
Abstract
Introduction
Cancer has been one of the major causes of death among older adults. Cancer screening is key for early detection, which may help prevent or alleviate cancer. E-health platforms have been a main discriminator of cancer-related knowledge. The Health Belief Model indicates an association between individual behaviors, intentions, and other psychological factors. Understanding the psychological mechanisms that mediate the effect of E-health use (EHU) on cancer screening intention is crucial for cancer prevention and treatment among older adults.
Methods
Cross-sectional data were from the National Trends in Health Information Survey 6 (HINTS6). Respondents aged 65-74 years were selected for the study, and the final sample size, excluding missing values, was 925. This study used a parallel mediation model to analyze the mediating role of psychological mechanisms through cancer worry and cancer fatalism. Regression analysis was conducted using SPSS to test the parallel mediation model.
Results
The study found a direct (b = .25, b p = .25, P < .001) positive association between E-health use and cancer screening intentions. In addition, this study revealed a parallel indirect association between E-health use and cancer screening intentions mediated by cancer fatalism (b = .003, b p = .003, 95% CI [.001, .004]) and cancer worry (b = .05, b p = .05, SE = .002, 95% CI [.04, .05]).
Conclusion
This study highlights the importance of EHU in promoting cancer screening intentions among older adults in the United States. Access to electronic health information can reduce cancer fatalism and increase cancer worry, ultimately leading to greater interest and intention to undergo cancer screening. These findings have implications for healthcare providers and policymakers aiming to improve cancer screening rates among older adults.
Plain Language Summary
Cancer is one of the major causes of death among older adults in the U.S. Appropriate cancer screening may facilitate early prevention or intervention of cancer and safeguard the well-being of older adults. As such, it is necessary to explore factors that encourage cancer screening among older adults. Analyzing representative data collected in the U.S., we have found that E-health use may promote cancer screening intention by increasing cancer worry while decreasing cancer fatalism. Our findings call for more accessible E-health services for older adults to potentially promote cancer screening.
Introduction
In the United States, cancer is the second leading cause of death. It is estimated that approximately 1660 people die from cancer in the United States every day, while 3 new cases of cancer are diagnosed every minute. 1 Early detection and screening are critical to improving cancer outcomes. 2 To achieve this, cancer screening is recognized as a proactive and effective measure for early detection of cancer and its prevention and treatment.2,3 The main role of cancer screening is to detect cancer at an early stage so that it can be treated in a timely manner, increasing the cure rate and reducing the mortality rate.4,5 With regular screening, potential cancers might be recognized before symptoms appear. 6 For older adults, timely cancer screening may significantly improve their survival. 7 As such, for most types of cancers, guidelines recommend regular screening among older adults between the ages of 65 and 74.8,9
E-health, the information and communication technologies (ICTs) utilized for health purposes,10,11 potentially serve as means to promote cancer screening. In response to the spread of cancer, E-health use (EHU) has been identified as a meaningful way to promote awareness and positive behaviors during the prevention and treatment phases of cancer.12,13 E-health allows people to access cancer-related knowledge quickly, efficiently, and conveniently, and implicitly influences their health behaviors and intentions.14-16 This is also the case for cancer screening, one of the most vital measures for the early detection and prevention of cancer. 17
Nonetheless, cancer screening rates among older adults remain relatively low. 18 At the same time, we know little about whether and how active EHU can promote cancer screening among older adults. In addition, older adults often face more challenges and barriers to accessing healthcare than their younger counterparts. 19 Therefore, it is crucial to identify the underlying mechanisms of how EHU influences individual health behaviors. We propose that the main reason for low cancer screening rates in the older population may be cancer fatalism (CF). In recent years, scholars have also begun to pay attention to people’s emotional responses after being exposed to cancer information on the Internet. 20 One of the key responses is cancer fatalism, which is defined as the negative belief about the causes of cancer that it cannot be prevented, diagnosed (including cancer screening), and is inevitably fatal. 21 Several studies have shown a relationship between searching for cancer information on electronic devices and CF, while demonstrating mixed results.22-24 Another key factor influencing cancer screening is cancer worry (CW), the negative emotions, including anxiety and fear, aroused by the risks of getting cancer. 25 Previous research has shown that CW could encourage intention for cancer screening.26,27 For older adults, despite the accumulating evidence, whether and how CF and CW serve as mechanisms linking EHU and cancer screening intention (CSI) is largely unclear among older adults who are still suitable for cancer screening (ie, those between age 65-74, according to guidelines). Though cancer screening intention does not always guarantee actual screening uptake behaviors, it is one of the most significant factors motivating such behaviors.28,29 As such, many interventions deem the promotion of cancer screening intention as their core goals. 30
This study seeks to address the aforementioned gap by analyzing representative data collected in the U.S. We propose and test a model wherein CF and CW serve as mechanisms linking EHU and cancer screening intention among older adults and demonstrate distinct effects. In doing so, this study contributes to the literature by identifying novel potential pathways that explain how EHU promotes cancer screening intention among older adults.
Literature Review and Hypotheses
Theoretical Framework
This study draws on the Health Belief Model (HBM), one of the best-known and most commonly used theoretical frameworks in health research,31,32 as the theoretical framework. HBM proposes concepts that shape the individual health behaviors, including perceived sensitivity and perceived severity. HBM has tested many facets of the association between health behaviors and psychological factors.33-35
Perceived susceptibility is the way in which an individual assesses risk and the likelihood of developing a particular condition, which is represented by cancer fatalism, the belief that cancer cannot be prevented, in this study. Individuals with high cancer fatalism perceive that cancer is inevitable and predetermined, which gives rise to the pessimistic belief that one is susceptible to cancer.36,37 As such, this study employs cancer fatalism to indicate the perceived susceptibility component of HBM. Additionally, perceived severity refers to the level of severity associated with an event or condition, which is reflected by cancer worry, the perceived risk of getting cancer, and the sense of apprehension. In contrast to generalized worry, cancer worry refers to an affective response to the threat of cancer, 38 which is a documented significant predictor of cancer screening.38-40
Regarding antecedents of health beliefs, information provided by E-health can influence the perception of susceptibility and severity. 41 For instance, individuals using E-health information will learn more about cancer, which contains not only cancer science and prevention but also about the dangers and threats of cancer. Access to this type of cancer information may have 2 psychological effects on the patient.
On the 1 hand, it may strengthen the individual’s confidence in cancer prevention and thus alleviate cancer fatalism (perceived susceptibility); on the other hand, it may also lead to varying degrees of cancer worry (perceived severity) as the more access to cancer information, the greater the awareness of its seriousness and vigilance. This study focuses on the impact of these 2 different psychological mechanisms as mediators in cancer screening.
Cancer Fatalism
Cancer fatalism refers to a deterministic attitude towards cancer, where individuals perceive it as inevitable and beyond their control. 26 Such belief can hinder cancer prevention and treatment efforts, leading to decreased motivation and engagement in cancer screening behaviours. 42 Several studies have revealed negative associations between cancer fatalism and cancer screening intentions.43-45 For instance, higher levels of cancer fatalism have been associated with decreased willingness to screen for breast cancer among African-American women, 46 as well as lower willingness to screen for colorectal cancer. 47 Analyzing a nationally representative sample in Britain, Beeken et al 43 have revealed that cancer fatalism may hinder early cancer detection. A recent study also illustrates how higher levels of cancer fatalism may lead individuals to be skeptical about the utility of preventive measures, thus reducing their motivation to participate in screening. 44 The belief that cancer cannot be prevented or controlled makes it more likely that people will neglect the importance of early detection.
Meanwhile, EHU has been found to increase individuals’ exposure to health information, thus altering negative beliefs about cancer so as to reduce cancer fatalism and subsequently influence their intentions to undergo cancer screening. 48 Individuals who use E-health information are more likely to have accurate knowledge about cancer and perceive it as a serious health issue. Such knowledge and awareness help individuals counter fatalistic beliefs, increasing the likelihood of engaging in cancer screening behaviours. 49
Taken together, EHU can increase the knowledge and awareness of individuals, thus reducing cancer fatalism and influencing the willingness to undergo cancer screening. Synthesizing the above literature viewpoints, this study proposes the hypothesis:
Cancer Worry
Characterized by negative cancer-related thoughts and concerns about personal susceptibility to the disease, 50 cancer worry is a powerful motivator for individuals to detect and address health problems, especially those related to cancer prevention and screening. 51
Numerous studies have demonstrated a positive association between cancer worry and cancer screening intentions, because cancer worry usually increases the importance people place on their health and triggers an awareness of the threat of the serious consequences of getting cancer, which increases their intention to take the initiative to undergo screening. For example, research has shown that higher levels of cancer worry are linked to increased self-examination, breast X-ray examination, and prostate cancer screening intentions.52,53
E-health has emerged as a valuable tool to provide individuals with accessible and up-to-date health information. 54 It has been found to increase individuals’ exposure to cancer-related information, which can heighten their cancer worry. 50 E-health use offers insights into risk factors, symptoms, and preventive measures, triggering concerns about personal susceptibility to cancer. 55 Consequently, individuals who use E-health frequently are likely to have higher levels of cancer worry. For instance, Zhu et al 56 reported that seeking information online may increase cancer worry among older adults. In alignment, Chae 57 uncovered evidence that online information about cancer increases cancer worry.
However, there are fewer studies exploring the impact of EHU use as a psychological mediator of cancer worry and its association with cancer screening intentions, and the results are different. Synthesizing the previous arguments, EHU may increase the individual’s access to health information, thus eliciting their concerns about cancer, and then affecting their willingness to undergo cancer screening. Therefore, this study proposes the following hypothesis:
E-Health Use and Cancer Screening
EHU and its impact on cancer screening intention have been the subject of extensive research. Some studies have shown a positive association between EHU and increased participation in cancer screening, like colorectal cancer screening among older adults. 58
Recent studies suggest that EHU may serve as an effective intervention to enhance intentions for cancer screening. Scholars notice that direct use and access to electronic health information provide individuals with accurate and up-to-date information about cancer and its screening benefits, thereby increasing their knowledge, awareness, and understanding of the importance of early detection.
59
Specifically, research has shown a positive association between EHU and breast cancer screening intentions among Korean-American women,
60
as well as colorectal cancer screening intentions among Korean-Americans.
61
Kukhareva et al
62
have also revealed that E-health intervention programs effectively enhanced lung cancer screening. The study conducted by Liu et al
63
also echoed the aforementioned findings in the Chinese population. In addition to this, a review
64
has suggested that EHU may significantly improve cervical cancer screening uptake. These findings indicate that EHU might be a valuable strategy to increase individuals’ intentions to undergo cancer screening. It has also been shown in the literature that regular EHU contributes to increased risk perception and a greater tendency to follow physician and medical recommendations for regular cancer screening.
65
Thus, this increased awareness may lead to a higher intention to undergo cancer screening, which leads to the following hypothesis:
In summary, the conceptual model in Figure 1 is proposed based on the literature review and hypotheses.
Methods
Sample
Data are from the sixth iteration of the National Cancer Institute’s (NCI) National Trends in Health Information Survey (HINTS6) (https://hints.cancer.gov/). The Health Information National Trends Survey (HINTS) is a nationally representative survey that has been conducted by the National Cancer Institute since 2003. Using a two-stage, probability-proportional-to-size design, the HINTS target population is all adults aged 18 or older in the civilian noninstitutionalized population of the United States. The HINTS program collects data on the American public’s need for, access to, and use of health-related information and health-related behaviors, perceptions, and knowledge. 66 This study, aligning with the design HINTS, analyzed cross-sectional data. The number of participants for each stage was reported in Figure S1 (in the supplemental material).
Data collection for HINTS 6 started on March 7, 2022 and concluded on November 8, 2022. The final HINTS 6 sample consists of 6252 respondents. This study included respondents aged 65-74, as guidelines recommended regular screening among older adults for most types of cancer in this age group.8,9 Cases with invalid replies are listed as missing values. The final sample size of this study is 925. As shown in Table 1, this study mainly included age (65-74), birth gender (female = 1, male = 0), education (from below 8 years = 1, 8
Measurement
Dependent variable, Cancer Screening Intention (CSI), is measured by a single item implemented in HINTS survey and used in previous research 67 on a five-point Likert scale (Table S1): How interested are you in having a cancer screening test in the next year (from 1 = Not at all to 5 = up-to-date with screening tests; M = 3.23, SD = 1.07)?
Independent variable, E-health use (EHU), is measured by on 4 items below (Cronbach’s α = .72). The 4 dichotomous items (Table S2) were summed to construct the variable (M = 2.75, SD = 1.32) ranging from 0 to 4, wherein 0 indicates that the respondent did not use electronic devices to access health information in the past year while 4 indicates that the respondent the electronic devices for purposes including look for health or medical information and view medical test results in the past year. 68
Mediator 1, Cancer Fatalism (CF), is measured by 4 items (Cronbach’s α = .67) originally derived from HINTS with a four-point Likert scale (Table S3), which was also used and validated in previous study. 69 The items were summed to construct CF, ranging from 1 to 4). Specifically, 1 indicates that a respondent has a very negative attitude towards cancer (cancer fatalism), and 4 means that the respondents have a very positive and optimistic attitude towards cancer (M = 2.15, SD = 0.65). Sample items included “There’s not much you can do to lower your chances of getting cancer”.
Mediator 2, Cancer Worry (CW), is measured by a single item 61 on a five-point Likert scale (Table S4), where 1 indicated respondents had never worried about cancer, and 5 indicated respondents were extremely worried about cancer (M = 2.70, SD = 1.19). Being used in HINTS survey, this single-item measure has been used and validated in previous works.56,70
The control variables were mainly to control for socio-demographically relevant variables to reduce confounding effects, including age (Mean = 65.05, SD = 2.81), birth gender (female = 1, male = 0), education, household income, and insurance status. Measurement ranges for all control variables were also linearly converted to a 0 - 1 scale.
Data Analysis
Data analysis was conducted in R 4.5.0. 71 Considering that HINTS contains survey weights to enhance representativeness, this study employed the srvyr package of R to replicate the survey weights of HINTS. On this basis, the survey package was used to conduct regression, adjusting for survey weights. Mediation effect as well as confidence intervals were estimated using the multivariate delta method, wherein confidence intervals excluding 0 indicated significant associations. 72 Variables in this study were also transformed according to the normalization of 0 (theoretical minimum value) to 1 (theoretical maximum value), and the unit of variable value is unified into percentages. On this basis, the regression coefficient obtained using 0-1 normalized variables was termed “percentage coefficient”, referred to as “b p ”, which established comparability among variables.73,74
The reporting of this study conforms to STROBE guidelines. 75 All measure items can be found in the supplemental material (Table S1-S4).
Ethical Approval
This study analyzed secondary data. The HINTS 6 general population survey was deemed “exempt research” under 45 CFR 46.104 and approved by the Westat IRB on 10 May, 2021 (Project # 6632.03.51) with amendment approved on 24 November, 2021 (Amendment ID #3597). HINTS 6 was also approved as “Not Human Subjects Research” by NIH Office of IRB Operations on 16, August 2021 (iRIS reference number: 562715).
Results
Preliminary Analysis
As shown in Table 1, there were slightly more females (55.8%) than males among the respondents. The average age of the respondents was about 69 years old (M = 2.82). Among these older adults, 76.0% of the respondents have some college or above. In terms of annual household income, the largest number of respondents (61.5%) had an annual household income below 74,999 dollars. Pearson correlation analysis (Table 2) revealed significant associations between the key variables in this study. 63 Also, Table 2 demonstrated descriptive statistics of focal variables.
Hypothesis Testing
H1 predicted that EHU was positively and indirectly associated with cancer screening intention through the mediation of cancer fatalism. As shown in Figure 2, the results suggested that EHU was negatively associated with cancer fatalism (b = −.02, b p = −.02, SE = .14, P < .001). In addition, cancer fatalism was negatively associated with cancer screening intention (b = −.19, b p = −.14, SE = .02, P < .001). Through the mediation of cancer fatalism, EHU was positively and indirectly associated with cancer screening intention (b = .003, b p = .003, SE = .001, 95% CI [.001, .004]). Thus, H1 was supported.
H2 predicted that EHU was positively associated with cancer screening intentions through the mediation of cancer worry. The results showed that EHU was negatively associated with cancer worry (b = .14, b p = .14, SE = .02, P < .001). Further, cancer worry was positively associated with cancer screening intention (b = .33, b p = .33, SE = .01, P < .001). Additionally, EHU was positively associated with cancer screening intentions through the mediation of cancer worry (b = .05, b p = .05, SE = .002, 95% CI [.04, .05]). Therefore, H2 was supported.
H3 predicted that EHU was positively and directly associated with cancer screening intention. The findings showed that EHU was directly and positively associated with cancer screening intention (b = .25, b p = .25, SE = .01, P < .001). Thus, H3 was supported.
As guidelines suggested that older adults with a smoking history within 15 years and currently smoking should take regular lung cancer screening,7,8 we also estimated the model within respondents aged between 65 and 80 and with a smoking history. The results were largely consistent with the model estimated among respondents aged between 65 and 74 (See Figure S2 in supplemental material).
Discussion
The purpose of this study was to examine the impact of E-health use (EHU) on cancer screening intentions (CSI) among older Americans, with a focus on the parallel mediating roles of cancer worry (CW) and cancer fatalism (CF). Findings reveal the relationship between the EHU, cancer fatalism, cancer worry, and cancer screening intentions among older Americans. The results of the data analysis also support all 6 hypotheses presented in this study. These findings provide valuable insights into the factors that influence cancer screening behaviors among older adults. This discussion section will delve more deeply into the meaning behind these findings, their relevance in the healthcare context, and potential avenues for future research.
Principle Findings
First, this study reveals that EHU is positively associated with cancer screening intentions among older Americans. This finding is consistent with previous research 76 on the importance of access to accurate health information in promoting disease prevention behaviors. The growing popularity of electronic health information provides individuals with a wealth of health-related information and general knowledge, enabling users to make sound judgments and appropriate decisions about their health. The finding that EHU was positively associated with a direct effect on willingness to undergo cancer screening underscores the importance of EHU in promoting willingness to undergo cancer screening among older adults. This suggests that the availability of easy-to-access health information through digital platforms can have a direct impact on an individual’s motivation to participate in cancer screening. It also suggests that older adults who regularly engage in EHU may be more likely to prioritize cancer screening, thereby improving early detection and amelioration of cancer.
Second, this study identifies 2 parallel mediating mechanisms: cancer fatalism and cancer worry. Higher levels of EHU were associated with lower levels of cancer fatalism and higher levels of cancer worry. Cancer fatalism is the belief that cancer is inevitable or incurable, leading to negative attitudes toward cancer prevention behaviors. The negative association between the EHU and cancer fatalism suggests that access to E-health information may challenge fatalism by providing accurate information about cancer prevention, early detection, and treatment options. Providing older adults with easy access to health information through digital platforms may help mitigate their fatalistic beliefs about cancer. This finding demonstrates the potential of EHU to help older adults overcome fatalistic attitudes and take proactive steps toward cancer screening. It also highlights the importance of electronic health information in promoting a positive outlook on screening.
Meanwhile, EHU was positively associated with CW, suggesting that EHU may increase the level of CW among older adults. Cancer worry reflects an emotional response to the threat of cancer and can serve as a psychological stimulus for engaging in preventive behaviors such as cancer screening. Exposure to E-health information may reveal information about cancer risk factors, symptoms, and the dangers of not engaging in timely cancer screening. This potentially increases individuals’ awareness of the importance of detecting cancer early and engaging in preventive behaviors, and encourages them to engage in cancer screening as early as possible. This means that digital health platforms might play a crucial role in raising awareness and concern about cancer, thus inspiring greater motivation for cancer screening.
In addition, CF is negatively correlated with CSI, indicating that higher levels of CF are associated with decreased interest in cancer screening. This implies that individuals with higher levels of fatalistic beliefs about cancer may be less likely to engage in cancer screening activities. Therefore, cancer fatalistic beliefs need to be addressed to promote proactive screening behavior among older adults. In addition, a positive correlation was found between CW and CSI, suggesting that people with higher levels of worry about cancer might be more likely to express interest and willingness to undergo cancer screening. This highlights the importance of addressing and managing cancer concerns to promote timely and regular screening practices. Analysis of the mediating role of cancer concern and worry with cancer fatalism suggests that interventions targeting these psychological factors are needed to enhance willingness to undergo cancer screening. For example, healthcare providers may develop tailored communication strategies that effectively communicate the risks and benefits of cancer screening while addressing common fears and misconceptions associated with cancer. By addressing concerns and fostering a sense of personal agency, healthcare providers may help alleviate barriers to cancer screening for older adults.
Finally, identifying the 2 psychological variables CW and CF above reveals that the overall positive impact of EHU on CSI emphasizes the combined effect of EHU on promoting older adults’ willingness to be screened for cancer. By addressing cancer concerns and fatalistic beliefs, and promoting access to health information, healthcare providers and policymakers may increase screening rates and improve cancer detection rates among older adults.
Practical Implications and Academic Contributions
The results of this study have important practical implications for healthcare providers, policymakers, researchers, and public health practitioners. First, EHU was positively associated with willingness to be screened for cancer. This emphasizes the role of electronic health information in promoting willingness to be screened for cancer and the importance of promoting access to accurate health information for older adults. Health interventions targeting older populations should incorporate digital strategies to enhance access to information and encourage cancer screening behaviors. Health information providers may utilize online and new media platforms to provide detailed information about cancer prevention, early detection, and treatment, thereby empowering older populations to make informed decisions about their health. Second, the parallel mediation effect revealed in this study suggests that EHU is linked with CSI by increasing CW while decreasing CF. Healthcare providers may provide older adults with easy access to electronic health information to mitigate fatalistic perceptions by providing accurate information about cancer prevention and treatment options. Nonetheless, it should be noted that high levels of CW are potentially harmful for individual well-being by, for example, intensifying emotional distress and threatening daily functioning.48,77 As such, we recommend healthcare providers and other related practitioners closely monitor the mental and physical health status of patients who participate in E-health interventions. Health organizations and policymakers may focus on developing user-friendly digital platforms to disseminate accurate and reliable health information. In addition, healthcare professionals are suggested to emphasize the importance of cancer screening and provide detailed information on screening procedures to increase individual awareness and concern about cancer. Third, policymakers can utilize the findings of this study to develop targeted interventions to increase cancer screening rates among the older adult population. For example, policymakers could allocate resources to develop user-friendly E-health information platforms for older adults or provide incentives for healthcare providers to utilize E-health information platforms for patient education. Strategies that focus on increasing perceptions of cancer risk, boosting health beliefs, dispelling misconceptions about cancer, and communicating the benefits of early detection through e-platforms could increase awareness of and participation in cancer screening programs among older adults. Additionally, though E-health information is widely accessible, individuals with relatively lower literacy in scanning information and assessing information quality may be excluded from obtaining benefits from E-health.78,79 Therefore, programs aiming at promoting literacy of individuals, especially those with lower health and E-health literacy, are needed.
From an academic perspective, this study contributes to the existing literature by providing empirical evidence on the relationship between EHU, CW, CF, and CSI among older adults. By analyzing the mediating role of psychological factors in the pathway from information acquisition to behavioral intentions and expanding understanding of the underlying mechanisms of health decision-making processes in older adults, these findings fill a knowledge gap in understanding the mechanisms by which digital health platforms influence cancer screening behaviors. At the same time, the study provides insight into the specific pathways through which these variables interact and influence each other. This knowledge can guide future research to develop more targeted interventions and explore other factors that may mediate or moderate these relationships.
Limitations and Directions for Future Research
Although this study provided valuable insights, some limitations should be recognized. Firstly, this study relied on publicly available cross-sectional data from HINTS6 self-reports, which may be subject to social desirability bias and recall bias. Participants may have overestimated their level of engagement with EHU or willingness to undergo cancer screening, resulting in an overestimated effect size. Future studies could incorporate objective measures such as actual screening rates or medical records to provide a more accurate assessment of an individual’s screening behavior, and could also start with website analysis or electronic health records to provide more accurate data.
Secondly, the cross-sectional design of this study hinders causal inferences in this study. Although the parallel mediator model proposed in this study is theoretically sound, longitudinal studies are needed to examine the long-term effects of E-health use on cancer screening behavior. As such, any causal interpretation of the findings should be made rather cautiously. To advance this study, future studies could employ longitudinal designs using panel data or random controlled trials to explore the causal relationships between E-health use, cancer fatalism, cancer apprehension, and cancer screening intentions.
Furthermore, CW and CSI in this study, due to the constraint of secondary data analysis, are assessed with single items. Though both measures were used and validated in previous works,56,67,70 this may still constrain the comprehensiveness of measurement and thus the robustness of analysis. Therefore, future research is suggested to use multi-item and multi-dimensional measures to better assess the variables. In addition to this, the measurement of CSI does not distinguish between different types of cancers that differ in recommendations, guidelines, risks, etc.8,9 Therefore, investigation in screening intentions within contexts of different types of cancers is needed to better examine the nuanced nature of cancer screening.
Also, it should be noted that CSI differs from cancer screening behaviors. Though being one of the strongest predictors of cancer screening behavior, CSI, like many other types of intentions, does not always guarantee actual behaviors.80,81 Therefore, we suggest that future work advance this study by measuring or tracking actual cancer screening behaviors to better assess whether EHU can promote cancer screening.
In addition to CF and CW investigated in this study, other psychological and societal factors may influence health behaviors including cancer screening. These factors may also affect EHU, CF, or CW, making them potential confounding factors for this study. These factors of concern may include, for instance, health literacy, social support, cancer awareness, and heath literacy.13,82 The list can go on. Future studies may address this limitation by exploring more factors and mechanisms that potentially promote cancer screening among older adults.
We also stress that this study did not adequately address the differential barriers to acquiring, filtering, assessing, and utilizing online health information faced by older adults, or the issue of digital divide that challenges the older adults. 83 As such, future studies are encouraged to explore how digital divide may hinder the effectiveness of E-health and its effect on cancer screening. Also, the heterogeneity within older adults, such as gender and income, may cause inequality in access to and use of E-health, 83 which should also be examined in future works.
Also, it should be noticed that this study was conducted in the sample from the United States. Therefore, the generalization of findings to other regions should be cautious. Future works are also encouraged to employ multi-national samples to advance external validity of this study.
Finally, qualitative research combined with a mixed methods approach could be used to gain a deeper understanding of the psychological processes behind the relationships examined in this study and to understand the experiences and perceptions of EHU among older adults and how it affects cancer screening intentions. Understanding the barriers and facilitators specific to this particular population could inform the development of targeted interventions.
In summary, the results and findings of this study illustrate the importance of providing older adults with easy access to accurate health information, addressing cancer concerns, and facilitating cancer screening behaviors, demonstrating significant associations between E-health use, cancer concerns, cancer fatalism, and cancer screening intentions among older adults in the United States. Also, this study explains the mediating role of cancer worry and fatalism to understand the psychological mechanisms by which EHU influences screening intentions. This suggests targeted interventions for providers to address psychological barriers and promote access to reliable E-health information. By understanding the complex interplay between cognitive and affective factors in the health decision-making process, healthcare providers can develop tailored strategies to improve cancer prevention and early detection among older adults. In addition, the results of this study help to fill knowledge gaps, refine practical interventions and academic theories, and suggest future research directions in the area of cancer screening behaviors and digital health interventions, paving the way for future research to explore innovative strategies for promoting preventive health behaviors in older adults.
Conclusion
This study examined the impact of EHU on CSI among older Americans. The findings emphasize the positive impact of EHU on cancer screening intentions among older adults. The positive association between EHU and willingness to undergo cancer screening highlights the importance of access to accurate health information in promoting cancer screening prevention behaviors. In addition, a parallel mediating effect between cancer fatalism and cancer worry was found, suggesting that EHU may reduce fatalistic beliefs while increasing individuals’ risk awareness and worry about cancer, thus potentially making older adults aware of the importance and urgency of getting cancer screening. These findings have implications for healthcare providers and policymakers in developing interventions to increase cancer screening rates in the older population.
Supplemental Material
Supplemental Material - Effect of E-Health Use on Cancer Screening Mediated Through Cancer Worry and Fatalism: A Cross-Sectional Study of Older Adults
Supplemental Material for Effect of E-Health Use on Cancer Screening Mediated Through Cancer Worry and Fatalism: A Cross-Sectional Study of Older Adults by Yu Zheng, Jiazheng Zayn Wang, Yingxia Zhu, and Xinshu Zhao in Cancer Control
Footnotes
Ethical Considerations
This study analyzed secondary data. The HINTS 6 general population survey was deemed “exempt research” under 45 CFR 46.104 and approved by the Westat IRB on 10 May, 2021 (Project # 6632.03.51) with amendment approved on 24 November, 2021 (Amendment ID #3597). HINTS 6 was also approved as “Not Human Subjects Research” by NIH Office of IRB Operations on 16, August 2021 (iRIS reference number: 562715).
Consent to Participate
All participants offered informed consent.
Author Contributions
Yu Zheng conceived the model idea and provided substantial guidance throughout the manuscript writing process. Jiazheng Zayn Wang conducted data processing and analysis and was a major contributor in writing the manuscript. Yingxia Zhu replicated the results of data processing and reviewed the manuscript. Xinshu Zhao served as the project leader, overseeing and ensuring the integrity of the research. All authors have thoroughly read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by grants of University of Macau, including CRG2021-00002-ICI, ICI-RTO-0010-2021, CPG2021-00028-FSS and SRG2018-00143-FSS, Xinshu Zhao PI; Macau Higher Education Fund, HSS-UMAC-2020-02, Xinshu Zhao PI.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
Appendix 1
Appendix 2
Zero-Order Pearson Correlations (N = 925)
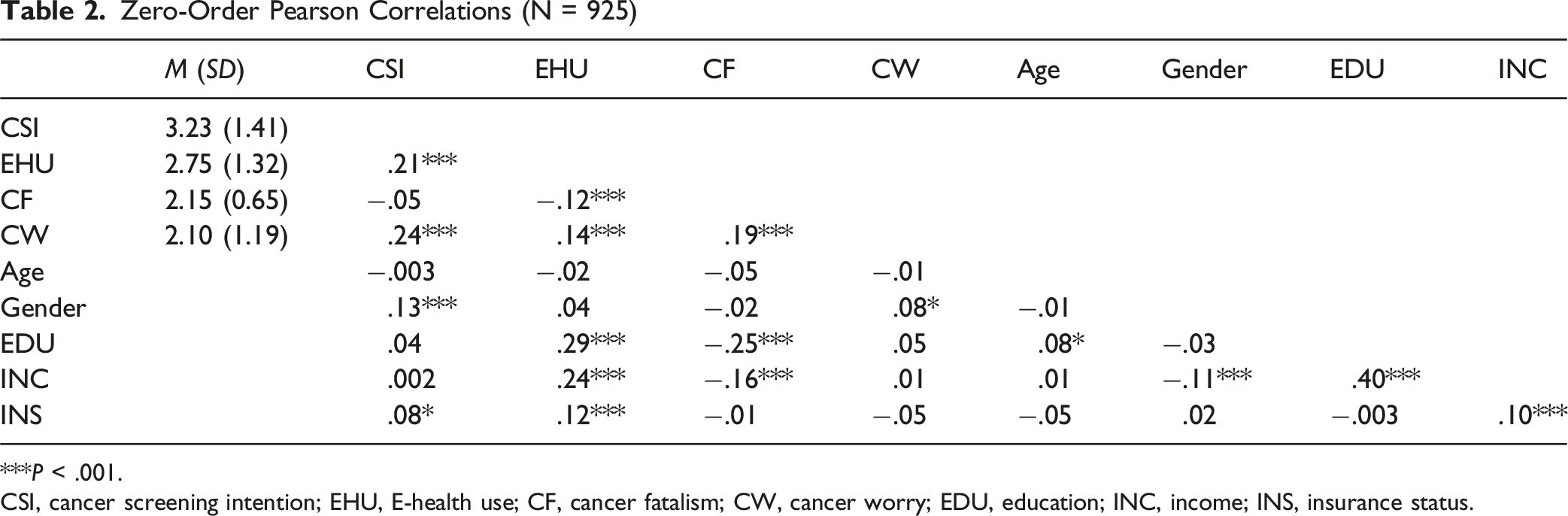
| M (SD) | CSI | EHU | CF | CW | Age | Gender | EDU | INC | |
|---|---|---|---|---|---|---|---|---|---|
| CSI | 3.23 (1.41) | ||||||||
| EHU | 2.75 (1.32) | .21*** | |||||||
| CF | 2.15 (0.65) | −.05 | −.12*** | ||||||
| CW | 2.10 (1.19) | .24*** | .14*** | .19*** | |||||
| Age | −.003 | −.02 | −.05 | −.01 | |||||
| Gender | .13*** | .04 | −.02 | .08* | −.01 | ||||
| EDU | .04 | .29*** | −.25*** | .05 | .08* | −.03 | |||
| INC | .002 | .24*** | −.16*** | .01 | .01 | −.11*** | .40*** | ||
| INS | .08* | .12*** | −.01 | −.05 | −.05 | .02 | −.003 | .10*** |
***P < .001.
CSI, cancer screening intention; EHU, E-health use; CF, cancer fatalism; CW, cancer worry; EDU, education; INC, income; INS, insurance status.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.