Pacific Islander backgrounds can help bridge gaps in trust, language, and cultural understanding. Third, collaboration with faith-based organizations, ethnic media, and community leaders can help disseminate accurate health messages through trusted channels. Fourth, public health efforts should consider integrating traditional health practices with evidence-based prevention models, which can increase community buy-in. Finally, multilingual and low-literacy educational materials should be made widely available to meet the diverse needs of these communities.
In terms of employment status, previous studies have shown that unemployed and self-employed individuals, who often experience higher levels of stress and anxiety related to their financial and social situations--are less likely to participate in cancer screening than regular employees.32,33 Part-time workers face similar challenges, possibly due to stressors in the work environment. 34 These stressors are associated with a pessimistic attitude toward health and healthcare, leading to negative cancer beliefs and health-information-seeking attitudes. Therefore, understanding the associations between employment status and cancer beliefs as well as health-information-seeking attitudes is crucial for developing effective public health strategies to improve cancer screening rates and overall health outcomes in these vulnerable populations.
All of our findings above emphasize the importance of social determinants of health, beyond cultural beliefs, in shaping cancer beliefs and health behaviors. Factors such as race/ethnicity and socioeconomic status, including employment status, influence access to healthcare resources and health-related attitudes and behaviors, and even cancer outcomes. 35 Addressing structural inequities through policy interventions, community education, and improved access to culturally and linguistically appropriate healthcare resources is critical for reducing disparities in cancer prevention and treatment.
Our study has several strengths, including a robust overall sample size of 1357 and the use of multiple methodologies for survey administration and recruitment. While some subsets are smaller, these diverse approaches aim to maximize representation and diversity across different groups. This is the first study reporting this finding specific to the Oregonian Asian/Pacific Islander population. It is one of the few studies to comprehensively examine cancer beliefs and information-seeking attitudes in a population-based samples with sufficient Asian/Pacific Islander respondents living in Oregon, a state where the Asian/Pacific Islander demographic is relatively small. This underrepresentation has contributed to a significant gap in population-based research focused on this group. Thus, our results address the gap in data on Asian/Pacific Islander population in Oregon. Limitations include a low survey response rate, which may limit the generalizability of our findings, and the underrepresentation of racial and ethnic minority populations. Only 0.8% of respondents identified as Black or African American, limiting statistical power and generalizability for this population. While this reflects Oregon’s small Black population (∼2%), the sample size restricts the power of analyses on this group. Additionally, we did not collect data on sociodemographic variables such as income, language spoken, or immigration status. The absence of these variables and the limitation of translation to non-English and non-Spanish languages restrict our ability to fully capture the diversity within the Asian/Pacific Islander population and to assess substantial heterogeneity across Asian/Pacific Islander populations in understanding health attitudes and beliefs. Future surveys that include these variables are warranted. Funding for focused research among Asian American populations remains scarce, despite Asian Americans being disproportionately affected by cancers of infectious origins. 36 For participants recruited through convenience sampling, individual-level address data were not collected, limiting our ability to examine neighborhood-level influences on healthcare access. Future surveys that include these sociodemographic and geospatial variables such as ZIP code or census tract are warranted to support more in-depth analyses of social and environmental impacts. Nevertheless, our significant findings on Asian/Pacific Islander population in Oregon shed light on their unique experiences and beliefs related to cancer, contributing to a broader understanding of health behaviors in this understudied population in Oregon. Future research comparing cancer-related beliefs and attitudes with actual screening behaviors in Oregon would provide a deeper understanding of how perceptions influence preventive health behaviors.
Conclusions
The study findings highlight the importance of addressing social determinants of health, such as race/ethnicity, employment status, access to culturally and linguistically relevant education and healthcare resources, in community outreach initiatives on cancer education and prevention. This research is critical for informing community outreach efforts which should incorporate culturally tailored message and inclusive communication that are aimed at improving cancer screening and health outcomes for understudied populations that may benefit most. Improving cancer-related beliefs and health-information-seeking attitudes among underserved populations, particularly Asian/Pacific Islanders and individuals who are unemployed or disabled, is essential to increasing screening uptake and reducing disparities in cancer outcomes. In conclusion, addressing the broader social and cultural context in which people form health beliefs is critical to achieving meaningful behavior change and health equity in cancer prevention.
Footnotes
Ethical Approval
The Oregon Health & Science University (OHSU) Institutional Review Board (Portland, Oregon, USA) approved this cross-sectional study as exempt for the use of secondary data analyses. The approval number is STUDY00027335, and the date of approval is May 31, 2024. Informed consent was waived by the IRB due to the use of de-identified data.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the National Cancer Institute 5P30CA016672 (J. Shannon). We also thank the Knight Cancer Institute’s Cancer Center Support Grant P30CA69533.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.