
Abstract
Introduction
American Indian and Alaska Native populations face persistent disparities in cancer incidence, mortality, and screening. In the Zuni Pueblo, health inequities persist for cancer screening rates, including cervical, breast, and colorectal cancer screening rates. This study evaluates the impact of a culturally tailored, community-based, cognitive-behavioral education intervention aimed at improving cancer-related knowledge, attitudes, and screening behaviors among Zuni adults.
Methods
A mixed-methods, community-engaged study was conducted with 117 Zuni adults (aged 21-75) who were non-adherent to United States Preventive Services Task Force cancer screening guidelines. Participants completed pre- and post-intervention surveys and engaged in age- and sex-specific cancer education sessions focused on cervical, breast, and/or colorectal cancer. Quantitative data were analyzed to assess changes in screening behavior and attitudes. Qualitative data from three post-intervention focus groups and two in-depth interviews (n = 12) were analyzed thematically to explore participant experiences and perceptions of the intervention.
Results
Post-intervention, screening attempts increased for all groups: 75% of younger women for cervical cancer, 60% of older women for mammograms, and 43% of men and 56% of women for stool blood tests. Participants reported higher odds of discussing their personal cancer risk with family, OR (95% CI) = 1.23 (1.12, 1.35), including significant associations for younger women and men. Qualitative participants emphasized the value of culturally specific content, visual materials, and social support in motivating screening. Barriers included limited appointment availability, transportation challenges, and concerns about confidentiality.
Conclusions
This culturally tailored education intervention enhanced cancer screening knowledge, attitudes, and behavior among Zuni Pueblo adults. Community engagement and culturally congruent messaging were essential to program success. Future efforts to reduce cancer disparities in indigenous communities should integrate Tribal perspectives, address structural barriers, and build sustainable, local capacity for cancer prevention and screening.
Keywords
Introduction
American Indian and Alaska Native (AI/AN) populations have historically experienced significant disparities in cancer incidence, mortality, and screening uptake.1-3 Cancer disparities are evident both in incidence and in stage at diagnosis. AI/AN populations experience higher incidence of colorectal and cervical cancers and are more often diagnosed at later stages. Although breast cancer incidence is lower among AI/AN women compared to non-Hispanic White women, AI/AN women are disproportionately diagnosed at later stages, highlighting a distinct disparity. 2
Key governmental reports and academic research studies consistently report that rates for cancer screening procedures and tests such as Papanicolaou smears (Pap smear or Pap test), mammograms, colonoscopies, and fecal occult blood tests (FOBT) are lower in AI/AN populations than the general US population.4-7 National data show significant gaps in cancer screening for AI/AN populations. 3 Biennial mammography rates are lower among AI/AN women than non-Hispanic White women (62% vs. 72%), and drop further among those receiving care through the Indian Health Service (IHS), where only 55% of women ages 52-64 years are screened. Colorectal cancer screening is also underutilized, with just 41% of AI/AN adults ages 50-75 using IHS services and 56% of AI/AN overall up to date, compared to 69% of non-Hispanic White adults. Cervical cancer screening deficits are especially pronounced for women served by IHS, where in 2023 only 33.8% of women ages 24-64 years were up to date with recommended screening. 8 Disparities in cancer screening are a key driver of the cancer stage at diagnosis disparity.
A growing body of literature has sought to document these disparities—particularly for cervical (CXC), breast (BC), and colorectal (CRC) cancers—while also exploring the multifaceted barriers to effective screening. However, despite these efforts, considerable challenges remain in both the quality of available evidence and in the development of culturally appropriate interventions. Theories and evidence indicate that when people have greater knowledge about screen-preventable cancers, they are more likely to seek and complete cancer screenings.9-11 Regular cancer screenings can help identify cancers at early and more effectively treatable stages. 11
Research has highlighted barriers including limited access to healthcare facilities, transportation challenges, and socioeconomic constraints.12,13 The literature often aggregates data across diverse Tribes and regions, masking important cultural and regional differences that could inform more tailored interventions. Some community-based interventions have shown promise by incorporating culturally tailored education and mobile health services, thereby increasing screening rates in pilot studies. While these strategies show promise, most have been limited to small pilot studies, often focused on a single cancer type and without sustained attention to Tribe-specific contexts or systemic barriers such as appointment access, transportation, and confidentiality. 14 Importantly, the most promising past efforts demonstrate community engagement in the design and implementation process, improving their cultural relevance, their potential impact, and long-term sustainability.14-16 These studies underscore the need for comprehensive, community-engaged interventions that are co-developed with Tribal partners to ensure cultural congruence, address structural barriers, and create lasting improvements in cancer screening and outcomes, as exemplified by the intervention tested in this study. Ultimately, improving cancer screening rates in these populations will depend on interventions that are not only evidence-based but also culturally congruent and systemically supported.
The body of recent research on cancer screening among AI/AN communities—particularly within the Zuni Pueblo—reveals a complex interplay of knowledge, cultural context, and systemic barriers that contribute to persistent disparities in cancer outcomes. Recent studies show that increased awareness and understanding of cancer risk are associated with screening behavior. For instance, research on CXC among Zuni women 17 and CRC on Zuni women and men 18 demonstrates that higher levels of cancer-specific knowledge significantly increase the likelihood of being screened. Similarly, findings indicate that enhanced health literacy is linked to improved screening behaviors for both CXC and CRC. 19 Additionally, perceptions of personal cancer risk among Zuni adults are influenced by factors such as family history, education, and overall knowledge about cancer risk factors. 20 These insights underscore the potential impact of educational interventions tailored to the cultural context of the Zuni community.
However, there are very few cancer screening and education programs tailored to AI/AN needs, let alone Tribe-specific communities.14,21,22 With collaboration from many Zuni stakeholders, our team developed a mixed-methods, multi-level, cognitive-behavioral cancer education program that centered Zuni experiences to improve knowledge about CXC, BC, and CRC cancer and cancer screening. This study aims to evaluate a pilot test of multicomponent culturally and linguistically appropriate intervention using a mixed-methods approach using both survey data and qualitative data, in terms of pre- and post-intervention changes in cancer-related attitudes, beliefs, and behaviors among people who participated in the education program intervention.
Methods
Overall Study Design
Overview of Study Design and Timeline a

aPlanned timeline interrupted by COVID-19 pandemic, public health mandates, and community needs.
Ethics
This study received research approval from the Zuni Pueblo Tribal Council, the Southwest Tribal Institutional Review Board (IRB) SWTIRB-2018-004 and the UNM HSC IRB (HRPO #18-264). All participants provided informed consent prior to and throughout each phase of data collection in this project. The reporting of this study conforms to the Good Reporting of A Mixed Methods Study (GRAMMS) guidelines. 23
Study Setting
Data for this study are from a community-engaged cancer control education intervention project conducted in Zuni Pueblo. The Pueblo is in a rural region of western New Mexico. Of the approximately 11,000 Zuni people, an estimated 7000 reside full-time in the Pueblo, where the median age is 33 years. 24 This study was conducted through a community–academic partnership between the Zuni Tribe and University of New Mexico researchers, guided by a Tribal Advisory Panel, with all materials developed through an iterative focus group process to ensure cultural and linguistic appropriateness. 25 Zuni team members, who are trained community health workers, also received training in research methods, survey administration, and qualitative data collection, and they led all stages of data collection and implementation of the education intervention to ensure cultural relevance and trust.
Participant Eligibility and Recruitment
Participants were eligible if they self-identified as American Indian, were members of the Zuni Tribe or married to a Zuni Tribal member and also if they met the United States Preventive Services Task Force (USPSTF) age and sex/gender criteria for the relevant cancer screenings. The education intervention for each group included the cancer or cancers that were specific to their sex/age status (CXC-only for younger women, CRC-only for men, and CXC, BC, and CRC for older women. Eligibility criteria were based on national screening recommendations current at study initiation (women aged 21-49 years eligible for CXC education; women aged 50-75 years for CXC, BC, and CRC education; and men aged 45-75 years for CRC education). During the study period, screening recommendations were updated to include younger women for certain services. To align with these changes, when necessary, women were reclassified into the older eligibility group. This adjustment ensured that analyses reflected current guideline definitions while maintaining internal consistency. For the purposes of analysis and discussion, participants are referred to as (1) women who received the CXC intervention only, (2) women who received BC, CRC, and CXC interventions, and (3) men who received the CRC intervention only. At screening, individuals were asked about their screening history to determine non-adherence and confirm age- and sex/gender-specific eligibility. While biological sex is the basis for these screenings, the term gender is used throughout the screening process and the materials based on practices aligned with the USPSTF. 26
Participants were recruited using a multi-pronged strategy. Recruitment began with randomly sampled streets from a complete enumeration of the Pueblo, with flyers delivered to all households on selected streets. Snowball sampling through initial contacts and key stakeholders supplemented this approach. Additional participants were reached through community events, high-traffic locations (e.g., post office, grocery store), flyers, word-of-mouth, and a local radio public service announcement (PSA). COVID-19 restrictions limited more active door-to-door recruitment, making these community-based strategies especially important. For the qualitative component, participants were drawn from those who completed both the pre- and post-intervention surveys and the education intervention, and who had consented to be contacted for follow-up.
All participants provided informed consent and were compensated for their time. Following the completion of the pre-survey and education program, women who received the CXC intervention only and men who received the CRC intervention only received $25 where women who received BC, CRC, and CXC interventions, received $50 following the completion of the pre-survey and education (screening completion was not incentivized for this program). Incentive amounts aligned with the length of time of the educational programs (older women received education on screenings for 3 cancers compared to only 1 cancer each for younger women and men). For participation in the qualitative data phase, participants received $50 merchandise cards for their time.
Multi-Level Cognitive Behavioral Cancer Education Program
Our intervention centered on the development of culturally tailored cancer informational materials designed specifically with and for the Zuni community. 25 Guided by a community-based participatory research approach, 15 we partnered with a Tribal Advisory Panel, local leaders, and community members to adapt existing evidence-based brochures, factsheets, and flipcharts for cancer screening education for CXC, BC, and CRC.
The intervention provided cancer-specific education based on the cancer-screenings recommended by USPSTF for each group (CXC for younger women, CRC for men, and CXC, CRC, and BC for older women). Each educational program included individual-level education sessions using flip charts to cover cancer risk, screening guidelines, and goal setting; contextual elements that encouraged conversations about personal and family cancer histories; and community-level materials such as PSAs, brochures, and posters. At the systems level, the program incorporated healthcare provider interactions, patient navigation, transportation services, and structured referral pathways between the Indian Health Service Zuni Service Unit and the UNM Comprehensive Cancer Center (UNM CCC).
The materials were developed to reflect Zuni language, artwork, photographs, and testimonials, and were written in plain, asset-based language to promote wellness and reduce fear around cancer. Iterative feedback from focus groups and pilot testing ensured that the materials were linguistically appropriate, responsive to community values, and aligned with Zuni cultural traditions, thereby strengthening both trust and relevance of the intervention. 25
The education program was administered in one-and-one and in group settings of 2-4 participants based on the availability and preference of the participant. The education sessions on age-/gender-specific cancers ranged from 1-2 hours. Following the education, the study team provided three reminders to participants on scheduling and/or obtaining age-gender appropriate screening. These reminders were either a phone call, text message, or home visit if the participant could not be reached via phone. The study team also provided additional support including providing transportation to the local healthcare facility. The reminders also ensured that retention occurred with participants from recruitment to the post-intervention survey, 6 to 8 months following the pre-survey.
Quantitative Data Collection
The pre and post intervention surveys documented age-/gender-specific, cancer-related screening patterns, attitudes, beliefs, and knowledge regarding cancers of the CXC, BC, and CRC. Survey development drew on multiple sources to ensure both scientific validity and cultural relevance: measures were adapted from the National Health Interview Survey (NHIS) and the Health Information National Trends Survey (HINTS), with additional items incorporated from prior validated studies conducted with diverse populations. Screening behaviors were measured using self-reported responses on both the pre- and post-intervention surveys. To address context-specific needs, a small set of new questions was created in consultation with Zuni stakeholders and subsequently piloted with community members to ensure clarity and appropriateness.
The study staff administered pre-intervention surveys to eligible participants from December 2022-April 2023 and post-intervention surveys to eligible participants from June 2023 through October 2023. All groups were interviewed about cancer beliefs, knowledge, and behaviors and each intervention group was interviewed about the specific cancer and related screening (BC, CXC, and CRC) that their education intervention highlighted. Thus, the survey varied in length based on intervention group. Surveys were conducted in person and over the phone based on participant availability and preferences.
Quantitative Data Analysis
Descriptive statistics were used to summarize baseline demographic characteristics of participants. Post-intervention cancer screening behaviors were analyzed stratified by age and gender groups using either Pearson’s Chi-squared test or Fisher’s exact test. Changes in cancer-related attitudes and self-reported behaviors were examined from pre-to post-education intervention. Where sample size permitted, bivariate analyses and odds ratios were estimated to assess associations between participant characteristics and screening behaviors. To accommodate the paired nature of the data, these odds ratios were obtained using logistic regression models that employed generalized estimating equations approaches. As covariates did not change from pre-to post-assessments, and within-participant changes were being considered, additional covariate adjustments were not employed. Statistical analyses were accomplished using SAS v9.4 (Cary, NC) and R 4.4.1.
Qualitative Data Collection
Participants were recruited for the focus groups from those that completed the post-intervention survey and selected “yes” for future contact for focus group participation (n = 68). Potential focus group participants include those that reported receiving and not receiving their screening during the 6 to 8 months of the program. We conducted one focus group with women who received the CXC intervention only (n = 3) for discussion of the CXC education intervention, one focus group with women who received BC, CRC, and CXC interventions, (n = 4) for the discussion of BC, CXC, and CRC education intervention, and the focus group and interviews with men who received the CRC intervention only (n = 3) for the discussion of the CRC education intervention. In addition, two men volunteered to participate but were unable to attend the scheduled group session. To ensure their perspectives were included, the focus group guide was administered individually to these participants. These individual interviews were analyzed together with the focus group data (total qualitative n = 12). This approach was consistent with our community-based participatory research (CBPR) framework, which emphasizes inclusivity and respect for all community members who wish to contribute.
Study team members conducted focus groups and interviews in person from October 2023 through November 2023. During each discussion, participants were given the opportunity to revisit the informational material (brochures, factsheets, and flipcharts), the education program itself, and the barriers and facilitators for the different cancers (BC, CRC, and CXC). We developed the focus group guides containing stem questions with follow-up probes to elicit feedback on the specifics for each of the three cancers. For example, participants were first broadly asked, “what did you think?” about the material, which then led to questions on comprehension of the content; impressions of the content and artwork; and sharing of the informational materials to family and friends. Focus group sessions lasted between 1 and 1.5 hours.
Qualitative Data Analysis
The qualitative analysis was conducted by four members of our research team. Three of the four team members were from Zuni Pueblo. Two members were community health workers who also served as data collection leads. The remaining two team members included a senior research scientist with an advanced degree and a PhD-level researcher with advanced training and experience in mixed methods research. This combination of locally grounded expertise and methodological specialization ensured that the analysis was both culturally responsive and rigorously executed.
Qualitative data analysis began with descriptive summaries of participant demographics to parallel the quantitative approach. An iterative thematic analysis was conducted using a combination of deductive and inductive coding strategies. We used a combination of deductive and inductive approaches in our thematic analysis. Deductive codes were developed a priori from the focus group guides and study aims (e.g., cancer knowledge, screening behaviors, healthcare experiences), while inductive coding was applied to identify unanticipated concepts, participant-driven insights, and emergent patterns beyond the guide.
The research team members independently coded transcripts and then met to compare coding, resolve discrepancies, and refine the codebook through consensus. Interrater reliability was assessed through repeated coding of selected transcripts until agreement was reached on code application. This process ensured both consistency across coders and inclusion of diverse interpretive perspectives. Mixed-methods triangulation was further achieved by comparing themes across participant subgroups (men, younger women, older women) and by integrating findings with the quantitative survey results.
Findings
Quantitative Results: Cancer Screening Behaviors
Following updates to screening recommendations, some women were reclassified into the older age group to reflect current eligibility. This resulted in a total of 131 participants who completed the baseline survey (23 women aged 21-44, 55 women aged 45-75, and 53 men aged 50-75). Of these, 125 completed the survey and education, and 117 completed all study components (pre-survey, education, and post-survey). Although recruitment targeted men aged 45-75 per USPSTF guidelines, enrolled male participants were aged 50-75. Analyses refer to these groups as (1) women who received CXC education only, (2) women who received BC, CRC, and CXC education, and (3) men who received CRC education only.
Characteristics of Education Intervention Participants Who Completed Both the Baseline and Follow-up Surveys, Overall and by Intervention Group
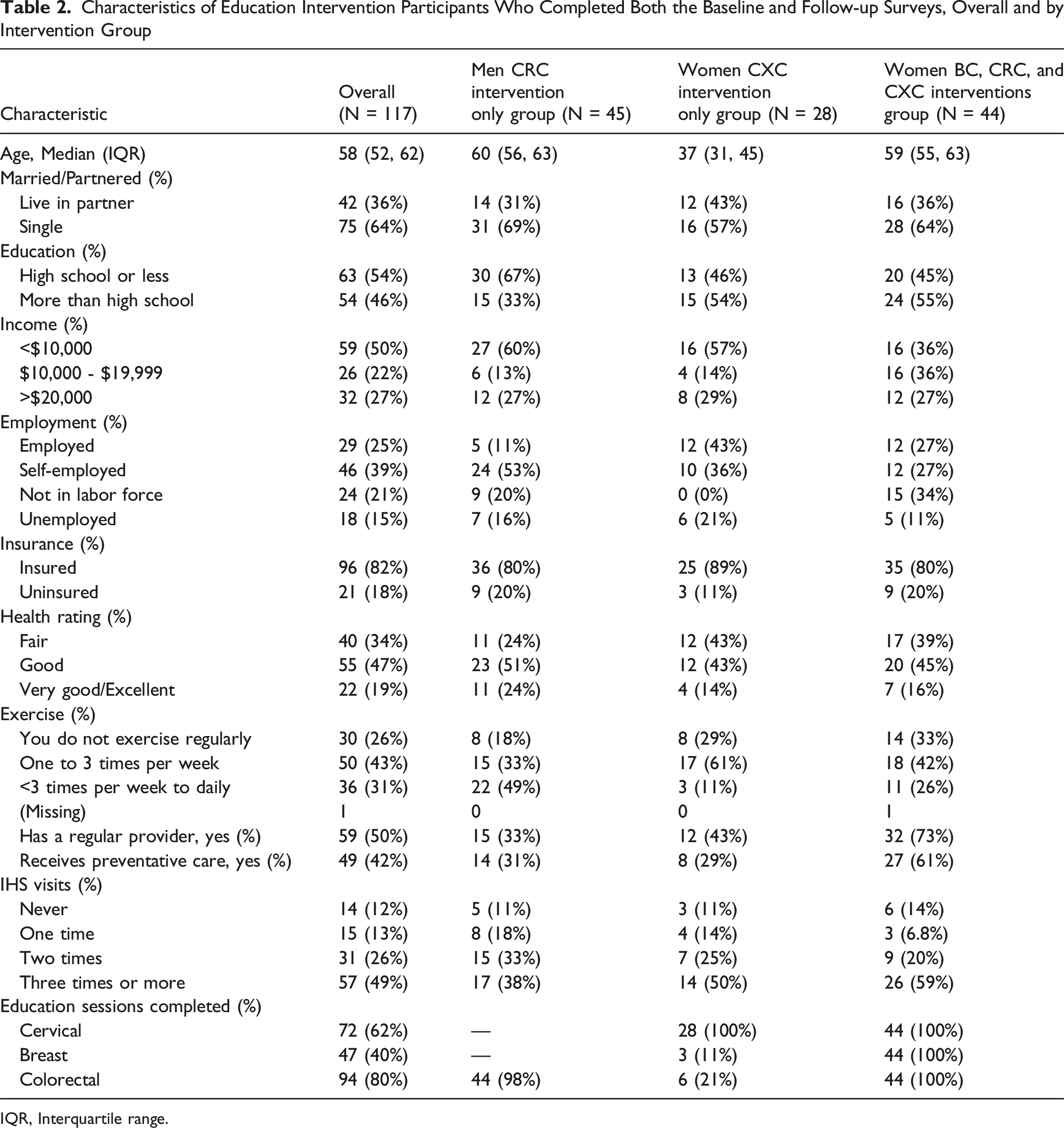
IQR, Interquartile range.
Bivariate Analyses of Post-intervention Cancer Screening Behaviors Between Intervention Groups
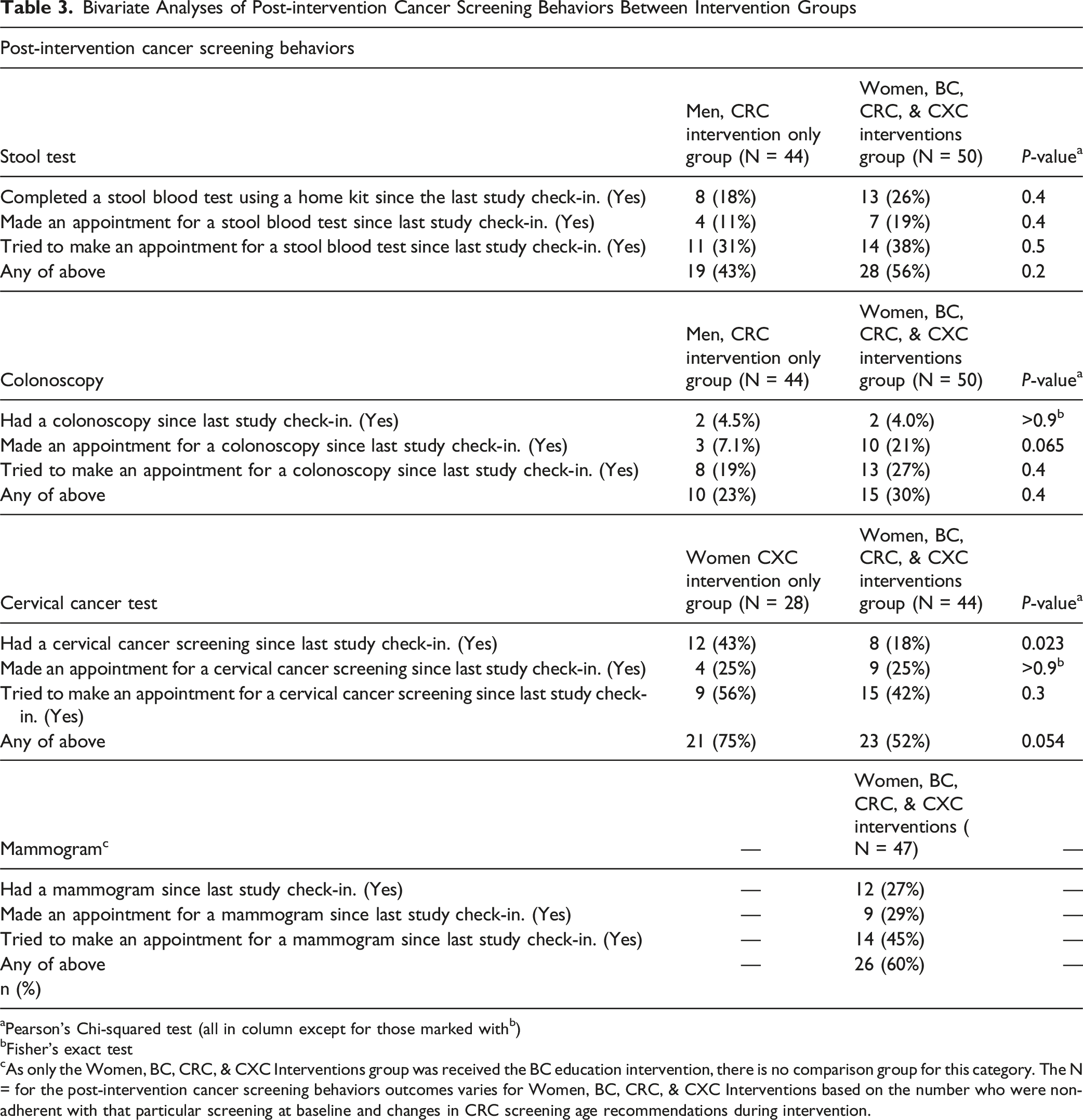
aPearson’s Chi-squared test (all in column except for those marked withb)
bFisher’s exact test
cAs only the Women, BC, CRC, & CXC Interventions group was received the BC education intervention, there is no comparison group for this category. The N = for the post-intervention cancer screening behaviors outcomes varies for Women, BC, CRC, & CXC Interventions based on the number who were non-adherent with that particular screening at baseline and changes in CRC screening age recommendations during intervention.
Quantitative Results: Cancer Attitudes and Behaviors
Numbers and Percentages of Individuals, Overall and Within Intervention Group Categories, Who Indicated That They Agree With Specific Attitudes, Beliefs, and Self-Reported Behaviors About Cancer Screening Pre- and Post-Education Interventions

Odds Ratio Estimates and 95% Confidence Intervals for Attitudes, Beliefs, and Self-Reported Behaviors About Cancer and Cancer Screening Pre- and Post-education Intervention

As shown in Table 4, participants generally reported positive shifts in cancer-related attitudes, beliefs, and self-reported behaviors following the education intervention. For example, the proportion of participants agreeing that the benefits of cancer screening outweigh any inconvenience increased from 80.3% to 86.3% overall. Similarly, the belief that family and friends would support them in screening rose from 88.9% to 94.0%. Notably, discussion of personal cancer risk with friends or relatives more than doubled, increasing from 18.0% pre-intervention to 38.5% post-intervention. Stratified findings suggested variation by age and gender. Younger women (women who received CXC education only) reported the largest gains in discussing personal cancer risk with friends or relatives (from 3.6% to 39.3%) and were more likely than older women or men to report changes in multiple domains.
These patterns are supported by the findings in Table 5, which presents odds ratio estimates for changes from pre-to post-intervention. Statistically significant increases were observed for the item “Have you ever discussed your personal risk for getting cancer with any of your friends or relatives?” with an overall odds ratio of 1.23 (95% CI: 1.12-1.35). This effect was especially pronounced among younger women (women who received CXC education only) (OR = 1.43, 95% CI: 1.20-1.71) and men (who received CRC education only) (OR = 1.31, 95% CI: 1.10-1.54). Other changes in attitudes and beliefs were in a positive direction but did not reach statistical significance.
Qualitative Results
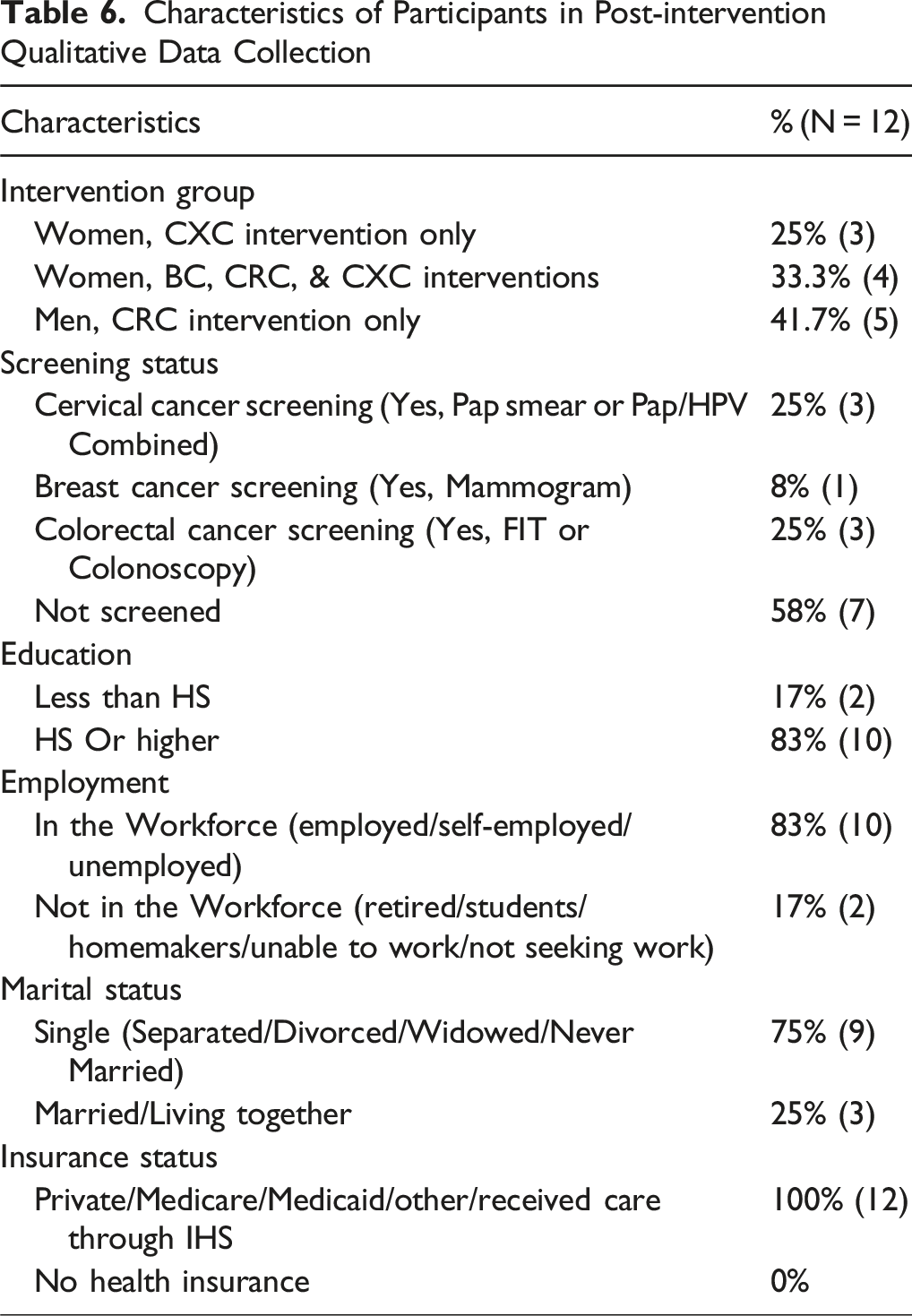
Characteristics of Participants in Post-intervention Qualitative Data Collection
Thematic Analysis With Supporting Quotes From Post-Intervention Qualitative Data

Together, these themes illustrate the complex interplay of individual, cultural, and systemic factors influencing cancer screening in the Zuni community. These themes cluster into three broader domains—education program and knowledge, cancer attitudes and behaviors, and healthcare experiences—which structure the presentation of qualitative findings that follow. Importantly, the qualitative results build on the quantitative survey findings by illuminating how and why observed changes occurred, offering nuanced insights into the cultural, social, and system-level dynamics that shape screening behaviors.
Qualitative Results: Education Program and Knowledge
Through the focus groups and in-depth interview participants shared a strong consensus that this education intervention was valuable. Table 6 displays the characteristics of the qualitative data collection participants. There was a mix of people who completed at least one screening after the education intervention (n = 5) and those who were in contemplation or preparation stages related to cancer screening. Participants reported learning from the education intervention; Table 7 reports the emergent themes and representative quotes from the data. Participants frequently described the cancer education program as a transformative learning experience that filled significant gaps in their prior understanding of cancer and screening. Many expressed that the program not only provided factual information but also helped reframe their perceptions of risk, action, and agency. One participant shared, “Because we weren’t educated. We didn’t know. But once I went through all of this, it kind of alleviated my fears like there’s still time. I can get educated. I can do this. … It was informative. This is a good thing. It was the best door I opened.” This quote captures a recurring narrative across the focus groups and interviews: education reduced fear, instilled hope, and motivated participants to take proactive steps toward their health. The sense of having “opened a door” reflects how increased knowledge enabled participants to envision new possibilities for cancer prevention and self-care.
They also shared educational material with family. It was valuable because it increased their knowledge about these cancers broadly and helped them by sharing that these cancers are treatable when detected early. The program helped them have conversations with their family and friends about cancer, cancer screening, and healthcare. They believed that the education groups where they learned together with others were a valuable experience and recommended having additional sessions.
Cervical, breast, and colorectal cancers can be a sensitive topic, even embarrassing, to discuss but the participants thought the educational material was engaging since it was tailored to Zuni and often expressed incentives to facilitate overcoming the embarrassment for screening. Participants emphasized the importance of receiving cancer education that was specifically relevant to their identities, experiences, and communities. Culturally tailored content—particularly information focused on Zuni—was seen as both affirming and essential for engagement and trust. One participant noted, “What really surprised me was the statistics about Native American women. And I am glad they had that in there because it wasn’t a study that was done in New York or something. It was something that pertained to me.” This response highlights how localized and culturally specific data helped participants connect personally to the content and see its relevance to their own lives. Another participant expressed a desire for more Native-centered resources, stating, “Most of the cancer [information] is, I’d say, for the White people, but we need to have it just on us. That way we can get an idea, a real grasp, on what is going on with us.” These reflections underscore how culturally tailored materials not only increased awareness but also promoted a sense of inclusion and ownership over health knowledge, reinforcing the importance of designing programs that reflect the cultural context and lived realities of Tribal communities. The education program had a positive impact. Clear, straightforward knowledge helped facilitate screening.
Qualitative Findings: Cancer Attitudes and Behaviors
Family and social support came up as especially important. While participants noted that sharing health details is difficult, all noted that they want to support others through health concerns and that their friends and family really want to be there for them, too. Finding ways to share the difficult health concerns, like cancer and even cancer screening, is something that the community wants to do for each other. Many noted that cancer is a topic that is rarely talked about, one being that others have strong feelings or beliefs about cancer thus avoiding the topic. However, participants shared how education has led them to start having more conversations with their family and friends, which is strengthening connections in addition to improving health care knowledge about cancer.
Participants described notable shifts in attitudes toward cancer and cancer screening, especially across generations. Younger individuals were perceived as more open to discussing health topics and more proactive in seeking preventive care. As one participant observed, “The generation now is different where they’re embracing different things now than where people will be more embarrassed and be like, ‘No, no.’ They’re not like that. If one person is on it, then they all be on it.” This quote reflects the role of peer influence and the emergence of collective behavior change, particularly among younger community members. Additionally, participants emphasized how communal gatherings and educational sessions fostered dialogue and created opportunities for information-sharing beyond the formal program. Another participant shared, “We really talk about it every time we gather like this… Then you get that information and start spreading it out to the community, if not your family.” This ripple effect—where information moves from individual participants to broader networks—illustrates how culturally grounded, group-based education can catalyze changes in both attitudes and behaviors. Together, these reflections highlight a shift from silence and stigma toward openness, discussion, and action in addressing cancer within Tribal communities.
The women shared that having Tribal leadership promote awareness in the community would be helpful. More men expressed that learning about cancer and gaining more knowledge on the topic can be intimidating and sometimes scary, but it can also be beneficial. There is hesitancy about screening but after realization, the person becomes more confident and thankful they took that step to be more aware and take control of their health.
Qualitative Findings: Healthcare Experiences
Participants shared positive experiences with healthcare, and some concerns about scheduling. The women reported mixed healthcare experiences with tradeoffs between proximity and appointment and wait times based on facilities, individuals report varying screening procedures and receiving results, and the issue of confidentiality in a small community. Overall, availability of appointments and having easier methods to make appointments would be a way to increase cancer screening. Transportation to healthcare facilities continues to be a barrier in the Zuni community.
Specific healthcare providers made a positive impact and impression. Participants identified strong, trusting relationships with healthcare providers as a key facilitator of cancer screening. These relationships were described as not only professional but also personal and culturally affirming. One participant shared how the identity and approach of a local provider enhanced their comfort with mammography: “[The healthcare provider doing mammograms] is a Zuni lady, but she makes you feel so comfortable. … At first, I was embarrassed, … but she was just joking around and sharing what she went through. … She just made me feel comfortable, so I don’t mind going back up there.” This reflection highlights how shared cultural background and empathetic communication can reduce discomfort and build trust, encouraging continued engagement in preventive care. Another participant emphasized the broader value of continuity and connection with a primary care provider, stating, “But I feel that by getting-- me making a choice to have that primary doctor, the relationship, the professional relationship between patient and doctor, it’s very beneficial and it’s helpful. And I really appreciate my doctor. He’s awesome.” These accounts underscore how respectful, person-centered care—especially when culturally attuned—can play a crucial role in overcoming barriers and supporting sustained participation in cancer screening.
Discussion
The integration of qualitative and quantitative strands strengthened interpretation of the findings, as community perspectives added nuance and depth to the quantitative patterns observed in screening behaviors. Taken together, the mixed-method findings demonstrate how community-informed education can both shift individual knowledge and behaviors and reshape broader communication patterns within families and peer groups. The pre-/post-survey data quantified improvements in knowledge, communication, and screening behaviors, while the qualitative data provided explanatory depth, highlighting the ways cultural tailoring, peer influence, and reduced stigma contributed to these changes. This integration aligns with prior studies showing that culturally grounded interventions improve cancer screening among American Indian and Alaska Native populations, yet our findings extend this literature by demonstrating subgroup-specific responses (e.g., notably among younger women and men) and by documenting how Tribal-specific adaptation fostered community-wide acceptance. In this way, the study both confirms the broader evidence base on the effectiveness of culturally tailored, multicomponent interventions, and adds new evidence on how tailoring to the unique cultural, linguistic, and social context of the Zuni community can help narrow subgroup disparities and normalize preventive behaviors.
Despite some positive associations between knowledge and screening, disparities persist due to a range of systemic and individual barriers. Research on BC screening 27 indicates that although many Zuni women have been screened at some point, adherence to screening guidelines is suboptimal—due to factors such as age and access to regular healthcare. Similar challenges are evident in CRC screening, where having a regular healthcare provider and holding fewer negative perceptions about tests (e.g., fecal occult blood testing) are critical for screening uptake. 18 Qualitative studies further reveal that inflexible clinic hours, transportation issues, brief patient-provider encounters, and the lack of effective reminder systems contribute significantly to low screening rates.16,25
Subgroup analyses revealed that some differences between participants narrowed after the intervention. Younger women, who initially reported lower engagement in cancer risk discussions, showed substantial post-intervention gains, while men also increased communication about cancer risk, aligning more closely with women’s responses. These patterns suggest that the program helped level pre-existing disparities in cancer-related communication and attitudes. Younger women appeared especially responsive to peer-influenced, culturally tailored messaging, while men benefited from gender-specific groups that reduced stigma. Older women showed smaller relative changes, consistent with a possible ceiling effect. Overall, these findings indicate that culturally grounded interventions can both elevate groups with lower baseline engagement and normalize preventive behaviors across the community.
The most important takeaway from these focus groups and in-depth interviews is that education content which is focused on American Indians and Tribe-specific cancer information and educational materials which are designed collaboratively with Zuni stakeholders and include testimonials on health, pictures, and artwork from Zuni create engagement and interest from Zuni participants in cancer education and screening.
Community input was pivotal in shaping these strategies. Focus groups with Zuni community members informed the development of informational materials that incorporate traditional health beliefs, native artwork, and local language, thereby enhancing cultural relevance and acceptance.25,27,28 Moreover, surveys assessing community preferences for various intervention approaches led to targeted, evidence-based recommendations for improving cancer screening. 28 These studies collectively suggest that multi-component interventions—ranging from personalized education and mailed screening tests to home visitations and enhanced provider support—are necessary to address both individual and system-level barriers.
Participants who have taken part in the cancer screening education program express that they have greater knowledge about cancer and motivation to seek cancer screenings. Those who completed a screening felt empowered about their health and wellbeing. Participants noted that they are starting to have conversations about cancer prevention with their families, friends, and community. An important finding was that some differences between subgroups of participants narrowed following the intervention. Younger women initially reported lower engagement in cancer risk discussions compared to older women and men, but post-intervention their rates increased substantially, such that subgroup differences diminished. Similarly, men showed notable gains in discussing cancer risk with family and friends, aligning more closely with women’s post-intervention responses. These patterns suggest that the educational program may have helped level pre-existing disparities in cancer-related communication and attitudes across demographic groups.
Several mechanisms may explain these convergences. Younger women appeared particularly responsive to culturally tailored, peer-influenced messaging, which may have amplified shifts in openness to dialogue and preventive care. For men, the opportunity to learn in gender-specific groups, combined with the normalization of sensitive conversations, may have reduced stigma and encouraged more active engagement. In contrast, older women, who already reported somewhat higher baseline knowledge and risk discussions, demonstrated smaller relative changes, indicating a possible “ceiling effect.” Together, these subgroup findings underscore how culturally tailored interventions can both elevate groups with lower baseline engagement and normalize preventive behaviors across the community. Future research should explore whether tailoring delivery modes (e.g., group-based learning for younger participants, provider reinforcement for older adults) can maximize impact across diverse subgroups.
Cancer and cancer screenings, especially for CXC, BC, and CRC, can be embarrassing and scary to talk about and to seek care for because of the sensitive and private nature of each type of cancer. Education, especially this type of community-based education, helps motivate participants to overcome embarrassment and fear to get screened. Local healthcare priorities should include a wider range of appointment options and consider ways to promote trust that health care information will stay private. There are some gaps in communication and processes for FOBT kits which if improved could have an impact on completion rates. Transportation to local and regional healthcare continues to be a challenge.
Strengths & Limitations
A key strength of this study is its use of a community-engaged, mixed methods design that combined quantitative surveys with qualitative focus groups and interviews, allowing us to capture both measurable changes in screening behaviors and the contextual factors that explain those changes. Additional strengths include the cultural tailoring of the intervention in close partnership with Zuni stakeholders. The involvement of Zuni research team members in study design, data collection, and analysis strengthened the cultural credibility of the findings and ensured that interpretation was grounded in community perspectives. While these strengths enhance the validity and relevance of the findings, several limitations should also be acknowledged.
Several limitations should be considered when interpreting these findings. First, the study relied on a pre–post design without a control group, limiting causal inference. Second, screening behaviors were self-reported, raising the possibility of recall or social desirability bias. The inclusion of culturally specific items on the pre- and post-intervention survey means generalizations should be made with attention to this context. The convenience sample may not be representative of all Zuni adults, and given the limited sample size, findings from these models are interpreted cautiously. Finally, the integration of quantitative and qualitative findings occurred at a single post-intervention time point, preventing assessment of longer-term sustainability of behavior change.
Overall, this study suggests that culturally tailored, community-led interventions may improve cancer screening knowledge and behaviors in American Indian populations while also helping to reduce subgroup disparities and foster community-wide normalization of preventive care.
Conclusion
Enhancing cancer knowledge, adapting health literacy assessments to better reflect cultural nuances, and addressing structural barriers are critical steps. Most importantly, integrating community preferences into the design of culturally tailored interventions offers a promising pathway to mitigate disparities and improve cancer outcomes among the Zuni and broader American Indian communities. The Zuni community can build on this project by continuing to use the culturally tailored flipcharts, brochures, and visuals in clinics, schools, and community gatherings, extending their reach beyond the study period. Community members’ sharing of materials with family suggests the potential for lasting influence through informal dialogue, while integration with local health services could formalize their use. More broadly, lessons such as the value of culturally specific messaging, sensitivity to confidentiality in small communities, and group-based education to reduce stigma can inform similar cancer prevention efforts in other Indigenous communities. Future efforts should continue to refine these strategies and rigorously evaluate their effectiveness in promoting guideline-concordant screening behaviors.
Footnotes
Acknowledgments
The authors gratefully acknowledge the Tribal stakeholders, including the Zuni Tribal Governor and his council members and the Tribal Advisory Panel members who contributed to the study activities. The authors are also grateful to the Zuni people who participated in the study.
Ethical Considerations
This study received research approval from the Zuni Pueblo Tribal Council, the Southwest Tribal Institutional Review Board (IRB) SWTIRB-2018-004 and the UNM HSC IRB (HRPO #18-264).
Consent to Participate
All participants provided informed consent prior to and throughout each phase of data collection in this project.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Cancer Institute of the National Institutes of Health grant R01CA192967 (Mishra PI), UNM Comprehensive Cancer Center (UNMCCC) Support Grant NIH/NCI P30CA118100 (Sanchez, PI), supplements to the UNMCCC Support Grant P30CA118100 (Sanchez PI; Mishra, PD), UNMCCC institutional pilot awards (PP-U1418-RS, PP-U1402-CaC, Mishra, PI), and the Institutional Development Award (IDeA) from the NIH/NIGMS P20GM103451 under the New Mexico IDeA Networks of Biomedical Research (NM-INBRE) Developmental Research Project Program (Mishra, PI of the Developmental Research Project).
Declaration of Conflicting Interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Data Availability Statement
Due to the nature of the ethical approval for this research, the data represented in this work are not publicly available.