
Abstract
Background
Colorectal cancer (CRC) is the 3rd most frequently diagnosed cancer and the 2nd leading cause of cancer death in the United States (US), and incidence and mortality rates in Oklahoma are higher for many American Indian (AI) populations than other populations. The AI CRC Screening Consortium addresses major regional CRC screening disparities among AIs with shared objectives to increase CRC screening delivery and uptake in AIs aged 50 to 75 years at average risk for CRC and to assess the effectiveness of implementations of the interventions. This manuscript reports environmental scan findings related to current practices and multi-stakeholder experiences with CRC screening in two Oklahoma Indian health care systems.
Method
We conducted a mixed methods environmental scan across five clinical sites and with multiple stakeholders to determine the scope and scale of colorectal cancer screening in two separate AI health care delivery systems in Oklahoma. Data collection consisted of a mixture of individual interviews and group discussions at an urban site, and four clinical care sites within a tribal health system.
Results
Sixty-two individuals completed interviews. Data from these interviews will inform the development of evidence-based intervention strategies to increase provider delivery, community access to, and community priority for CRC screening in diverse AI health care delivery systems. Conversations with patients, providers, and clinical leadership point to individual and system-level opportunities for improvement at each site, shaped in part by differences in the delivery of services, structure of the health care system, and capacity to implement new intervention strategies. The thematic areas most central to the process of evidenced-based intervention development included: current practices, needs and recommendations, and CRC site priorities.
Conclusion
Environmental scan data indicated clear opportunities for individual and system-level interventions to enhance CRC screening and was critical for understanding readiness for EBI implementation at each site.
Background
Colorectal cancer (CRC) is the third most frequently diagnosed cancer and continues to be the second leading cause of cancer death in the general US population.1,2 Overall incidence of CRC has been declining, particularly among older age groups. 3 However, unlike older non-Hispanic White (NHW) populations, American Indian (AI) populations in the US have not experienced decreases in CRC incidence.3-6 Cancer incidence and mortality are also higher overall among AI than NHW persons3,6 living in the 637 counties that contain federally recognized tribal reservations or trust lands or are adjacent to them. 7 AI persons with CRC also have disproportionate late-stage disease at diagnosis compared with NHWs.3,4,6 This leads to worse overall8,9 and CRC-specific 10 survival rates for AI persons than NHW persons. Furthermore, CRC mortality from 1990-2017declined in most racial and ethnic groups in the US (average annual percent change 1.6 %-2.8%) but the decline was much lower in AI and Alaska Native populations (0.2%). 3
Even among AI populations in the US, it is important to consider regional variations in cancer incidence and mortality.11,12 In the Southern Plains, including Oklahoma, and the Southwest, AI persons had increases in both CRC incidence and mortality from 1990-2009, whereas AI in other regions had lower rates in both incidence and mortality. 6 In Oklahoma, a state with the second largest population of AIs in the US, 13 CRC age-adjusted incidence corrected for racial misclassification was highest among all racial groups, and was 1.7 times higher than that for NHWs (64.0/100,000 vs 38.5/100,000, respectively. 14 Age-adjusted CRC mortality in 2015 (the most recent year that corrected for racial misclassification) was also highest among AI and was 1.8 times higher than the state’s NHW population (28.9/100,000 vs. 17.1, respectively. 14
Cancer screening programs are largely responsible for the overall declining incidence among screening eligible populations as well as mortality in the US.3,15,16 Despite the proven effectiveness of CRC screening,16-18 AI populations have lower screening prevalence than the NHW or the general population, with some having among the lowest in the nation.19-26 Regional differences in CRC screening in the US general population are notable. 12 Moreover,27,28 region screening difference in the US follow patterns seen in incidence and mortality. While Oklahoma has the sixth lowest prevalence (64%) of up-to-date screening among all states, 3 only 51% of AI in the Indian Health Service (IHS) Oklahoma City Area are up to date. 29 While not all AI individuals receive CRC screening at IHS facilities, these numbers point to the importance of understanding barriers and facilitators to screening in a range of tribal health systems.
Barriers that occur at individual, community, clinical and health care system-levels impede the implementation of CRC screening interventions among AI communities. Some of these barriers include low per capita health care payments at clinics in the IHS, tribal health service, and urban Indian health programs, 30 especially for cancer care. 31 Other barriers for some AI patients include cost, insurance coverage, fear, stigma, lack of transportation, embarrassment, privacy issues, cultural beliefs about cancer screening, and lack of symptoms.20,32–35
These challenges show the need to implement effective CRC screening interventions specific to a range of tribal health care delivery systems and specific to the needs of AI persons. Few reports exist for any implementation of CRC screening in AI communities, 36 and none systematically evaluate the implementation of USPSTF evidence-based interventions (EBIs) and coordination of follow-up. Evidence-based interventions (EBIs) are proven strategies to increase the use of CRC screening tests. Multicomponent interventions that combine two or more EBIs lead to greater success in screening rates. 37 None of the trials in The Community Guide 37 focus on AI participants.
Environmental scans provide information about processes of care, approaches and awareness of screening, and help healthcare agencies identify the most promising areas for EBIs to meet the specific needs of the community, patients and the healthcare systems serving them. Derived from use in business and organizational studies, environmental scans are tools that are increasingly used in public health research and delivery fields to collect program development data for needs-assessment, decision-making, and strategic planning.38,39 This manuscript reports on our process of using environmental scan data to identify composite needs across partner sites to inform the development of EBIs for improving CRC screening in select tribal health care systems in Oklahoma. The environmental scans identified promising areas for EBIs in each of the partnering tribal health systems, and these findings served as the basis for developing the local interventions currently being piloted at each site. Included here is a broad summary of findings from the environmental scan data conducted with the Tribal and Urban Indian health care facilities in Oklahoma. This manuscript provides a roadmap for using qualitative environmental scan data to develop evidenced-based interventions for improving CRC screening in diverse tribal health care settings.
Methods
The consortium has completed the first phase of environmental scans. These data will inform the development of intervention strategies to increase provider delivery, community access to, and community priority for CRC screening at AI health care delivery systems in Oklahoma. This first phase of data collection informed the development of EBIs, currently being implemented in pilot sites across the consortium. These EBIs aligned with the Accelerating Colorectal Cancer Screening and Follow-up through Implementation Science (ACCSIS) program. The current manuscript focuses on the experience of the Oklahoma sites.
Interview/Focus Group Demographic Data by Site.

CNHSA provides primary care services to over 100,000 AI patients of whom over 17,000 are within the ages of 50 and 75 years. This tribal health system provides primary care services to Choctaw and other tribal citizens living in a this mostly rural area, presenting an opportunity to understand better perspectives associated with rural health care delivery in tribal populations.
Stakeholder interviews were conducted by university researchers (JB, MH) in collaboration with CRC Navigators at each site (JD, MG). CRC Navigators are the point persons at each site who help coordinate CRC screening and referrals, track screening rates, and document the implementation of EBIs. CRC Navigators from each site were instrumental in facilitating the environmental scan interviews by coordinating time and space for researchers to meet with patients and clinic staff. While the assistance of the local CRC Navigators during recruitment may have introduced some level of bias in attracting participants who may have been more reticent to participate otherwise, it was clear that their presence also promoted levels of trust among the clinic staff and patient populations necessary to facilitate expeditious data collection. Recruitment for individual patient interviews, for example, would almost certainly have been a lengthier process without the assistance of the CRC Navigators who already had some level of rapport with the patient base. Navigators did not influence the selection of specific participants, but assisted in the identification of individuals who met the approved inclusion criteria.
Individual interviews lasted about 30-45 minutes each and were conducted in private locations throughout the clinics, while small group discussions with providers were mostly conducted over the course of approximately hour-long lunch breaks. Description of the study goals and procedures were explained to all participants during the consenting process. The duration of data collection varied for each site. The qualitative interviews at the UIHCF were completed over two days. One researcher (MH), in collaboration with UIHCF Navigator (JD), completed back-to-back interviews with individual patients and one group discussion with providers over the course of five visits to the clinic. Data collection within the CNHSA was complex. The CN’s large geographic area involved substantial travel and coordination. Four clinics within the CNHSA system were selected for this first environmental scan phase based on size, capacity, population served, proximity to urban areas, and staffing. All interviews and group discussions were conducted over the course of one day per clinical site, by a single researcher (JB) working in collaboration with the CNHSA Navigator (MG). Approvals from the Choctaw Nation IRB, the Oklahoma City Area Indian Health Service IRB and the University of Oklahoma Health Sciences IRB were obtained prior to all data collection. The reporting of this study conforms to COREQ guidelines. 42
Results
Description of Themes for Qualitative Analysis]
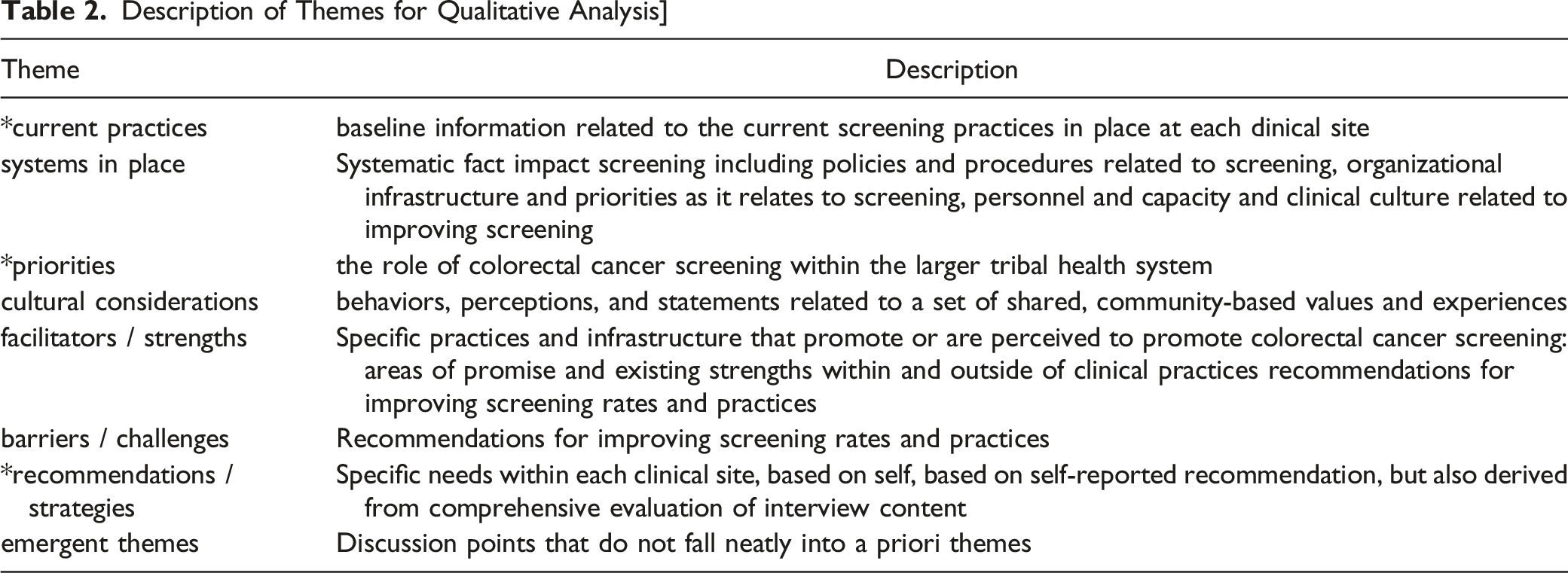
Conversations with stakeholders- including patients, providers, and leadership- provided rich data related to individual and system-level opportunities to improve CRC screening and care. A detailed thematic and discourse analysis of the full environmental scan data will be the focus of subsequent publications, but here we focus only on select themes most relevant to the development and implementation of EBIs across the pilot sites. Central to EBI development were the following thematic areas: current practices, needs and recommendations, and CRC priorities at each site.
UIHCF promotes fecal immunochemical test (FIT) as a front-line approach to screening and has already developed specific protocols, timelines, and personnel roles to facilitate the return of these screening kits. FIT kits are prioritized in this health system, in part, because UIHCF does not perform colonoscopies on site. Patients needing a colonoscopy are referred elsewhere, either locally if the patient has private insurance or, as is the case for most UIHCF patients, to one of two Indian Health Service or Tribal hospitals more than an hour away. This latter option is critically important for those who need it but also presents significant expenditures of time and resources for all parties. Opportunities for individual and system-level interventions here could focus on efficiency and rate of return of FIT kits, reduction of structural barriers to care for patients needing colonoscopies, and outreach to a diverse patient population.
At the start of this study, CNHSA utilized colonoscopies as a first line of screening, in large part because two of their eight primary care sites perform this procedure. Patients were referred outside of the system only if the patient was high-risk or preferred to use private insurance. As such, CNHSA has procedures in place to promote colonoscopy as the primary screening test, including EMR reminders, multi-sector clinical participation through a Global Program designed to synchronize policies across sites, a Healthy Aging Program to facilitate patient navigation through the screening process, and tribal programs to address specific barriers associated with completion of screenings (e.g. a fast-track system to reduce number of visits, ride share for tribal members, travel vouchers, on-site housing). These facilitators to screening are well-received by those familiar with them, but there remain opportunities for improvements in education, outreach, and synchronization of prevention priorities, policies, and screening practices across the clinical sites.
Composite Needs and Recommendations for Improving CRC Screening.

There was variation across partner sites related to capabilities and priorities for CRC screening, but a set of composite needs relevant to both UIHCF and CNHSA sites became clear. Interview data related to needs and recommendations- more than all other thematic categories from the interviews- produced actionable guidance that then informed the development of EBIs. Many of these needs were paired together for purposes of finalizing a set of clear multicomponent (MC) interventions to be applied across multiple health systems; for example, some sites identified the need to better track the return of FIT cards, while another site expressed a need for cost analyses to assess different testing options. These needs were grouped together as “Data” needs. Once classified in this way, each site could more easily assess their current practices and identify appropriate interventions relevant to their needs.
Discussions with UIHCF providers, for example, make clear their organizational priorities are aligned with CRC screening: “Our CEO’s initiative has become cancer care and prevention… so I think cancer screening in general is taking a forefront” (UIHCF providers). Providers here describe how competitions to “increase FIT kit hand out and return” promote a culture of prevention that incentivizes screenings and recognizes those who “do [their] job really well” (UIHCF providers). Establishing prevention as a priority among the entire team of providers also facilitates clear and consistent messaging from providers to patients. UIHCF patients with whom we spoke report that their first experience or knowledge of CRC screening often came from receiving a FIT kit from the clinic nurse during their appointment. Patients who characterize the FIT kits as “simple” are those who also report receiving clear instruction from their providers, suggesting that positive patient-provider interactions around screening then promote positive perceptions of prevention and screening receptivity.
As mentioned above, CNHSA prioritized colonoscopies as a first-line approach to CRC screening. The capacity to perform colonoscopies within their own health system is a tremendous benefit to patients who otherwise would be required to seek such services outside of the tribal health system. This capacity presents specific opportunities for system-level enhancements related to CRC screening, but these opportunities can be difficult to fully realize alongside competing health care priorities. The CNHSA’s service area includes 10 1/2 counties in southeast Oklahoma, including the lowest income region of the state, and a specific challenge for this system is the multitude of health disparities that present in the service area. It is difficult to prioritize colorectal cancer within a health system that serves a population afflicted by compounding co-morbidities, such as diabetes and heart disease, that tend to garner more attention and resources. A CNHSA care provider explains, “We are set up for diabetes…we are set up for that” (CN 24). Patients with whom we spoke describe diabetes as something that they see everywhere, “something that their friends and neighbors have” (CN 23), while colon cancer is less talked about and often only when individuals present with symptoms. Another CNHSA care provider suggests, “There could be some opportunities for some more education to maybe bring [CRC] back toward the front again…maybe some extra education. That never hurts to keep it at the forefront of peoples’ thoughts” (CN 8). Understanding local priorities- including competing priorities- is one step toward a roadmap to potentially more relevant interventions to address prevention, education and outreach, capacity, and balancing multiple health priorities.
Results from Planning Phase Environmental Scans to Identify Intervention Strategies for Increasing CRC Screening.

The EBIs in Table 4 align with Solberg’s conceptual framework for how small- to medium-sized medical practices can improve the implementation of evidence-based guidelines. 43 Solberg’s model of practice change, drawing on lessons from the Chronic Care Model (CCM) and the Model for Improvement, includes three pillars of practice improvement that correspond to the EBIs included in Table 3: 1) prioritize the change area- through community and patient education; 2) change capacity- through the reduction of structural barriers; and 3) change process content- by increasing provider delivery and continuous quality improvement (CQI). 43 Moving forward with the implementation of these EBIs, it is of particular interest to understand the processes whereby these interventions change and improve CRC screening.
Discussion
The approach to conducting an environmental scan described here was useful for establishing the beginnings of a roadmap toward developing EBIs across tribal health systems. Evidence-based interventions (EBIs), especially when two or more are combined into a multicomponent intervention, 37 are proven strategies to increase the use of CRC screening tests. Based on a systematic review of 88 studies evaluating intervention effects on cancer screening, the Community Preventive Services Task Force (CPSTF) reports the use of multi-component interventions should be applicable to urban or rural settings, healthcare systems, communities, or both, and different racial or ethnic groups. 37 The Community Guide findings, however, do not include any trials relevant to AI communities, a point that underscores the need to understand the impact of multi-component EBIs on CRC screening in diverse tribal health systems.
The environmental scan identified site-specific information related to current screening practices, specific needs and recommendations, and local priorities as it pertains to improving CRC screening uptake in AI communities. This information was then used to inform the selection of multicomponent interventions to be implemented across sites. Opportunities to improve delivery of care were not consistent across sites, an observation we expected given the different structures of the health care systems (Urban vs. Tribal), needs of the service populations, available resources, and variable priorities of the partner sites. One site, for example, had already established CRC screening as a priority with clinical and administrative mechanisms in place to support this work, while the other site was looking to enhance CRC screening within a health system that was committed to addressing other standing health priorities (such as diabetes). Likewise, increasing screening colonoscopies may not make sense for sites that refer patients out for the procedure, just as sites that perform their own colonoscopies may benefit more from interventions to improve coordination of care.
These differences matter and attention must be paid to how these distinctions impact important areas of patient care, including trust, resource allocation, access and barriers, and tailored outreach. Stakeholder feedback from the environmental scan was key to understanding the multifaceted ways that each health system navigated the barriers and opportunities to improve CRC screening at their own sites. The pathway to improve CRC screening is not uniform for all tribal health systems.
The approach described here is an example of how cross-site collaboration can lead to site-specific improvements in CRC screening. For example, we know that CRC screening and preventive services are often not addressed at a typical acute care clinic visit. To overcome these barriers, UIHCF implemented standing orders for stool card testing, distributes FIT kits at their pharmacy, public health stations, and other sites within their complex and drop boxes for discretely returning completed FIT kits are present. Notably, the experience with standing orders at UIHCF influenced CNHSA to implement standing orders at its clinics. We view this “cross-fertilization” as a strong reason for having Navigators for all clinics meet regularly to discuss successes and challenges.
Conclusion
This article reports on the utility of using environmental scan data to identify composite needs to improve CRC screening across diverse tribal health systems in Oklahoma. Environmental scan data from qualitative interviews and focus groups with multiple stakeholders indicated clear opportunities for individual and system-level interventions to enhance CRC screening. The environmental scan had utility for documenting current clinical practices, identifying needs and recommendations, and understanding site-specific CRC screening priorities; this information was critical for understanding the foundation for CRC screening and readiness for EBI implementation at each site.
Environmental scans provide a means to capture variability in capacity, local priorities, and observable efforts to address cultural considerations across diverse tribal health care systems. The work presented here offers the beginnings of roadmap, or template, for using environmental scan data to improve CRC screening within diverse tribal health systems. The environmental scan results provide clear paths to meaningful recommendations, though it is worth stating that these findings achieve the most value when made in combination with a comprehensive clinical evaluation that includes all relevant operators for program improvement. The environmental scan portion of this project is the first in a series of activities designed to engage multisector healthcare teams to provide educational opportunities regarding CRC and CRC screening, implement system-level strategies to increase provider delivery of CRC screening to eligible, average risk, AI participants, and to improve the navigational process for those with a positive CRC screen to appropriate diagnostic, treatment, and management services. The findings from this more expansive, comprehensive process will be made available in forthcoming manuscripts.
Intervention strategies should not follow a one-size-fits-all model. The successes (and failures) of intervention strategies must be contextually linked to local data. Given the high rate of colorectal cancer incidence and even higher rate of colorectal cancer mortality affecting American Indian populations, it is critical to implement screening strategies that address local variation across tribal health systems.
Our approach was premised on the value of multi-site collaborations; university and tribal partners collaborated to establish shared goals, to create a cross-site data collection instrument, and to share preliminary findings. We are currently expanding this approach to additional sites and will conduct environmental scans in additional sites, including Indian Health Service sites, across Oklahoma. The findings from this initial work, both in terms of the feasibility and usefulness of this approach, will inform how we proceed in subsequent sites.
Footnotes
Acknowledgments
We would like to acknowledge the tribal partners who participated in the design and conduct of this research, as well as the tribal citizens and employees who agreed to participate in the project. We would like to acknowledge the following individuals who contributed their time, ideas, and assistance in the development of this project: Paul Spicer, Gloria Tallbull, and Slate Boyer.
Author’s Contributions
JB led the data collection and analysis and drafted the initial version of the manuscript; DR, JC, ZN and MD reviewed and provided substantial content to the manuscript and assisted with data analysis; MD is PI of the project; TC, MG, HL, JD, MH and JB participated in data collection; MH provided project coordination; all authors participated in the conceptualization and implementation of the project and provided input on this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by grant P30CA225520 from the National Institutes of Health.
Ethical Approval
This project and manuscript was reviewed and approved by the University of Oklahoma Health Sciences Center Institutional Review Board (IRB NUMBER: 9970), the Choctaw Nation Institution Review Board, and the Oklahoma City Area Indian Health Service IRB. All participants provided written informed consent.
Data Availability
The datasets generated and/or analyzed during the current study are not publicly available per agreements with participating sovereign Tribal partners.