
Abstract
Cervical cancer is the fourth most common cancer affecting women worldwide, and the second leading cancer in Ethiopia. Screening gives protective benefits associated with a reduction in the incidence of invasive cervical cancer and mortality. However, the level of cervical cancer screening uptake is not well document in the country. This study aimed to determine the prevalence and predictors of cervical cancer screening service uptake among women aged 25 years and above in Sidama zone, southern Ethiopia, 2019. A cross-sectional study was conducted among 838 women aged 25 and above years by using an interviewer-administered questionnaire. Multi-stage sampling technique was employed to identify households with women age of 25 and above years who were residing in the selected kebele for more than 6 months. Descriptive and multivariable logistic regression done. P-value <0.05 was considered as significant and presented by adjusted odds ratio (AOR) with 95% C.I. This study showed that among 838 women, only 17.8% (95%CI, 15.2%-20.5%) have undergone for cervical cancer screening. Being age of 35-39 (AOR = 5.2, 95% CI = 2.6-10.6), College and above Educational level (AOR = 3.8, 95% CI = 1.5-9.6), Ever had HIV test (AOR = 2.8, 95% CI = 1.82-4.4) and high perceived self-efficacy (AOR = 4.4, 95% CI = 1.527-12.84) were significant predictors for cervical cancer screening service uptake. The magnitude of cervical cancer screening uptake among women aged 25 years and above was lower than that of the recommended coverage of the target group by the national guideline. Age of women, educational status of women, ever had HIV test, and high perceived self-efficacy were important factors of cervical cancer screening service uptake. So it is very crucial improving cervical cancer screening uptake, through creating awareness and educating women, about the advantage of screening in early detection and management of cervical cancer screening utilization
Introduction
Cervical cancer is the growth of abnormal cells on the lining of the cervix. here are 2 main types of cervical cancers, Squamous cell carcinoma (SCC) which is the most common type, accounting for about 7 out of 10 (70%) cases and Adenocarcinoma which is a less common type (about 25% of cases), starts in the glandular cells of the cervix. 1
The primary cause of cervical pre-cancer and Squamous cervical cancer is persistent or chronic infection with one or more of the high-risk (cancer-causing or oncogenic) types of Human papillomavirus (HPV), Though there are more than 100 types of HPVs, 7 out of 10 (70%) of only 2 types of HPV:16 cause all cervical cancer cases reported throughout the world and 18. 2
Besides HPV, cervical cancer, early sexual intercourse, parity, having multiple sexual partners, smoking, low immune status and sexually transmitted infection (STI) and co-infection, oral contraceptive and occupation are among the commonly reported risk. 3
Cervical cancer is the fourth most common cancer affecting women worldwide, in 2012, globally 528,000 new cervical cases and 266,000 deaths are estimated. Almost 70% of the global burden falls in areas with lower levels of development. 4 There are some high-risk regions, with estimated age-specific rates 30 and above per 100, 000, including Eastern Africa (42.7), Melanesia (33.3), Southern (31.5) and middle Africa (30.6). Cervical cancer remains the most common cancer in eastern and middle Africa. 5 In Ethiopia, it estimated that 29.43 million women were at risk of developing cervical cancer, with an estimated 7,095 and 4,752 annual numbers of new cases and deaths, respectively. 6,7 It is one of the second leading cause of cancer among all women and the leading cause of cancer-related deaths among women 15 to 44 old years. About 4.8% of women in the general population are estimated to harbour cervical HPV-16/18 infection at a given time, and 67.9% of invasive cervical cancers attributed to HPV 16 or 18. 7
Early detection of cervical cancer, by screening all women in the target age 25 years and above for HPV, followed by treatment of detected precancerous lesions can prevent the progression to cancer. Some of the strategies suggested by Ethiopia national cervical cancer prevention program (ENCCP) are population-based cervical cancer screening using (visual screening using acetic acid) VIA for all women aged 30-49 every 5 years and screened women positive on VIA cryotherapy as a treatment option. 8
In Ethiopia, the planned screening coverage was 80%, but not achieved. The data from some health facility compiled from 1996-2008 showed that 30.3% of all cancers diagnosed were cervical cancer. The estimated coverage of cytology-based cervical cancer screening is 1.6% in urban and 0.4% in a rural area. 9 The estimation needs to be aided by assessment results, and the service uptake needs improvement. So, optimizing the estimated low cervical cancer screening service utilization needs direct researches to come-up with valid population-specific and nationwide assessment result statistics, identification of factors and information about uptake of cervical cancer screening. However, few studies were done in different corners of the country, and most of them were among different each other by their study population. Therefore, this study aimed to determine cervical cancer screening service uptake and associated factors among women age 25 and above in Sidama Zone, southern Ethiopia.
Methods and Materials
Study Area
The study was conducted in Sidama zone. Three districts were selected randomly. Sidama zone is one of the 14 zones in SNNPR, and it is located in the Northeastern part of the region. The administration of Sidama zone located at 275 km south of Addis Ababa. The zone covers a total area of about 698.8km2, and it consists of 30 woreda and 7 administrative towns and 596 (526 rural 70 urban) kebele (the lowest administrative hierarchy). It is one of the most densely populated zones. The zone has a population density of 451.83 per square km according to 2007 Ethiopia central statistics agency (CSA) census. According to the data from Sidama Zonal Health department report by 2019, The Sidama Zone population estimates for the year 2018/ 2019 is 3,893,816 of which 1,939,120 are male, and 1,954,696 of them are female. From the total female population, 61 percent 1,192,364 women’s are aged 25 years below. 10
Study Design and Period
The community-based cross-sectional study design was employed from February 5 to March 15/2019 in the Sidama zone.
Population and Eligibility
All women aged 25 years and above, who resided the Sidama zone, in 3 randomly selected kebele during the study period, were used for the interview. The first household was randomly selected using the simple random sampling, and the rest was identified by calculating the interval of the sampling ‘k’ value. The women interviewed for data collection was a resident for at least 6 months and was able to respond to the interviewer. The age of the women identified for the interview was at least 25 years of age.
Sample Size Determination
The sample size was determined using a single population proportion formula based on 95% confidence interval. The margin of error was taken 4% and assuming the uptake of cervical cancer screening 19.8% based on data from a previous study on a similar population in Mekelle, Northern Ethiopia. 11
Based on these assumptions, the sample size was 381 after added 10% none respondent rate and multiplying with the design effect of 2. The final sample was 838.
Sampling Method
Multi-stage sampling technique method was employed. From the 19 Sidama zone districts, 3 districts were selected using simple random sampling. From 3 selected districts have a total of 75 kebeles. Of these 13 representing kebele were selected based on a simple random sampling. At the last stage of the sampling procedure, 838 households were selected from 3518 households using a systematic random sampling technique. The total sample size was distributed to each district selected kebele proportionate to the size of their households.
The sampling frame was taken from households’ folder of the health extension workers after checking for an update from their respective kebele listing. After Folders checked for updated, a rapid survey was conducted in that selected kebele to get target households. After getting sampling frame, women aged 25 years and above were selected from each kebele by using systematic sampling technique at the regular interval after giving code for each target households.
Data Collection Tools and Procedures
The structured questionnaire was used after adapted and modified from different kinds of literature. 12 The questionnaire was developed in English and translated to the local language and then back-translated to English to check for its consistency. A pre-test was done among 5% of households Hawassa zuria district. Based on the pre-test, corrections were made on the questionnaire.
The eligible women were interviewed from house to house by trained data collectors, and supervision was conducted on the process of the data collection.
The data was collected by 6 BSc holder nurses and 2 supervisors who have a Master degree in public health. They are fluent in the local language. Training was given for data collectors and supervisors for 3 days.
Data Quality Assurance
Data quality was assured by using a structured, pre-tested and interviewer-administered questionnaire. The questionnaire was assessed for clarity, and challenging questions to understand and respond were rephrased. Six data collectors and 2 supervisors were used to collecting data and supervision. Data collectors and supervisors trained for 3 days before data collection. Consistency and completeness were checked in the daily base during the interview period by supper visors and principal investigator. Again at the end of each days, the principal investigator was collected the all filled questionnaire during day time from data collectors and was checked for completeness and consistency. The necessary feedback given to the data collectors and supervision conducted accordingly.
Data Management and Analysis Plan
The entire filled questionnaires were checked for incompleteness and inconsistency. Data were coded and entered into Epi-data version 3.1 and was exported to SPSS version 20 for statistical analysis. Descriptive statistical analysis was used to compute frequency, percentage and mean for independent and dependent variables. A crude and adjusted odds ratio from Bivariate and multivariate logistic regression analyses were used to measure the association between variables. All Variables with (P < 0.25) in the bivariate logistic analysis were entered into the multivariate logistic analysis. It was done to increase the number of variables to have to be included in the model. Multicollinearity effect was checked by using a linear diagnostic test of mean-variance inflation factor (VIF) at a cutoff point 10. The Hosmer-Lemeshow goodness of fit test was used to check whether the model adequately fits the data with p-value (p > 0.05). Logistic regression was used to adjust for possible confounding variables. Odds ratio with 95% CI, P-values below 0.05 was considered significant.
Study Variables and Their Measurements
The dependent variable is cervical cancer screening uptake. Factors included in the model as independent variables are, Socio-demographic factors (age, educational status, occupation, marital status), Perception of women on cervical cancer screening (perceive susceptibility, severity, benefit, self-efficacy, cues to action and barriers), knowledge on risk factors (early sexual intercourse, having multiple sexual partners, use of modern oral contraceptive and multiparty), Associated factors (knowledge, HIV and STI).
Perceived susceptibility
Participants whose answers regarding susceptibility to cervical cancer from provided 5 items, whose median were below 3 were considered as low perceived susceptibility and above 3 were considered as high perceived susceptibility. 13
Perceived benefits
Participants whose answers regarding benefits to cervical cancer from provided 5 items, whose median were below 3 were considered as low perceived benefits and above 3 were considered as high perceived benefits. 13
Perceived barriers
Participants whose answers regarding barriers to cervical cancer from provided 10 items, whose median were below 3 were considered as low perceived barriers and above 3 were considered as high perceived barriers. 13
Perceived severity
Participants whose answers regarding barriers to cervical cancer from provided 8 items, whose median were below 3 were considered as low perceived severity and above 3 were considered as high perceived severity. 13
Perceived self-efficacy
Participants whose answers regarding self-efficacy to cervical cancer screening from provided 5 items, whose median were below 3 were considered as low perceived self-efficacy and above 3 were considered as high perceived self-efficacy. 13
Cues to actions
Participants whose answers regarding cues to actions to cervical cancer screening from provided 7 items, whose median were below 3 were considered as low perceived cues to actions and above 3 were considered as high perceived cues to actions. 13
Knowledge was assessed by categorizing into 3. Good knowledge were whose answers regarding knowledge of the risk of cervical cancer, viewed 8 items were scored 32 to 40 from 40 points (80-100%), satisfactory knowledge was those answered 24-28 from 40 points (60-70%), and poor knowledge were those answered below 24 from 40 points (<60%). 14
Result
Socio-Demographic Characteristics of the Study Participants
A total of 838 mothers were included in the study, with a response rate of 100%. The mean age of participants is 36.19 ± 6.380 S.D. years, with a minimum of 25 and maximum of 49 years. The study participants were dominantly protestant, which is 690(82.3%) followed by Catholic 79 (9.4%). The majority, 813 (97%) of study subjects were married. Of all 333 (39.7%) were attended primary school, 673 (80.3%) were housewives, 85 (10.1%) self-employed and 51 (6.1%) government employees (Table 1).
Socio-Demographic Characteristics of the Selected Women Aged 25 Years and Above in Sidama Zone Southern Ethiopia, 2019.

Reproductive characteristics of women
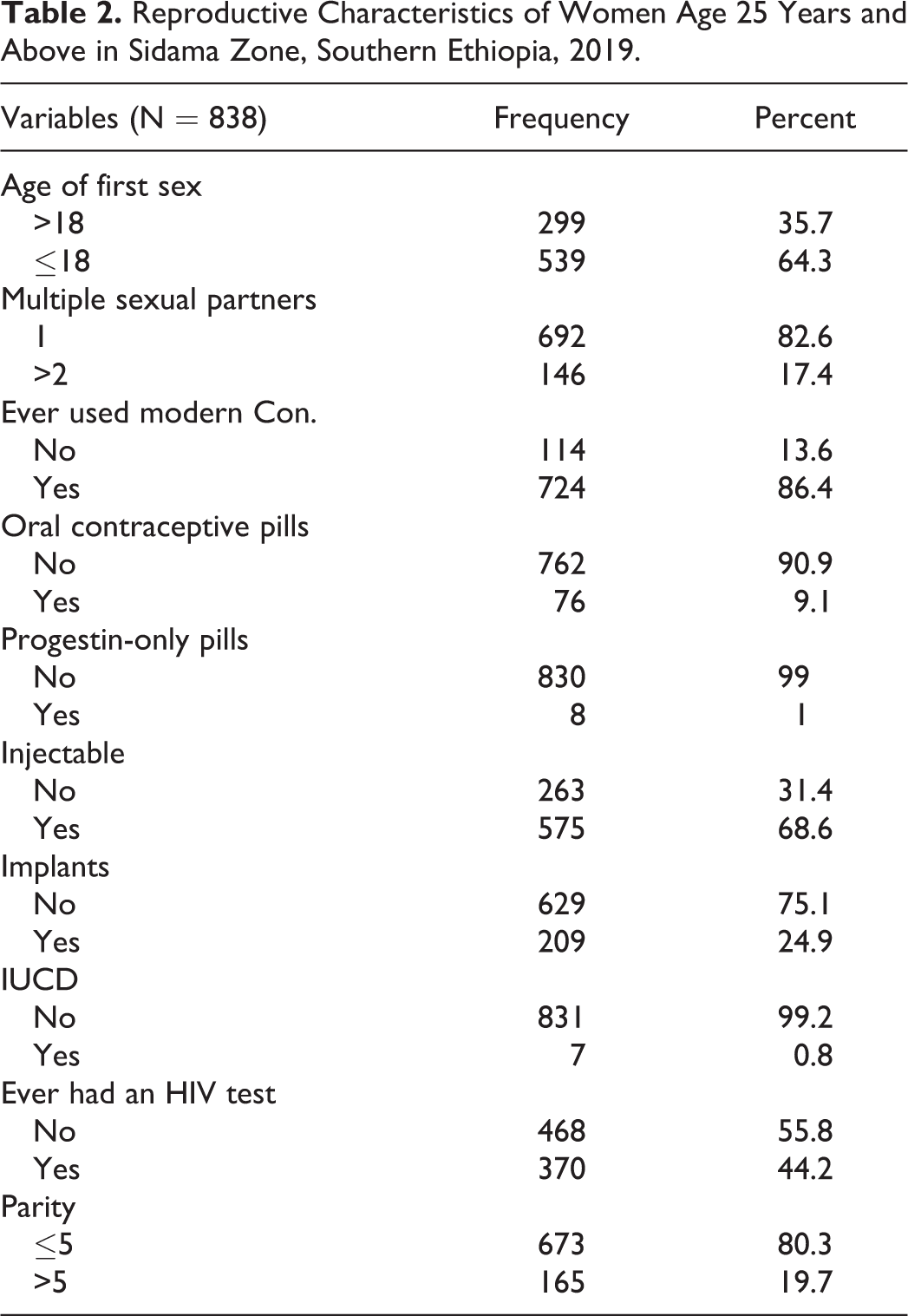
Five hundred thirty-nine women, (64.3%) had first sexual intercourse at the age of 18 or below. The mean age for first sexual intercourse was17.8 ± 1.965 with a minimum of 12 and maximum of 25 years. Majority of the women, 673 (80.3%) have given birth less than 5. Of all the respondents, 724 (86.4%) had used modern contraceptives. From those who were used modern contraceptives, 575 (68.6%) used injectable, and only 76 (9.4%) used oral contraceptives. Among the study participants, 146 (17.4%) had a history of multiple sexual partners in their life (Table 2).
Reproductive Characteristics of Women Age 25 Years and Above in Sidama Zone, Southern Ethiopia, 2019.
Knowledge of Risk Factors Associated with Cervical Cancer
Of total participants, 36(4.2%) had good knowledge of risk factors associated with cervical cancer. Majority of participants 489 (58.4%) had satisfactory knowledge, and 313 (37.4%) had poor knowledge.
Perception of Cervical Cancer Screening
Majority 764(91.2%) of the respondents had low perceived susceptibility 801(95.6%) were reported high perceived severity and 738(88.5%) high perceived benefits (Table 3).
Perception of Women Aged 25 Years and Above on Cervical Cancer Screening Uptake Among Women Aged 25 Years and Above in Sidama Zone, Southern Ethiopia, 2019 (N = 838).

Source of Information on Cervical Cancer Screening Uptake
The primary source of information for cervical cancer screening uptake was health extension workers which accounts126 (15%), followed by developmental health army52 (6.2%) and health worker32 (3.8%) (Figure 1). Cervical cancer screening uptake among the participants is found to be 149 (17.8%) at (95% CI, 15.2-20.5).

Source of information on cervical cancer screening uptake among women aged 25 years and above in Sidama zone, southern Ethiopia, 2019.
Factors Associated With Cervical Cancer Screening
After controlling for all others, women with high perceived self-efficacy, age of respondent, Educational status of respondent and HIV test were significantly associated with cervical cancer screening service uptake.
Women in the age category of 35-39 years old were 5 times more likely have cervical cancer screening uptakes when compared to women with the age category of 25-29 years old(AOR = 5.2, 95% CI = 2.5-10.6).
Study participants who attended primary education were about 2 times more likely undergo cervical cancer screening service uptakes than who have attended no formal education (AOR = 1.9, 95% CI = 1.1-3.2).
Women who ever had HIV tests were nearly 3 times more likely have cervical cancer screening uptakes when compared to women who have no practicing HIV test (AOR = 2.8, 95% CI = 1.8-4.4).
Study respondents who perceived high self-efficacy were 4times more likely to undergo cervical cancer screening uptakes when compared with perceived low self-efficacy(AOR = 4.4, 95% CI = 1.5-12.8) (Table 4).
Bivariate and Multivariate Analysis for Factors Associated With Cervical Cancer Service Uptake Among Women Aged 25 Years and Above in Sidama Zone, Southern Ethiopia, 2019.

Abbreviations: AOR, adjusted odds ratio; COR, crude odds ratio.
*=P. value < 0.05.
**=P. value < 0.01, 1 = reference.
Discussion
This study showed that among 838 women only 17.8% (95%CI, 15.2-20.5) have undergone cervical cancer screening uptake. Age of women (AOR = 3.7, 95% CI = 1.794-7.5), Educational status of women (AOR = 1.9, 95% CI = 1.1-3.2), Ever had HIV test (AOR = 2.8, 95% CI = 1.8-4.4) and high perceived self-efficacy were (AOR = 4.4, 95% CI = 1.527-12.8) were significant factors for cervical cancer screening service uptake.
This study found that the prevalence of cervical cancer screening uptake among women is 17.8% (95% CI, 15.2-20.5). This result almost consistency with the study conducted in Mekelle 19.8% (2015). The finding of this study is also higher than other studies conducted in other parts of Ethiopia, like Addis Ababa 12.8%, 15 Hawassa 11.4% (2015), 16 Hosanna Town, Hadiya zone 9.9 (2015), 17 Arba Minch town, Southern Ethiopia 5.9%, 18 Finote Selam in Amhara regional state Northwest Ethiopia 3% (2017). 19 This might be because the study was done at the initiation period of cervical cancer screening service at Health Centers and age variation among study participants which the study done in Finote Selam includes only women in age 30-49 years. Currently, in Ethiopia, the expansion of the cervical cancer screening service centers was done. An integration of services with delivery case team at the health facility level, creating awareness for Health extension workers and Health developmental army to mobilize a community for cervical cancer screening service uptakes were also done by the Government. However, it is quite low, when compared to other countries like, Jamaica 40.7%, 20 china 63.7%, 21 Brazil 73%, 5 Georgia 67%, 5 Austria 80% 5 and the neighbor country Kenya, which is Kenya 36%. 22 This may be due to variation of socioeconomic status, which leads to a difference in the level of awareness of women on cervical cancer screening service
The women in the age category of 35-39 years old were 5 times more likely to have cervical cancer screening uptakes when compared to women with the age category of 25-29 years old. This finding is consistent with the study conducted in Mekelle, 23 Addis Ababa 23 and population-based WHO steps study in Ethiopia. 24 This might be due to aged women may visit a health facility for various gynecological problems and then quickly get the screening service for cervical cancer.
The result of this study showed that women those attended at least primary education were 2 times undergone for cervical cancer screening when compared to women who were attended no formal education. This finding is similar to the study conducted in Addis Ababa 23 and Eastern China. 21 This might be due to educated women may have more awareness and information than women with no education.
From this study, women who had ever test for HIV were 3 times undergo cervical cancer screening uptake. This differs from the study conducted in rural Uganda, which was not significantly associated with ever had HIV test. 25 This is because, in Ethiopia, currently, the cancer screening service was integrated with maternal and child health services at all level of health facilities.
From this study, it indicated that women who have high perceived self-efficacy were 4 times undergo for cervical cancer screening uptakes compared to women who have low perceived self-efficacy. The similar to study conducted in Bishoftu, East Shoa. 26 This may be due to developing confidence through information dissemination for cervical cancer screening.
Conclusion
The magnitude of cervical cancer screening uptakes in this study among age-eligible women was lower than that of the recommended coverage of the target group by the national guideline. Age of women, Educational status of women, ever had HIV test and high perceived self-efficacy were important factors of cervical cancer screening service uptake. However, this screening uptake shows a recent increase in uptake in cervical cancer screening when compared to other studies conducted in Ethiopia before. This implies that the current expansion and introduction of routine cervical cancer screening free of charges and availability of service in government health institutions might be significantly improved cervical cancer screening uptakes. Health extension workers were the primary source of information for cervical cancer screening uptake. They are playing a crucial role in the increment of service utilization. So Health extension workers must emphasize on providing client-centered education.
Supplemental Material
Supplemental Material, Sampling_frame - Prevalence and Predictor of Cervical Cancer Screening Service Uptake Among Women Aged 25 Years and Above in Sidama Zone, Southern Ethiopia, Using Health Belief Model
Supplemental Material, Sampling_frame for Prevalence and Predictor of Cervical Cancer Screening Service Uptake Among Women Aged 25 Years and Above in Sidama Zone, Southern Ethiopia, Using Health Belief Model by Ermias Yunkura Gemeda, Belayneh Bekele Kare, Dereje Geleta Negera, Lalisa Gemechu Bona, Bedilu Deribe Derese, Netsanet Bogale Akale, Kurabachew Mengistu Kebede, Dubale Dulla Koboto and Achamyelesh Gebretsadik Tekle in Cancer Control
Footnotes
Authors’ Note
This study was approved by the Institutional Review Board of Hawassa University, College of Medicine and Health Sciences (No. IRB/047/11, dated 26/02/2019). The participation of study participants was voluntary. An oral consent was obtained from all participants prior to their participation in the study.
Acknowledgments
The authors hereby express their deep gratitude to Hawassa University, Vice President for Research and Technology Transfer Office, Research and Technology coordinator office of College of Medicine and Health Science for allowing us to conduct this study. We like to express our deep gratitude to 838 participants who agreed to participate in this study and the District of Sidama Zone: Yirgalem district, Shebadino district and Boricha district for their willingness and coordination to collect study data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.