
Abstract
Introduction
American Indians and Alaska Natives (AIANs) experience significant cancer incidence and mortality disparities, with elevated cancer risk factor exposure, lower cancer screening rates, and poorer quality of cancer care relative to non-Hispanic Whites. To address these issues, the Southeastern American Indian Cancer health Equity Partnership (SAICEP) was formed to understand and address cancer disparities among southeastern American Indians (AIs).
Methods
SAICEP formed in 2021 through the Community Outreach and Engagement offices of the NCI-designated Comprehensive Cancer Centers in North Carolina (NC). The catchment areas for these cancer centers include the tribal homelands for eight state and federally recognized Tribes, representing the largest AI populations in the eastern US. SAICEP seeks to: (1) increase awareness of cancer health needs of AI populations; (2) expand access to cancer health education and build community capacity to address cancer health needs; (3) develop collaborative research relationships to better understand and address the AI cancer burden.
Results
For Aim 1, SAICEP created a virtual speakers’ series, featuring prominent AI cancer researchers and clinicians, hosted by the UNC Lineberger Cancer Network three times a year. To date, 10 webinars have been convened, with a total of 538 participants. For Aim 2, SAICEP participates in tribal events throughout the year, reaching over 3500 AIs and disseminating printed cancer educational materials and giveaways. For Aim 3, SAICEP secured funding to conduct analyses to assess cancer incidence, mortality, and care quality for NC AIs, to collect information to understand community cancer needs and culturally adapt and disseminate information on cancer screening and risk reduction.
Conclusion
Through its targeted research and engagement, SAICEP has successfully moved towards achieving its goal of understanding and addressing cancer disparities among AIs in NC. Future directions will involve the development of a community advisory board and collaborations with Tribes in other states.
Plain Language Summary
American Indians and Alaska Natives (AIANs) face significant challenges with cancer, including greater exposure to risk factors, lower screening rates, limited access to quality care compared to non-Hispanic Whites, and higher rates of cancer-related deaths. To address these issues, the Southeastern American Indian Cancer health Equity Partnership (SAICEP) was created. SAICEP’s mission is to understand and address the burden of cancer among American Indian (AI) people in our combined service area. SAICEP was formed in 2021 as a partnership between the three NCI designated cancer centers in North Carolina, which serve multiple tribal nations and Urban Indian organizations. SAICEP engages with Native people through initiatives like a virtual speakers’ series featuring AI cancer experts. So far, SAICEP has hosted 10 webinars, reaching 538 attendees. Additionally, SAICEP participates in tribal events, sharing educational materials and information to help communities understand and reduce cancer risks. Our team has also secured funding to study cancer trends, care quality, and community needs for AIs in North Carolina, which helps identify ways to improve care and support cancer prevention. SAICEP’s efforts have made meaningful progress toward understanding and addressing cancer disparities among AIs. Looking ahead, the group plans to create a community advisory board and expand its work to include partnerships with Tribes in other states. By combining research, education, and community outreach, SAICEP aims to ensure AI communities have the tools and resources they need to fight cancer.
Introduction
American Indians and Alaska Natives (AIANs) have significant disparities in incidence and mortality for certain cancers. 1 For example, compared to non-Hispanic White men, AIAN men have higher rates of prostate cancer mortality, largely manifested through higher rates of advanced cancer at diagnosis and lower rates of definitive treatment. Infectious disease-related cancers, such as liver, stomach and cervical, are also significantly higher in this population.1-4
Rates of exposure to cancer risk factors and cancer screening vary dramatically by Tribe and geographic region. 1 In general, use of commercial tobacco, obesity and physical inactivity, type 2 diabetes and alcohol consumption are higher in AIAN populations, as well as infection with human papillomavirus (HPV), Heliobacter pylori and the hepatitis b and c virus also appear to be higher in this population. 1
One challenge in understanding the burden of cancer in AIANs is the misclassification of race in medical records which adversely affect our interpretation of cancer incidence, mortality and quality of care in this population.5-7 An analysis published in 2009 showed a 18% misclassification rate for cancer incidence among American Indians in North Carolina. 8 While strategies have been implemented to address this issue, the effect of this approach for American Indians who are not a member of a federally-recognized Tribe remains unknown. 8
The purpose of this paper is to provide an overview of the development and implementation of a partnership across three nationally recognized cancer centers designed to provide insights into the cancer burden of American Indians in North Carolina (NC). The American Indian population in North Carolina is one of the largest in the US, and many of those who identify as American Indian are affiliated with non-federally recognized Tribes. 8 In this paper, we document our successes and lessons learned in our research, community engagement and outreach and future directions to enhance our efforts.
Methods
North Carolina American Indian Population
North Carolina is currently home to the largest American Indian population in the eastern US, with a population of over 300 000 people identifying as American Indian/Alaskan Native (approximately 3% of the state’s population).
9
This includes eight Tribes recognized by the state and/or federal government.
9
These Tribes are sovereign nations of people each with its own government structure unique to the Tribe.
9
The State is also home to four urban Indian organizations that operate in the four largest metropolitan areas.
9
These organizations are 501(c)(3) non-profit agencies but are also recognized by the state as governing bodies that serve Native people, regardless of tribal affiliation, in a specified geographic location.
9
The State Recognition process is enforced through the NC Commission of Indian Affairs (NCCIA).
10
The NCCIA is an inter-tribal political entity that operates within the NC Department of Administration.
10
The NCCIA Board of Directors is made up of representatives from each Tribe and urban Indian organization, as well as an Executive Director who manages multiple staff and project coordinators.
10
Collaboration with the NCCIA is just as essential to SAICEP’s work as collaborations with individual tribal communities. (Figure 1). American Indian Tribes and Urban Indian Centers in NC.
Description of SAICEP Partnership
In the spring of 2021, the Associate Directors of the Community Outreach and Engagement (COE) offices at the three National Cancer Institute (NCI)-designated comprehensive cancer centers in North Carolina at Atrium Health Wake Forest Baptist Comprehensive Cancer Center, the Duke Cancer Institute, and the UNC Lineberger Comprehensive Cancer Center, met to discuss coordinating engagement activities with American Indian Tribes in our respective catchment areas.
Atrium Health Wake Forest Baptist Comprehensive Cancer Center (AHWFBCCC) serves communities across the state of North Carolina as well as certain counties in Virginia and South Carolina with the mission of reducing cancer incidence, mortality, and morbidity. Community outreach and engagement activities at AHWBCCC occur through the Office of Cancer Health Equity, which is led by Dr Nadine Barrett. Dr Rachel Denlinger-Apte, Assistant Professor of Public Health Sciences with expertise in tobacco policy, contributes to the SAICEP leadership from AHWFBCCC with Dr Barrett.
16
The Duke Cancer Institute (DCI) focuses on reducing the cancer burden and promoting health equity, and serves 67 North Carolina counties, 31 Virginia counties, and 6 South Carolina counties. Established in 1973, the DCI was one of the original 8 NCIs in the United States. Today, the DCI has six locations and sees over 66 000 patients. Community outreach and engagement activities at DCI occur through their Community Outreach, Engagement and Equity office, led by Dr Tomi Akinyemiju, who also serves in the SAICEP co-leadership capacity.13-15 Established in 1975, UNC Lineberger (UNC Lineberger) is the only public and comprehensive cancer center in North Carolina, serving patients from all 100 countries in the state. The SAICEP leadership at UNC Lineberger includes Dr Stephanie Wheeler, Associate Director of COE and Dr Ronny Bell, an enrolled member of the Lumbee Tribe and Associate Director of Cancer Care Access and Excellence.11,12 (Figure 2). Map of Three Cancer Center Catchment Areas.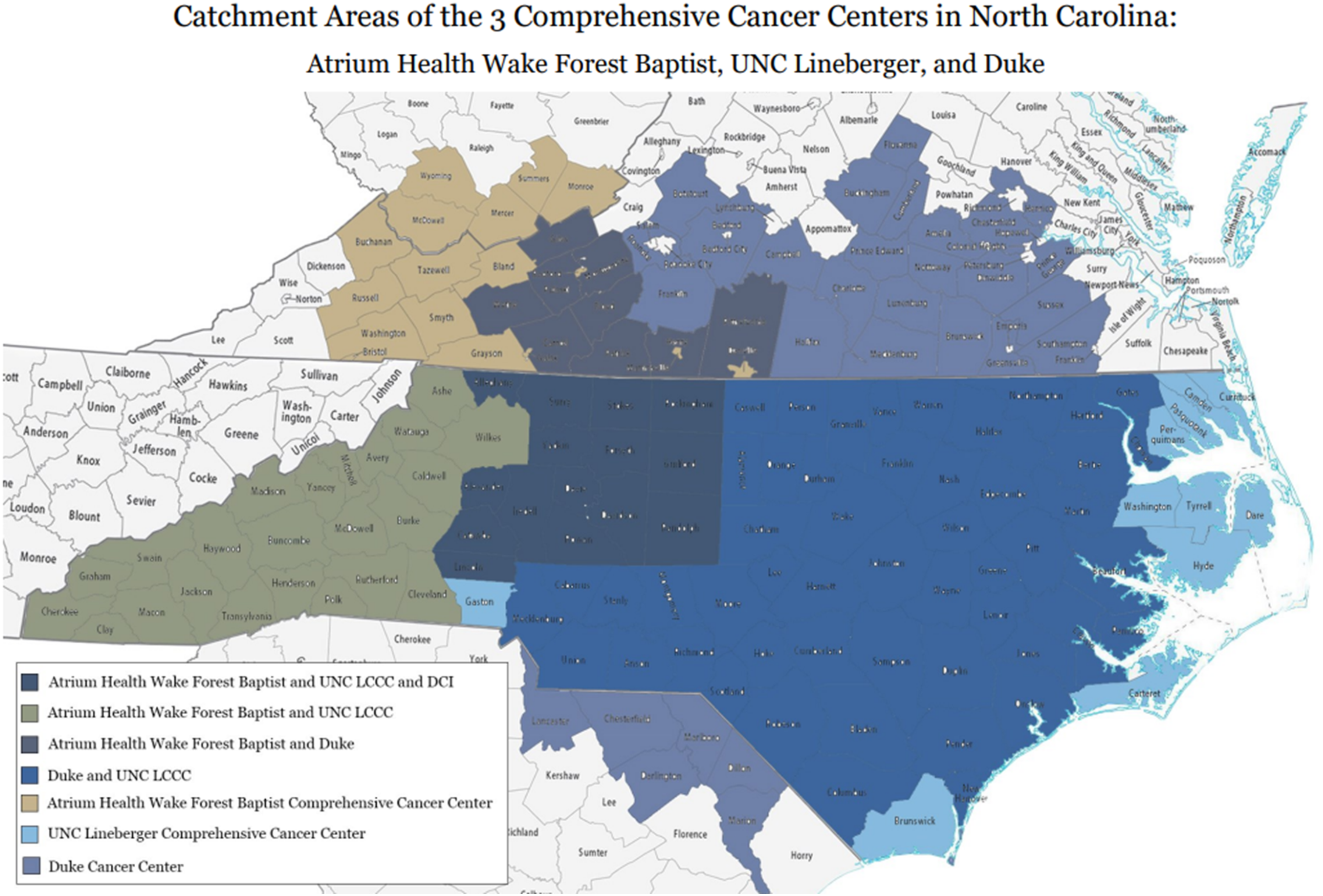
In July 2021, SAICEP officially launched, with the stated mission to understand and address the cancer-health related needs of American Indians in the catchment area of the three cancer centers that make up the partnership. The SAICEP team, across the three institutions, accomplishes this in three core areas: community outreach, cancer health education, and equitable research. SAICEP prioritizes sustainable relationships with the Tribes and Native serving organizations in our combined catchment areas. This includes ensuring our presence at tribally led powwows, health fairs, and community gathering, in which we aim to provide support and learn by attending programming that educates on community and cultural practices. Our outreach efforts are centered on a respect for tribal sovereignty, cultural understanding, and the co-creation of solutions tailored to the unique needs of each community.
Results
SAICEP Research
In 2022, SAICEP received the first of three collaboration grants from the V Foundation. These grants, supported through the foundation’s annual Victory Ride event, are available to support research initiatives that include representation across all three cancer centers in North Carolina. The aims of our first grant were: Aim 1: Led by the UNC team, assess regional variation in cancer incidence, prevalence, stage of diagnosis, mortality and quality of care for NC AI populations identified with cancer diagnoses from 2003-2019 through the NC Central Cancer Registry (NCCCR) via data accessed through the Cancer Information and Population Health Resource (CIPHR); Aim 2: Led by the DCI team, building on prior engagement activities with NC AI communities, including the 2020 Native Pathways to Health Project and the NCI-funded Healing Walk Project, assess cancer health information needs and barriers and facilitators associated with cancer care through qualitative methods (e.g., talking circles) and survey methodologies supported by tribal leaders; Aim 3: Led by the AHWFBCCC team, map assets, community strengths, and resources available in NC AI communities that can support cancer health equity across the continuum, in partnership with Tribes and AI youth leaders. 17
Through our CIPHR analyses (Aim 1), SAICEP was able to identify the most common incident cancers in the NC AIAN population (breast, prostate, lung and bronchus and colorectal) and showed that liver cancer had the highest disparities of incidence compared to non-Hispanic Whites. The cancers showing the highest mortality rate disparities in this population were prostate, stomach and liver. SAICEP also showed that NC AIANs were more likely that non-Hispanic Whites to receive poorer cancer care at end of life, demonstrated through higher rates of hospital and ICU admissions as well as emergency room visits.18,19
Our Aim 2 goals in this first V Foundation grant involved conducting talking circles within three tribal communities in the state (Lumbee, Coharie, Haliwa Saponi). Talking circles are traditionally Indigenous ways that Native communities have come together to share stories and education. Talking circles may also serve as a culturally tailored qualitative data collection method.20,21 We adapted the qualitative survey questions to a talking circle platform with the assistance of Native individuals who had extensive experience leading talking circles. We had two respected Native community health workers assist us with leading the talking circles, which allows us to be culturally humble while still gaining insights on the feelings and challenges regarding health. Themes that emerged from the talking circles included: the challenges associated with accessing trusted, culturally respectful medical care and the geographic distance from tribal communities to cancer care services, the contemporary and historical exposure to chemicals in the community food and water systems and other factors associated with the social determinants of health (poverty, education, etc.). Community assets and prevention factors included the resilience of their tribal communities, culture and faith/spirituality and increased awareness of health issues.
For Aim 3, SAICEP partnered with the North Carolina Native American Youth Organization (NCNAYO) to conduct a photovoice project within their respective tribal communities. After receiving photovoice training, the youth took photos and wrote about their experiences related to three prompts: (1) What does cancer look like in your community; (2) What things in your community make it easier to avoid cancer? (3) What are the obstacles within your tribal community that make it hard to avoid cancer? Four central themes emerged from the photovoice activities: (1) The importance of having American Indian health care providers in the community; (2) The pervasiveness of commercial tobacco in their communities; (3) The connection with Native culture as it relates to promoting health; and, (4) The impact of faith and the faith community in sustaining health and wellness. 22
Our second V Foundation grant focused on lung cancer, which was chosen after reviewing the cancer disparity data collected from our first year of funding, based The aims for this grant were: (1) Led by the UNC team, explore trends in tobacco cessation treatment, low-dose CT (LDCT) screening, and cancer care outcomes among AIs and non-Hispanic White populations in NC between 2003 and 2020. (2) Led by the AHWFBCCC team, expand assessment of commercial tobacco and alternative tobacco products used by AIAN populations in collaboration with the NCCIA; Led by the DCI team, adapt the Duke Smoking Cessation Program to enhance cultural relevance for NC AIAN communities, and revise educational materials, decision aids, and community referral resources to improve utilization of LDCT screening among eligible AI residents.
[Our aim 1 analysis has shown measurable disparities in the quality of care at the end of like for AIAN lung cancer patients compared to non-Hispanic Whites. Examining care in the month prior to death, NC AIANs had higher hospital admissions rates (RR, 1.14 [1.07-1.22]), ICU admissions (RR, 1.24 [1.08-1.42]), more than one ED visits (RR, 1.27 [1.09-1.47]), and death in the hospital (RR, 1.22 [1.06-1.40]). 23
For Aim 2, a collaboration called the North Carolina American Indian Adult Tobacco Survey (NCAIATS) was formed between SAICEP, the NCCIA and the Tobacco Prevention and Control Branch of the NC Division of Health and Human Services. Using COVID-19 state funding provided to the NC DHHS, the NCAIATS worked with the NCCIA to hire a project coordinator and data collectors in the tribal communities to attend community events to encourage completion of the online survey in all eight Tribes and urban Indian organizations. 23 The survey instrument used was the CDC American Indian Adult Tobacco Survey, modified to suit the needs of our project and our tribal communities. 24 Preliminary results indicate that about 2500 surveys were completed, with approximately 28% reporting current cigarette use, more than double the rate for North Carolina. A significant challenge in completing and analyzing survey data was the influx of “bot” surveys, which took significant time and resources to clean the data set.
For Aim 3, work is ongoing to achieve our stated aims. A lung cancer education print and video resource has been developed, which includes information on lung cancer symptoms, lung cancer prevalence in AI communities, and the differentiation between commercial tobacco and traditional tobacco. The print resource is currently available on the SAICEP website and social media page and is disseminated at our community cultural events. 25
The focus for our ongoing Year 3 V Foundation grant is gastric cancer, which showed in our Year 1 analysis to be one of the cancer sites with the highest level of mortality disparity compared to non-Hispanic Whites. The UNC Lineberger team will analyze its CIPHR data to document indicators of quality of care for NC AIAN gastric cancer patients. The DCI team brought in a collaborator, Dr.Meira Epplein, who is an expert on the epidemiology of gastric cancer. Efforts are currently underway to conduct h. pylori screenings in three of the NC tribal communities and to distribute educational materials focused on increasing awareness of gastric cancer risk factors and symptoms. 26
SAICEP Speakers Series
Since September 2021, SAICEP has hosted 10 webinars in its Speakers Series through the UNC Lineberger Cancer Network series for providers, researchers, and community members. The SAICEP Speaker Series rotates its hosting responsibilities among UNC Lineberger, DCI, and AHWFBCCC. These webinars host speakers who focus on bringing awareness to AIAN cancer health topics. Common themes discussed include cancer prevention, diagnosis, treatments, disparities, and the intersection of Indigenous healing methods with western medicine. The Speaker Series webinar has featured speakers from 10 unique Tribes and has hosted one webinar focused on the health of an individual Tribe – the Catawba Nation.
SAICEP Webinar Speakers Series.

Community Engagement Events
SAICEP Community Outreach Events and Reach.

SAICEP Presentations at State and National Conferences.

Various members of the SAICEP team across the three cancer centers have ensured that the work we do is shared with both the communities we work with as well as our peers who also work in cancer health. So far, we have presented 10 community workshops at various tribal led conferences and meetings in North Carolina. Our team has also presented our work at 19 state and national conferences in the form of workshops, poster presentations, and roundtable discussions. Community workshops have taken place at statewide gatherings of tribal members including the annual NC American Indian Unity Conference, and the UNC Pembroke Southeastern American Indian Studies Conference, among others. Presenting our work at state and national conferences provides the ability to collaborate with other cancers who also engage with Native communities in their areas, as well as allows us to share our work in its early stages so other might learn from what we have accomplished.
Discussion
The mission of the SAICEP is to understand and address the cancer health needs of American Indians in our catchment area and beyond. We achieve this through community engagement, culturally tailored education and equitable research with tribal communities. Our team has worked to attend a number of tribally led community events like powwows and tribal health fairs where we engage with communities and individuals to introduce our initiative and team members and share the collective resources that are culturally adapted to the communities we serve from our cancer centers. We have presented our work to our community members as well as our peers in the cancer health network. Sustaining meaningful partnerships with Native governments, communities, and individuals is vital to the work we do.
The SAICEP initiative has a long road ahead as we continue to prioritize building relationships with all tribal nations and organizations in our region. In June of 2024 the SAICEP held its first annual strategic planning retreat in partnership with a local tribal, the Occaneechi Band of the Saponi Nation. At the retreat, we developed a 3-year strategic plan and identified five action items to accomplish in this time frame. Action items included: (1) Strengthen and expand AI- related partnerships to increase engagement in NC and beyond; (2) Foster cross-cultural training, education, and workforce development; (3) Develop and implement a sustainability plan for SAICEP’s long-term impact; (4) Expand the scope of AI research and promote equitable access to it; and, (5) Increase access to quality care across the life course and the cancer control continuum. These themes were generated through our lessons learned through our talking circles in three of the tribal communities and with tribal leaders, in our SAICEP seminar series, and in our interactions with tribal members at community events and from attendees at our presentations at conferences. We are also committed to expanding our geographic footprint to include the Catawba Nation of South Carolina.
Moving forward, SAICEP would like to prioritize the voice of the Native community throughout all aspects of our work. To accomplish this, a new project has recently emerged in the SAICEP initiative with the formation and launch of a community advisory board (CAB) to help guide our efforts. The eight-member CAB represents several NC Tribes from both urban and rural Native communities. The CAB was developed with four main goals, (1) establish community partnerships, (2) engage with Native communities, (3) provide cancer health education and (4) work with our team to allocate cancer health resources. The CAB had its first convening on February 4, 2025, which was very successful. The discussion with the CAB allowed us to share what we have learned through our engagement activities and hear from them about potential new priorities for our work.
While there would have been some merit in forming and convening a CAB at the onset of our partnership, several factors prohibited that from occurring, including the lack of staff and financial resources to support the CAB, the need to engage with tribal leaders across the country to introduce ourselves and learn from them about their priorities around cancer and tribal health, and to ensure we had adequate representation across the tribal communities in our state, many of whom were recruited to participate in the CAB through our community engagement activities.
The SAICEP team set out in 2021 on a bold and ambitious initiative to formulate plans to understand and address the cancer burden among AIs in North Carolina, a state with a relatively large and diverse AI population. Our plan intended to capitalize on the strengths of our collective NCI-designated comprehensive cancer centers and our commitment to serve this population in a culturally-respectful manner. We are continuing to learn, but have made significant steps in achieving our mission, and, with the assistance of our CAB, will continue to move forward with achieving cancer health equity for AIs in our state, and, hopefully, across the southeastern US.
Footnotes
Acknowledgements
The authors wish to thank the leadership of the Tribes and urban Indian organizations in North Carolina, as well as the North Carolina Commission of Indian Affairs and the North Carolina Native American Youth Organization, for their support of our work. We also express our appreciation to Mr Tony Locklear (Lumbee) and Ms Vivette Logan-Jeffries (Occaneechi Band of the Saponi Nation) for their collaboration with the SAICEP team and for leading our talking circles. The authors wish to acknowledge the efforts of Carla Strom, MLA, Administrative Director of Community Outreach and Engagement at the Vanderbilt-Ingram Comprehensive Cancer Center, for her efforts to support the development and work of SAICEP during her time as Assistant Director of Community Outreach and Engagement at the Atrium Health Wake Forest Baptist Comprehensive Cancer Center. We also wish to thank the members of the tribal communities across the state for participating in our projects and attending our educational sessions. Finally, we wish to thank The V Foundation for Cancer Research for their ongoing financial support of our work.
Ethical Approval
The work described in this manuscript was approved by the Institutional Review Boards (IRBs) of Duke Health, the University of North Carolina at Chapel Hill, and the Wake Forest University School of Medicine as it was led by each institution. As relevant, tribal approval was approved for the specific Tribes that participated in our research activities. Duke Health Institutional Review Board: Protocol ID# Pro00111767 (All project activities). University of North Carolina at Chapel Hill: IRB Approval# 22-0674 (Year 1); IRB Approval# 23-0225 (Year 2); IRB Approval# 23-3282 (Year 3). Wake Forest University School of Medicine: IRB Approval# IRB00088237 (Community Asset Mapping and Photovoice Project); IRB00094932 (American Indian Tobacco Survey).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: SAICEP is supported by funding from three Victory over Cancer grants from the V Foundation for Cancer Research as well as Cancer Center Support Grants (CCSG) from the Atrium Health Wake Forest Baptist Comprehensive Cancer Center, the Duke Cancer Institute, and the University of North Carolina Lineberger Comprehensive Cancer Center.
Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.