
Abstract
Introduction
The deaf and hard of hearing (DHH) community experiences lower cancer screening rates than the general population. Cancer worry and fatalism can influence cancer screening, along with race, and the interaction of intrinsic factors with DHH health behavior needs to be investigated.
Objectives
The study examines the association of the intersection of race and hearing status with cancer worry and fatalism.
Methods
This study analyzed cross-sectional survey data from NCI HINTS-ASL (for DHH adults) and NCI HINTS (for hearing adults). Multivariable logistic regression models were used to assess (i) the association of race-hearing status intersection with cancer worry and fatalism, as well as (ii) the relationship between hearing status and outcomes within each race.
Results
The study found that the overall interaction between race and hearing status was significantly associated with both high cancer worry and fatalism, with African American (AA)/Black and Asian/Other having higher odds of worry [1.17 (0.83, 1.64); 1.19 (0.85, 1.66), respectively] and other groups having lower worry than White hearing (P < 0.0001), and all deaf having less concern about cancer fatalism (P < 0.0001). Within each racial group, White DHH respondents had lower odds of cancer worry [aOR (95% CI): 0.72 (0.58, 0.91); P < 0.01] and fatalism [0.55 (0.46, 0.67); P < 0.0001] compared to White hearing respondents, while DHH AA/Black [1.89 (1.06, 3.37); P = 0.03], Asian/Other [2.39 (1.06, 3.37); P = 0.03], and Hispanic [1.95 (1.18, 3.22); P < 0.01] respondents had significantly higher odds of cancer worry and lower odds of cancer fatalism [Black: 0.50 (0.23, 1.09); P = 0.07; Asian/Other: [0.68 (0.42, 1.09); P = 0.10]; Hispanic: [0.69 (0.40, 1.17)]; P = 0.16] compared to their hearing counterparts.
Conclusion
DHH individuals have different odds of experiencing cancer worry and fatalism compared to their hearing counterparts. Inclusion of individuals with sensory disabilities in a larger cancer study sample enriches the diversity of perspectives, ensuring that the findings reflect a broader range of experiences and needs. More research into contributory factors in the signing DHH population is needed.
Plain Language Summary
The deaf and hard of hearing (DHH) community shows lower cancer screening rates than the general population. This study explores how concerns and negative beliefs about cancer (known as cancer worry and fatalism) are different between DHH and hearing people from racial groups.
Introduction
Despite evidence that cancer screening reduces morbidity and mortality, certain subgroups of the deaf and hard of hearing (DHH) population that uses American Sign Language (ASL) receive screening at markedly lower rates than the general population.1-4 DHH people generally receive less cancer screening because of factors ranging from limited cancer knowledge to barriers in communication during shared decision-making. What remains to be investigated are specific intrinsic factors that may be contributing to this disparity. Some of these intrinsic factors include information seeking and socioeconomic status, both of which can influence cancer worry (defined as the “negative-valenced responses experienced by individuals regarding cancer as an uncertain health issue.” 5 ) and fatalism “the belief that death is inevitable in the presence of cancer and that being diagnosed with cancer is predetermined and beyond the control of the individual.” 6 ). The degree of cancer worry and fatalism may also be influenced by access to cancer-related information.7,8 While the relationship of interrelating intrinsic factors with health outcomes have been investigated with the DHH population,9-13 there is scant literature investigating the role of cancer worry and fatalism among DHH adults.14,15
Cancer worry can also be described as “an emotional reaction to the threat of cancer.” 13 Studies on the relationship between cancer worry and cancer screening uptake are mixed. Cancer worry has been found to either promote or deter cancer screening uptake, depending on the level of worry. One study proposed that the complex relationship is characterized by an inverted U shape-- high and low levels of worry can deter screening and moderate levels can encourage it. 16 Another study, among families at increased risk of breast/ovarian cancer, supports the idea that moderate worry about cancer can promote screening. 15
Loosely paralleling the relationship between cancer worry and screening, the association between cancer fatalism (distinct from cancer worry) and cancer screening may be weak or strong, despite adjusting for background variables.6,16 In other words, people with fatalistic thinking about cancer may either seek or avoid cancer screening. 17
There are numerous studies on cancer worry and fatalism that examine various groups and underrepresented populations. The National Institutes of Health’s (NIH) Health Information National Trends Survey (HINTS; https://hints.cancer.gov/) 18 items address cancer worry and cancer fatalism. These survey items create opportunities for exploring relationships between cancer and sociodemographic variables, most notably: race. For example, previous studies of HINTS measures indicate that race may play a role in the relationship between cancer worry and outcome fatalism.19-22 Race has been directly associated with likelihood of cancer worry, with a study exploring the role of socioeconomic status (SES) on the differences in cancer beliefs, cognitions, and emotions between non-Hispanic Black people and non-Hispanic White people showing lower rates of cancer worry among Black participants. 19 However, Black people experiencing low education and income were more likely to demonstrate higher cancer outcome fatalism compared to non-Hispanic White people. The same study asserts that SES and race together in a social class-driven society perpetuates racial gaps in cancer worry and fatalism. 19
In the DHH community, health outcomes among racial subgroups compared to their hearing counterparts are slowly being brought to light after years of being pooled into 1 big “People of Color” group and compared to DHH White people in analyses.23,24 Cancer-related outcomes and other measures among DHH adults are even more understudied, much less the relationship between cancer behavior and perceptions in this population.
No study has previously evaluated the intersection of race and hearing status with cancer worry and outcome fatalism, which is the focus of our study. We chose to focus on cancer worry and fatalism to clarify each of their roles in each DHH person’s cancer outcome—do findings in hearing individuals also hold true for those who are DHH? If there is a difference, then this is important because the unique lived experiences of DHH racial subgroups should be considered in developing recommendations and interventions for heterogenous minority populations such as the DHH community. Our research questions were: (1) Is there an interaction between race and hearing status for cancer worry and cancer fatalism after adjusting for other characteristics?; and (2) For each racial group, do cancer worry and cancer fatalism differ between deaf and hearing people after adjusting for other characteristics?
Materials and Methods
Study Design and Survey Questionnaire
Gallaudet DHH data collection
The Institutional Review Board of Gallaudet University in Washington, D.C. on June 15, 2016 approved (PJID #2774) an earlier cross-sectional research study (2017-2023) from which unweighted data was drawn to conduct secondary analyses for this paper. In that study, adult participants (18 years and older), and DHH (defined as having experienced bilateral hearing loss by the age of 13) answered a set of questions about demographics, health indicators (eg, regular provider), and their perceptions of cancer (see Kushalnagar et al., 2017, for more information). 25 All of these questions were administered in ASL and English.
Research staff began recruitment through national channels with focus on DHH community members who use ASL. Several approaches were used for recruiting DHH signers across the USA, including Hawaii, Alaska, and Puerto Rico. Approaches included personal networks, distributing flyers to DHH community organizations, institutions, and platforms, and posting on deaf-centered organization websites and e-newsletters (eg, Gallaudet University, National Black Deaf Advocates, state Associations of the Deaf, etc.). Research staff provided prospective participants with an information flyer, discussed the study purpose and procedures, reviewed inclusion and exclusion criteria, and answered any questions they might have had to determine eligibility and interest.
Individuals who self-reported that they used ASL as their primary language were included in the study. Individuals who were 17 years old or younger, as well as those who had unilateral hearing loss were excluded. Participants provided signed informed consent before enrolling in the study. The online survey took approximately 1 hour to complete, with research staff available in-person or over videophone for support when technology was not available or participants needed further assistance. No names or identifying information were collected as part of this online survey. Participants were given a $25 valued gift card as a gratuity.
NCI HINTS 5, Cycle 1
The Health Information National Trends Survey 5, Cycle 1 was administered by mail between January 25 and May 5, 2017 “to provide the National Cancer Institute with a comprehensive assessment of the American public’s current access and use of information about cancer across the cancer care continuum from cancer prevention, early detection, diagnosis, treatment and survivorship”. This was a multi-stage national survey of civilian, non-institutionalized adults in the US. The first stage was a sample of addresses from the strata of “low” and “high” minority areas with an oversampling from the “high” minority areas. The next stage selected an adult (aged 18± years) from each household. The respondents were asked whether they were “deaf” or not. All respondents were assigned a final weight and a set of 50 replicate weights that accounted for the sample design and non-response. We used data only from respondents who responded to the English survey and did not report being deaf from this survey for our secondary data analysis. 26
Questions
The research questions are shown in Figure 1. HINTS survey items used to measure outcome (cancer worry and cancer fatalism) and covariate (cancer avoidance) variables.
The survey responses for cancer worry, cancer fatalism, and cancer avoidance questions as listed in Figure 1 were recoded into dichotomous variables. This was done to increase the likelihood of true distinction between the “low and high” worry scales and the “agree and disagree” scales, which had little to no difference in the individual responses. 27
Statistical Analyses
The reporting of this study followed STROBE guidelines. 28 The 2 data sets were merged; the final sample weight and the replicate weights were set to 1 for the unweighted data for the deaf and the weights provided by HINTS were used for the hearing respondents. 26 All analyses with complete data used the final weight and the replicate weights to obtain the point estimates and jackknife variance estimates and were conducted in SAS 9.4 (SAS Institute, Cary, NC, USA) and SUDAAN 11.0.4 (RTI International, NC, USA). A two-sided P < 0.05 was considered significant.
The main outcomes—cancer worry (low, high), perceived cancer fatality (agree, disagree) and the covariate cancer avoidance (agree, disagree)—were re-categorized as shown in Figure 1. The categories for the other variables were as follows: race/ethnicity - White, African American (AA)/Black, Asian/Other and Hispanic; education - high school degree or less (HS), some college, college degree; gender - male, female; having a regular provider - no, yes; and hearing status - deaf, hearing. Age was considered as a continuous variable.
Summary statistics (proportions, means, standard errors (SE)) were obtained for all characteristics by hearing status (Deaf/Hearing). Significance of the differences in the character distributions between the groups were tested with chi-square test (categorical variables: race/ethnicity, education, gender, having a regular provider, cancer avoidance, worried about cancer and thinking about death when thinking about cancer) and the Wald-F (continuous variables: age in years).
Adjusted odds ratios (aOR) and 95% confidence intervals (CI) were obtained from separate multivariable logistic regression models to (i) assess whether the interaction between race and hearing status was associated with the outcomes (high cancer worry and cancer fatalism); (ii) assess the relationship of hearing status with the outcomes within each race category. Regressions adjusted for age (continuous), gender (female/male), education (high school/some college/college graduate), regular provider (no/yes), and cancer avoidance (low/high). Because cancer avoidance has similar distribution across hearing status and is associated with the study outcomes (cancer worry and fatalism),29,30 it was included as a covariate in the regression model.
Data Availability
The primary data from HINTS 5, Cycle 1 is publicly available on the National Cancer Institute’s HINTS website’s Public Use Dataset (https://hints.cancer.gov/data/download-data.aspx). The secondary data generated in this study from HINTS-ASL are available upon reasonable request to the corresponding author.
Results
Distribution of Respondent Characteristics by Hearing Status.

aBased on the two-sided chi-square test or the Wald-F test.
bWeighted estimates.
cMight not add to the total due to missing values.
Adjusted Odds Ratios (aOR), 95% Confidence Intervals (CI), and P-Values Obtained From 2 Separate Multivariable Logistic Regressions Associating Characteristics With High Worry and Perceived Cancer Fatalism (Reported as Agree to Thinking About Death When Thinking About Cancer). a

aAdjusted for Age in years (continuous), Gender (Female/Male), Education (<=HS/Some college/College graduate), Regular Provider (No/Yes) and Cancer Avoidance (Low/High). Used final weight and replicate weights for the Jackknife variance estimates.
The overall interaction between race and hearing status was significantly associated with high cancer worry (P < 0.0001). Compared with White hearing respondents, non-Hispanic White DHH, Hispanic DHH respondents, non-Hispanic AA/Black hearing, hearing non-Hispanic Asian/Other respondents and hearing Hispanic had lower odds of cancer worry [aOR (95% CI): 0.76 (0.59,0.99), 0.92 (0.62, 1.35), 0.86 (0.52, 1.42), 0.58 (0.30, 1.10), and 0.69 (0.47, 1.02), respectively]. Conversely, non-Hispanic DHH African American/Black and non-Hispanic DHH Asian/Other had higher odds [1.17 (0.83, 1.64) and 1.19 (0.85, 1.66), respectively] of cancer worry.
The overall interaction between race and hearing status was also significantly associated with cancer fatalism (P < 0.0001); compared with White hearing, DHH White, DHH African American/Black, DHH Asian/Other, and DHH Hispanic respondents all had lower odds of cancer fatalism [0.56 (0.48, 0.66), 0.54 (0.43, 0.69), 0.81 (0.64, 1.02), and 0.82 (0.64, 1.05), respectively] while hearing AA/Black, hearing Asian/Other and hearing Hispanic respondents had higher odds [1.27 (0.88, 1.84), 1.12 (0.74, 1.69), and 1.21 (0.74, 1.97), respectively] of cancer fatalism. Although the DHH all had lower odds, the DHH White and Black had almost half the odds while the AA/Black had the highest odds among all the hearing persons.
Adjusted Odds Ratios (aOR), 95% Confidence Intervals (CI), and P-Values Obtained From 2 Separate Multivariable Logistic Regressions Associating Characteristics With High Worry and Cancer Fatalism Within Each Race Group a .
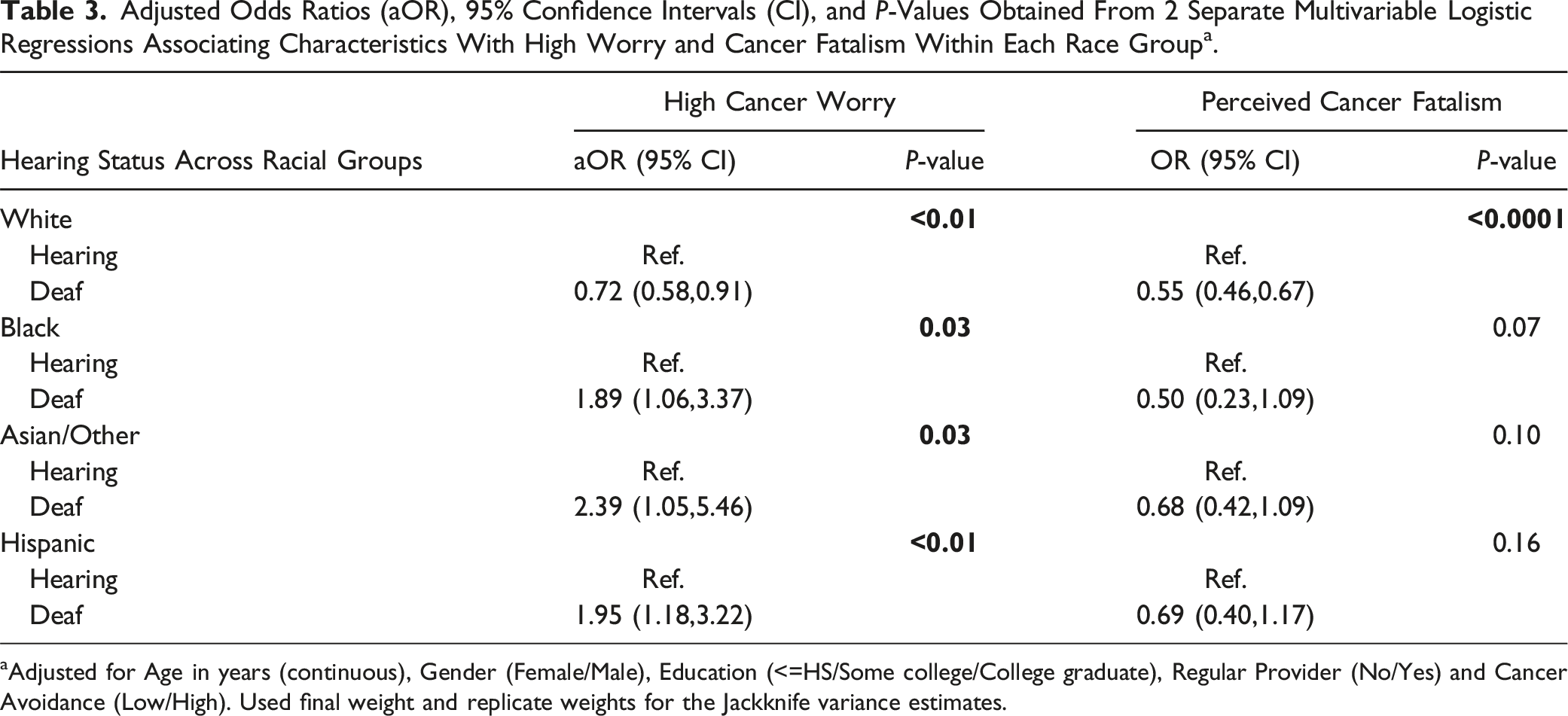
aAdjusted for Age in years (continuous), Gender (Female/Male), Education (<=HS/Some college/College graduate), Regular Provider (No/Yes) and Cancer Avoidance (Low/High). Used final weight and replicate weights for the Jackknife variance estimates.
African American/Black DHH and hearing respondents were significantly more likely to report high cancer worry [1.89 (1.06, 13.37); P = 0.03]; however, African American/Black DHH people had lower odds of experiencing cancer fatalism [0.50 (0.23, 1.09); P = 0.07].
Results for Asian/Other and Hispanics were similar to that of the African Americans/Blacks with DHH counterparts more likely to report high cancer worry [2.39 (1.05, 5.46); P = 0.03 for Asian/Other and 1.95 (1.18, 3.22); P < 0.01 for Hispanic, respectively] and lower perception of cancer fatalism [0.68 (0.42, 1.09); P = 0.10 and 0.69 (0.40, 1.17); P = 0.16] than their hearing counterparts.
Supplementary Tables S1 through S4 details the logistic regression models assessing the relationship of hearing status with cancer worry and cancer fatalism for each racial group, with the hearing population in the racial group of focus as the reference within each model. The statistical influence of cancer avoidance for each group is also displayed in the Supplementary Tables.
Discussion
Our study findings showed an association between cancer fatalism and the overall intersection of race and hearing status. We also found associations between cancer worry and the overall intersection of race and hearing status. Below, we describe and discuss our findings of cancer worry and cancer fatalism across hearing status within racial groups, then in the overall DHH population.
Cancer Worry Across Hearing Status Within Each Racial Group
Within the non-Hispanic White DHH group, significant interaction was observed for cancer worry and hearing status, with lower odds of reporting high rates of cancer worry, compared to White hearing respondents (more of whom have higher odds of reported higher rates of cancer worry). Conversely, DHH individuals who are non-Hispanic African American/Black, Asian/Other, and Hispanic were more likely to report higher rates of cancer worry compared to hearing respondents. This difference in cancer worry is interesting, since 55% of the DHH participants were found to have college degrees. The role of education being associated with higher health literacy might not be as robust in the community due to cultural and linguistic barriers affecting access, understanding, and proper utilization of health-related information. The interaction of race and education within the DHH population with health literacy could shed some insight on why and how DHH individuals of different races with different educational attainment perceive cancer risks as they do. A systematic review focusing on cancer health literacy in the DHH patient population have considered the effect of degree of hearing loss and of preference for audio vs text vs sign language for information. 10 Another study into the role of internal health locus of control (IHLC) on DHH women’s cervical cancer information assimilation showed that IHLC scores didn’t significantly predict greater cervical cancer knowledge over time, even with a sample that skewed to highly educated participants. 31 This does suggest the need for a study into the relationships between cancer health literacy, health behaviors, and cancer perceptions within the signing DHH community to better explain the findings from this study.
Cancer Fatalism Across Hearing Status Within Each Racial Group
For cancer fatalism, within racial group analyses indicated that DHH respondents were more likely to report lower rates of cancer fatalism compared to hearing respondents . Additionally, within the non-Hispanic White subsample, fatalism was observed to be significantly lower among DHH compared to hearing non-Hispanic White respondents. This finding is interesting, since, in the general population, fatalistic beliefs about cancer are often higher among people who self-identify as belonging to a racial and ethnic minority group, compared with non-Hispanic white people. 32 A review of several studies with adults from racial and ethnic minority groups appears to suggest that low health literacy may increase fatalistic beliefs and lower knowledge of cancer risk factors.32-35 These studies focus on hearing individuals from various racial and ethnic minority groups and their results are not necessarily generalizable to the DHH population, who often do not have access to auditorily-delivered health information in a primarily-speaking society. Having a college degree, as 55% of the DHH participants in this study do, does not always necessarily translate into high health literacy. The relationship between education/degree attainment and health literacy in the DHH community might not be robust due to limited access to information, as briefly touched on in the preceding subsection and further discussed below.
Cancer Worry and Cancer Fatalism in the DHH Population
Thus, the findings that DHH people from minoritized ethnoracial groups having higher rates of cancer worry and lower odds of fatalistic beliefs than hearing people from minoritized ethnoracial groups might be influenced by sociocognitive factors that may be explained beyond race and hearing status. For example, an individual who is DHH and does not have access to cancer information may not have sufficient information to rationalize the risks of cancer and might end up insufficiently assessing the lethality of cancer. Studies that reported a connection between low health literacy and fatalistic beliefs about cancer did not include DHH individuals in their samples. Low health-literate individuals in these studies are able to hear and therefore may have had access to some cancer information in a primarily auditory speaking environment. The information that they gained access to may be inadequate yet adequate to create a level of fatalistic beliefs about cancer.
DHH signers generally have limited avenues of accessing verifiable health information in a primarily speaking society. They are often restricted to in-person discussions with health care providers, which comes with its own set of barriers.8,36-38 Widely disseminated and easily accessible sources of cancer-specific health information in ASL 39 along with increased opportunities to discuss the topic with health literate sources in sign language, may improve DHH individuals’ ability to internalize and objectively evaluate their risk perceptions of cancer. Objective evaluation of cancer information is contingent on DHH individuals having sufficient levels of health literacy, which may be impacted by incidental learning opportunities frequently limited to auditory mediums.40,41
A national study exploring cancer fatalism, health literacy, and cancer information seeking in the US public showed that people who had limited health literacy were less likely to have ever sought cancer information and more likely to endorse fatalistic beliefs about cancer. 35 This prior research drove the initial speculation that DHH individuals would be more likely to report higher cancer worry and fatalistic thinking. Since this study’s findings show that DHH adults belonging to racial and ethnic minority groups do indeed report higher odds of worrying about cancer when compared to hearing counterparts, this affirms the initial speculation regarding cancer worry, with the exception of White DHH adults’ lower odds of experiencing high cancer worry.
As for cancer fatalism, the study findings indicate that there is a need to elucidate the factors contributing to the lower rates of cancer fatalism in White DHH individuals compared to White hearing individuals, alongside the non-significant reduced odds of fatalistic thinking among DHH individuals identifying with other racial and ethnic groups. A factor that must be considered is the intersection of race and DHH identities. For instance, hearing individuals who have low functional health literacy will still be able to acquire incidental information about cancer through multiple sources, both visual and auditory, which can contribute to increasing their fatalistic thinking about cancer. However, DHH individuals do not have the same breadth of access to cancer information as hearing individuals, which can affect their rates of cancer worry and fatalism. The role of limited health literacy on cancer risk perception and fatalistic thinking may be heightened for DHH individuals who belong to racial and ethnic minority groups in the US that are historically medically underserved and may have culturally-influenced attitudes towards cancer.
Strengths and Limitations
This study has strengths and limitations. While self-selection was a limitation in our study, there are several strengths. This study included ASL and English languages in the survey. For participants who did not have technology, we provided face to face interviews and aided them with completing the survey. Finally, the study sample is geographically diverse with respondents living across USA, Puerto Rico, Hawaii, and Alaska.
Besides self-selection, another limitation was that DHH participants who are college graduates were overrepresented in the DHH dataset, with 4% more than the observed 51% in the DHH population (see Garberglio et al, 2019). 42 Some research has shown that higher levels of education are correlated with increased cancer worry, but this is not necessarily generalizable to the DHH signing community. 43 Increased recruitment among DHH who have attained lower levels of education as well as specific racial groups might aid in confirming our findings. Also, due to the cross-sectional nature of the data, strong and accurate causal inferences cannot be made between the study variables, but the presence of significant associations between race and hearing status with cancer worry and fatalism reveals a need to further explore this phenomenon within the DHH population.
Conclusion
This study integrates existing literature on cancer worry and risk perceptions, such as fatalism, with available information regarding barriers to health care for the ASL-using DHH community. This study is relevant due to the dearth of literature on the mentioned topics, and the authors hope this study engenders further attention to—and research—into the interplay of cancer, risk perceptions and behaviors, and the ASL-using DHH community. While this study notes differences between DHH adults compared to hearing counterparts for cancer worry and fatalism, addressing those differences requires some type of educational intervention in the DHH community. Future studies should apply the lens of racial and ethnic differences when creating clinical or educational interventions to improve cancer screening rates and ensure reasonable levels of cancer worry and fatalism among deaf, deafblind, and hard of hearing people who use sign language.
The DHH community would benefit from increased discussions around cancer screening, diagnosis, and treatment. The focus should be on facilitating access to information for DHH, while recognizing that racial differences in the community can be mediated by variables such as socioeconomic status and education.19,37,38 ASL-using Community Health Workers or Navigators (CHW/CHN) as part of an integrative health medicine model could be a valuable resource in providing cancer information to DHH people who are not up-to-date on cancer screenings. 44 CHWs/CHNs or equivalent figures may help inform DHH people about cancer knowledge and empower them to seek out credible and accurate cancer information, coping strategies, and boost overall health literacy.
Additionally, DHH racial and ethnic communities have national organizations (eg, National Association of the Deaf, National Black Deaf Advocates, Council De Manos, National Deaf Asian Congress), where opportunities to disseminate cancer-related health information could be capitalized on. Most of the aforementioned national organizations also have state or local chapters that can prioritize the topic of education and participate in partnerships with local health systems and resources to promote the health of the regional signing DHH communities. Creating asynergy between organizations, health systems, signing CHW/CHNs, and DHH community leaders in addressing disparities in cancer knowledge and decision making is significant and has strong potentials to lead to marked positive changes in cancer knowledge and outcomes.
Future Directions
A model may be needed to define the threshold of literacy required to appropriately apply knowledge towards managing healthy levels of cancer worry and fatalism. The health care system needs a better understanding of how health literacy, information seeking, and attitudes towards cancer influence the DHH community’s cancer worry and fatalism. Effective cancer education that communicates accurate information can empower community members to take a healthier, more proactive approach to cancer screening and treatment, with manageable levels of worry and fatalistic thinking about cancer.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Study was funded by NIH 8U01DC021718-02 grant and diversity supplement grant 8U01DC021718-02S1, both awarded to PI Poorna Kushalnagar, Ph.D.